- Purulent surgical infection

Содержание
- 2. Overall manifestations Signs of sepsis or other systemic disease are nonspecific and include disturbances of thermoregulation
- 3. 3. Respiratory disturbances - apnea, tachypnea (respirations >60/min), grunting, flaring of the alae nasi, intercostal or
- 4. Hematogenous Osteomyelitis Hematogenous infection begins in the medullary cavity of bones, is encased in a rigid
- 5. PATHOPHYSIOLOGY Microorganisms enter bone (Phagocytosis). Phagocyte contains the infection Release enzymes Lyse bone
- 6. PATHOPHYSIOLOGY Bacteria escape host defenses by: Adhering tightly to damage bone Persisting in osteoblasts Protective polysaccharide-rich
- 7. PATHOLOGY Acute ? Congested or thrombosed vessels Chronic ? Necrotic bone Absence of living osteocyte Mononuclear
- 8. Stages Toxic (adynamic) stage Septicopyemic stage Local stage
- 9. Forms Acute Osteomyelitis Sub-acute Osteomyelitis Chronic Osteomyelitis
- 10. Symptoms in newborn Clinical of septicemia : fever (36 - 74 %) irritable, refuses to feed,
- 11. Symptoms in infant Drowsy Irritable History of birth difficulties History of umbilical artery catheterization Metaphyseal tenderness
- 12. Symptoms in child Severe pain Malaise Fever Toxemia History of recent infection Local inflammation pus escape
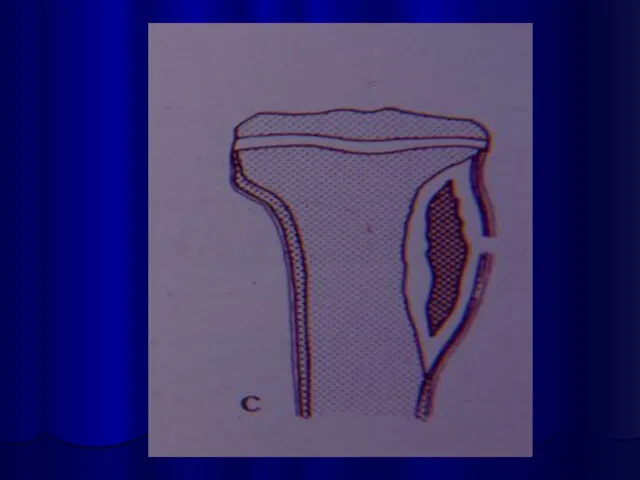
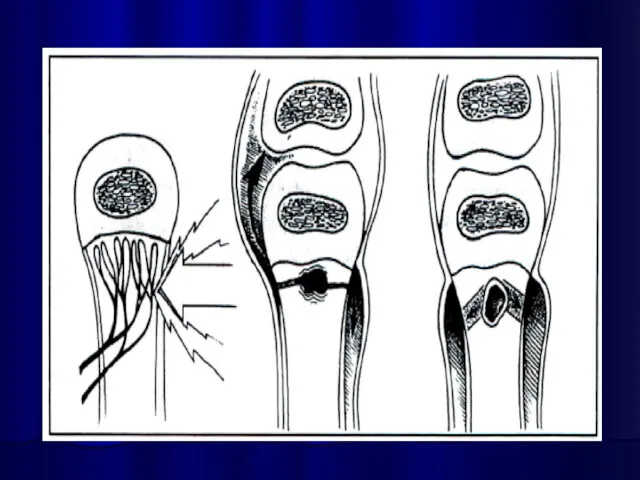
- 13. Outcomes Suppuration: 4-5 days Pus formation Subperiosteal abscess Pus spreading epiphysis joint medullary cavity soft tissue
- 14. Necrosis Bone death by the end of a week Bone destruction ← toxin ← ischemia Epiphyseal
- 16. New bone formation By the end of 2nd week (10 – 14 days) New bone formation
- 18. Joint capsule of 4 metaphysis cause of osteomyelitis Femoral head and neck ( hip ) Humeral
- 20. Septic Arthritis
- 21. Differential diagnosis Toxic synovitis Juvenile rheumatoid arthritis Cellulitis Pyomyositis Psoas abscess
- 22. Investigation Laboratory tests Plain film Ultrasonic diagnosis Aspirate bone liquid CT-scan
- 26. Septic arthritis Of Right hip
- 27. Investigation : Aspiration confirm diagnosis smear for cell and organism culture and sensitivity test
- 28. HEMATOGENOUS OSTEOMYELITIS Microbiologic features Staphylococci ? Aureus, Epidermidis Streptococci ? Group A & B Haemophilus influenzae
- 29. TREATMENT Initial treatment shoud be aggressive. Inadequate therapy ? Chronic disease Antibiotic use: Surgery Parenteral High
- 30. Antibiotic treatment
- 31. TREATMENT Indication for Surgery Diagnostic Hip joint involvement Neurologic complication Poor Sequestration
- 32. PROGNOSIS Is related to: Causative organisms Duration of symptoms & sign Patient age Duration of antibiotic
- 33. COMPLICATION Bone abscess Bacteremia Fracture Loosing of the prosthetic implant Overlying soft-tissue cellulitis Draining soft-tissue tract
- 34. Post Osteomyelitis Treatment
- 35. Septic Osteomyelitis Post Osteomyelitis Scar
- 36. Post Osteomyelitis Deformity of the Forearm
- 37. Necrotizing pneumonia Necrotizing pneumonia is characterized by inflammation of the alveoli and terminal airspaces in response
- 38. Pathophysiology The alveoli fill with proteinaceous fluid, which triggers a brisk influx and polymorphonuclear cells followed
- 39. Physical examination Newborns: rarely cough they more commonly present with tachypnea, retractions, grunting, and hypoxemia grunting
- 40. Toddlers and preschoolers: most often present with fever, cough (productive or nonproductive), tachypnea, and congestion sometimes
- 41. Generalized symptoms Intoxication sundrome Nasal flaring Auscultation: dry or bubbling rales, wheezing, diminished breath sounds, tubular
- 42. Extrapulmonary symptoms Abdominal pain or an ileus accompanied by emesis in patients with lower lobe pneumonia.
- 43. Diagnosis Laboratory tests (inflammation signs). Radiography Lung aspirate Sputum culture Blood culture Polymerase chain reaction Skin
- 45. Segmental-lobar opacification
- 46. Segmental-lobar opacification with pleural effusion
- 48. Differential diagnosis Afebrile Pneumonia Syndrome Airway Foreign Body Aspiration Syndromes Bronchiectasis Bronchiolitis Bronchitis, Acute and Chronic
- 49. Antibacterial therapy Cephalosporins (III-IV gen.): Ceftriaxone (Rocephin), Cefotaxime (Claforan), Cefuroxime (Zinacef, Ceftin, Kefurox). Macrolide antibiotics: Azithromycin
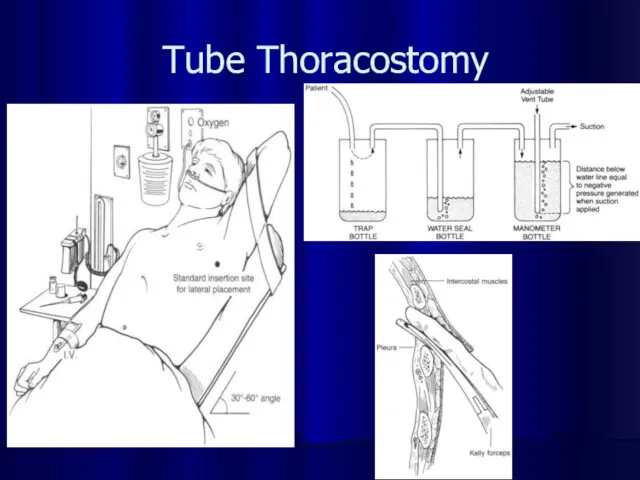
- 50. Tube Thoracostomy
- 53. Necrotic phlegmon Purulent lesions in the skin and hypodermic tissue, usually this process localisations in the
- 55. Causes Vulnerability epidermis A lot of intrecellular liquid Progress vasculature Congenital hypoplasia subjacent tissues
- 56. Clinical stages Intoxication syndrome Hyperaemia Compression soft tissues Edema Fluctuation Exfolation skin
- 57. Differential diagnosis Aseptic necrosis Erythematous erysipelas Idiopathic erysipelas Phlegmonous erysipelas
- 58. Treatment Fluid therapy Antibacterial therapy (cephalosporinis III- IV gen.) General health-improving therapy Surgical treatment – chess
- 61. Omphalitis Omphalitis is an infection of the umbilical stump. Omphalitis typically presents as a superficial cellulitis
- 62. Associated risk factors include the following: Low birth weight ( Prior umbilical catheterization Septic delivery Prolonged
- 63. Clinic Purulent or malodorous discharge from the umbilical stump Periumbilical erythema Edema Tenderness Ecchymoses Progression of
- 64. Differential diagnosis Umbilical fistula Soaking umbilical Enterocystoma
- 65. Complications Necrotizing fasciitis Myonecrosis Sepsis Septic embolization Particularly endocarditis and liver abscess formation Abdominal complications
- 66. Treatment Fluid therapy Antibacterial therapy (cephalosporinis III- IV gen.) Surgical care: management of necrotizing fasciitis and
- 67. Neonatal Sepsis Clinical syndrome of systemic illness accompanied by bacteremia occurring in the first month of
- 68. Early Onset First 5-7 days of life Usually multisystem fulminant illness with prominent respiratory symptoms (probably
- 69. Late Onset May occur as early as 5 days but is most common after the first
- 70. Causative organisms Primary sepsis Group B streptococcus Gram-negative enterics (esp. E. coli) Listeria monocytogenes, Staphylococcus, other
- 71. Risk factors Prematurity and low birth weight Premature and prolonged rupture of membranes Maternal peripartum fever
- 72. Clinical presentation Clinical signs and symptoms are nonspecific Differential diagnosis RDS Metabolic disease Hematologic disease CNS
- 73. Temperature irregularity (high or low) Change in behavior Lethargy, irritability, changes in tone Skin changes Poor
- 74. Diagnosis Cultures Blood Confirms sepsis 94% grow by 48 hours of age Urine Don’t need in
- 75. Treatment Antibiotics Primary sepsis: ampicillin and gentamicin Nosocomial sepsis: vancomycin and gentamicin or cefotaxime Change based
- 76. Supportive therapy Respiratory Oxygen and ventilation as necessary Cardiovascular Support blood pressure with volume expanders and/or
- 78. Скачать презентацию
Overall manifestations
Signs of sepsis or other systemic disease are
Overall manifestations
Signs of sepsis or other systemic disease are
3. Respiratory disturbances - apnea, tachypnea (respirations >60/min), grunting, flaring of
3. Respiratory disturbances - apnea, tachypnea (respirations >60/min), grunting, flaring of
Hematogenous Osteomyelitis
Hematogenous infection begins in the medullary cavity of bones,
Hematogenous Osteomyelitis
Hematogenous infection begins in the medullary cavity of bones,
PATHOPHYSIOLOGY
Microorganisms enter bone (Phagocytosis).
Phagocyte contains the infection
Release enzymes
Lyse bone
PATHOPHYSIOLOGY
Microorganisms enter bone (Phagocytosis).
Phagocyte contains the infection
Release enzymes
Lyse bone
PATHOPHYSIOLOGY
Bacteria escape host defenses by:
Adhering tightly to damage bone
Persisting in osteoblasts
Protective
PATHOPHYSIOLOGY
Bacteria escape host defenses by:
Adhering tightly to damage bone
Persisting in osteoblasts
Protective
PATHOLOGY
Acute ? Congested or thrombosed vessels
Chronic ? Necrotic bone
Absence of
PATHOLOGY
Acute ? Congested or thrombosed vessels
Chronic ? Necrotic bone
Absence of
Stages
Toxic (adynamic) stage
Septicopyemic stage
Local stage
Stages
Toxic (adynamic) stage
Septicopyemic stage
Local stage
Forms
Acute Osteomyelitis
Sub-acute Osteomyelitis
Chronic Osteomyelitis
Forms
Acute Osteomyelitis
Sub-acute Osteomyelitis
Chronic Osteomyelitis
Symptoms in newborn
Clinical of septicemia : fever (36 - 74 %)
Symptoms in newborn
Clinical of septicemia : fever (36 - 74 %)

Symptoms in infant
Drowsy
Irritable
History of birth difficulties
History of umbilical artery catheterization
Metaphyseal tenderness
Symptoms in infant
Drowsy
Irritable
History of birth difficulties
History of umbilical artery catheterization
Metaphyseal tenderness
Symptoms in child
Severe pain
Malaise
Fever
Toxemia
History of recent infection
Local inflammation pus escape from
Symptoms in child
Severe pain
Malaise
Fever
Toxemia
History of recent infection
Local inflammation pus escape from
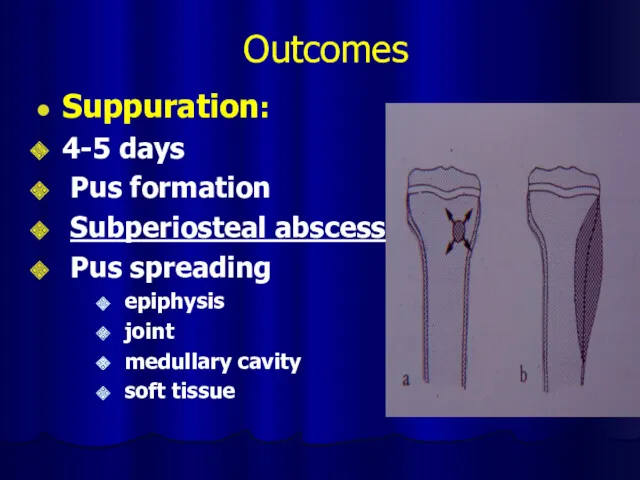
Outcomes
Suppuration:
4-5 days
Pus formation
Subperiosteal abscess
Pus spreading
epiphysis
joint
medullary
Outcomes
Suppuration:
4-5 days
Pus formation
Subperiosteal abscess
Pus spreading
epiphysis
joint
medullary
Necrosis
Bone death by the end of a week
Bone destruction ← toxin
Necrosis
Bone death by the end of a week
Bone destruction ← toxin
New bone formation
By the end of 2nd week
(10 – 14
New bone formation
By the end of 2nd week (10 – 14

Joint capsule of 4 metaphysis cause of osteomyelitis
Femoral head and
Joint capsule of 4 metaphysis cause of osteomyelitis
Femoral head and
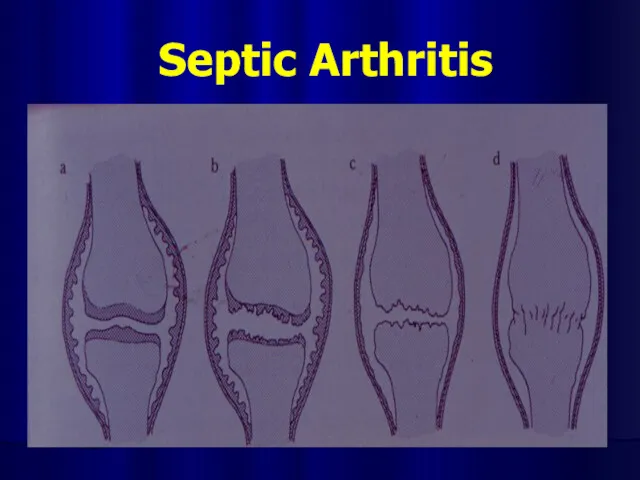
Septic Arthritis
Septic Arthritis
Differential diagnosis
Toxic synovitis
Juvenile rheumatoid arthritis
Cellulitis
Pyomyositis
Psoas abscess
Differential diagnosis
Toxic synovitis
Juvenile rheumatoid arthritis
Cellulitis
Pyomyositis
Psoas abscess
Investigation
Laboratory tests
Plain film
Ultrasonic diagnosis
Aspirate bone liquid
CT-scan
Investigation
Laboratory tests
Plain film
Ultrasonic diagnosis
Aspirate bone liquid
CT-scan




Septic arthritis
Of
Right hip
Septic arthritis
Of
Right hip
Investigation : Aspiration
confirm diagnosis
smear for cell and organism
culture and sensitivity
Investigation : Aspiration
confirm diagnosis
smear for cell and organism
culture and sensitivity
HEMATOGENOUS OSTEOMYELITIS
Microbiologic features
Staphylococci ? Aureus, Epidermidis
Streptococci ? Group A & B
Haemophilus
HEMATOGENOUS OSTEOMYELITIS
Microbiologic features
Staphylococci ? Aureus, Epidermidis
Streptococci ? Group A & B
Haemophilus
TREATMENT
Initial treatment shoud be aggressive.
Inadequate therapy ? Chronic disease
Antibiotic use:
Surgery
Parenteral
High doses
Good
TREATMENT
Initial treatment shoud be aggressive.
Inadequate therapy ? Chronic disease
Antibiotic use:
Surgery
Parenteral
High doses
Good
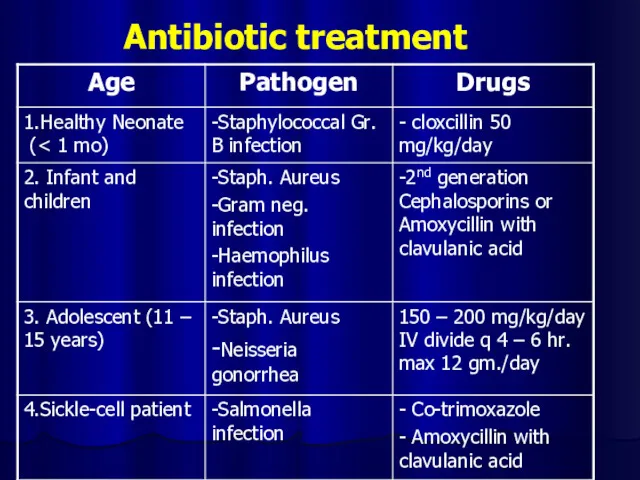
Antibiotic treatment
Antibiotic treatment
TREATMENT
Indication for Surgery
Diagnostic
Hip joint involvement
Neurologic complication
Poor
Sequestration
TREATMENT
Indication for Surgery
Diagnostic
Hip joint involvement
Neurologic complication
Poor
Sequestration
PROGNOSIS
Is related to:
Causative organisms
Duration of symptoms & sign
Patient age
Duration of antibiotic
PROGNOSIS
Is related to:
Causative organisms
Duration of symptoms & sign
Patient age
Duration of antibiotic
COMPLICATION
Bone abscess
Bacteremia
Fracture
Loosing of the prosthetic implant
Overlying soft-tissue cellulitis
Draining soft-tissue tract
COMPLICATION
Bone abscess
Bacteremia
Fracture
Loosing of the prosthetic implant
Overlying soft-tissue cellulitis
Draining soft-tissue tract

Post Osteomyelitis Treatment
Post Osteomyelitis Treatment

Septic Osteomyelitis
Post Osteomyelitis Scar
Septic Osteomyelitis
Post Osteomyelitis Scar

Post Osteomyelitis Deformity of the Forearm
Post Osteomyelitis Deformity of the Forearm
Necrotizing pneumonia
Necrotizing pneumonia is characterized by inflammation of the alveoli
Necrotizing pneumonia
Necrotizing pneumonia is characterized by inflammation of the alveoli
Pathophysiology
The alveoli fill with proteinaceous fluid, which triggers a brisk influx
Pathophysiology
The alveoli fill with proteinaceous fluid, which triggers a brisk influx
Physical examination
Newborns:
rarely cough
they more commonly present with tachypnea, retractions, grunting, and
Physical examination
Newborns:
rarely cough
they more commonly present with tachypnea, retractions, grunting, and
Toddlers and preschoolers:
most often present with fever, cough (productive or nonproductive),
Toddlers and preschoolers:
most often present with fever, cough (productive or nonproductive),
Generalized symptoms
Intoxication sundrome
Nasal flaring
Auscultation: dry or bubbling rales, wheezing, diminished breath
Generalized symptoms
Intoxication sundrome
Nasal flaring
Auscultation: dry or bubbling rales, wheezing, diminished breath
Extrapulmonary symptoms
Abdominal pain or an ileus accompanied by emesis in
Extrapulmonary symptoms
Abdominal pain or an ileus accompanied by emesis in
Diagnosis
Laboratory tests (inflammation signs).
Radiography
Lung aspirate
Sputum culture
Blood culture
Polymerase chain reaction
Skin tests (TB
Diagnosis
Laboratory tests (inflammation signs).
Radiography
Lung aspirate
Sputum culture
Blood culture
Polymerase chain reaction
Skin tests (TB

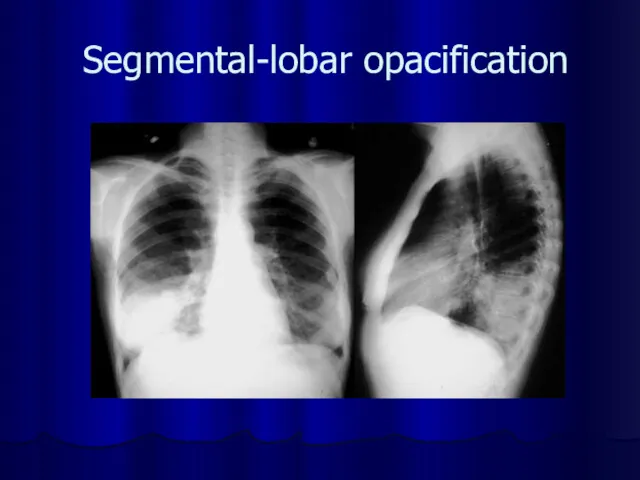
Segmental-lobar opacification
Segmental-lobar opacification
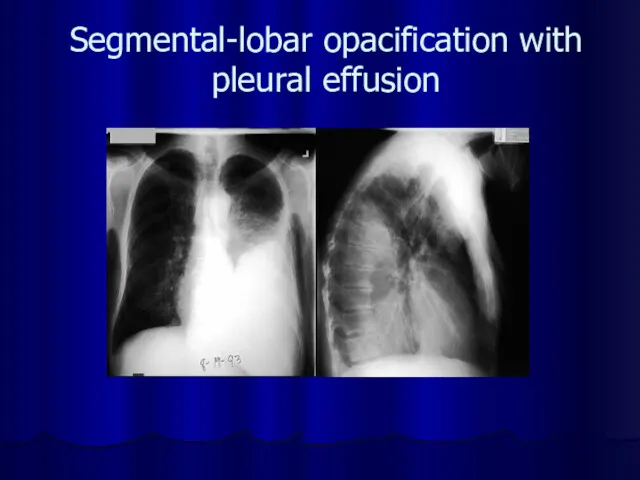
Segmental-lobar opacification with pleural effusion
Segmental-lobar opacification with pleural effusion

Differential diagnosis
Afebrile Pneumonia Syndrome
Airway Foreign Body
Aspiration Syndromes
Bronchiectasis
Bronchiolitis
Bronchitis, Acute and Chronic
Chronic
Differential diagnosis
Afebrile Pneumonia Syndrome
Airway Foreign Body
Aspiration Syndromes
Bronchiectasis
Bronchiolitis
Bronchitis, Acute and Chronic
Chronic
Antibacterial therapy
Cephalosporins (III-IV gen.): Ceftriaxone (Rocephin), Cefotaxime (Claforan), Cefuroxime (Zinacef, Ceftin,
Antibacterial therapy
Cephalosporins (III-IV gen.): Ceftriaxone (Rocephin), Cefotaxime (Claforan), Cefuroxime (Zinacef, Ceftin,
Tube Thoracostomy
Tube Thoracostomy

Necrotic phlegmon
Purulent lesions in the skin and hypodermic
tissue,
Necrotic phlegmon
Purulent lesions in the skin and hypodermic
tissue,

Causes
Vulnerability epidermis
A lot of intrecellular liquid
Progress vasculature
Congenital hypoplasia subjacent tissues
Causes
Vulnerability epidermis
A lot of intrecellular liquid
Progress vasculature
Congenital hypoplasia subjacent tissues
Clinical stages
Intoxication syndrome
Hyperaemia
Compression soft tissues
Edema
Fluctuation
Exfolation skin
Clinical stages
Intoxication syndrome
Hyperaemia
Compression soft tissues
Edema
Fluctuation
Exfolation skin
Differential diagnosis
Aseptic necrosis
Erythematous erysipelas
Idiopathic erysipelas
Phlegmonous erysipelas
Differential diagnosis
Aseptic necrosis
Erythematous erysipelas
Idiopathic erysipelas
Phlegmonous erysipelas

Treatment
Fluid therapy
Antibacterial therapy (cephalosporinis III- IV gen.)
General health-improving therapy
Surgical treatment –
Treatment
Fluid therapy
Antibacterial therapy (cephalosporinis III- IV gen.)
General health-improving therapy
Surgical treatment –


Omphalitis
Omphalitis is an infection of the umbilical stump. Omphalitis typically
Omphalitis
Omphalitis is an infection of the umbilical stump. Omphalitis typically
Associated risk factors include the following:
Low birth weight (<2500 g)
Associated risk factors include the following:
Low birth weight (<2500 g)
Clinic
Purulent or malodorous discharge from the umbilical stump
Periumbilical erythema
Edema
Clinic
Purulent or malodorous discharge from the umbilical stump
Periumbilical erythema
Edema

Differential diagnosis
Umbilical fistula
Soaking umbilical
Enterocystoma
Differential diagnosis
Umbilical fistula
Soaking umbilical
Enterocystoma

Complications
Necrotizing fasciitis
Myonecrosis
Sepsis
Septic embolization
Particularly endocarditis and liver abscess formation
Abdominal
Complications
Necrotizing fasciitis
Myonecrosis
Sepsis
Septic embolization
Particularly endocarditis and liver abscess formation
Abdominal

Treatment
Fluid therapy
Antibacterial therapy (cephalosporinis III- IV gen.)
Surgical care: management of necrotizing
Treatment
Fluid therapy
Antibacterial therapy (cephalosporinis III- IV gen.)
Surgical care: management of necrotizing
Neonatal Sepsis
Clinical syndrome of systemic illness accompanied by bacteremia occurring in
Neonatal Sepsis
Clinical syndrome of systemic illness accompanied by bacteremia occurring in
Early Onset
First 5-7 days of life
Usually multisystem fulminant illness with
Early Onset
First 5-7 days of life
Usually multisystem fulminant illness with
Late Onset
May occur as early as 5 days but is most
Late Onset
May occur as early as 5 days but is most
Causative organisms
Primary sepsis
Group B streptococcus
Gram-negative enterics (esp. E. coli)
Listeria monocytogenes, Staphylococcus,
Causative organisms
Primary sepsis
Group B streptococcus
Gram-negative enterics (esp. E. coli)
Listeria monocytogenes, Staphylococcus,
Risk factors
Prematurity and low birth weight
Premature and prolonged rupture of membranes
Maternal
Risk factors
Prematurity and low birth weight
Premature and prolonged rupture of membranes
Maternal
Clinical presentation
Clinical signs and symptoms are nonspecific
Differential diagnosis
RDS
Metabolic disease
Hematologic disease
CNS disease
Cardiac
Clinical presentation
Clinical signs and symptoms are nonspecific
Differential diagnosis
RDS
Metabolic disease
Hematologic disease
CNS disease
Cardiac
Temperature irregularity (high or low)
Change in behavior
Lethargy, irritability, changes in tone
Skin
Temperature irregularity (high or low)
Change in behavior
Lethargy, irritability, changes in tone
Skin
Diagnosis
Cultures
Blood
Confirms sepsis
94% grow by 48 hours of age
Urine
Don’t need in infants
Diagnosis
Cultures
Blood
Confirms sepsis
94% grow by 48 hours of age
Urine
Don’t need in infants
Treatment
Antibiotics
Primary sepsis: ampicillin and gentamicin
Nosocomial sepsis: vancomycin and gentamicin or cefotaxime
Change
Treatment
Antibiotics
Primary sepsis: ampicillin and gentamicin
Nosocomial sepsis: vancomycin and gentamicin or cefotaxime
Change
Supportive therapy
Respiratory
Oxygen and ventilation as necessary
Cardiovascular
Support blood pressure with volume expanders
Supportive therapy
Respiratory
Oxygen and ventilation as necessary
Cardiovascular
Support blood pressure with volume expanders
 Деятельность медицинской сестры в осуществлении мероприятий по профилактике миопии среди школьников
Деятельность медицинской сестры в осуществлении мероприятий по профилактике миопии среди школьников Мениски. Шов менисков или резекция? Что выбрать при повреждениях менисков коленного сустава?
Мениски. Шов менисков или резекция? Что выбрать при повреждениях менисков коленного сустава? Биожүйелердің электрөткізгіштігі
Биожүйелердің электрөткізгіштігі Узкий таз в акушерстве
Узкий таз в акушерстве Условные предложения. Виды условных предложений
Условные предложения. Виды условных предложений Грязелечение
Грязелечение Адресная доставка лекарственных нанопрепаратов в применении к моделям рака на доклиническом этапе исследований
Адресная доставка лекарственных нанопрепаратов в применении к моделям рака на доклиническом этапе исследований Гигиенические основы физического воспитания и закаливания детей и подростков
Гигиенические основы физического воспитания и закаливания детей и подростков Профессия врача. Одна из самых нужных и важных профессий
Профессия врача. Одна из самых нужных и важных профессий Самостоятельная работа интерна. Нарушения пищевого поведения
Самостоятельная работа интерна. Нарушения пищевого поведения Скульптурное моделирование лица
Скульптурное моделирование лица Перитонит, панкреатит, сепсис
Перитонит, панкреатит, сепсис Природно-очаговое заболевание чума
Природно-очаговое заболевание чума Pulp involvement
Pulp involvement ВИЧ-инфекция и СПИД
ВИЧ-инфекция и СПИД МРТ в диагностики ишемического инсульта. Сосудистая патология. Лекция 3
МРТ в диагностики ишемического инсульта. Сосудистая патология. Лекция 3 Сибирская язва. Возбудитель, эпидемиология, патогенез, диагностика, лечение, профилактика
Сибирская язва. Возбудитель, эпидемиология, патогенез, диагностика, лечение, профилактика Өкпе туберкулезі
Өкпе туберкулезі Почки. Анатомия почки. Нефрэктомия
Почки. Анатомия почки. Нефрэктомия Сахарный диабет у детей
Сахарный диабет у детей Тромбоэмолдық синдром
Тромбоэмолдық синдром Классификации психического дизонтогенеза
Классификации психического дизонтогенеза Медики - структура. Структура медицинского образования в Германии
Медики - структура. Структура медицинского образования в Германии Принципы рационального питания
Принципы рационального питания Сравнительный анализ методов хирургического лечения стрессового недержания мочи у женщин
Сравнительный анализ методов хирургического лечения стрессового недержания мочи у женщин Генетика негіздері
Генетика негіздері Склеродермия. Этиология склеродермии
Склеродермия. Этиология склеродермии Орнитоз (пситтакоз)
Орнитоз (пситтакоз)