- Tetanus. Distribution

Содержание
- 2. Brief history of disease 5th century BC: Hippocrates first described the disease 1884: Carle and Rattone
- 3. Distribution In developing countries, neonatal tetanus is a leading cause of neonatal mortality, accounting for over
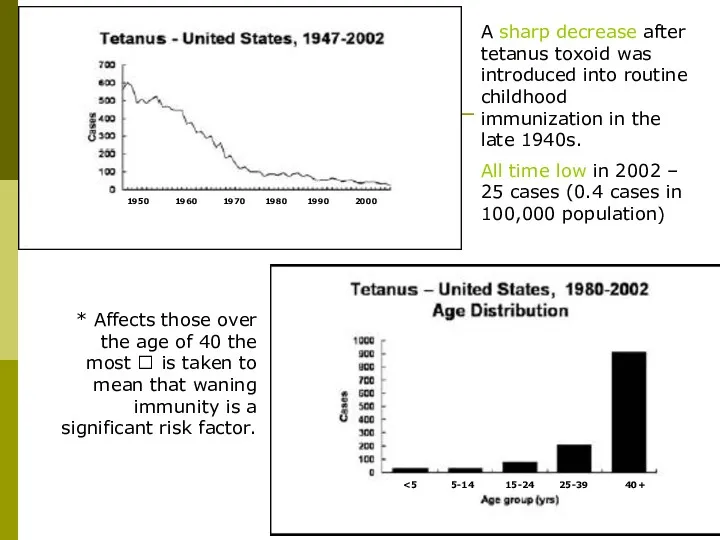
- 4. 1950 5-14 15-24 25-39 40+ A sharp decrease after tetanus toxoid was introduced into routine childhood
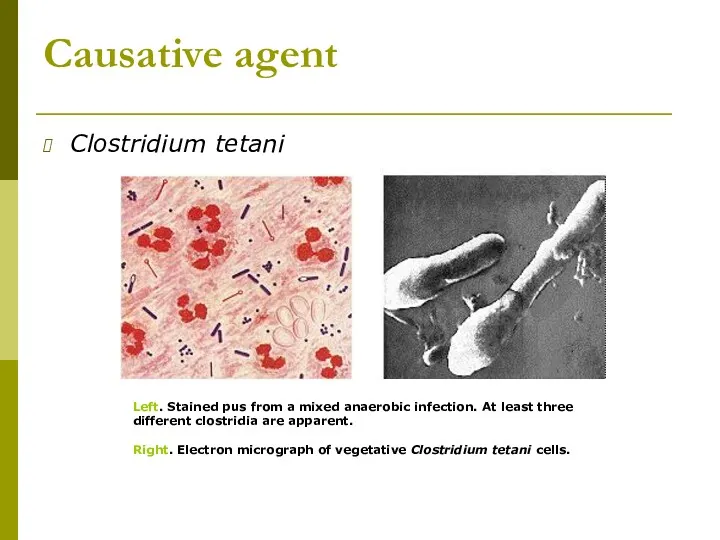
- 5. Causative agent Clostridium tetani Left. Stained pus from a mixed anaerobic infection. At least three different
- 6. Morphology & Physiology Relatively large, Gram-positive, rod-shaped bacteria Spore-forming, anaerobic. Found in soil, especially heavily-manured soils,
- 7. Virulence & Pathogenicity Not pathogenic to humans and animals by invasive infection but by the production
- 8. Tetanus toxin Produced when spores germinate and vegetative cells grow after gaining access to wounds. The
- 9. Initially binds to peripheral nerve terminals Transported within the axon and across synaptic junctions until it
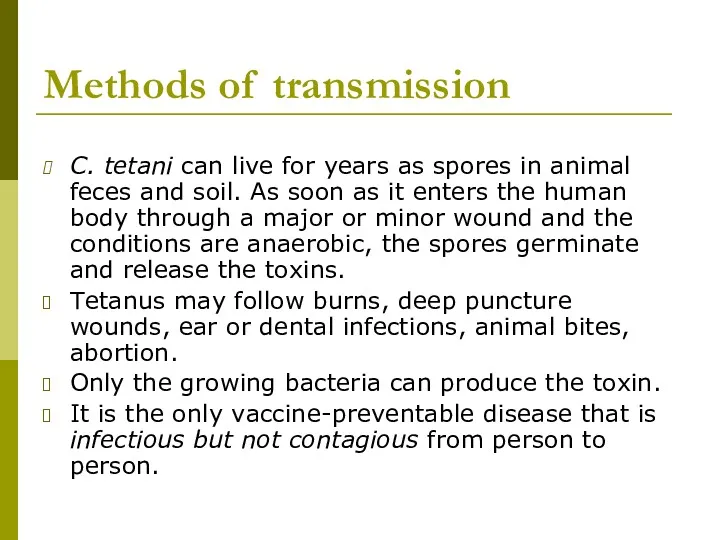
- 10. Methods of transmission C. tetani can live for years as spores in animal feces and soil.
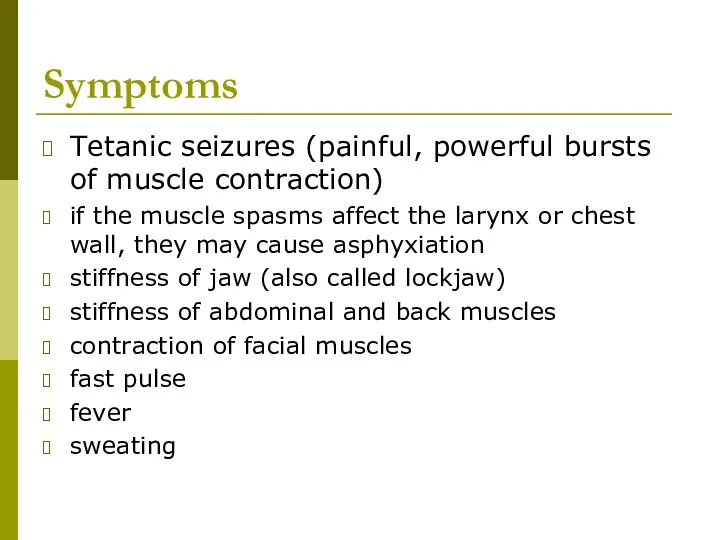
- 11. Symptoms Tetanic seizures (painful, powerful bursts of muscle contraction) if the muscle spasms affect the larynx
- 12. The back muscles are more powerful, thus creating the arc backward “Oposthotonus” by Sir Charles Bell,
- 13. Types of tetanus: local, cephalic, generalized, neonatal Incubation period: 3-21 days, average 8 days. Uncommon types:
- 14. Most common types: Generalized tetanus descending pattern: lockjaw ? stiffness of neck ? difficulty swallowing ?
- 15. Methods of diagnosis Based on the patient’s account and physical findings that are characteristic of the
- 16. Clinical treatment If treatment is not sought early, the disease is often fatal. The bacteria are
- 17. Method of prevention - immunization A person recovering from tetanus should begin active immunization with tetanus
- 18. What else can be done? Remove and destroy the source of the toxin through surgical exploration
- 20. Скачать презентацию
Brief history of disease
5th century BC: Hippocrates first described the
Brief history of disease
5th century BC: Hippocrates first described the
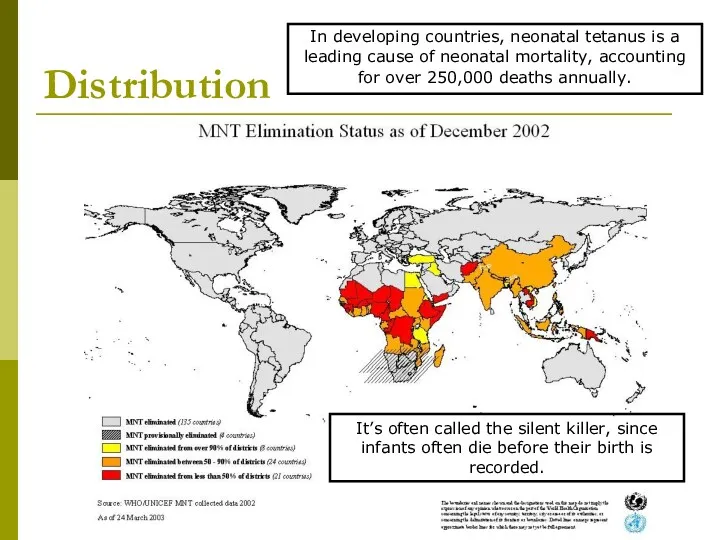
Distribution
In developing countries, neonatal tetanus is a leading cause of
Distribution
In developing countries, neonatal tetanus is a leading cause of
1950
<5
5-14
15-24
25-39
40+
A sharp decrease after tetanus toxoid was introduced into routine childhood
1950
<5
5-14
15-24
25-39
40+
A sharp decrease after tetanus toxoid was introduced into routine childhood
Causative agent
Clostridium tetani
Left. Stained pus from a mixed anaerobic infection.
Causative agent
Clostridium tetani
Left. Stained pus from a mixed anaerobic infection.
Morphology & Physiology
Relatively large, Gram-positive, rod-shaped bacteria
Spore-forming, anaerobic.
Found in soil, especially
Morphology & Physiology
Relatively large, Gram-positive, rod-shaped bacteria
Spore-forming, anaerobic.
Found in soil, especially
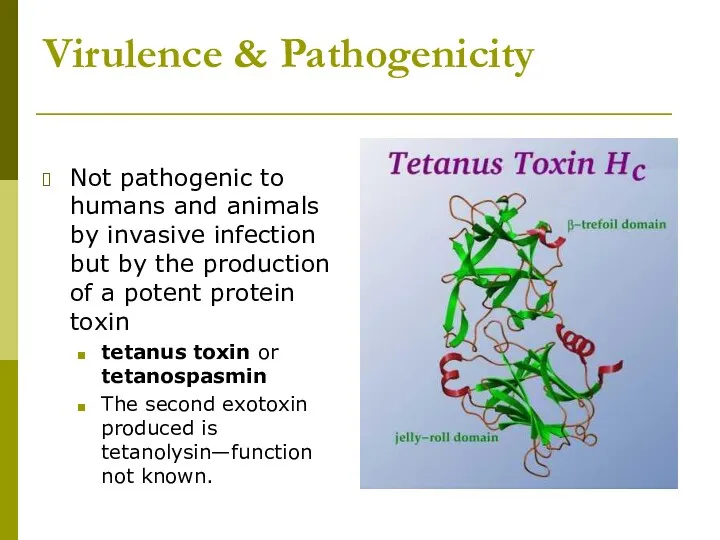
Virulence & Pathogenicity
Not pathogenic to humans and animals by invasive infection
Virulence & Pathogenicity
Not pathogenic to humans and animals by invasive infection
Tetanus toxin
Produced when spores germinate and vegetative cells grow after gaining
Tetanus toxin
Produced when spores germinate and vegetative cells grow after gaining
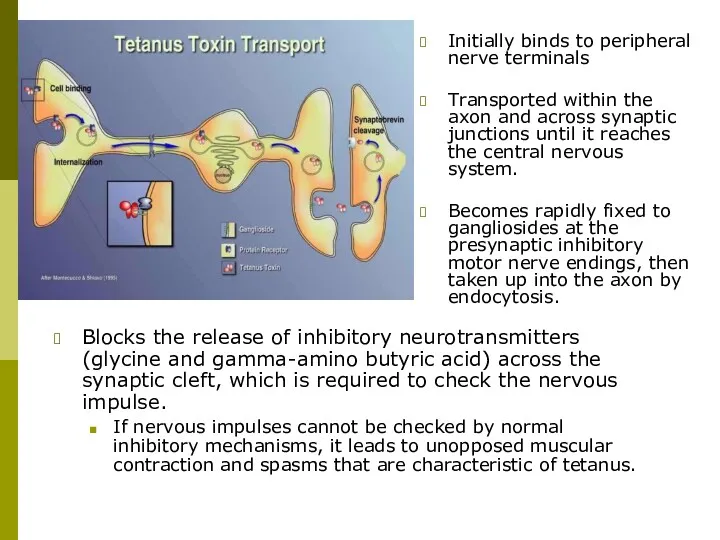
Initially binds to peripheral nerve terminals
Transported within the axon and across
Initially binds to peripheral nerve terminals
Transported within the axon and across
Methods of transmission
C. tetani can live for years as spores in
Methods of transmission
C. tetani can live for years as spores in
Symptoms
Tetanic seizures (painful, powerful bursts of muscle contraction)
if the muscle
Symptoms
Tetanic seizures (painful, powerful bursts of muscle contraction)
if the muscle
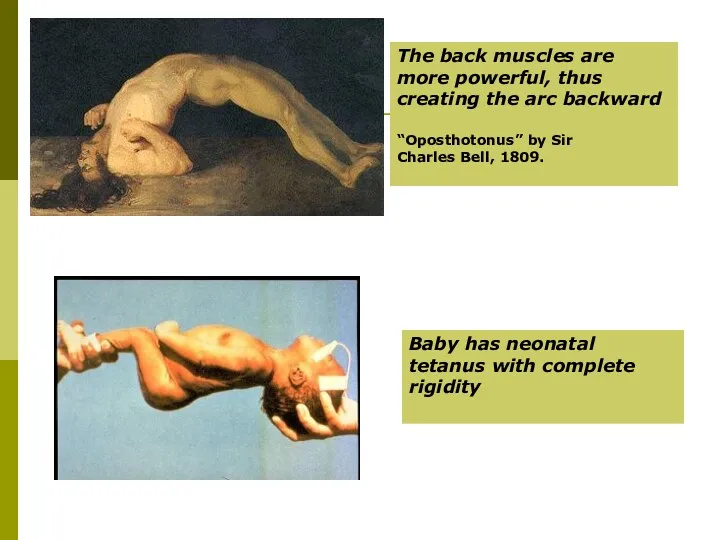
The back muscles are more powerful, thus creating the arc backward
The back muscles are more powerful, thus creating the arc backward
Types of tetanus:
local, cephalic, generalized, neonatal
Incubation period: 3-21 days, average
Types of tetanus:
local, cephalic, generalized, neonatal
Incubation period: 3-21 days, average
Most common types:
Generalized tetanus
descending pattern: lockjaw ? stiffness of
Most common types:
Generalized tetanus
descending pattern: lockjaw ? stiffness of
Methods of diagnosis
Based on the patient’s account and physical findings that
Methods of diagnosis
Based on the patient’s account and physical findings that
Clinical treatment
If treatment is not sought early, the disease is often
Clinical treatment
If treatment is not sought early, the disease is often
Method of prevention - immunization
A person recovering from tetanus should begin
Method of prevention - immunization
A person recovering from tetanus should begin
What else can be done?
Remove and destroy the source of the
What else can be done?
Remove and destroy the source of the
 Геморрагический васкулит
Геморрагический васкулит Гипертонический криз
Гипертонический криз Кіші жас балалардығы жедел аппендицттің ағымының ерекшелігі
Кіші жас балалардығы жедел аппендицттің ағымының ерекшелігі Физикалық қауіпті және зиянды өндірістік факторлар
Физикалық қауіпті және зиянды өндірістік факторлар Оценка собственного физического развития
Оценка собственного физического развития Гигиеническая оценка микроклимата помещения
Гигиеническая оценка микроклимата помещения Механическая желтуха
Механическая желтуха Питание и беременность
Питание и беременность Абсцессы и флегмоны скуловой области
Абсцессы и флегмоны скуловой области Эфференттік иннервацияға әсер ететін заттар. Холинергиялық заттар. Адренергиялық заттар
Эфференттік иннервацияға әсер ететін заттар. Холинергиялық заттар. Адренергиялық заттар Ведение беременности и родов при синдроме портальной гипертензии
Ведение беременности и родов при синдроме портальной гипертензии Лейкоз ауруы кезіндегі зертханалық әдістер
Лейкоз ауруы кезіндегі зертханалық әдістер A clinical case of Renal cell carcinoma
A clinical case of Renal cell carcinoma Сведения о медицинской организации. Форма № 30
Сведения о медицинской организации. Форма № 30 Ризикована поведінка
Ризикована поведінка История неврологии
История неврологии Гепатомегалия и гепатолиенальный синдром. Лечение хронических гепатитов, циррозов печени
Гепатомегалия и гепатолиенальный синдром. Лечение хронических гепатитов, циррозов печени 20231213_9klass_immunitet
20231213_9klass_immunitet Болезнь Лайма
Болезнь Лайма Менингококковая инфекция
Менингококковая инфекция Массаж при нарушениях развития центральной нервной системы. ДЦП
Массаж при нарушениях развития центральной нервной системы. ДЦП Элементы возрастной психологии и их учет в деятельности врача
Элементы возрастной психологии и их учет в деятельности врача Десмургия
Десмургия Жарақат және жарақат түрлері
Жарақат және жарақат түрлері Организация инфекционного контроля и инфекционной безопасности пациентов и медперсонала на примере отделения терапевтического
Организация инфекционного контроля и инфекционной безопасности пациентов и медперсонала на примере отделения терапевтического История болезни: множественная миома матки. Полип эндометрия
История болезни: множественная миома матки. Полип эндометрия Балаларда ас корыту жуйесі бұзылыстарының семиотикасы мен синдромдары
Балаларда ас корыту жуйесі бұзылыстарының семиотикасы мен синдромдары Суд над наркотиками
Суд над наркотиками