- The Heart

Содержание
- 2. Imaging of the heart will be considered under the following headings: 1. Simple x-ray 2. Screening
- 3. Simple x-ray A simple x-ray of the chest is mandatory as the first imaging investigation in
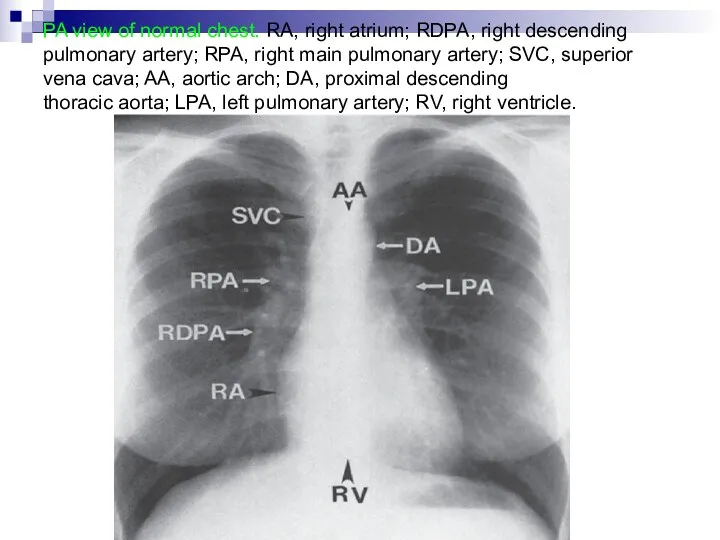
- 4. PA view of normal chest. RA, right atrium; RDPA, right descending pulmonary artery; RPA, right main
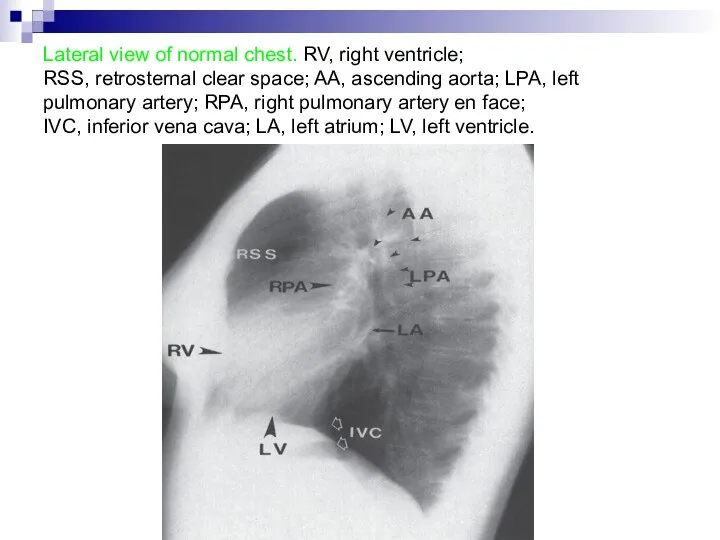
- 5. Lateral view of normal chest. RV, right ventricle; RSS, retrosternal clear space; AA, ascending aorta; LPA,
- 6. Screening Cardiac calcification is seen at screening with an image intensifier than on a simple film.
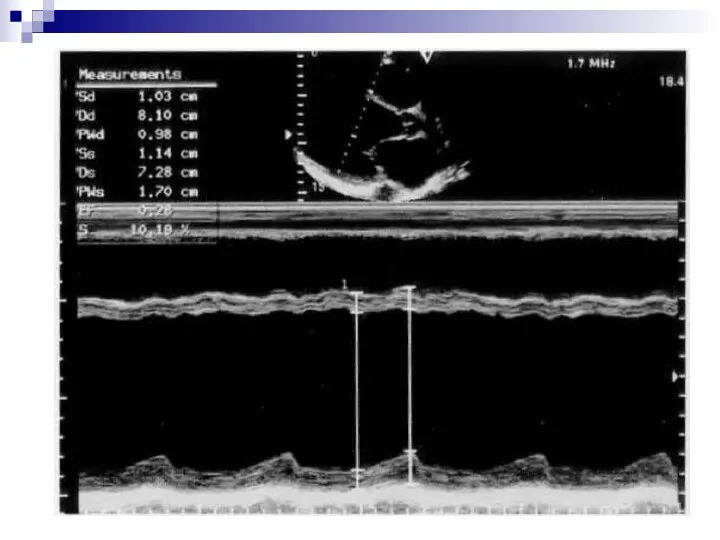
- 7. Echocardiography 1. Echocardiography is a highly versatile technique, which is central in cardiological diagnosis but is
- 8. 3. Patient is positioned in a 45 degree semierect position rotated towards his/her left side to
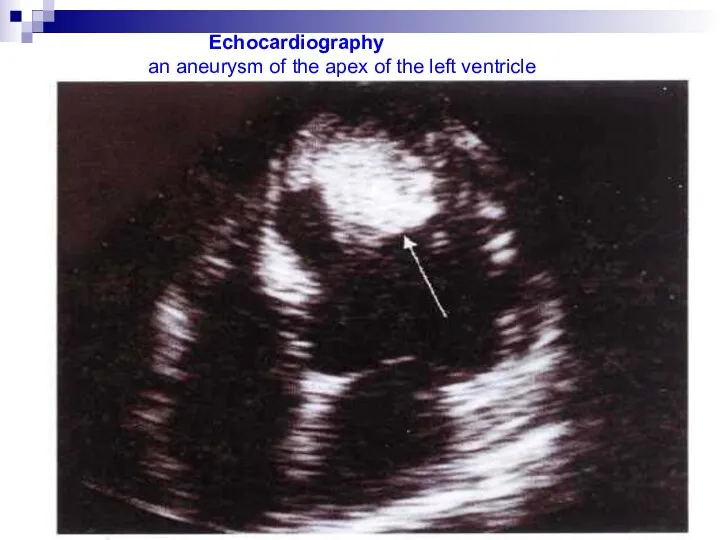
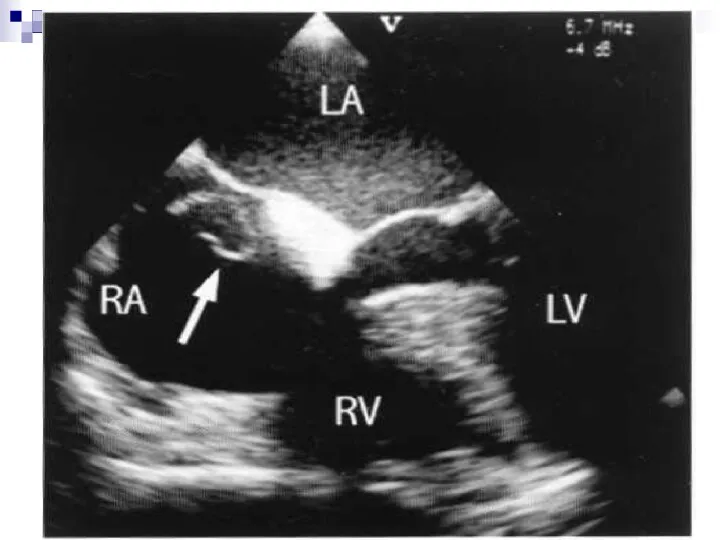
- 9. Echocardiography an aneurysm of the apex of the left ventricle
- 11. Apical four-chamber transthoracic echocardiogram in a patient with hypertrophic cardiomyopathy.
- 13. Doppler examination Doppler evaluation allows the study 1. of different flow velocities within the cardiac chambers
- 14. Apical continuous-wave Doppler trace in a patient with dynamic left ventricular outflow tract obstruction due to
- 15. Cardiac catheterization This procedure requires the introduction of a catheter into the heart and manipulation of
- 16. Right heart catheterization This can be performed percutaneously or after surgical exposure of a vein in
- 17. The site of the catheter tip can be confirmed by taking pressure recordings during the investigation
- 18. Left heart catheterization The usual technique of left heart catheterization is for the radiologist to introduce
- 19. Isotope scanning Technetium-99m pyrophosphate accumulates in damaged myocardium whereas thallium-201 produces a deficient uptake in territories
- 20. demonstrates a partially reversible perfusion defect in th interventricular septum and posterior wall of the left
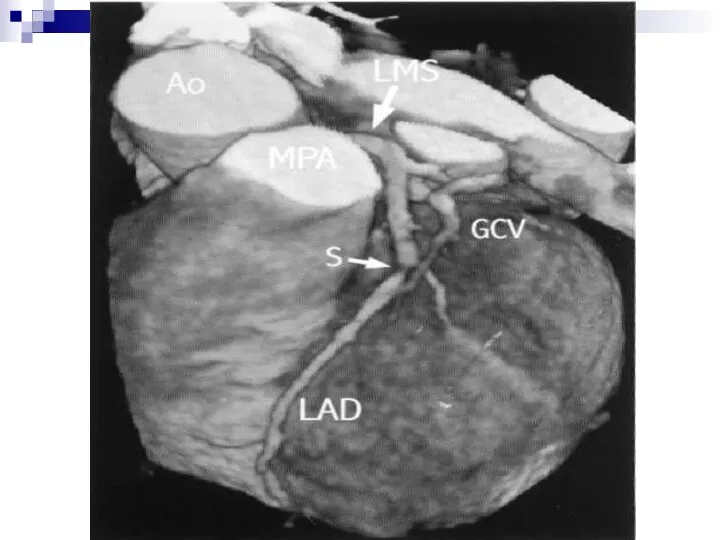
- 21. CT scan CT evaluation of the heart is useful for detecting: 1. the atherosclerotic disease of
- 22. Axial composite image
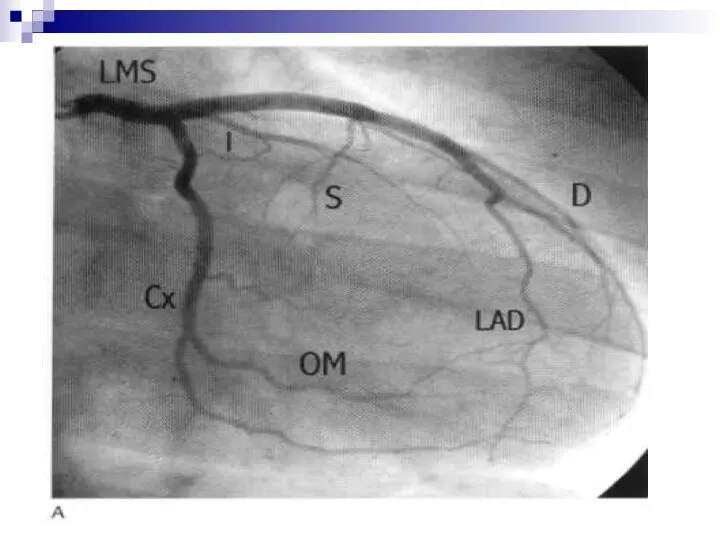
- 24. Arteriography Vascular access is usually obtained using a percutaneous approach via the femoral artery. Any major
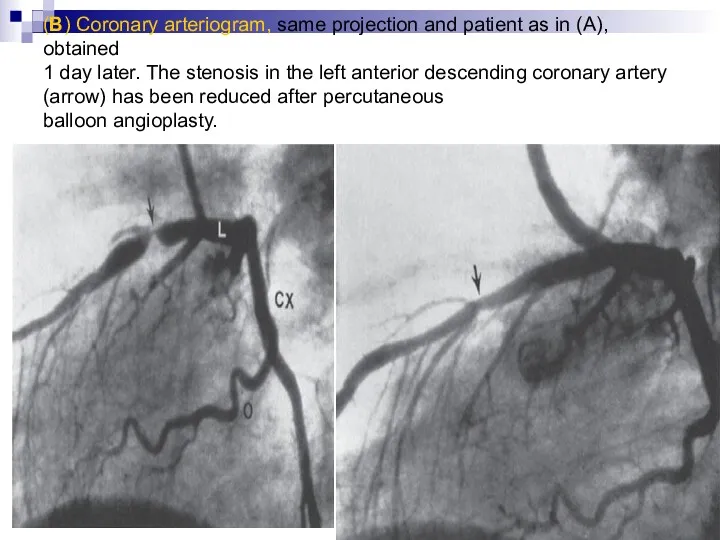
- 26. (B) Coronary arteriogram, same projection and patient as in (A), obtained 1 day later. The stenosis
- 27. Normal aortogram of transverse arch in patient suspected of having traumatic aortic injury. (B)Aortogram in a
- 28. Intravenous digital subtraction angiography This technique is utilized to visualize the arterial system by injection of
- 29. MRI MRI is fast gaining popularity as the investigation of choice in most cardiac pathologies. Assessment
- 30. Perfusion scanning gives the estimation of the surviving and infracted myocardium following myocardial infarction. Cardiac tumors
- 31. MRI image
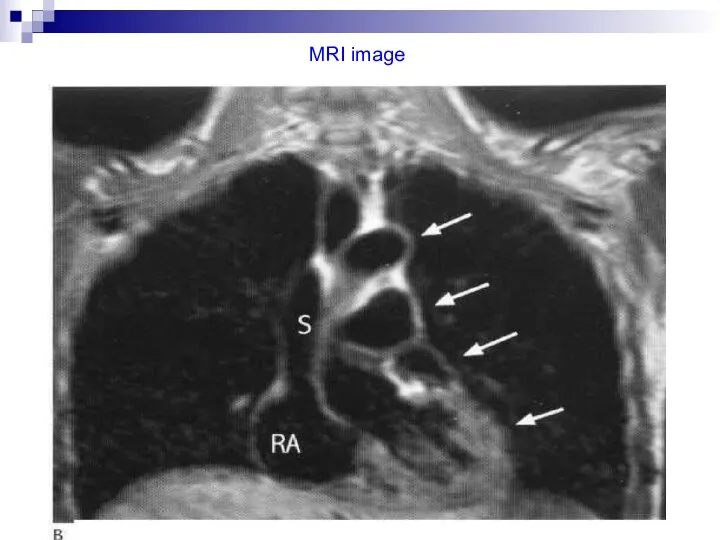
- 32. MRI image
- 33. MRI image
- 34. Cardiac pulsation Normally, pulsation on the left border is much more prominent than on the right
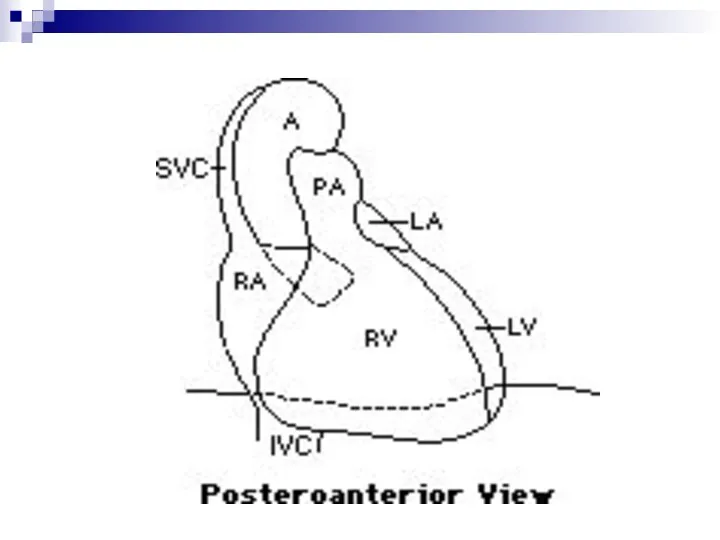
- 35. Posterioanterior Projection the upper right border is formed by: 1. the SVC 2. the lower cardiac
- 36. the left border has three well-defined segments: 1. the uppermost is formed by the aortic arch
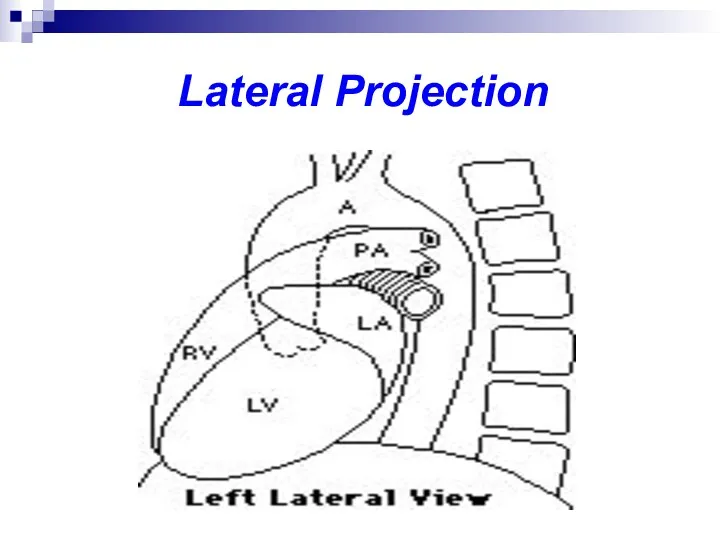
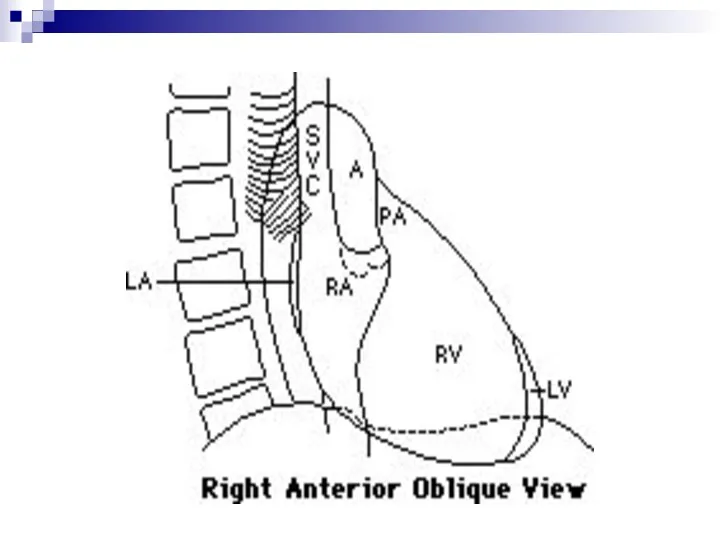
- 38. Lateral Projection
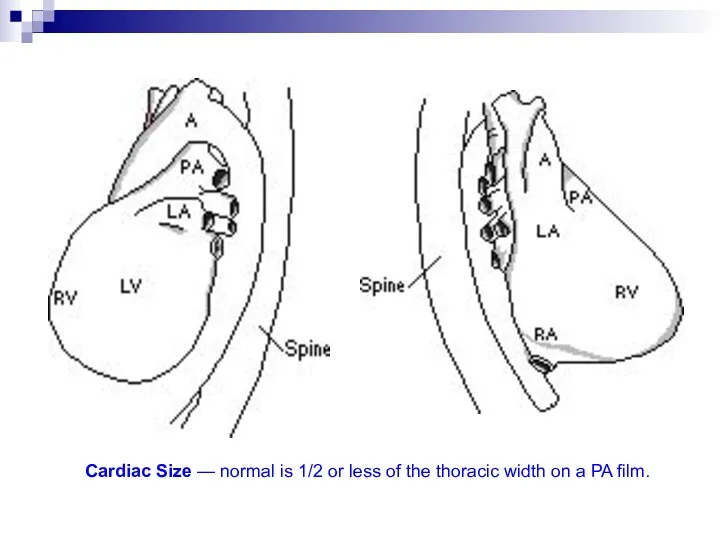
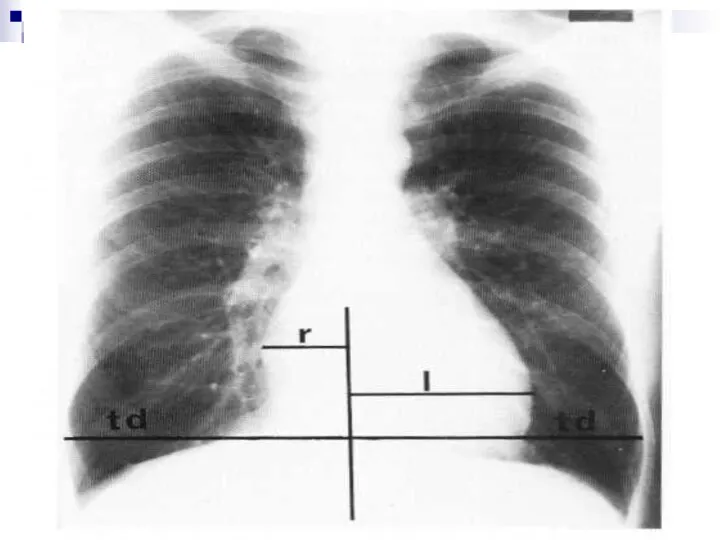
- 41. Cardiac Size — normal is 1/2 or less of the thoracic width on a PA film.
- 42. Technical Factors • The heart appears larger on AP than PA views. • Film during expiration
- 43. Cardiothoracic ratio (CT) It is a simple method of estimating cardiac enlargement. Estimation of CT ratio
- 45. The causes for increased CT ratio due to nonstandard radiographic techniques include: poor inspiration supine position
- 46. Expiratory phase on a PA radiograph. Note the low lung volumes, apparent enlargement of the cardiac
- 47. AP (A) and PA (B) radiographs of the chest in same patient on same day. Note
- 48. Common causes of cardiomegaly Valvular heart diseases like mitral stenosis, mitral regurgitation, aortic regurgitation Pericardial diseases
- 49. Causes of small heart constrictive pericarditis Addison’s disease Pulmonary emphysema
- 50. Enlargement of the heart It may be general, involving all chambers or eccentric involving one or
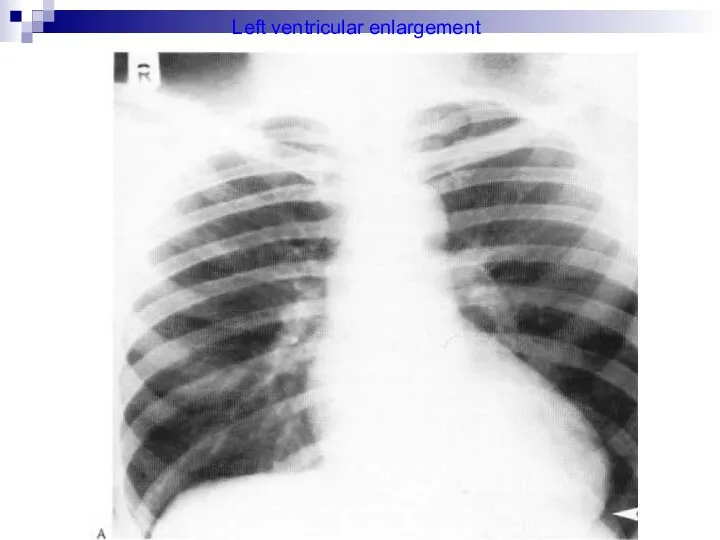
- 51. The common causes of the left ventricular enlargement are: hypertension aortic regurgitation aortic stenosis coronary arteriosclerosis
- 52. The left ventricle enlarges to the left and posteriorly and only slightly to the right and
- 53. Left ventricular enlargement
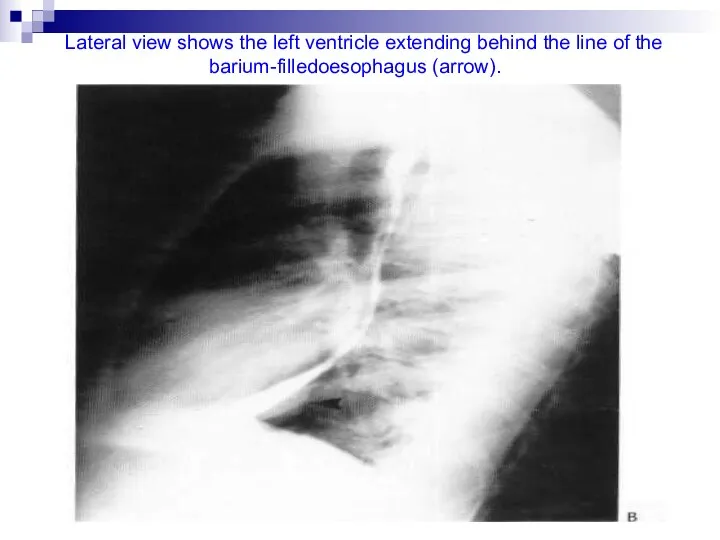
- 54. Lateral view shows the left ventricle extending behind the line of the barium-filledoesophagus (arrow).
- 55. The common causes of right ventricle enlargement are: mitral stenosis congestive failure chronic pulmonary diseases tricuspid
- 56. Right ventricle when enlarges, it does so by a broadening of its triangular shape. It enlarges
- 57. Direct signs of right ventricular enlargement are: upward and outward displacement of the ventricular border elevation
- 58. Indirect signs are: prominent right atrial border dilated pulmonary trunk signs of pulmonary hypertension
- 59. Gross right ventricular enlargement
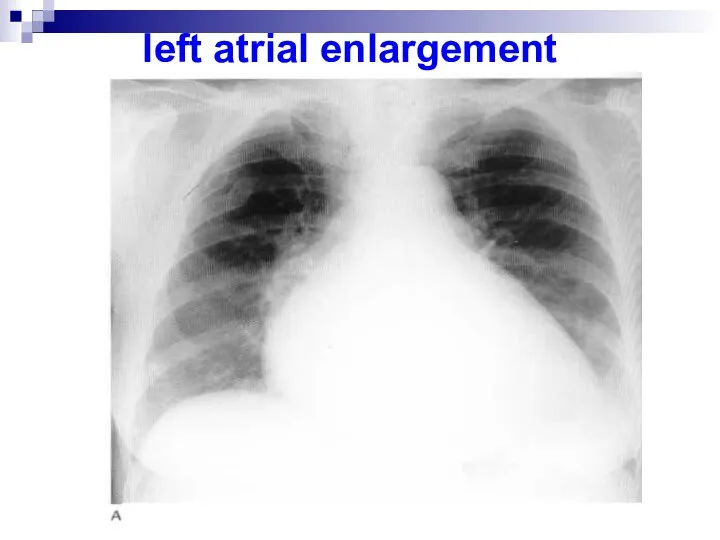
- 60. The common causes of left atrial enlargement are: ischemic heart disease mitral stenosis mitral regurgitation aortic
- 61. On the anterior view the right atrium forms less than the lower half to the right
- 62. left atrial enlargement
- 63. The causes of the right atrium enlargement are: Shunts into right atrium (left ventricular – right
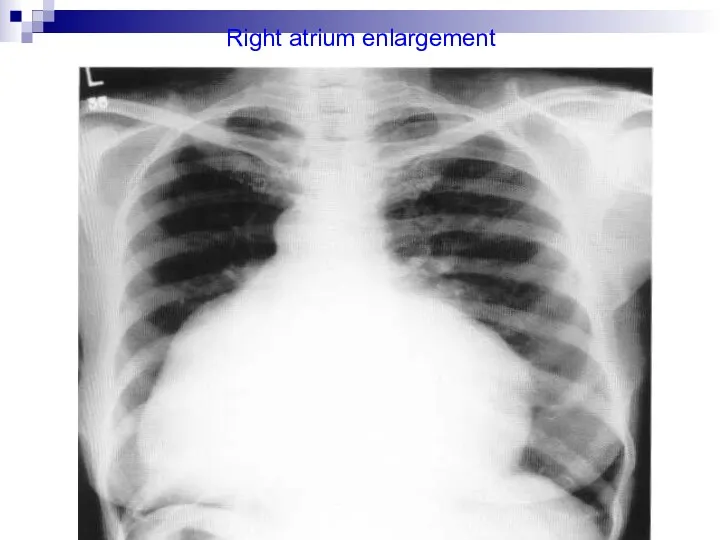
- 64. Right atrium enlargement
- 65. Essential hypertension It is a common cause of cardiac enlargement. In most cases there is unfolding
- 66. Left heart enlargement is common in prolonged hypertension. The apex lies below the dome of the
- 67. The pulmonary artery and the conus are somewhat dilated. The enlargement hazy outline of the hilar
- 68. Chronic nephritis The heart is enlarged in 80% cases. Marked rounding of the left ventricle is
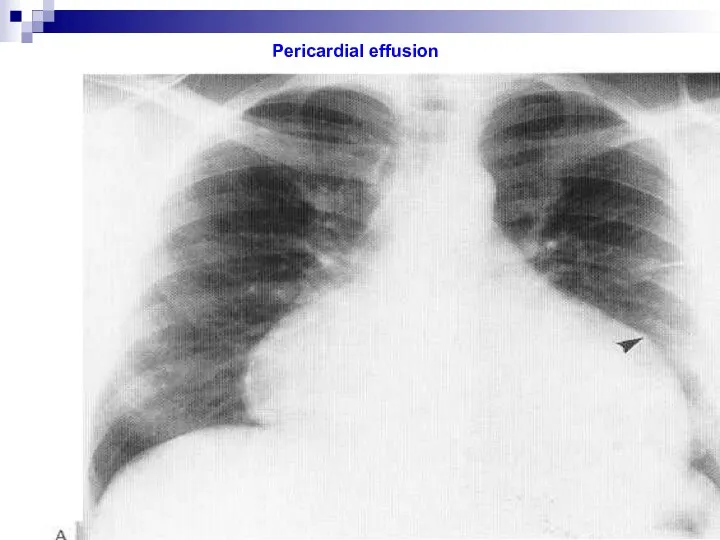
- 69. Pericardial effusion A pericardial effusion is a collection of fluid in the pericardial sac, the fluid
- 70. Radiological features Chest film: illustrates a symmetrically enlarges and globular cardiac shadow only when there is
- 71. CT: may also identify the aetiology, e.g. mediastinal malignancy. MRI: accurate for diagnosis and also images
- 72. Causes Infective viral bacterial tuberculosis Uraemia Posmyocardial infarction Myxoedema Malignancy bronchial and mediastinal tumors with pericardial
- 73. Pericardial effusion
- 74. Cardiac failure Cardiac failure is said to be present when tissue demands cannot be adequately supplied
- 75. Radiological features On a chest x-ray the following may be seen: cardiac enlargement upper-lobe vascular prominence:
- 76. interstitial pulmonary oedema: initially, prominence of the upper-lobe and narrowing of the lower-lobe vessels. As venous
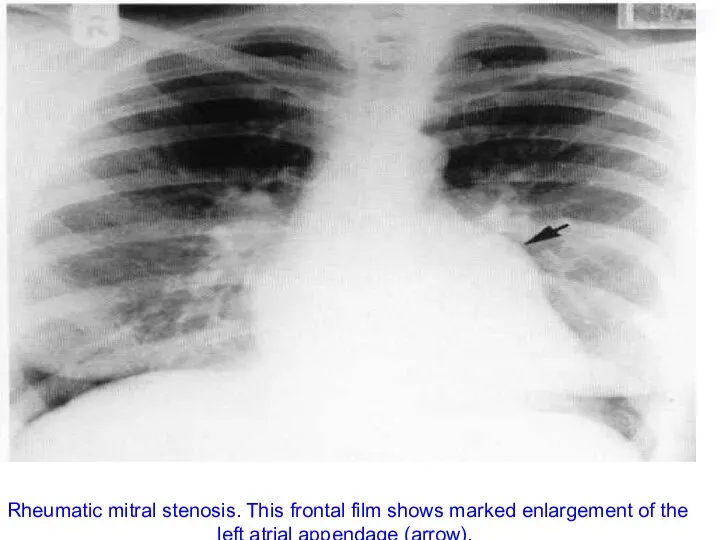
- 77. Valvular diseases of heart Mitral stenosis Mitral stenosis presenting in infancy or early childhood is due
- 78. In posterioanterior view An enlarged left auricle is seen as dense pear-shaped opacity lying transversely inside
- 79. In right oblique view The enlargement left auricle bulges backwards and obliterates the translucent retrocardiac space.
- 80. Elevation of left main bronchus due to enlarged left atrium may be seen. Horizontally Kerley “B”
- 81. Rheumatic mitral stenosis. This frontal film shows marked enlargement of the left atrial appendage (arrow).
- 82. Mitral regurgitation Mitral incompetence may result from functional or anatomical disturbance of the cusps. Familial cases
- 83. In mild regurgitation heart size may remain normal. In late cases, moderate cardiac enlargement suggests left
- 84. Aortic valve stenosis In ninety percent it is congenital in origin. Heart is never more than
- 85. Aortic regurgitation Congenital regurgitation is usually due to bicuspid valve whose cusps elongates or lack support.
- 86. * The ventricle enlarges mainly downwards and many cause no increase in transverse diameter. * A
- 87. Coarctation of aorta It is a congenital narrowing of the aortic lumen in the region of
- 88. X-ray shows: * enlargement of heart in the early weeks after birth and become very large
- 89. Pulmonary stenosis Pulmonary valve stenosis is always congenital. The heart is usually normal in size with
- 90. Pulmonary regurgitation It may be: congenital acquired functional
- 91. Isolated pulmonary regurgitation is a benign lesion unless associated with pulmonary hypertension. The heart and pulmonary
- 92. Venous hypertension When there is an increase in resistance to flow beyond the pulmonary capillaries, pressure
- 93. When the capillary pressure exceeds the normal plasma osmotic pressure to 25 mmHg fluid including fibrin
- 94. Deep septal lines are caused by edema of deep tissue probably around the lymphatics. One of
- 95. In hilar edema, fluid collects in the loose connective tissue. The outline of the vessels becomes
- 96. When the pulmonary venous pressure reaches 30 mmHg, edema fluid may be no longer contained within
- 97. Pulmonary hemosiderosis is due to focal deposition of hemosiderin. The lung show diffuse mottling in all
- 98. Fallot’s tetralogy Consists of: ventricular septal defect right ventricular outflow tract obstruction pulmonary stenosis right ventricular
- 99. Plain radiograph features: the heart is usually is not enlarged at birth but may enlarge later
- 101. Ventricular septal defect is abnormal opening between the two ventricles. Types: membranous muscular
- 102. Chest radiograph: left atrium is enlarged associated hypertrophy of right ventricle and left ventricle increased pulmonary
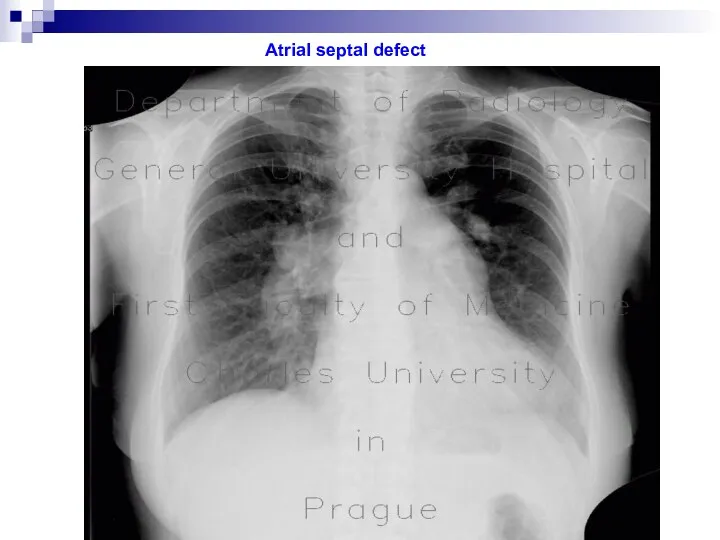
- 103. Atrial septal defect Atrial septal defect is the abnormal communication between the right and the left
- 104. Chest radiograph: enlargement of right atrium and right ventricle pulmonary vascular prominence in lung field (plethora)
- 105. Atrial septal defect
- 106. Cardiac tumors metastasis from bronchogenic carcinoma, mediastinal tumors, melanoma, and lymphoma are the most common malignant
- 108. Скачать презентацию
Imaging of the heart will be considered under the following
Imaging of the heart will be considered under the following
Simple x-ray
A simple x-ray of the chest is mandatory
Simple x-ray
A simple x-ray of the chest is mandatory
PA view of normal chest. RA, right atrium; RDPA, right descending
pulmonary
PA view of normal chest. RA, right atrium; RDPA, right descending pulmonary
Lateral view of normal chest. RV, right ventricle;
RSS, retrosternal clear space;
Lateral view of normal chest. RV, right ventricle; RSS, retrosternal clear space;
Screening
Cardiac calcification is seen at screening with an image
Screening
Cardiac calcification is seen at screening with an image
Echocardiography
1. Echocardiography is a highly versatile technique, which is central
Echocardiography
1. Echocardiography is a highly versatile technique, which is central
3. Patient is positioned in a 45 degree semierect position rotated
3. Patient is positioned in a 45 degree semierect position rotated
Echocardiography
an aneurysm of the apex of the left ventricle
Echocardiography
an aneurysm of the apex of the left ventricle
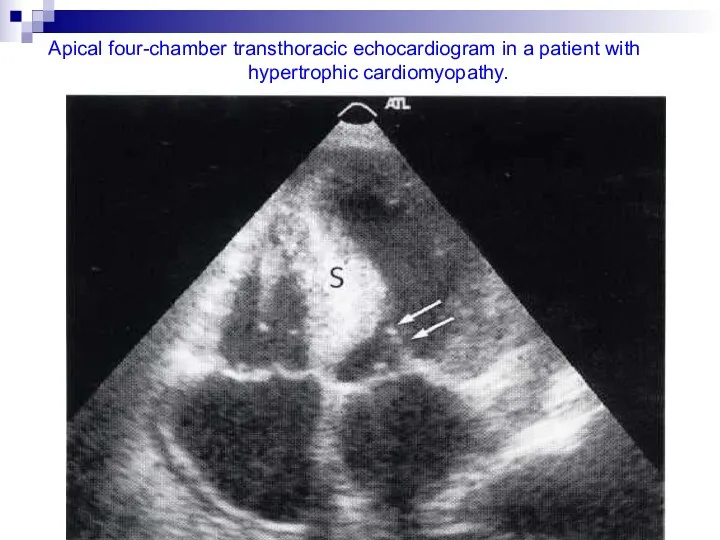
Apical four-chamber transthoracic echocardiogram in a patient with hypertrophic cardiomyopathy.
Apical four-chamber transthoracic echocardiogram in a patient with hypertrophic cardiomyopathy.
Doppler examination
Doppler evaluation allows the study
1. of different
Doppler examination
Doppler evaluation allows the study
1. of different
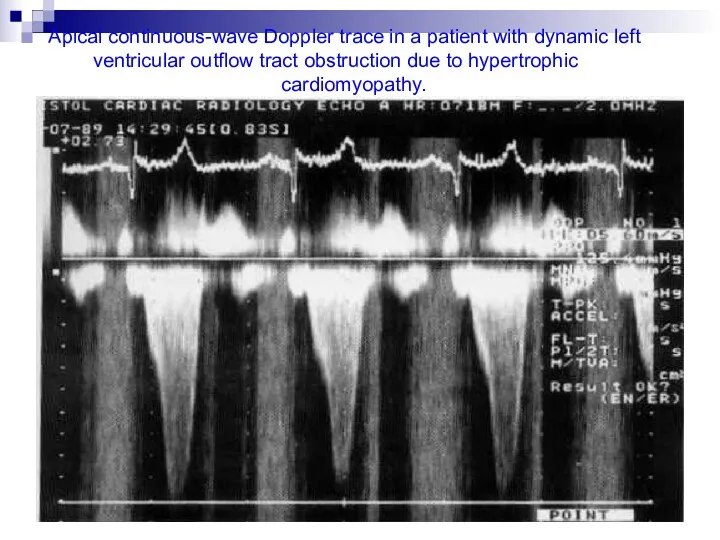
Apical continuous-wave Doppler trace in a patient with dynamic left
Apical continuous-wave Doppler trace in a patient with dynamic left
Cardiac catheterization
This procedure requires the introduction of a catheter into
Cardiac catheterization
This procedure requires the introduction of a catheter into
Right heart catheterization
This can be performed percutaneously or after surgical
Right heart catheterization
This can be performed percutaneously or after surgical
The site of the catheter tip can be confirmed by taking
The site of the catheter tip can be confirmed by taking
Left heart catheterization
The usual technique of left heart catheterization is
Left heart catheterization
The usual technique of left heart catheterization is
Isotope scanning
Technetium-99m pyrophosphate accumulates in damaged myocardium whereas thallium-201 produces
Isotope scanning
Technetium-99m pyrophosphate accumulates in damaged myocardium whereas thallium-201 produces

demonstrates a partially reversible perfusion defect in th interventricular
septum and
demonstrates a partially reversible perfusion defect in th interventricular septum and
CT scan
CT evaluation of the heart is useful
CT scan
CT evaluation of the heart is useful
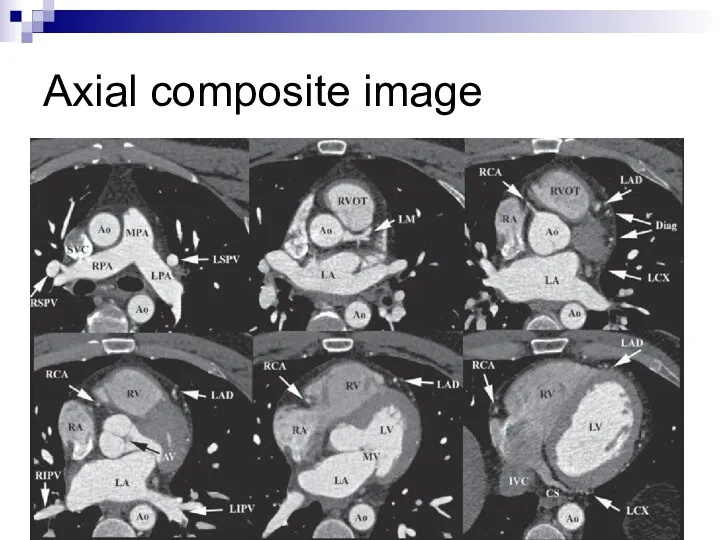
Axial composite image
Axial composite image
Arteriography
Vascular access is usually obtained using a percutaneous approach via
Arteriography
Vascular access is usually obtained using a percutaneous approach via
(B) Coronary arteriogram, same projection and patient as in (A), obtained
1
(B) Coronary arteriogram, same projection and patient as in (A), obtained 1
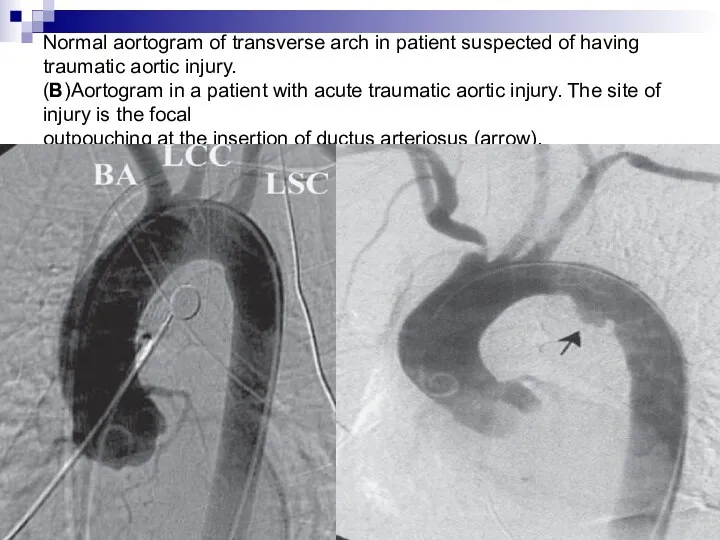
Normal aortogram of transverse arch in patient suspected of having traumatic
Normal aortogram of transverse arch in patient suspected of having traumatic
Intravenous digital subtraction angiography
This technique is utilized to visualize the
Intravenous digital subtraction angiography
This technique is utilized to visualize the
MRI
MRI is fast gaining popularity as the investigation of choice
MRI
MRI is fast gaining popularity as the investigation of choice
Perfusion scanning gives the estimation of the surviving and infracted myocardium
Perfusion scanning gives the estimation of the surviving and infracted myocardium
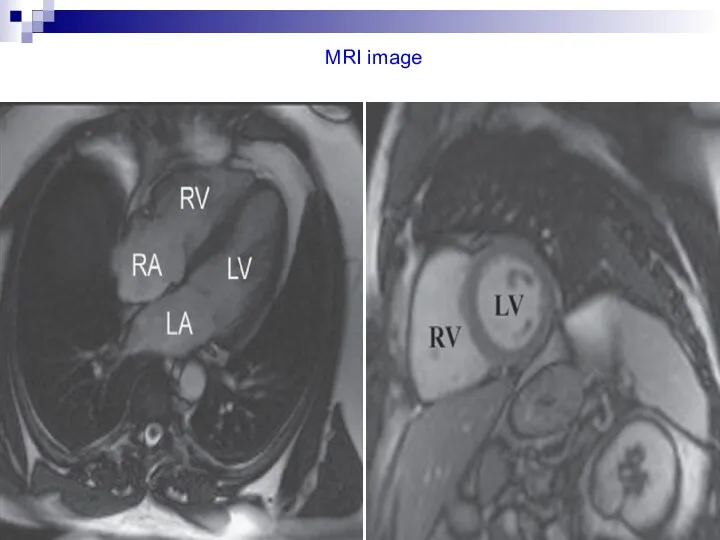
MRI image
MRI image

MRI image
MRI image
MRI image
MRI image
Cardiac pulsation
Normally, pulsation on the left border is much more
Cardiac pulsation
Normally, pulsation on the left border is much more
Posterioanterior Projection
the upper right border is formed by:
1. the
Posterioanterior Projection
the upper right border is formed by:
1. the
the left border has three well-defined segments:
1. the uppermost
the left border has three well-defined segments:
1. the uppermost
Lateral Projection
Lateral Projection
Cardiac Size — normal is 1/2 or less of the thoracic
Cardiac Size — normal is 1/2 or less of the thoracic
Technical Factors
• The heart appears larger on AP than PA
Technical Factors
• The heart appears larger on AP than PA
Cardiothoracic ratio (CT)
It is a simple method of estimating cardiac
Cardiothoracic ratio (CT)
It is a simple method of estimating cardiac
The causes for increased CT ratio due to nonstandard radiographic
The causes for increased CT ratio due to nonstandard radiographic

Expiratory phase on a PA radiograph. Note
the low lung volumes, apparent
Expiratory phase on a PA radiograph. Note the low lung volumes, apparent
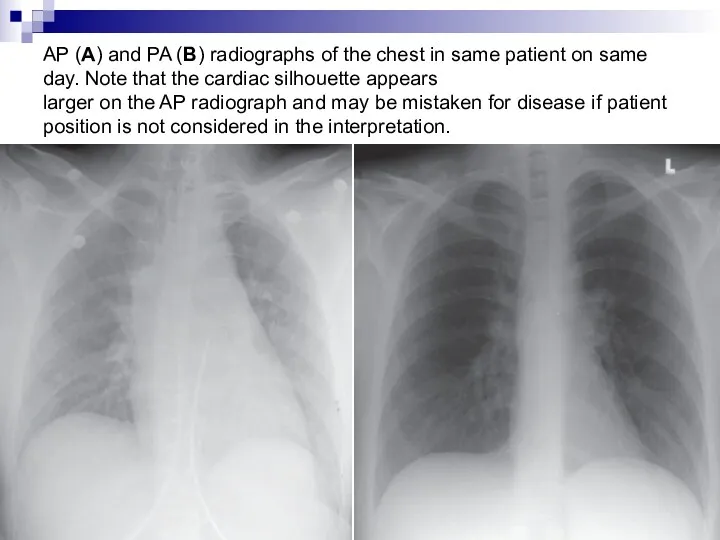
AP (A) and PA (B) radiographs of the chest in same
AP (A) and PA (B) radiographs of the chest in same
Common causes of cardiomegaly
Valvular heart diseases like mitral stenosis, mitral
Common causes of cardiomegaly
Valvular heart diseases like mitral stenosis, mitral
Causes of small heart
constrictive pericarditis
Addison’s disease
Pulmonary emphysema
Causes of small heart
constrictive pericarditis
Addison’s disease
Pulmonary emphysema
Enlargement of the heart
It may be general, involving all chambers
Enlargement of the heart
It may be general, involving all chambers
The common causes of the left ventricular enlargement are:
hypertension
aortic regurgitation
aortic
The common causes of the left ventricular enlargement are:
hypertension
aortic regurgitation
aortic
The left ventricle enlarges to the left and posteriorly and only
The left ventricle enlarges to the left and posteriorly and only
Left ventricular enlargement
Left ventricular enlargement
Lateral view shows the left ventricle extending behind the line
Lateral view shows the left ventricle extending behind the line
The common causes of right ventricle enlargement are:
mitral stenosis
congestive failure
chronic
The common causes of right ventricle enlargement are:
mitral stenosis
congestive failure
chronic
Right ventricle when enlarges, it does so by a broadening of
Right ventricle when enlarges, it does so by a broadening of
Direct signs of right ventricular enlargement are:
upward and outward
Direct signs of right ventricular enlargement are:
upward and outward
Indirect signs are:
prominent right atrial border
dilated pulmonary trunk
signs of pulmonary
Indirect signs are:
prominent right atrial border
dilated pulmonary trunk
signs of pulmonary
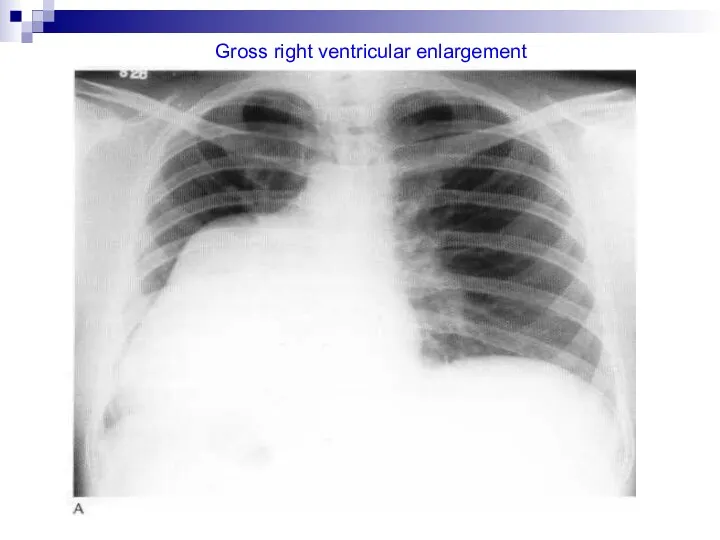
Gross right ventricular enlargement
Gross right ventricular enlargement
The common causes of left atrial
enlargement are:
ischemic heart disease
mitral
The common causes of left atrial
enlargement are:
ischemic heart disease
mitral
On the anterior view the right atrium forms less than the
On the anterior view the right atrium forms less than the
left atrial enlargement
left atrial enlargement
The causes of the right atrium enlargement are:
Shunts into right
The causes of the right atrium enlargement are:
Shunts into right
Right atrium enlargement
Right atrium enlargement
Essential hypertension
It is a common cause of cardiac enlargement.
Essential hypertension
It is a common cause of cardiac enlargement.
Left heart enlargement is common in prolonged hypertension.
The apex lies
Left heart enlargement is common in prolonged hypertension.
The apex lies
The pulmonary artery and the conus are somewhat dilated.
The enlargement
The pulmonary artery and the conus are somewhat dilated.
The enlargement
Chronic nephritis
The heart is enlarged in 80% cases. Marked rounding
Chronic nephritis
The heart is enlarged in 80% cases. Marked rounding
Pericardial effusion
A pericardial effusion is a collection of fluid in
Pericardial effusion
A pericardial effusion is a collection of fluid in
Radiological features
Chest film: illustrates a symmetrically enlarges and globular
Radiological features
Chest film: illustrates a symmetrically enlarges and globular
CT: may also identify the aetiology, e.g. mediastinal malignancy.
MRI: accurate for
CT: may also identify the aetiology, e.g. mediastinal malignancy.
MRI: accurate for
Causes
Infective
viral
bacterial
tuberculosis
Uraemia
Posmyocardial infarction
Myxoedema
Malignancy
bronchial and mediastinal tumors with pericardial invasion
Collagen vascular
Causes
Infective
viral
bacterial
tuberculosis
Uraemia
Posmyocardial infarction
Myxoedema
Malignancy
bronchial and mediastinal tumors with pericardial invasion
Collagen vascular
Pericardial effusion
Pericardial effusion
Cardiac failure
Cardiac failure is said to be present when tissue
Cardiac failure
Cardiac failure is said to be present when tissue
Radiological features
On a chest x-ray the following may be
Radiological features
On a chest x-ray the following may be
interstitial pulmonary oedema: initially, prominence of the upper-lobe and narrowing of
interstitial pulmonary oedema: initially, prominence of the upper-lobe and narrowing of
Valvular diseases of heart
Mitral stenosis
Mitral stenosis presenting in infancy
Valvular diseases of heart
Mitral stenosis
Mitral stenosis presenting in infancy
In posterioanterior view
An enlarged left auricle is seen as dense
In posterioanterior view
An enlarged left auricle is seen as dense
In right oblique view
The enlargement left auricle bulges backwards
In right oblique view
The enlargement left auricle bulges backwards
Elevation of left main bronchus due to enlarged left atrium may
Elevation of left main bronchus due to enlarged left atrium may
Rheumatic mitral stenosis. This frontal film shows marked enlargement of
Rheumatic mitral stenosis. This frontal film shows marked enlargement of
Mitral regurgitation
Mitral incompetence may result from functional or anatomical disturbance
Mitral regurgitation
Mitral incompetence may result from functional or anatomical disturbance
In mild regurgitation heart size may remain normal.
In late cases,
In mild regurgitation heart size may remain normal.
In late cases,
Aortic valve stenosis
In ninety percent it is congenital
Aortic valve stenosis
In ninety percent it is congenital
Aortic regurgitation
Congenital regurgitation is usually due to bicuspid valve whose
Aortic regurgitation
Congenital regurgitation is usually due to bicuspid valve whose
* The ventricle enlarges mainly downwards and many cause no increase
* The ventricle enlarges mainly downwards and many cause no increase
Coarctation of aorta
It is a congenital narrowing of the aortic
Coarctation of aorta
It is a congenital narrowing of the aortic
X-ray shows:
* enlargement of heart in the early weeks
X-ray shows:
* enlargement of heart in the early weeks
Pulmonary stenosis
Pulmonary valve stenosis is always congenital.
The heart
Pulmonary stenosis
Pulmonary valve stenosis is always congenital.
The heart
Pulmonary regurgitation
It may be:
congenital
acquired
functional
Pulmonary regurgitation
It may be:
congenital
acquired
functional
Isolated pulmonary regurgitation is a benign lesion unless associated with pulmonary
Isolated pulmonary regurgitation is a benign lesion unless associated with pulmonary
Venous hypertension
When there is an increase in resistance to flow
Venous hypertension
When there is an increase in resistance to flow
When the capillary pressure exceeds the normal plasma osmotic pressure to
When the capillary pressure exceeds the normal plasma osmotic pressure to
Deep septal lines are caused by edema of deep tissue probably
Deep septal lines are caused by edema of deep tissue probably
In hilar edema, fluid collects in the loose connective tissue. The
In hilar edema, fluid collects in the loose connective tissue. The
When the pulmonary venous pressure reaches 30 mmHg, edema fluid may
When the pulmonary venous pressure reaches 30 mmHg, edema fluid may
Pulmonary hemosiderosis is due to focal deposition of hemosiderin. The lung
Pulmonary hemosiderosis is due to focal deposition of hemosiderin. The lung
Fallot’s tetralogy
Consists of:
ventricular septal defect
right ventricular outflow tract obstruction
pulmonary stenosis
right
Fallot’s tetralogy
Consists of:
ventricular septal defect
right ventricular outflow tract obstruction
pulmonary stenosis
right
Plain radiograph features:
the heart is usually is not enlarged at
Plain radiograph features:
the heart is usually is not enlarged at
Ventricular septal defect
is abnormal opening between the two
Ventricular septal defect
is abnormal opening between the two
Chest radiograph:
left atrium is enlarged
associated hypertrophy of right ventricle and
Chest radiograph:
left atrium is enlarged
associated hypertrophy of right ventricle and
Atrial septal defect
Atrial septal defect is the abnormal communication
Atrial septal defect
Atrial septal defect is the abnormal communication
Chest radiograph:
enlargement of right atrium and right ventricle
pulmonary vascular prominence
Chest radiograph:
enlargement of right atrium and right ventricle
pulmonary vascular prominence
Atrial septal defect
Atrial septal defect
Cardiac tumors
metastasis from bronchogenic carcinoma, mediastinal tumors, melanoma, and lymphoma
Cardiac tumors
metastasis from bronchogenic carcinoma, mediastinal tumors, melanoma, and lymphoma
 Клиникалық жағдай
Клиникалық жағдай Артериальная гипертензия у детей. Неотложная терапия
Артериальная гипертензия у детей. Неотложная терапия Биохимия крови
Биохимия крови Апластические анемии
Апластические анемии Недостаточность митрального клапана
Недостаточность митрального клапана Жатыр мойны және денесінің обыры тақырыбына презентация
Жатыр мойны және денесінің обыры тақырыбына презентация Методы исследования жевательного аппарата
Методы исследования жевательного аппарата Диагностика отосклероза по данным МСКТ
Диагностика отосклероза по данным МСКТ Анатомически узкий таз
Анатомически узкий таз Дифференциальная диагностика болей в грудной клетке
Дифференциальная диагностика болей в грудной клетке Основы рационального питания. Физиолого-гигиеническая характеристика пищевых веществ
Основы рационального питания. Физиолого-гигиеническая характеристика пищевых веществ Мініінвазивна хірургія в комплексному лікуванні кіст підшлункової залози
Мініінвазивна хірургія в комплексному лікуванні кіст підшлункової залози Методы лучевой диагностики заболеваний мочевыделительной системы. Лучевая анатомия и семиотика
Методы лучевой диагностики заболеваний мочевыделительной системы. Лучевая анатомия и семиотика Нейроэндокринды синдромдар
Нейроэндокринды синдромдар Gmp – тиісті өндірістік тәжірибе
Gmp – тиісті өндірістік тәжірибе Острые лейкозы
Острые лейкозы Кардиотокография (КТГ)
Кардиотокография (КТГ) Нейроспид. История
Нейроспид. История Тісжегі қуысы туралы түсінік. Тісжегі қуыстарын егеп-тазалаудың негізгі қағидалары мен кезеңдері
Тісжегі қуысы туралы түсінік. Тісжегі қуыстарын егеп-тазалаудың негізгі қағидалары мен кезеңдері Синдром слабости синусового узла
Синдром слабости синусового узла Гинекологические заболевания у коров
Гинекологические заболевания у коров Шок. Гиповолемический и кардиогенный шок. Дифференциальная диагностика. Интенсивная терапия шока различной этиологии
Шок. Гиповолемический и кардиогенный шок. Дифференциальная диагностика. Интенсивная терапия шока различной этиологии Многоплодная беременность
Многоплодная беременность Термические и химические ожоги. Электротравма
Термические и химические ожоги. Электротравма Энцефалит клещевой
Энцефалит клещевой Наследственные болезни
Наследственные болезни Жан тазалығы, тән тазалығы
Жан тазалығы, тән тазалығы Физическая антисептика
Физическая антисептика