- Mood Disorders

Содержание
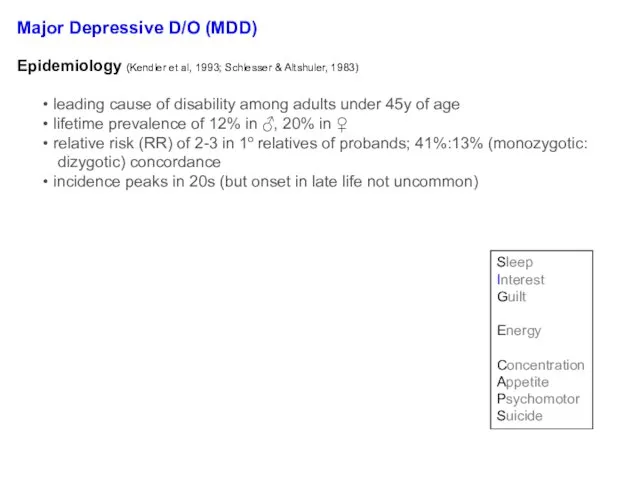
- 2. Objectives Mood, affect, mood disorders (mood D/O’s) Nosology, epidemiology, treatment (tx) of: Major depressive disorder (MDD)
- 3. Mood - The subjective sense indicates the long, deep and constant feeling that affects a person,
- 4. Mood - The subjective sense indicates the long, deep and constant feeling that affects a person,
- 5. Mood v. Affect “mood” a sustained emotional attitude typically garnered through pt self-report “affect” the way
- 6. Major Depressive Disorder
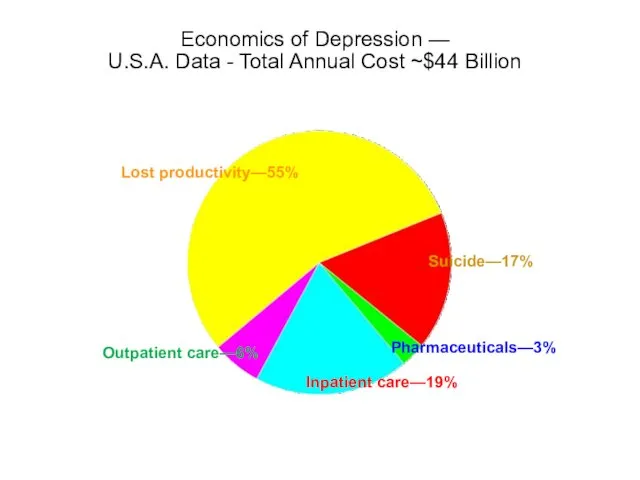
- 7. Economics of Depression — U.S.A. Data - Total Annual Cost ~$44 Billion 9 Lost productivity—55% Suicide—17%
- 8. Major Depressive D/O (MDD) Diagnosis req’s ≥1 major depressive episode (MDE) MDE = ≥2wks of signif
- 9. Question: When does a major depressive episode (MDE) ≠ Major Depressive Disorder?
- 10. Major Depressive D/O (MDD) EXCLUSIONS: not attributable to a substance/medication or another medical condition no prior
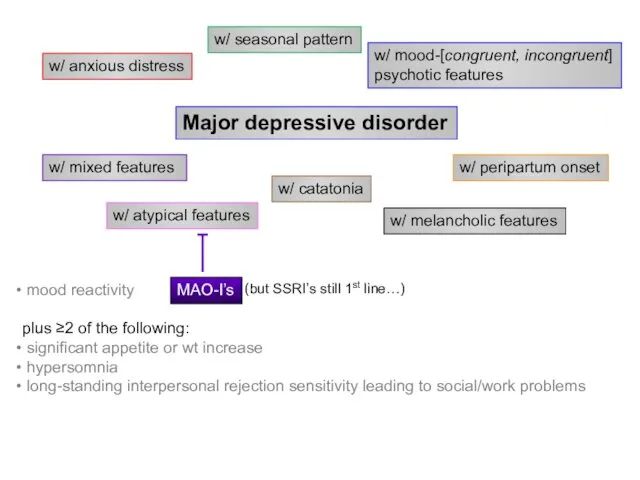
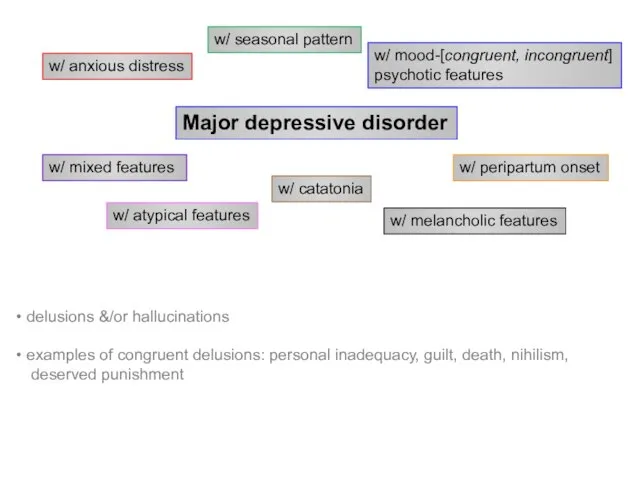
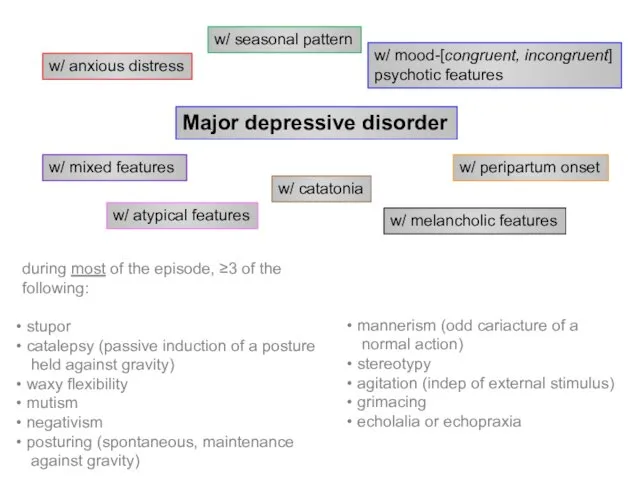
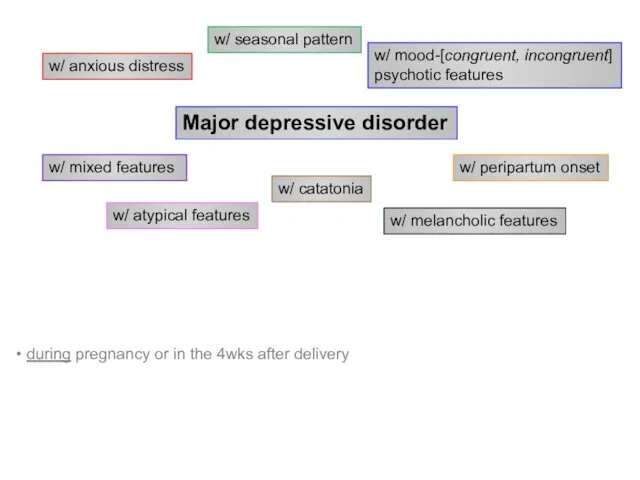
- 11. Major depressive disorder w/ anxious distress w/ mixed features w/ atypical features w/ melancholic features w/
- 12. Major depressive disorder w/ anxious distress w/ mixed features w/ atypical features w/ melancholic features w/
- 13. Major depressive disorder w/ anxious distress w/ mixed features w/ atypical features w/ melancholic features w/
- 14. Major depressive disorder w/ anxious distress w/ mixed features w/ atypical features w/ melancholic features w/
- 15. Major depressive disorder w/ anxious distress w/ mixed features w/ atypical features w/ melancholic features w/
- 16. Major depressive disorder w/ anxious distress w/ mixed features w/ atypical features w/ melancholic features w/
- 17. Major depressive disorder w/ anxious distress w/ mixed features w/ atypical features w/ melancholic features w/
- 18. Major depressive disorder w/ anxious distress w/ mixed features w/ atypical features w/ melancholic features w/
- 19. Belmaker RH and Agam G, NEJM 2008, 358:55-68 iproniazid (1957) imipramine (1959)
- 20. Question: Do antidepressants have additional actions besides inhibition of reuptake transporters? “…the Zoloft cartoon” from: http://gifsoup.com/webroot/animatedgifs/50426_o.gif;
- 21. Chronic antidepressant treatment increases neurogenesis in adult rat hippocampus. Malberg JE, Eisch AJ, Nestler EJ, Duman
- 22. Subsequent hypotheses about MDD altered glutamatergic transmission ↓’d GABAergic transmission monoamine-Ach imbalance disruption of endogenous opioid
- 23. Key brain areas involved in regulation of mood (A) Ventromedial prefrontal cortex (VMPFC)1 Modulates pain and
- 24. Key brain areas involved in regulation of mood (cont.) (A) Amygdala: regulates cortical arousal and neuroendocrine
- 25. Brain atrophy in depression? 1. Bremner JD, et al. Am J Psychiatry. 2000;157(1):115-118. 2. Images courtesy
- 26. Major Depression: Cognition Learned helplessness (Seligman) (Seligman & Maier, 1967) Attribution of lack of control over
- 27. Seligman & Beck Seligman Attributions are: Internal Stable Global I am inadequate (internal) at everything (global)
- 28. Cognitive theories Beck’s theory: 31 Character of pessimism (NegativeTriad) Habits of negativity (Negative schemas) Erroneous thinking
- 29. Characteristic biases Arbitrary inference Selective abstraction Overgeneralization Magnification and minimization 32
- 30. Behavioral theories Learned helplessness/hopelessness is a behavioral theory with a cognitive twist. Reduction in reinforcement leads
- 31. Availability of reinforcers The amount of reinforcement available is a function of Personal characteristics Environment or
- 32. Interpersonal theory Reduced interpersonal support Experiences of rejection Due to social structure Inadequate social networks Others
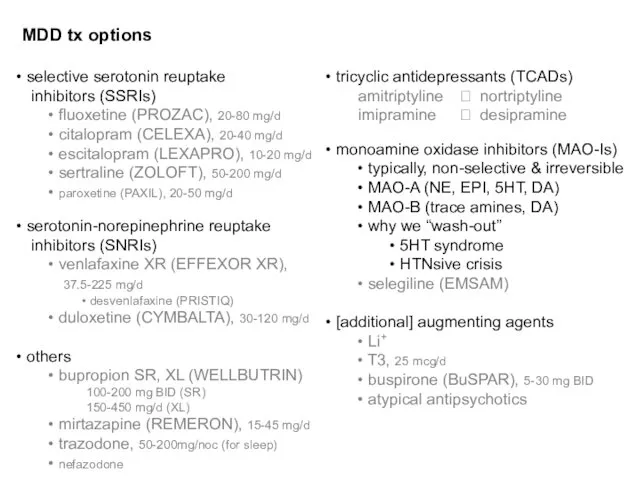
- 33. MDD tx options selective serotonin reuptake inhibitors (SSRIs) fluoxetine (PROZAC), 20-80 mg/d citalopram (CELEXA), 20-40 mg/d
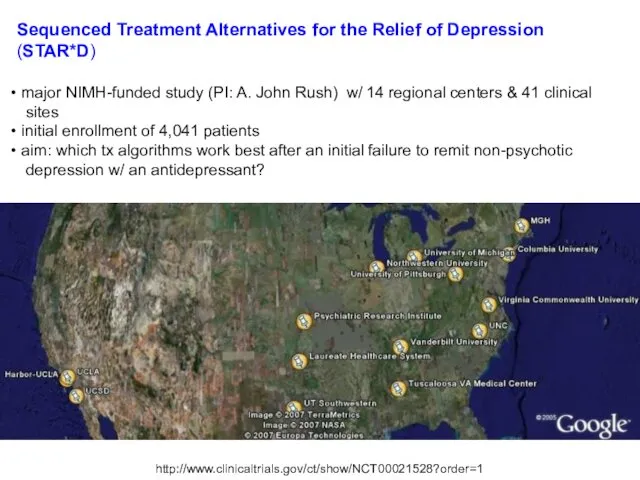
- 34. Sequenced Treatment Alternatives for the Relief of Depression (STAR*D) major NIMH-funded study (PI: A. John Rush)
- 35. Trivedi MH et al, Am J Psychiatry. 2006 Jan;163(1):28-40 47% response rate on citalopram (by *QIDS-SR,
- 36. MDD tx options Ψtherapy cognitive bx therapy (CBT) interpersonal therapy (IPT) psychodynamic therapy interventional Ψ electroconvulsive
- 37. Major Depressive D/O (MDD) NATURAL HISTORY (Frank E and Thase ME, 1999 & DSM-5) recovery usually
- 38. Kendler KS, et al. Am J Psychiatry. 2000;157(8):1243-1251. Number of Previous Depressive Episodes 10 Risk (Odds
- 39. Persistent depressive disorder (dysthymia) 2y of depressed mood (1y in children/adolescents) most of the day, more
- 40. Persistent depressive disorder (dysthymia) may be more treatment-resistant (TxR) than straightforward MDD EPIDEMIOLOGY lifetime prevalence =
- 41. Case 1. 36yo F presenting w/ 3mos of ↓mood. She reports getting only ~4h of sleep/noc
- 42. Premenstrual dysphoric d/o Criterion A. In most menstrual cycles, ≥5 sxs in the final week before
- 43. Premenstrual dysphoric d/o (M)ood (labile &/or irritable &/or anxious) Sleep Interest Body Energy Concentration Appetite Out
- 44. Disruptive mood dysregulation disorder *severe recurrent temper outbursts (verbal or behavior) grossly disproportionate to the situation
- 45. Bipolar disorder
- 46. Bipolar D/O (BD) Epidemiology Diagnostic criteria: BD I ≥ 1 manic episode MDE is neither sufficient
- 47. Bipolar D/O (BD) Manic episode: elevated mood & ≥1wk of at least 3 of the following
- 48. Bipolar Disorder (BD) EXCLUSIONS: another medical cause substance/medication causes SPECIFIERS: same as w/ MDD plus: rapid
- 49. Bipolar Disorder (BD) MORE on ‘w/ mixed features’… IF full criteria met for both poles, the
- 50. Case 1 - continued Prior hx to date: 36yo F w/ 3mos of depressed mood tx’d
- 51. Case 1 - continued Is manic switch a real concern? mood stabilizer = primarily Li+, VPA,
- 52. Biology of Bipolar D/O (BD) failure of linkage studies Janice Egeland – 2 decades of work
- 53. *’s 2 accompanying papers (same issue of Nature) unable to replicate chr11 assocn’s in independent pedigrees
- 54. Linkage studies 6q (LOD 4.19 narrow), 8q (LOD 3.40 broad) (still hold-up in meta-analyses – e.g.,
- 55. More on select GWA-identified candidates CACNA1C α1 subunit of a voltage-dependent Ca2+ channel per citations in
- 56. Bipolar Disorder (BD) – treatment The old standard: mood stabilizer + reuptake blocker Debunked: gabapentin (NEURONTIN)
- 57. John Cade. Ψist at a provincial hospital in Australia figured mania was 2/2 an abnormally secreted
- 58. Bipolar Disorder (BD) – treatment (cont’d) Li+ v. Depakote / valproate (VPA) (Bowden CL, 2001) Li+
- 59. Bipolar Disorder (BD) – treatment (cont’d) How many agents to use? combination tx often helpful in
- 60. Bipolar Disorder (BD) – natural history 60% of manic episodes immediately precede an MDE MDE’s usually
- 61. Cyclothymic D/O 2y of fluctuating mood (1y in children, adolescents) hypomanic symptoms (but NOT episodes) dysthymic
- 62. Differential diagnosis
- 63. Phenocopies and gray areas… Anxiety D/O’s (esp. GAD, PTSD) Schizoaffective D/O Delirium Dementia Personality D/O’s Substance/Medication-induced
- 64. Depressive, Bipolar & Related D/O d/t a Another Medical Condition Endocrine (e.g., thyroid, hypothalamic-pituitary-adrenal/HPA) Neurologic (e.g.,
- 65. Substance/Medication-induced Depressive, Bipolar & Related D/O ILLICITS can be from intoxication or withdrawal phases EtOH –
- 66. Mood D/O’s lab w/u CBC Chem panel TSH B12 U-tox U-preg (dep on demographics) RPR (syphilis)
- 67. Summary – cont’d Diagnostic building blocks (not counting mixed feature possibilities…)
- 68. 5 Myths and Facts About Suicide Myth #1: People who talk about killing themselves rarely commit
- 69. 5 Myths and Facts About Suicide Myth #2: The suicidal person wants to die and feels
- 70. 5 Myths and Facts About Suicide Myth # 3: If you ask someone about their suicidal
- 71. 5 Myths and Facts About Suicide Myth # 4: All suicidal people are deeply depressed. 43
- 72. 5 Myths and Facts About Suicide Myths # 5: Suicidal people rarely seek medical attention. 44
- 73. Socio-demographic Risk Factors Male > 60 years Widowed or Divorced White or Native American Living alone
- 74. Clinical Risk Factors Previous Attempts Clinical depression or schizophrenia Substance Abuse Feelings of hopelessness Severe anxiety,
- 75. Suicide:Treatment Problem-solving Cognitive behavioral therapy Coping skills Stress reduction 47
- 76. Additional case presentations
- 77. Case 2. 18yo M high school student who was BIB his parents to the ER after
- 78. Case 3. 50yo F, under-employed and barely hanging-on with temp agency work, comes in for her
- 80. Major depressive disorder (MDD) – Key Points MDD can be a chronic, recurrent, and progressive condition1,2
- 81. Summary Mood D/O’s are Ψ conditions where emotional dysregulation is the primary issue. Mood d/o’s can
- 83. Скачать презентацию
Objectives
Mood, affect, mood disorders (mood D/O’s)
Nosology, epidemiology, treatment (tx)
Objectives
Mood, affect, mood disorders (mood D/O’s)
Nosology, epidemiology, treatment (tx)
Mood - The subjective sense indicates the long, deep and constant
Mood - The subjective sense indicates the long, deep and constant
Mood - The subjective sense indicates the long, deep and constant
Mood - The subjective sense indicates the long, deep and constant
Mood v. Affect
“mood”
a sustained emotional attitude
typically garnered through pt
Mood v. Affect
“mood”
a sustained emotional attitude
typically garnered through pt
Major Depressive Disorder
Major Depressive Disorder
Economics of Depression —
U.S.A. Data - Total Annual Cost ~$44 Billion
9
Lost
Economics of Depression —
U.S.A. Data - Total Annual Cost ~$44 Billion
9
Lost
Major Depressive D/O (MDD)
Diagnosis req’s ≥1 major depressive episode (MDE)
MDE =
Major Depressive D/O (MDD)
Diagnosis req’s ≥1 major depressive episode (MDE)
MDE =
Question:
When does a major depressive episode (MDE) ≠ Major Depressive Disorder?
Question:
When does a major depressive episode (MDE) ≠ Major Depressive Disorder?
Major Depressive D/O (MDD)
EXCLUSIONS:
not attributable to a substance/medication or another
Major Depressive D/O (MDD)
EXCLUSIONS:
not attributable to a substance/medication or another
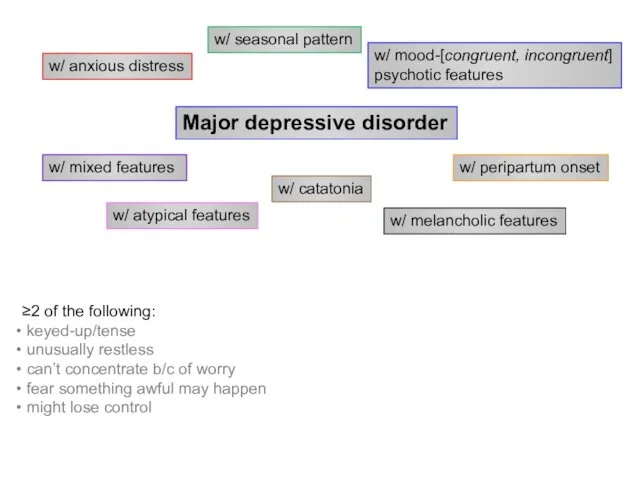
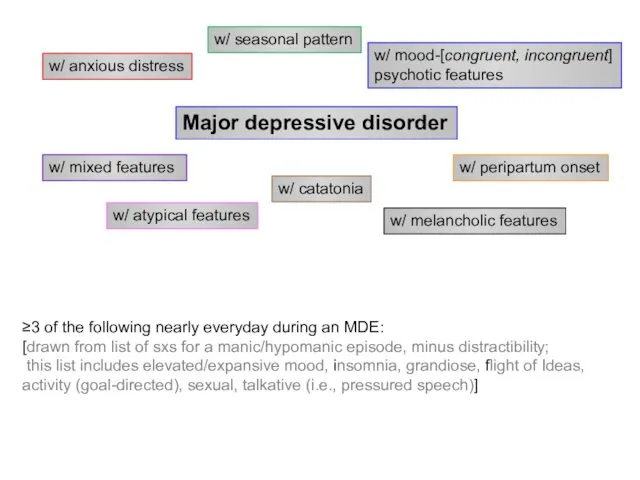
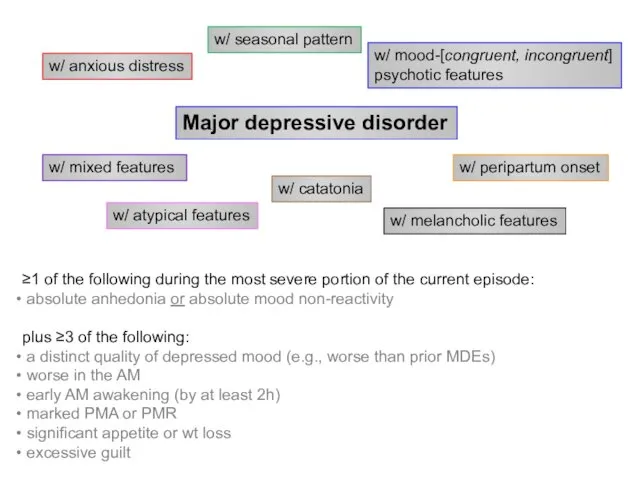
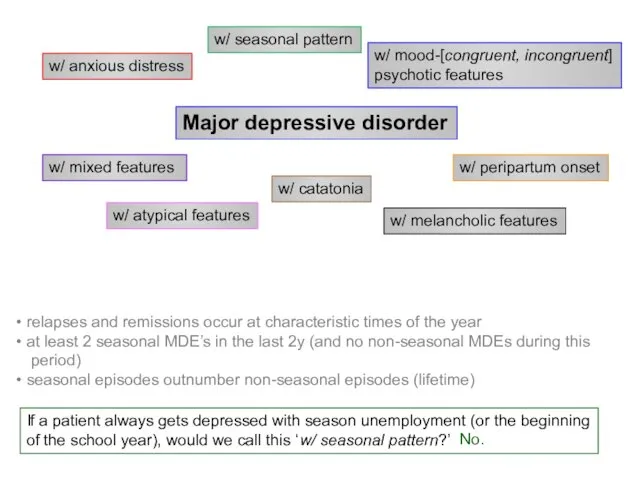
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Major depressive disorder
w/ anxious distress
w/ mixed features
w/ atypical features
w/ melancholic features
w/
Belmaker RH and Agam G, NEJM 2008, 358:55-68
iproniazid (1957)
imipramine (1959)
Belmaker RH and Agam G, NEJM 2008, 358:55-68
iproniazid (1957)
imipramine (1959)
Question:
Do antidepressants have additional actions besides inhibition of reuptake transporters?
“…the Zoloft
Question:
Do antidepressants have additional actions besides inhibition of reuptake transporters?
“…the Zoloft
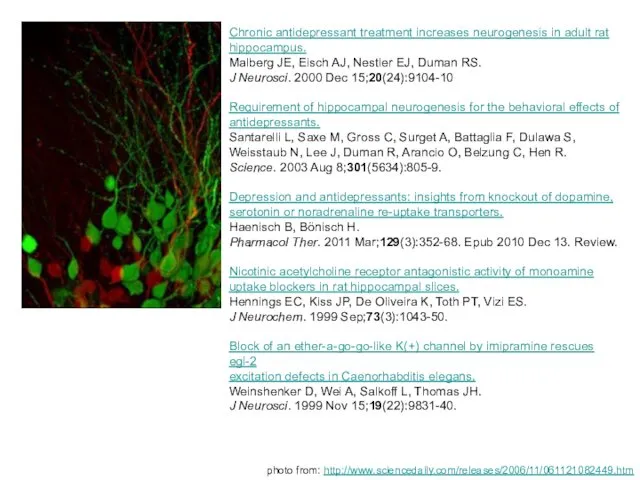
Chronic antidepressant treatment increases neurogenesis in adult rat
hippocampus.
Malberg JE, Eisch AJ,
Chronic antidepressant treatment increases neurogenesis in adult rat
hippocampus.
Malberg JE, Eisch AJ,
Subsequent hypotheses about MDD
altered glutamatergic transmission
↓’d GABAergic transmission
monoamine-Ach imbalance
disruption of endogenous
Subsequent hypotheses about MDD
altered glutamatergic transmission
↓’d GABAergic transmission
monoamine-Ach imbalance
disruption of endogenous
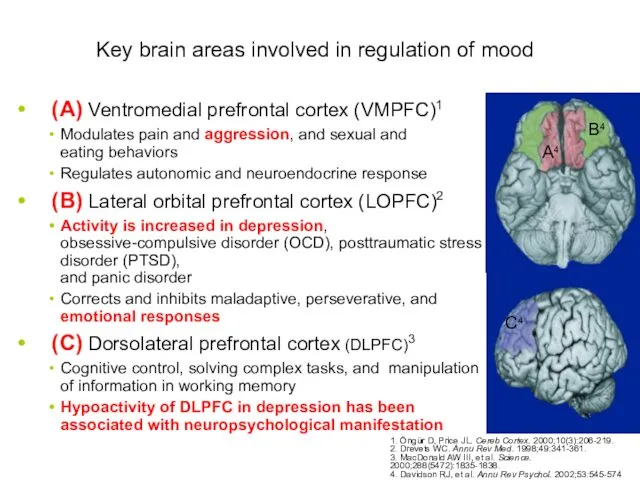
Key brain areas involved in regulation of mood
(A) Ventromedial prefrontal cortex
Key brain areas involved in regulation of mood
(A) Ventromedial prefrontal cortex
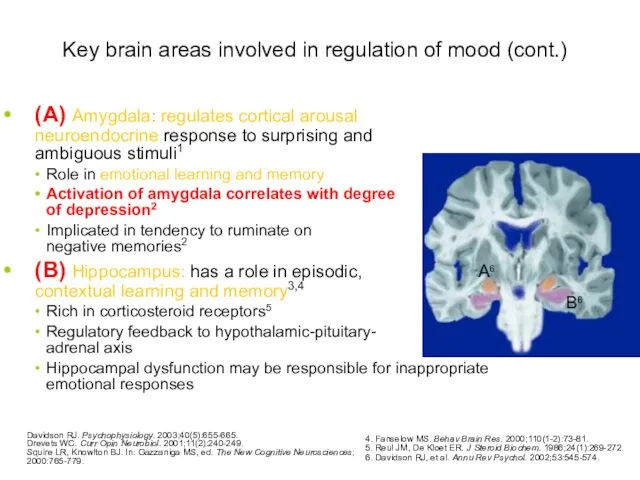
Key brain areas involved in regulation of mood (cont.)
(A) Amygdala: regulates
Key brain areas involved in regulation of mood (cont.)
(A) Amygdala: regulates
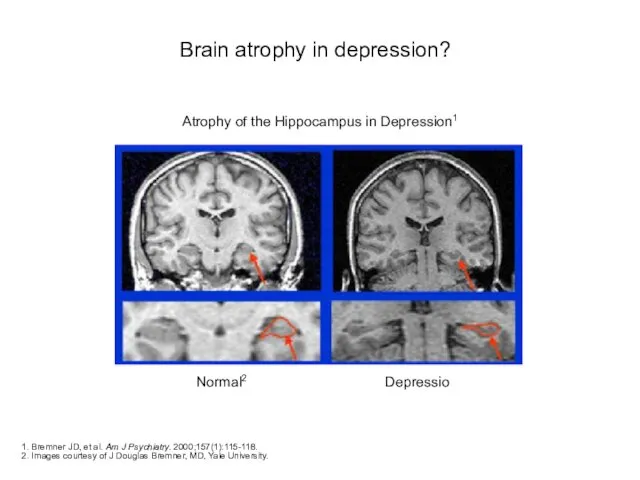
Brain atrophy in depression?
1. Bremner JD, et al. Am J Psychiatry.
Brain atrophy in depression?
1. Bremner JD, et al. Am J Psychiatry.
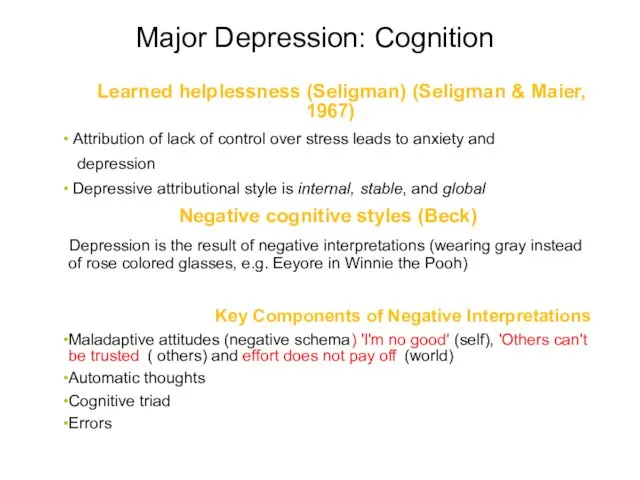
Major Depression: Cognition
Learned helplessness (Seligman) (Seligman & Maier, 1967)
Attribution
Major Depression: Cognition
Learned helplessness (Seligman) (Seligman & Maier, 1967)
Attribution
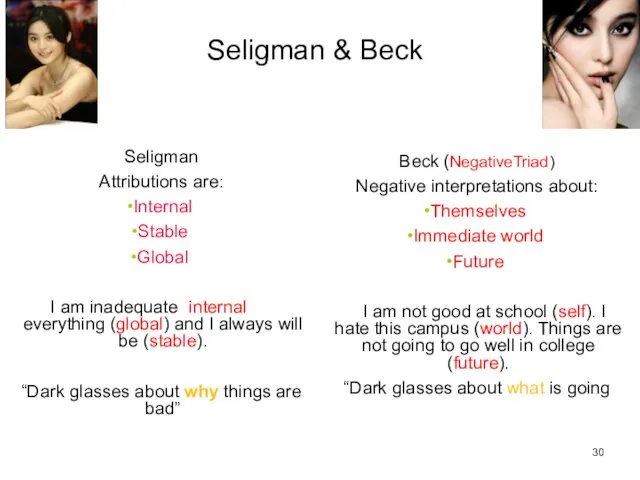
Seligman & Beck
Seligman
Attributions are:
Internal
Stable
Global
I am inadequate (internal) at everything (global) and
Seligman & Beck
Seligman
Attributions are:
Internal
Stable
Global
I am inadequate (internal) at everything (global) and
Cognitive theories
Beck’s theory:
31
Character of pessimism (NegativeTriad)
Habits of negativity (Negative schemas)
Erroneous thinking
Cognitive theories
Beck’s theory:
31
Character of pessimism (NegativeTriad)
Habits of negativity (Negative schemas)
Erroneous thinking
Characteristic biases
Arbitrary inference
Selective abstraction
Overgeneralization
Magnification and minimization
32
Characteristic biases
Arbitrary inference
Selective abstraction
Overgeneralization
Magnification and minimization
32
Behavioral theories
Learned helplessness/hopelessness is a behavioral theory with a cognitive twist.
Reduction
Behavioral theories
Learned helplessness/hopelessness is a behavioral theory with a cognitive twist.
Reduction
Availability of reinforcers
The amount of reinforcement available is a function of
Personal
Availability of reinforcers
The amount of reinforcement available is a function of
Personal
Interpersonal theory
Reduced interpersonal support
Experiences of rejection
Due to social structure
Inadequate social networks
Others
Interpersonal theory
Reduced interpersonal support
Experiences of rejection
Due to social structure
Inadequate social networks
Others
MDD tx options
selective serotonin reuptake
inhibitors (SSRIs)
fluoxetine (PROZAC), 20-80
MDD tx options
selective serotonin reuptake
inhibitors (SSRIs)
fluoxetine (PROZAC), 20-80
Sequenced Treatment Alternatives for the Relief of Depression
(STAR*D)
major NIMH-funded study
Sequenced Treatment Alternatives for the Relief of Depression
(STAR*D)
major NIMH-funded study
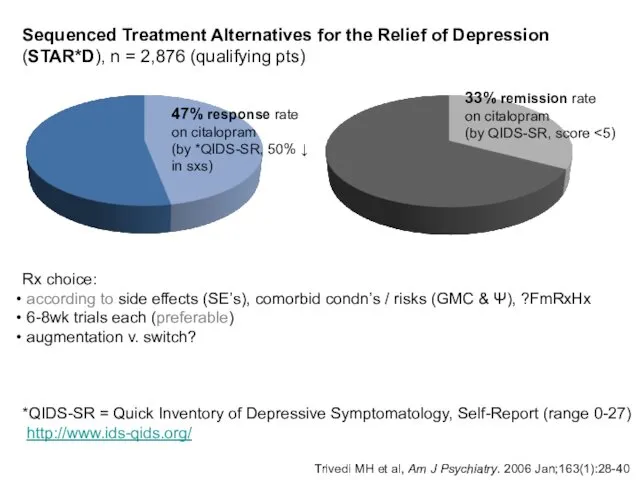
Trivedi MH et al, Am J Psychiatry. 2006 Jan;163(1):28-40
47%
Trivedi MH et al, Am J Psychiatry. 2006 Jan;163(1):28-40
47%
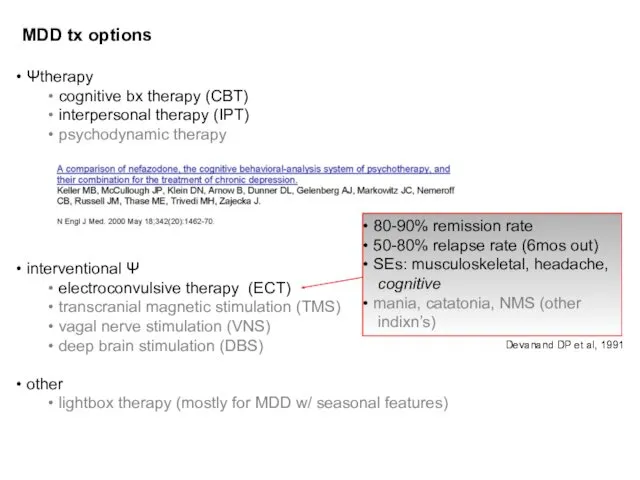
MDD tx options
Ψtherapy
cognitive bx therapy (CBT)
interpersonal therapy (IPT)
MDD tx options
Ψtherapy
cognitive bx therapy (CBT)
interpersonal therapy (IPT)
Major Depressive D/O (MDD)
NATURAL HISTORY (Frank E and Thase ME, 1999
Major Depressive D/O (MDD)
NATURAL HISTORY (Frank E and Thase ME, 1999
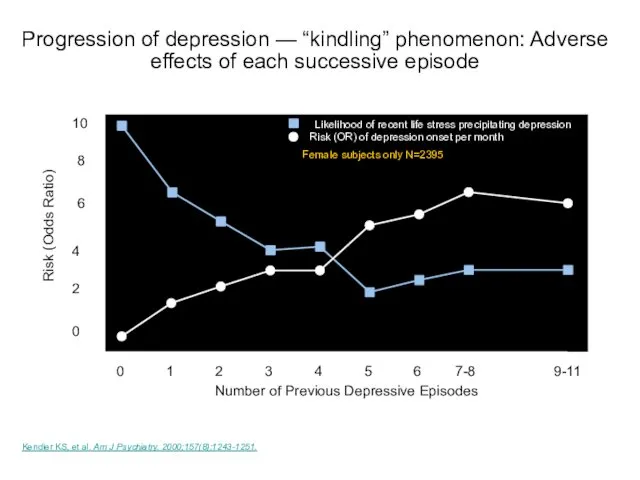
Kendler KS, et al. Am J Psychiatry. 2000;157(8):1243-1251.
Number of Previous Depressive
Kendler KS, et al. Am J Psychiatry. 2000;157(8):1243-1251.
Number of Previous Depressive
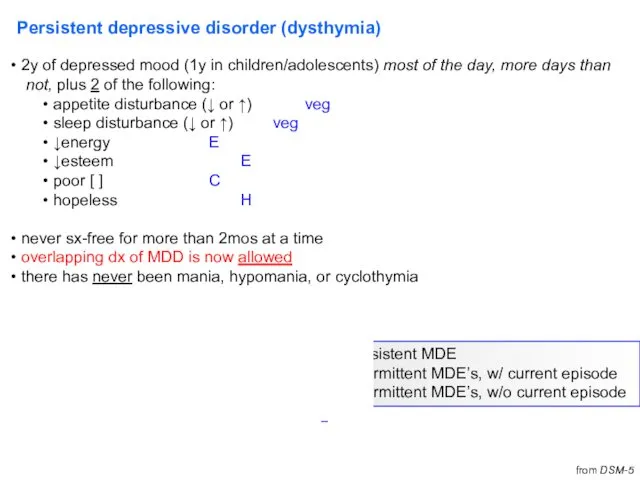
Persistent depressive disorder (dysthymia)
2y of depressed mood (1y in children/adolescents)
Persistent depressive disorder (dysthymia)
2y of depressed mood (1y in children/adolescents)
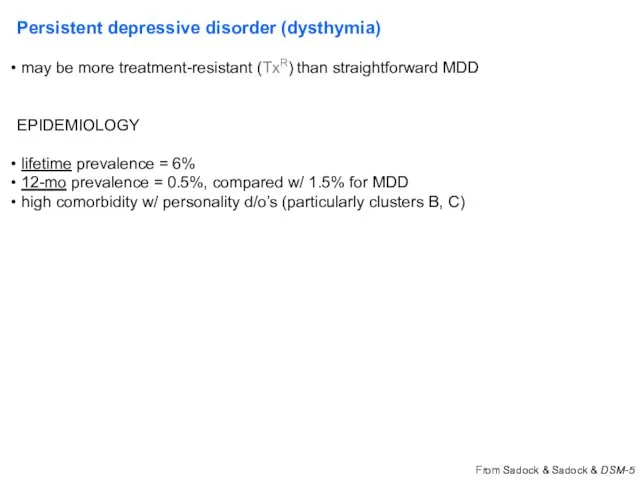
Persistent depressive disorder (dysthymia)
may be more treatment-resistant (TxR) than straightforward
Persistent depressive disorder (dysthymia)
may be more treatment-resistant (TxR) than straightforward
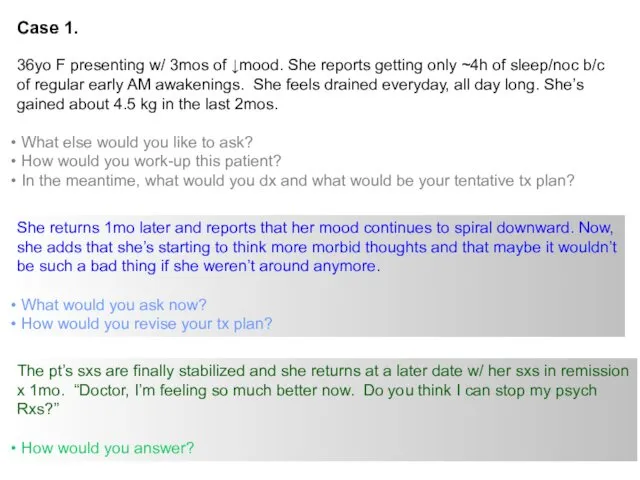
Case 1.
36yo F presenting w/ 3mos of ↓mood. She reports getting
Case 1.
36yo F presenting w/ 3mos of ↓mood. She reports getting
Premenstrual dysphoric d/o
Criterion A. In most menstrual cycles, ≥5 sxs in
Premenstrual dysphoric d/o
Criterion A. In most menstrual cycles, ≥5 sxs in
Premenstrual dysphoric d/o
(M)ood (labile &/or irritable &/or anxious)
Sleep
Interest
Body
Energy
Concentration
Appetite
Out of control
Treatment:
SSRI
Premenstrual dysphoric d/o
(M)ood (labile &/or irritable &/or anxious)
Sleep
Interest
Body
Energy
Concentration
Appetite
Out of control
Treatment:
SSRI
Disruptive mood dysregulation disorder
*severe recurrent temper outbursts (verbal or behavior)
Disruptive mood dysregulation disorder
*severe recurrent temper outbursts (verbal or behavior)
Bipolar disorder
Bipolar disorder
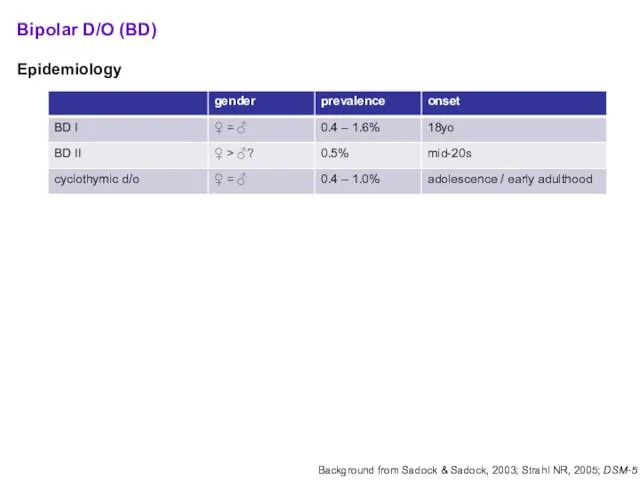
Bipolar D/O (BD)
Epidemiology
Diagnostic criteria:
BD I
≥ 1 manic episode
MDE
Bipolar D/O (BD)
Epidemiology
Diagnostic criteria:
BD I
≥ 1 manic episode
MDE
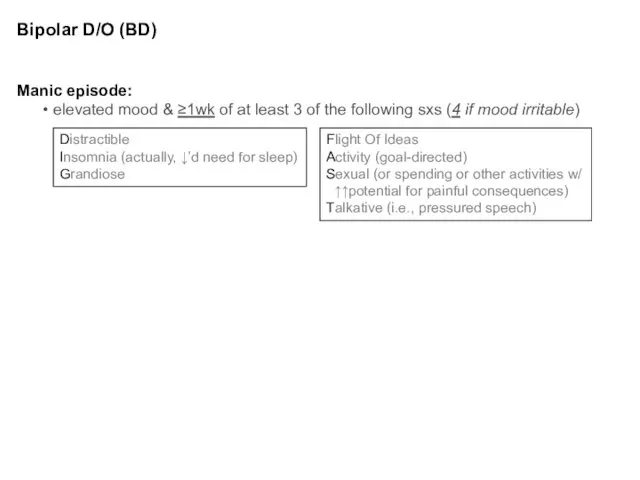
Bipolar D/O (BD)
Manic episode:
elevated mood & ≥1wk of at least
Bipolar D/O (BD)
Manic episode:
elevated mood & ≥1wk of at least
Bipolar Disorder (BD)
EXCLUSIONS:
another medical cause
substance/medication causes
SPECIFIERS:
same as w/
Bipolar Disorder (BD)
EXCLUSIONS:
another medical cause
substance/medication causes
SPECIFIERS:
same as w/
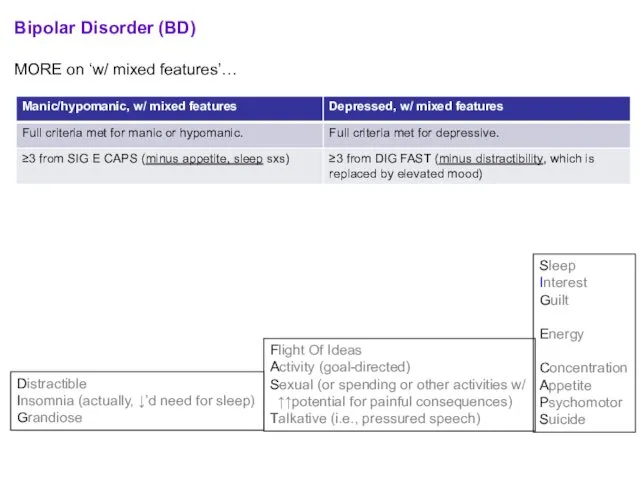
Bipolar Disorder (BD)
MORE on ‘w/ mixed features’…
IF full criteria met for
Bipolar Disorder (BD)
MORE on ‘w/ mixed features’…
IF full criteria met for
Case 1 - continued
Prior hx to date:
36yo F w/ 3mos
Case 1 - continued
Prior hx to date:
36yo F w/ 3mos
Case 1 - continued
Is manic switch a real concern?
mood stabilizer =
Case 1 - continued
Is manic switch a real concern?
mood stabilizer =
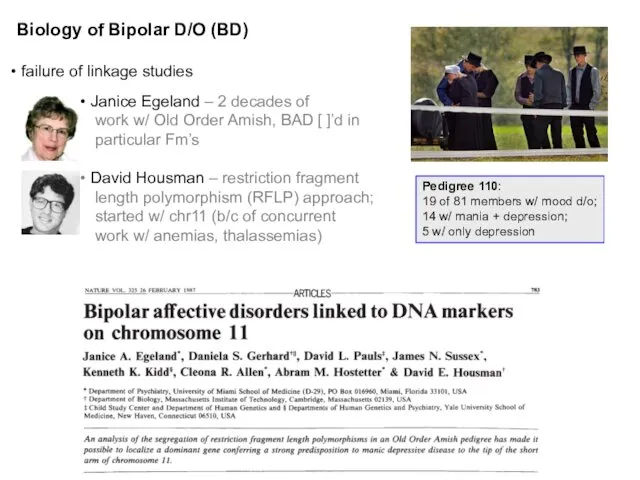
Biology of Bipolar D/O (BD)
failure of linkage studies
Janice Egeland
Biology of Bipolar D/O (BD)
failure of linkage studies
Janice Egeland
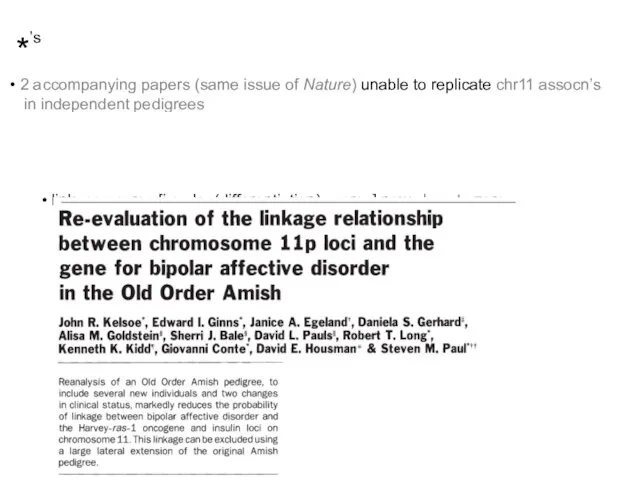
*’s
2 accompanying papers (same issue of Nature) unable to replicate
*’s
2 accompanying papers (same issue of Nature) unable to replicate
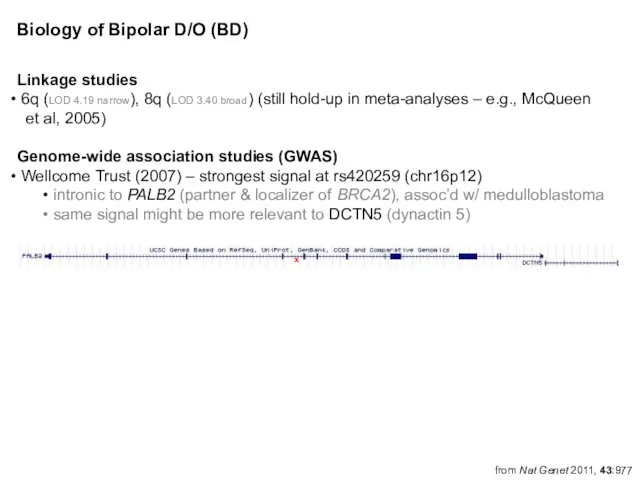
Linkage studies
6q (LOD 4.19 narrow), 8q (LOD 3.40 broad) (still
6q (LOD 4.19 narrow), 8q (LOD 3.40 broad) (still
More on select GWA-identified candidates
CACNA1C
α1 subunit of a voltage-dependent
More on select GWA-identified candidates
CACNA1C
α1 subunit of a voltage-dependent
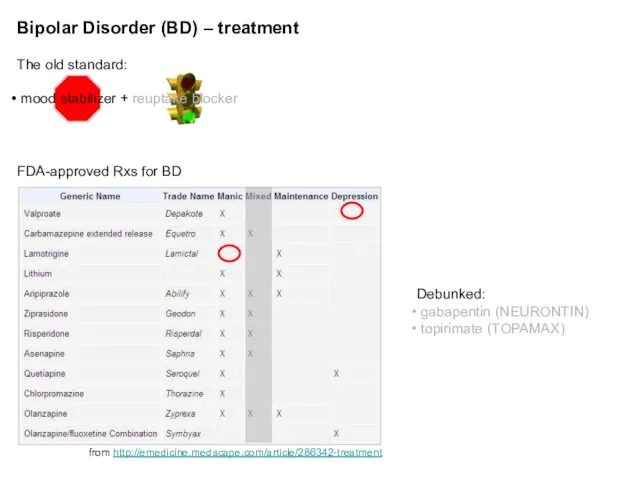
Bipolar Disorder (BD) – treatment
The old standard:
mood stabilizer + reuptake
Bipolar Disorder (BD) – treatment
The old standard:
mood stabilizer + reuptake
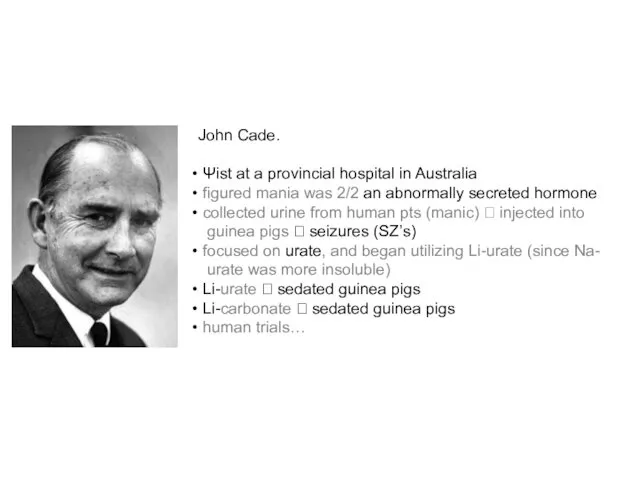
John Cade.
Ψist at a provincial hospital in Australia
figured mania
John Cade.
Ψist at a provincial hospital in Australia
figured mania
Bipolar Disorder (BD) – treatment (cont’d)
Li+ v. Depakote / valproate (VPA)
Bipolar Disorder (BD) – treatment (cont’d)
Li+ v. Depakote / valproate (VPA)
Bipolar Disorder (BD) – treatment (cont’d)
How many agents to use?
combination
Bipolar Disorder (BD) – treatment (cont’d)
How many agents to use?
combination
Bipolar Disorder (BD) – natural history
60% of manic episodes immediately
Bipolar Disorder (BD) – natural history
60% of manic episodes immediately
Cyclothymic D/O
2y of fluctuating mood (1y in children, adolescents)
hypomanic
Cyclothymic D/O
2y of fluctuating mood (1y in children, adolescents)
hypomanic
Differential diagnosis
Differential diagnosis
Phenocopies and gray areas…
Anxiety D/O’s (esp. GAD, PTSD)
Schizoaffective D/O
Phenocopies and gray areas…
Anxiety D/O’s (esp. GAD, PTSD)
Schizoaffective D/O
Depressive, Bipolar & Related D/O d/t a Another Medical Condition
Endocrine
Depressive, Bipolar & Related D/O d/t a Another Medical Condition
Endocrine
Substance/Medication-induced Depressive, Bipolar & Related D/O
ILLICITS
can be from intoxication or
Substance/Medication-induced Depressive, Bipolar & Related D/O
ILLICITS
can be from intoxication or
Mood D/O’s lab w/u
CBC
Chem panel
TSH
B12
U-tox
U-preg
Mood D/O’s lab w/u
CBC
Chem panel
TSH
B12
U-tox
U-preg
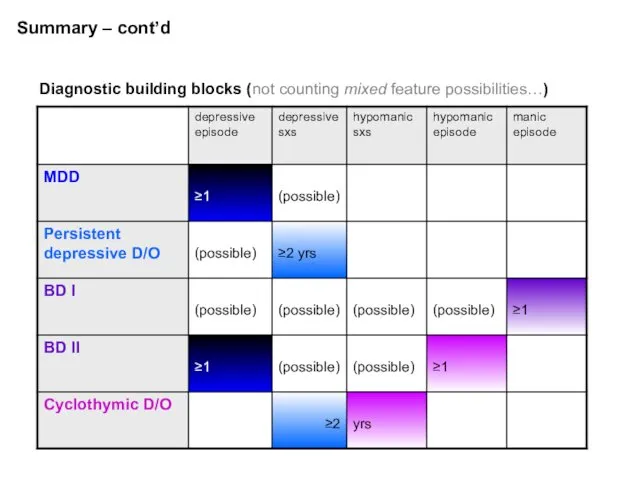
Summary – cont’d
Diagnostic building blocks (not counting mixed feature possibilities…)
Summary – cont’d
Diagnostic building blocks (not counting mixed feature possibilities…)
5 Myths and Facts About Suicide
Myth #1:
People who talk about killing
5 Myths and Facts About Suicide
Myth #1:
People who talk about killing
5 Myths and Facts About Suicide
Myth #2:
The suicidal person wants to
5 Myths and Facts About Suicide
Myth #2:
The suicidal person wants to
5 Myths and Facts About Suicide
Myth # 3:
If you ask someone
5 Myths and Facts About Suicide
Myth # 3:
If you ask someone
5 Myths and Facts About Suicide
Myth # 4:
All suicidal people are
5 Myths and Facts About Suicide
Myth # 4:
All suicidal people are
5 Myths and Facts About Suicide
Myths # 5:
Suicidal people rarely seek
5 Myths and Facts About Suicide
Myths # 5:
Suicidal people rarely seek
Socio-demographic Risk Factors
Male
> 60 years
Widowed or Divorced
White or Native American
Living alone
Socio-demographic Risk Factors
Male
> 60 years
Widowed or Divorced
White or Native American
Living alone
Clinical Risk Factors
Previous Attempts
Clinical depression or schizophrenia
Substance Abuse
Feelings of hopelessness
Severe anxiety,
Clinical Risk Factors
Previous Attempts
Clinical depression or schizophrenia
Substance Abuse
Feelings of hopelessness
Severe anxiety,
Suicide:Treatment
Problem-solving
Cognitive behavioral therapy
Coping skills
Stress reduction
47
Suicide:Treatment
Problem-solving
Cognitive behavioral therapy
Coping skills
Stress reduction
47
Additional case presentations
Additional case presentations
Case 2.
18yo M high school student who was BIB his parents
Case 2.
18yo M high school student who was BIB his parents
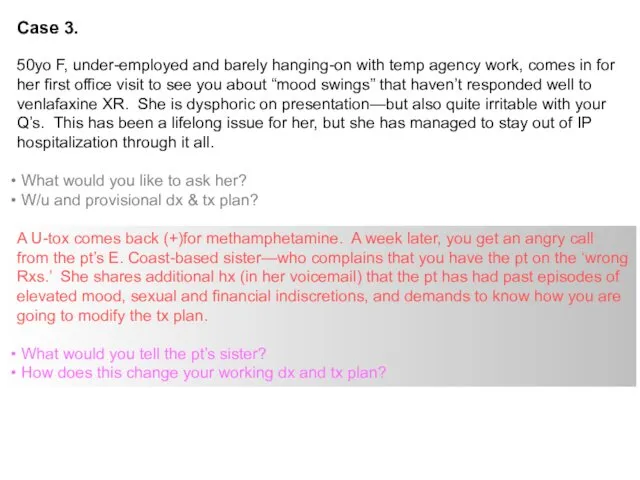
Case 3.
50yo F, under-employed and barely hanging-on with temp agency work,
Case 3.
50yo F, under-employed and barely hanging-on with temp agency work,
Major depressive disorder (MDD) – Key Points
MDD can be a chronic,
Major depressive disorder (MDD) – Key Points
MDD can be a chronic,
Summary
Mood D/O’s are Ψ conditions where emotional dysregulation is the
Summary
Mood D/O’s are Ψ conditions where emotional dysregulation is the
 Эмоциональная сфера дошкольников в подготовительной группе
Эмоциональная сфера дошкольников в подготовительной группе Struktura zachowań rekreacyjnych od koncepcji systemu do struktury rekreacji. (Wykład 2)
Struktura zachowań rekreacyjnych od koncepcji systemu do struktury rekreacji. (Wykład 2) Особенности личностного своеобразия детей с нарушением речи и коммуникации
Особенности личностного своеобразия детей с нарушением речи и коммуникации Как быть англичанином
Как быть англичанином Критерии готовности к школе
Критерии готовности к школе Иллюзии
Иллюзии Theories of personality
Theories of personality Психолого-педагогическое сопровождение участников образовательной деятельности на этапе подготовки к итоговой аттестации
Психолого-педагогическое сопровождение участников образовательной деятельности на этапе подготовки к итоговой аттестации Навички для психологічного відновлення
Навички для психологічного відновлення Как преодолеть стресс
Как преодолеть стресс Дизайн-мышление педагога дополнительного образования
Дизайн-мышление педагога дополнительного образования Этические особенности работы психолога с детьми и подростками
Этические особенности работы психолога с детьми и подростками Что такое – обида?
Что такое – обида? Мотивация. Общая характеристика учебной мотивации
Мотивация. Общая характеристика учебной мотивации Қиял дегеніміз
Қиял дегеніміз Управление стрессами
Управление стрессами Психодрама. Создание и развитие психодрамы
Психодрама. Создание и развитие психодрамы Конфликтные ситуации в деятельности вожатого и их разрешение. Возрастные особенности детей
Конфликтные ситуации в деятельности вожатого и их разрешение. Возрастные особенности детей Медиативные навыки: инструментарий медиатора
Медиативные навыки: инструментарий медиатора Мышление в психическом развитии. Лекция 6
Мышление в психическом развитии. Лекция 6 Темперамент и выбор профессии
Темперамент и выбор профессии Психологія пам’яті
Психологія пам’яті Общение как специфический вид деятельности
Общение как специфический вид деятельности Катализаторы креативности
Катализаторы креативности Отношение пожилых к старости
Отношение пожилых к старости Введение в психологию. Предмет, задачи и методы психологии
Введение в психологию. Предмет, задачи и методы психологии Жесты и мимика как невербальные средства общения
Жесты и мимика как невербальные средства общения Эмпирические исследования познавательных процессов. ОПП- 2
Эмпирические исследования познавательных процессов. ОПП- 2