- Congenital intestinal obstruction

Содержание
- 2. Oesophageal atresia Oesophageal atresia is defined as an interruption in the continuity of the oesophagus with
- 3. At least 18 different syndromes have been reported in association with oesophageal atresia. The best known
- 4. Types of tracheo-oesophageal fistula
- 6. Clinic The earliest symptom of oesophageal atresia is a polyhydramnios in the second half of pregnancy.
- 7. Prenatal diagnosis - polyhydramnios
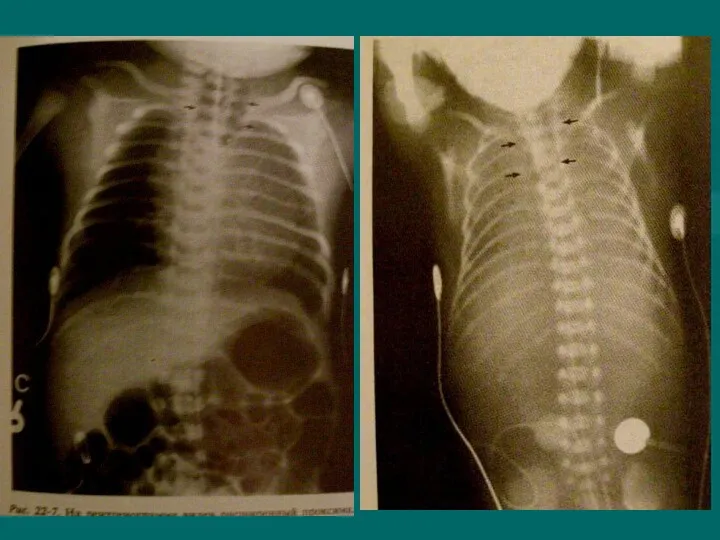
- 8. Inability to pass nasogastric tube. Abdominal Xray with air in the stomach excludes esophageal atresia A
- 10. Differential diagnosis Intranatal asphyxia of newborn Birth injury of brain Aspiration pneumonia Congenital diaphragmatic hernia with
- 11. Complications Early complications include: Anastamotic leak, recurrent TEF, tracheomalacia. Late Complications include: Anastamotic stricture (25%), reflux
- 12. Treatment Operation includes TEF ligation, transection, and restoration with end-to-end anastamosis.
- 15. Hypertrophic Pyloric Stenosis
- 16. Infantile hypertrophic pyloric stenosis (IHPS) is a common surgical condition encountered in early infancy, occurring in
- 17. Cause of hypertrophic circular muscle abnormal peptidergic innervation, abnormality of nitrergic innervation, abnormalities of extracellular matrix
- 18. Clinic Age is 3-6 weeks (1 month of age) A 4 week old infant presents with
- 19. Initially there is only regurgitation of feeds,but over several days vomiting progresses to be characteristically projectile.
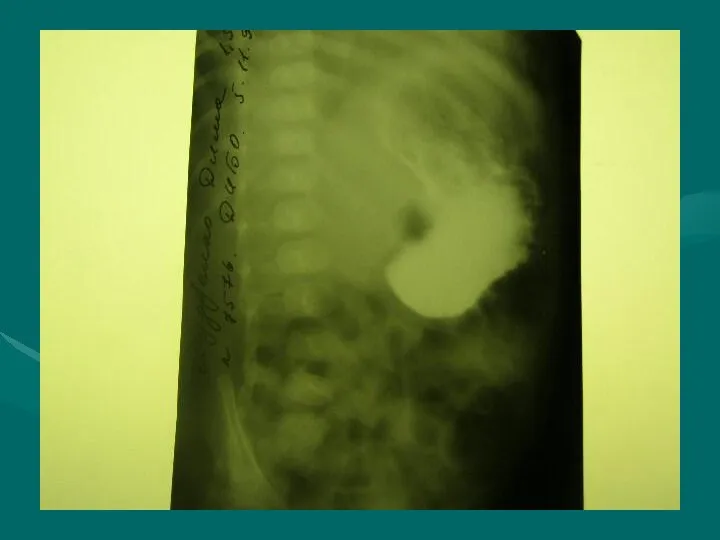
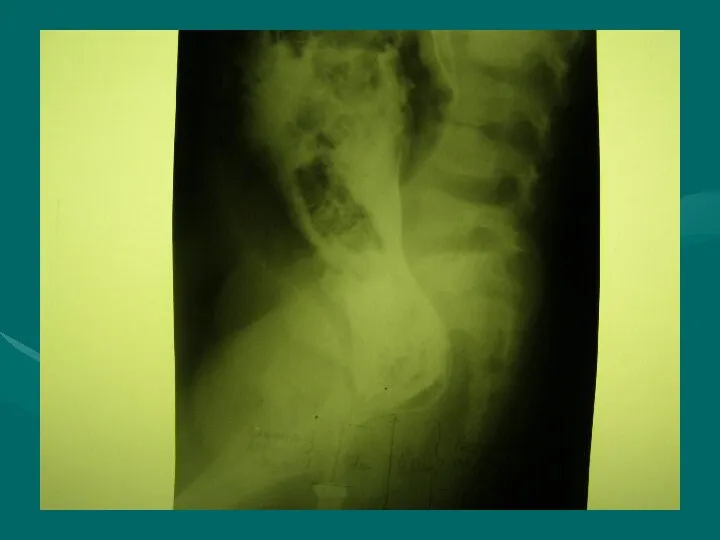
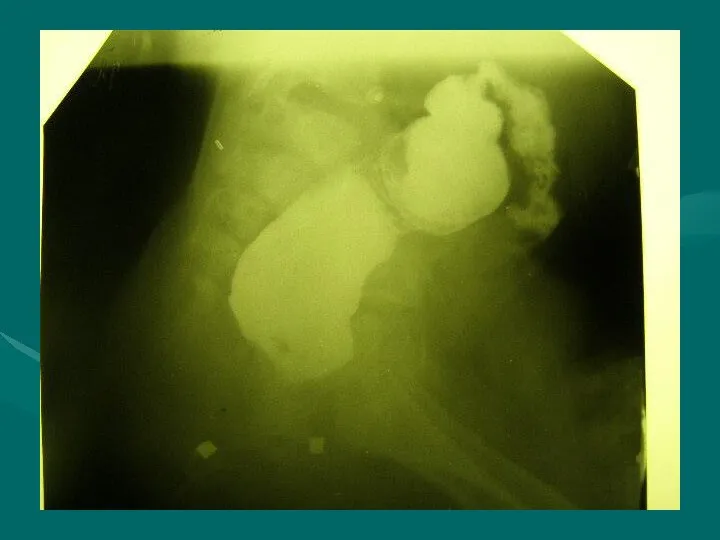
- 20. X-ray symptom Increas of stomach Gastric peristalsis “Beak symptom” or pylorus narrowing Deceleration evacuation of contrast
- 23. Differential diagnosis Congenital pyloric stenosis Stomach impassability Duodenal obstruction Vomiting syndrome
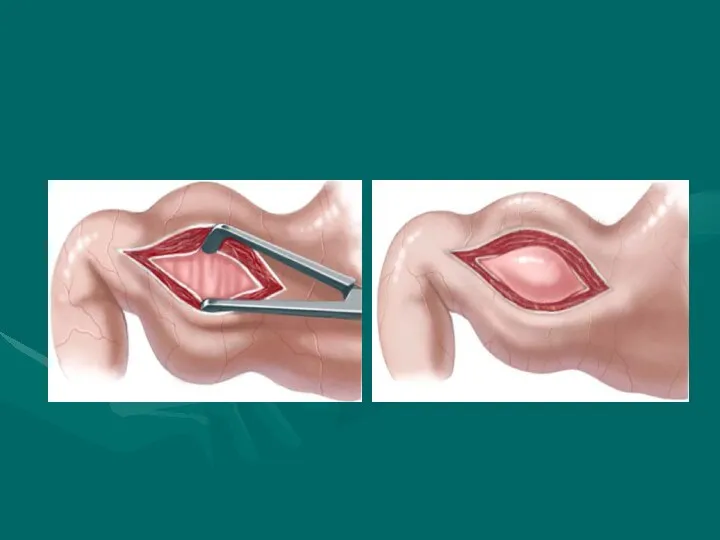
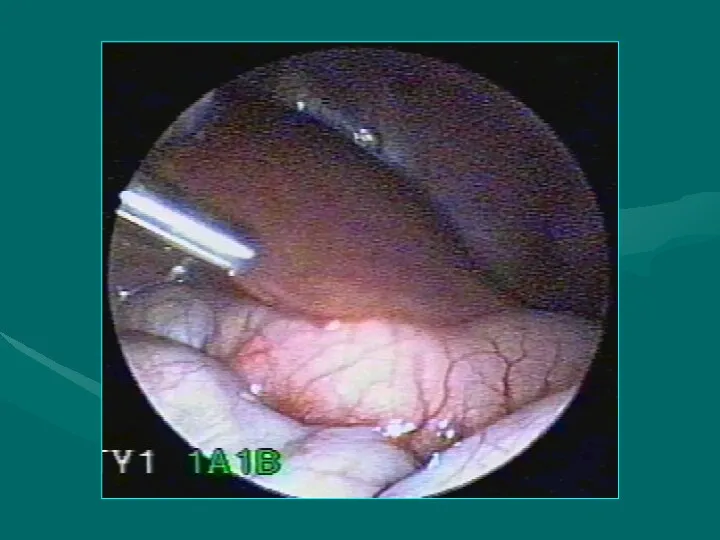
- 24. Treatment The operation for pyloric stenosis is not an emergency and should never be undertaken until
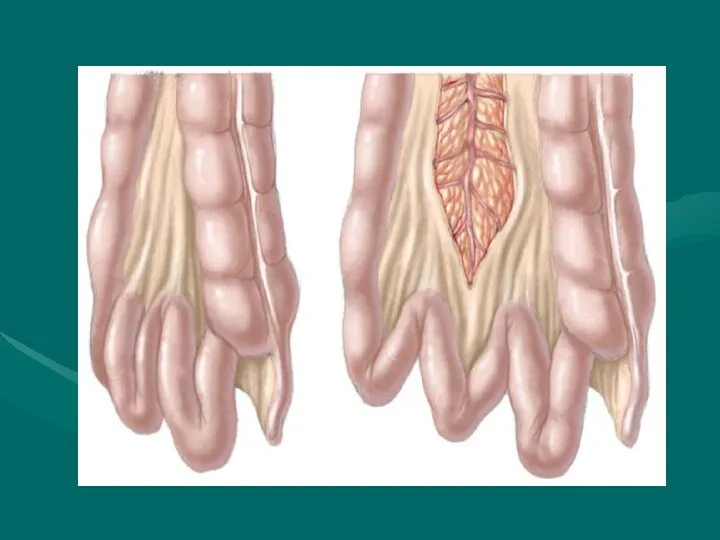
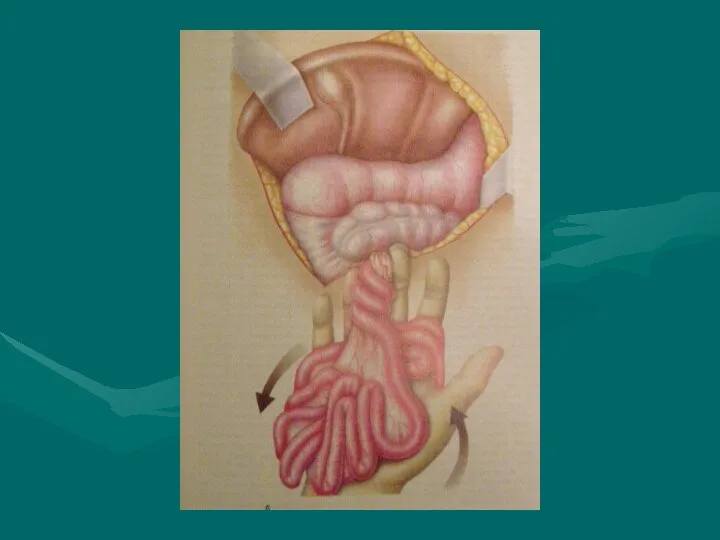
- 31. Duodenal obstruction During the embryonic period the duodenojejunal loop rotates 270° around the superior mesenteric artery
- 33. Duoenal obstruction, with the possibility of vascular compromise, is due to either an associated volvulus or
- 36. An infant with abdominal tenderness and blood per rectum is suggestive of bowel ischaemia due to
- 38. Differential diagnosis Pylorospasm Pyloric stenosis Congenital diaphragmatic hernia Helminthic invasion Helminthic cholecystitis
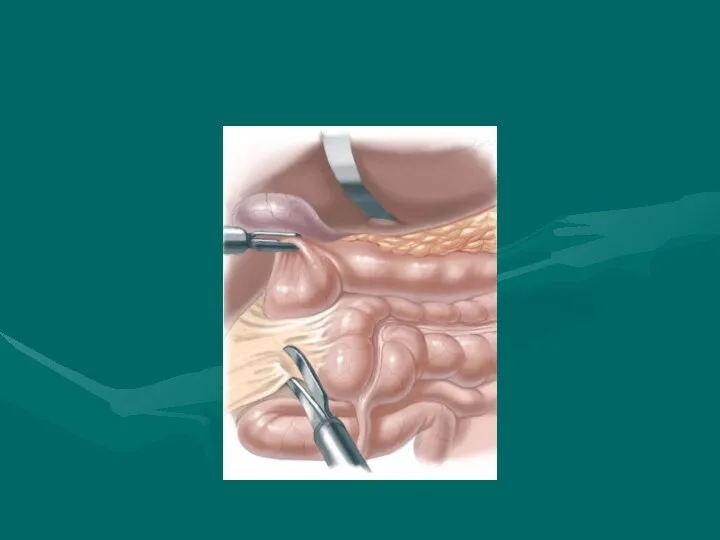
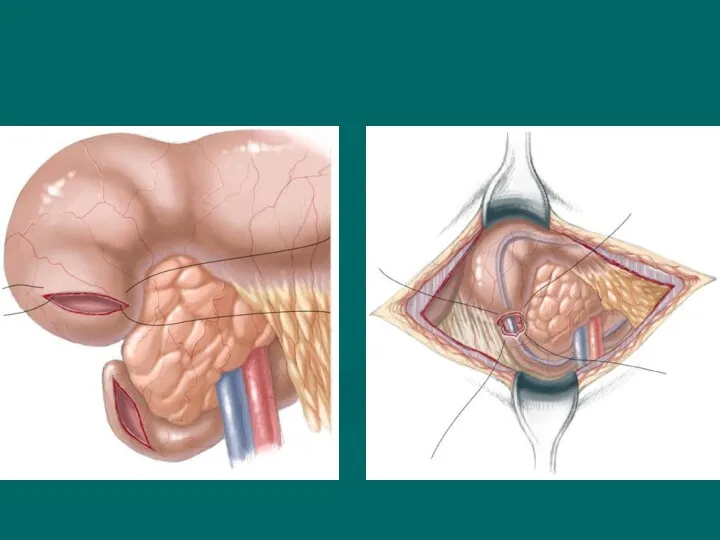
- 39. Treatment Duodenoduodenostomy is the procedure of choice for patients with duodenal atresia, stenosis and annular pancreas.
- 41. Hirschprung’s disease Hirschsprung’s disease (HD) is characterised by an absence of ganglion cells in the distal
- 42. Сlassification (Lenushkin, 1989) Anatomic forms: Rectal Rectosigmoid Segmental Subtotal Total form Clinic forms Compensated Subcompensated Decompensated
- 43. Clinic Of all cases of HD, 80–90% produce clinical symptoms and are diagnosed during the neonatal
- 44. A full-term neonate has bilious emesis during first and second days of life. The abdomen is
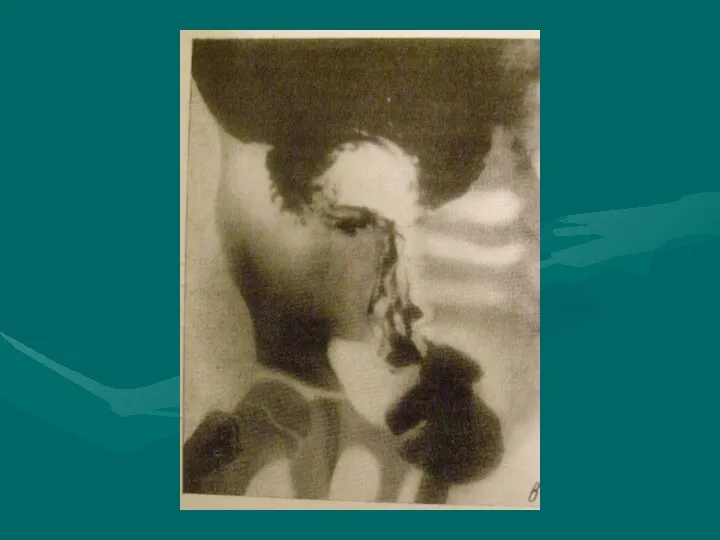
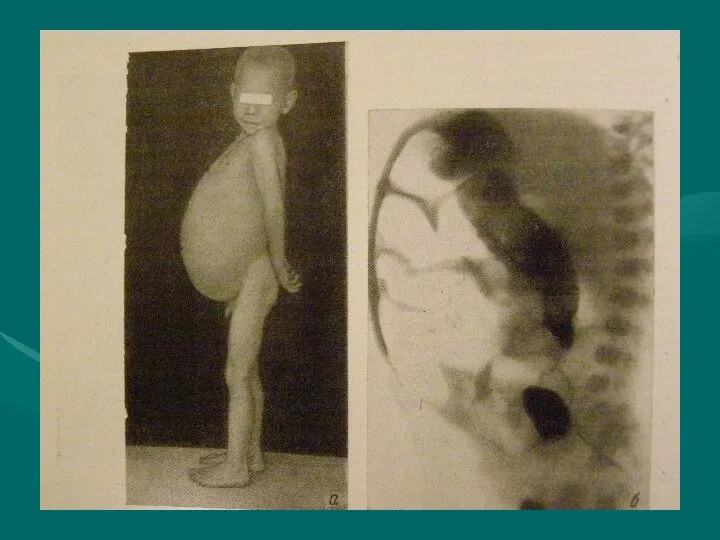
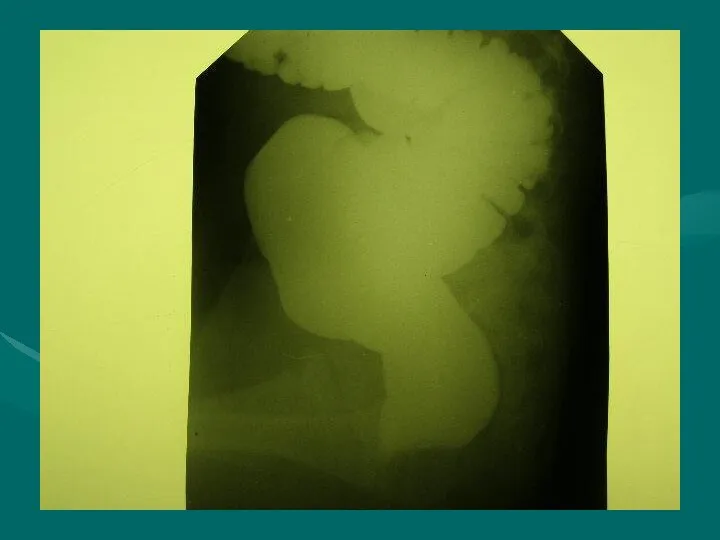
- 46. Diagnostic work-up includes: Contrast enema showing a contracted rectum with dilated bowel above. Failure to evacuate
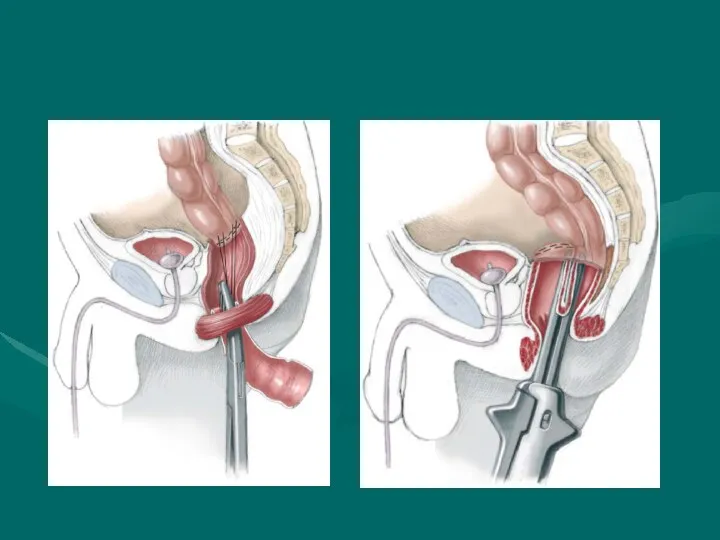
- 49. Surgical treatment Soave endo-rectal pull through with removal of the diseased distal bowel with coloanal anastamosis
- 52. Anorectal anomalies Anorectal malformations, represent a wide spectrum of defects. Surgical techniques useful to repair the
- 53. Сlassification
- 55. External fistula: Vaginal fistula Perineal fistula Scrotal fistula Internal fistula: Vaginal fistula Fistula in the urinary
- 56. Perineal Fistula This malformation represents the simplest of the spectrum. In this defect, the rectum opens
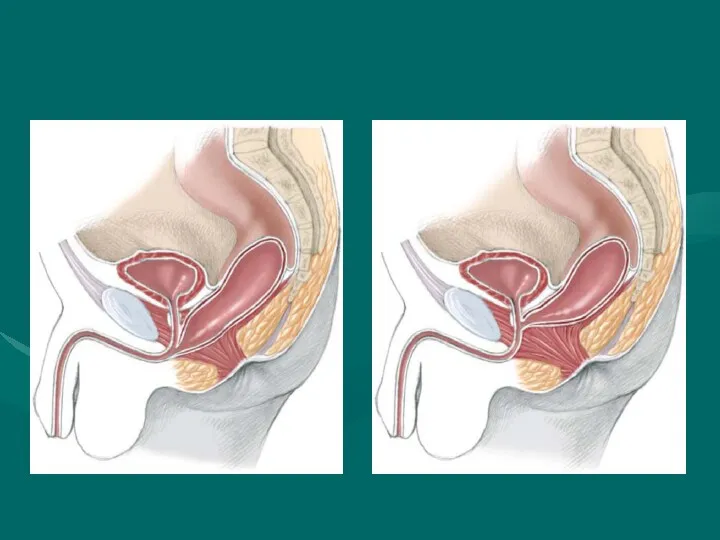
- 58. Rectourethral Fistula. This group of patients include two specific categories: (a) rectourethral bulbar fistula (Fig 3),
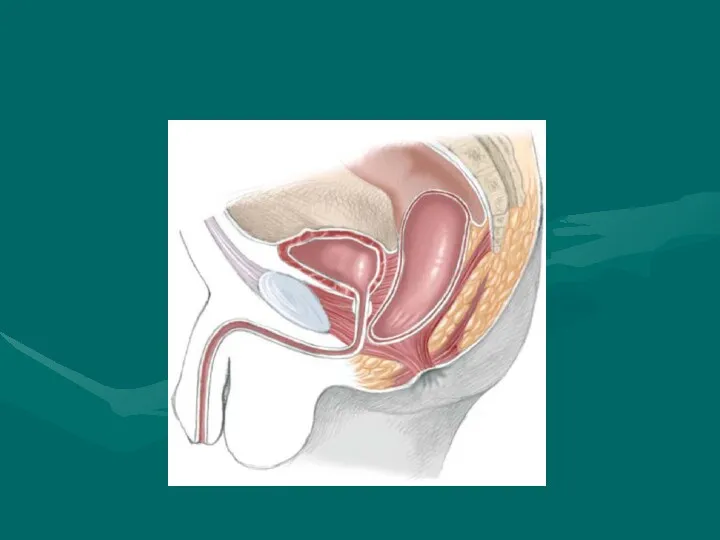
- 60. Imperforate Anus Without Fistula This particular malformation is unique.When we say imperforated anus without fistula, we
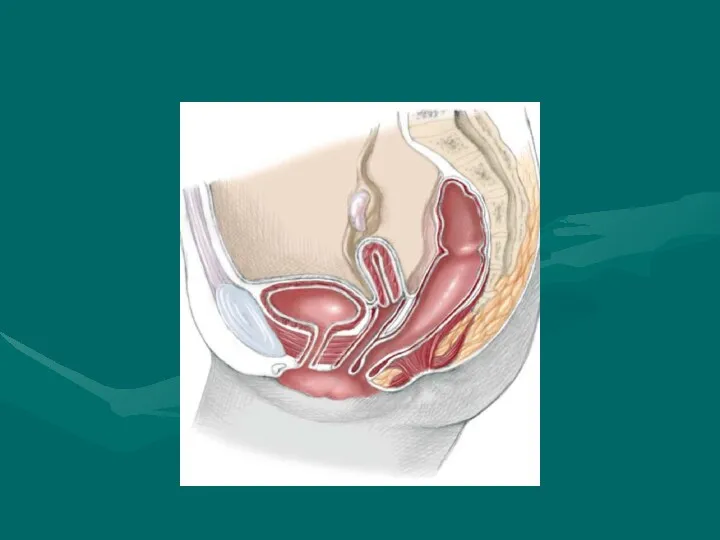
- 64. Rectoperineal Fistula. This defect is equivalent to the recto-perineal fistula in males already described. Bowel control
- 66. Cloaca. A cloaca is defined as a malformation in which the rectum, vagina and urethra are
- 68. INTUSSUSCEPTION
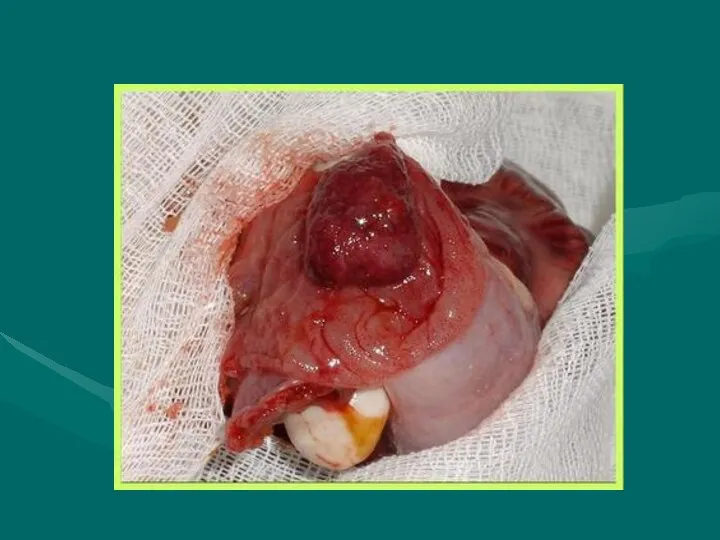
- 69. INTUSSUSCEPTION DEFINITION Telescoping of a proximal segment of the intestine (intussusceptum) into a distal segment (intussuscipiens)
- 71. INTUSSUSCEPTION ANATOMIC LOCATIONS ILEOCOLIC MOST COMMON IN CHILDREN ILEO-ILEOCOLIC SECOND MOST COMMON ENTEROENTERIC ILEO-ILEAL, JEJUNO-JEJUNAL MORE
- 73. PATHOPHYSIOLOGY Precipitating mechanism unknown Obstruction of intussusceptum mesentery Venous and lymphatic obstruction Ischemic necrosis occurs in
- 74. ETIOLOGIES Majority of pediatric intussusceptions idiopathic (85-90%) LYMPHOID HYPERPLASIA POSSIBLE ETIOLOGY Mechanical abnormalities may act as
- 75. EPIDEMIOLOGY Incidence 2 - 4 / 1000 live births Usual age group 3 months - 3
- 76. INTUSSUSCEPTION CLINICAL CHARACTERISTICS Early Symptoms PAROXYSMAL ABDOMINAL PAIN SEPARATED BY PERIODS OF APATHY POOR FEEDING AND
- 77. PHYSICAL EVALUATION Moderately to severely ill Irritable, limited movement Most are at least 5-10% dehydrated 80%
- 78. INTUSSUSCEPTION STAGES I. Bright clinical manifestation II. Pseudodysenteric stage III. Peritonitis
- 79. Ultrasonic diagnostics
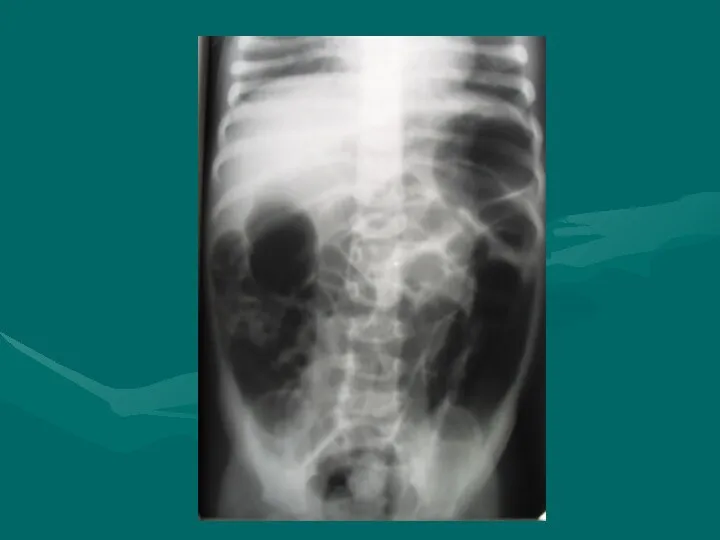
- 83. RADIOGRAPHIC EVALUATION Plain radiographs (acute abdominal series) Plain films suggestive in majority, but cannot rule out
- 86. TREATMENT Obstructive surgical emergency Pediatric surgeon notified immediately Supportive Therapy AGGRESSIVE FLUID RESUSCITATION ELECTROLYTES NASOGASTRIC TUBE
- 87. INTUSSUSCEPTION PNEUMATIC REDUCTION Theoretical Advantages LESS INFLAMMATION IF PERFORATION OCCURS Method AIR INSUFFLATION LIMITED TO MAXIMUM
- 88. INTUSSUSCEPTION NON-OPERATIVE REDUCTION CONTRAINDICATIONS Absolute Contraindications PERITONEAL SIGNS SUSPECTED PERFORATION Relative Contraindications SYMPTOMS > 24-48 HRS
- 89. INTUSSUSCEPTION FAILURE OF NON-OPERATIVE REDUCTION Factors associated with failure SYMPTOMS > 48 HRS RECTAL BLEEDING SMALL
- 90. Acquired intestinal obstruction Acquired intestinal obstructions are a partial or complete blockage of the small or
- 91. Intestinal obstructions can be mechanical or nonmechanical. Mechanical obstruction is caused by the bowel twisting on
- 92. Clinic 1. Abdominal pain 2. Vomiting 3. Constipation 4. Intoxication syndrome
- 93. Diagnosis X-ray examination Ultrasonic diagnostics Computed tomography Diagnostic testing will include a complete blood count (CBC),
- 94. Treatment Preoperative preparation: a. inserting a nasogastric tube to suction out the contents of the stomach
- 96. Скачать презентацию
Oesophageal atresia
Oesophageal atresia is defined as an interruption in the continuity
Oesophageal atresia
Oesophageal atresia is defined as an interruption in the continuity
At least 18 different syndromes have been reported in association with
At least 18 different syndromes have been reported in association with
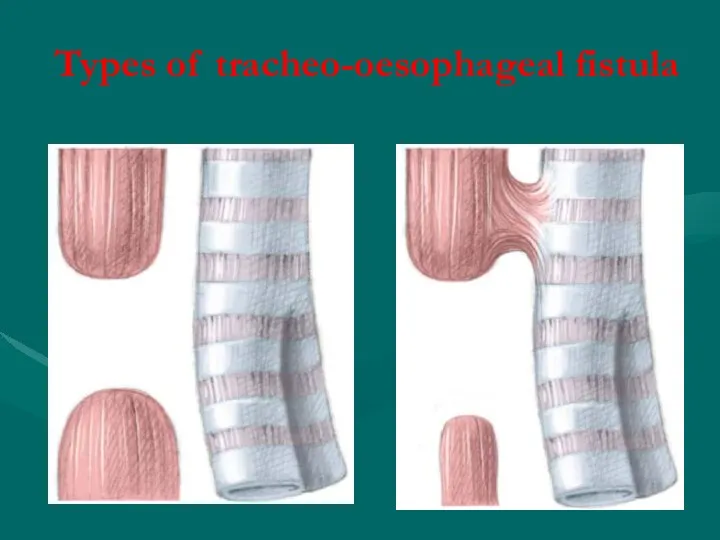
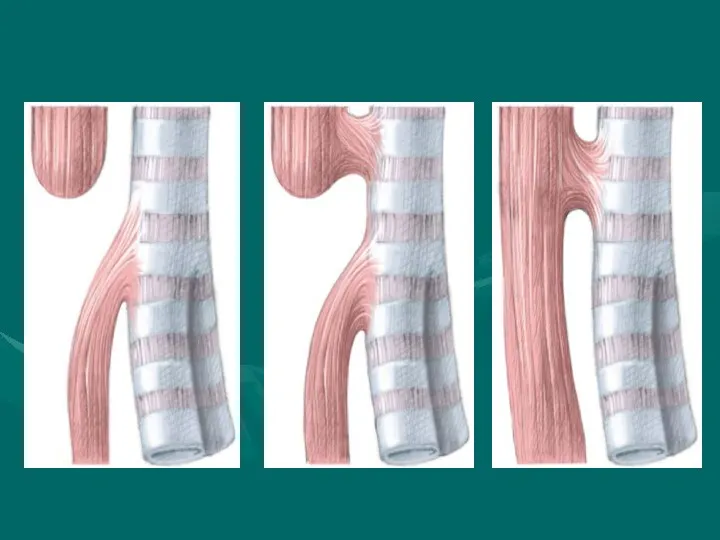
Types of tracheo-oesophageal fistula
Types of tracheo-oesophageal fistula
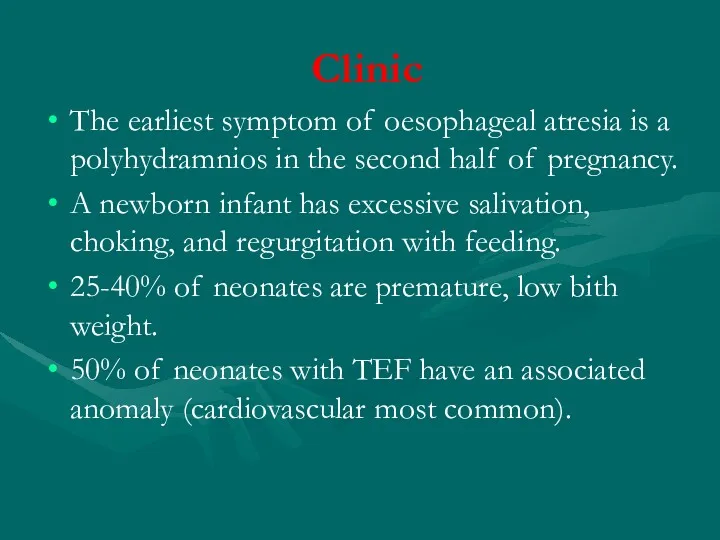
Clinic
The earliest symptom of oesophageal atresia is a polyhydramnios in
Clinic
The earliest symptom of oesophageal atresia is a polyhydramnios in
Prenatal diagnosis - polyhydramnios
Prenatal diagnosis - polyhydramnios
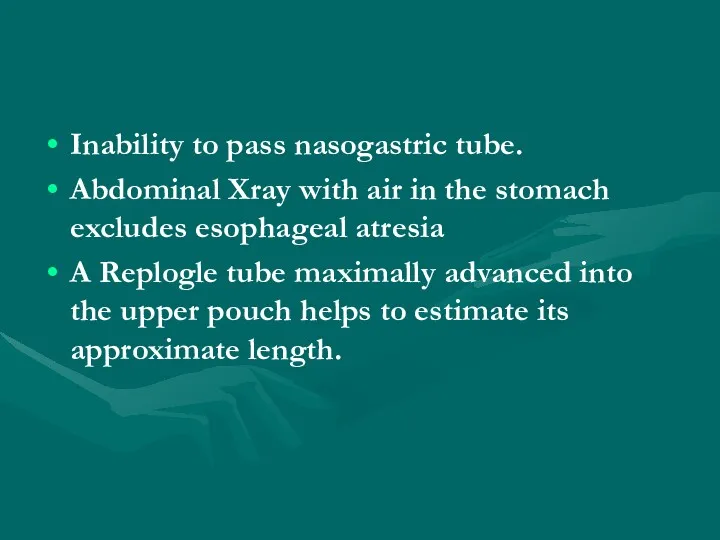
Inability to pass nasogastric tube.
Abdominal Xray with air in the stomach
Inability to pass nasogastric tube.
Abdominal Xray with air in the stomach
Differential diagnosis
Intranatal asphyxia of newborn
Birth injury of brain
Aspiration pneumonia
Congenital diaphragmatic hernia
Differential diagnosis
Intranatal asphyxia of newborn
Birth injury of brain
Aspiration pneumonia
Congenital diaphragmatic hernia
Complications
Early complications include: Anastamotic leak, recurrent TEF, tracheomalacia.
Late Complications include:
Complications
Early complications include: Anastamotic leak, recurrent TEF, tracheomalacia.
Late Complications include:
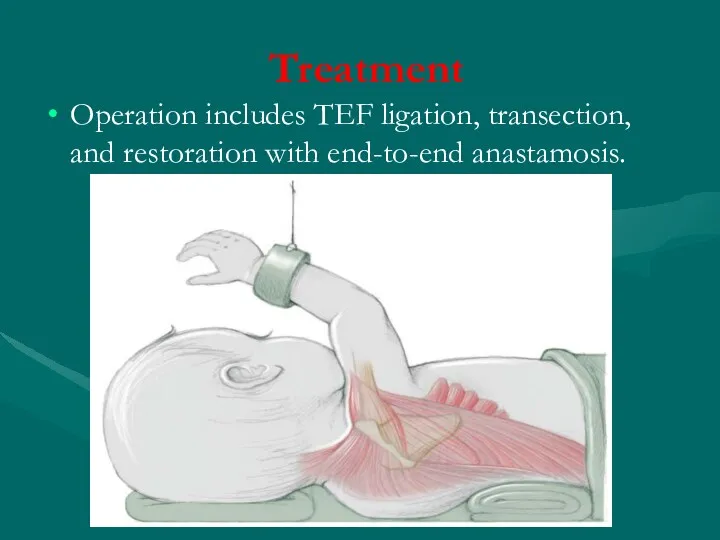
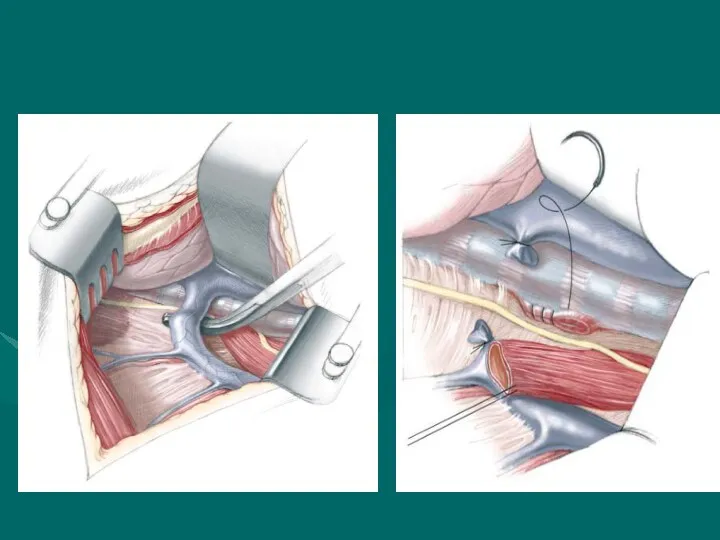
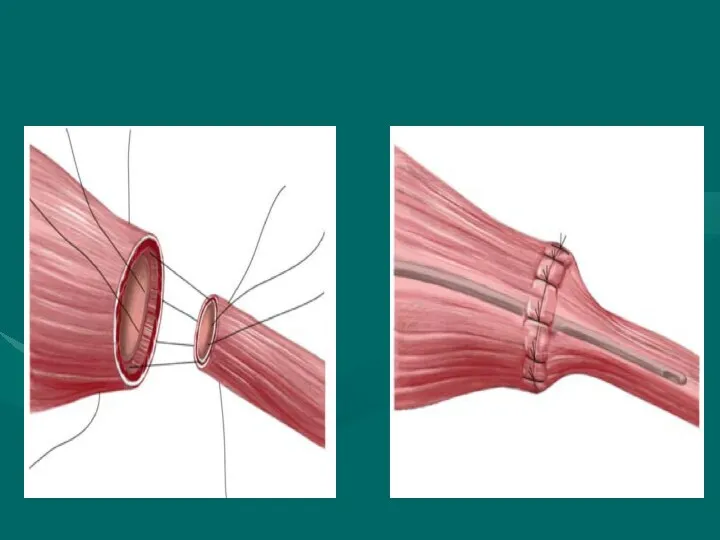
Treatment
Operation includes TEF ligation, transection, and restoration with end-to-end anastamosis.
Treatment
Operation includes TEF ligation, transection, and restoration with end-to-end anastamosis.
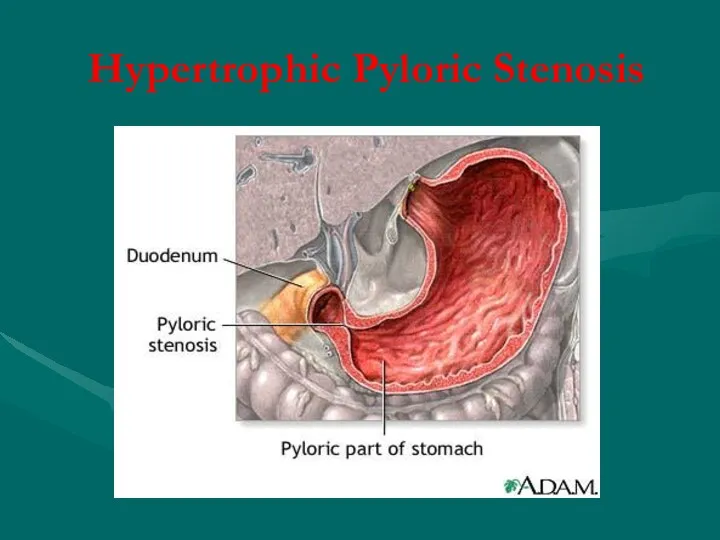
Hypertrophic Pyloric Stenosis
Hypertrophic Pyloric Stenosis
Infantile hypertrophic pyloric stenosis (IHPS) is a common surgical condition encountered
Infantile hypertrophic pyloric stenosis (IHPS) is a common surgical condition encountered
Cause of hypertrophic circular muscle
abnormal peptidergic innervation,
abnormality of nitrergic innervation,
abnormalities of
Cause of hypertrophic circular muscle
abnormal peptidergic innervation,
abnormality of nitrergic innervation,
abnormalities of
Clinic
Age is 3-6 weeks (1 month of age)
A 4 week old
Clinic
Age is 3-6 weeks (1 month of age)
A 4 week old
Initially there is only regurgitation of feeds,but over several days vomiting
Initially there is only regurgitation of feeds,but over several days vomiting
X-ray symptom
Increas of stomach
Gastric peristalsis
“Beak symptom” or pylorus narrowing
Deceleration evacuation of
X-ray symptom
Increas of stomach
Gastric peristalsis
“Beak symptom” or pylorus narrowing
Deceleration evacuation of

Differential diagnosis
Congenital pyloric stenosis
Stomach impassability
Duodenal obstruction
Vomiting syndrome
Differential diagnosis
Congenital pyloric stenosis
Stomach impassability
Duodenal obstruction
Vomiting syndrome
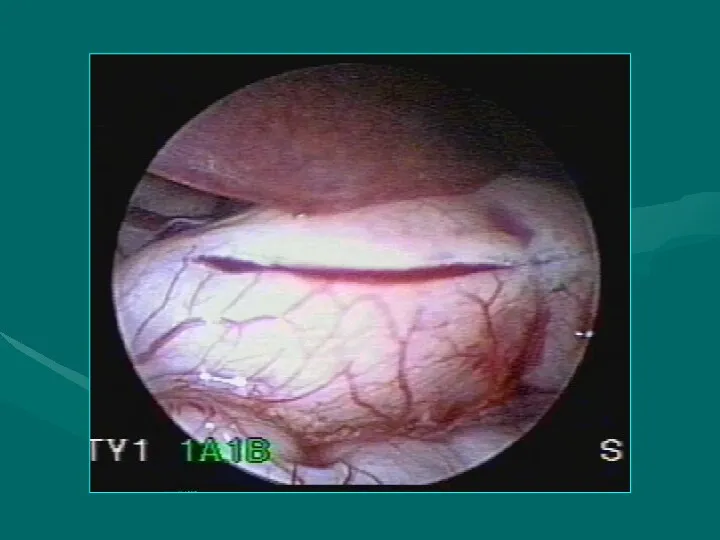
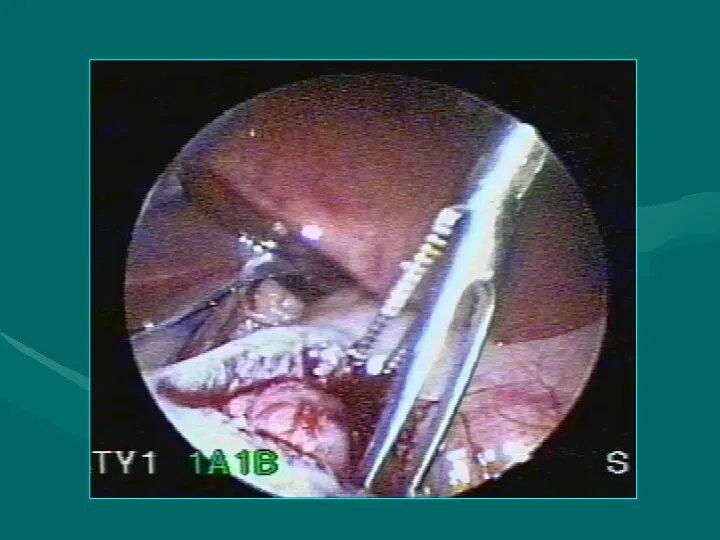
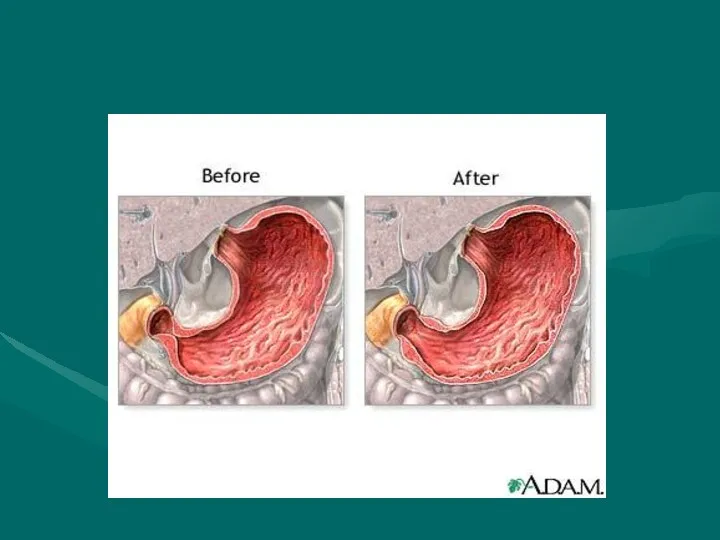
Treatment
The operation for pyloric stenosis is not an emergency and
Treatment
The operation for pyloric stenosis is not an emergency and

Duodenal obstruction
During the embryonic period the duodenojejunal loop rotates 270° around
Duodenal obstruction
During the embryonic period the duodenojejunal loop rotates 270° around
Duoenal obstruction, with the possibility of vascular compromise, is due to
Duoenal obstruction, with the possibility of vascular compromise, is due to

An infant with abdominal tenderness and blood per rectum is suggestive
An infant with abdominal tenderness and blood per rectum is suggestive
Differential diagnosis
Pylorospasm
Pyloric stenosis
Congenital diaphragmatic hernia
Helminthic invasion
Helminthic cholecystitis
Differential diagnosis
Pylorospasm
Pyloric stenosis
Congenital diaphragmatic hernia
Helminthic invasion
Helminthic cholecystitis
Treatment
Duodenoduodenostomy is the procedure of choice for patients with duodenal atresia,
Treatment
Duodenoduodenostomy is the procedure of choice for patients with duodenal atresia,
Hirschprung’s disease
Hirschsprung’s disease (HD) is characterised by an absence of ganglion
Hirschprung’s disease
Hirschsprung’s disease (HD) is characterised by an absence of ganglion

Сlassification
(Lenushkin, 1989)
Anatomic forms:
Rectal
Rectosigmoid
Segmental
Subtotal
Total form
Clinic forms
Compensated
Subcompensated
Decompensated
Сlassification
(Lenushkin, 1989)
Anatomic forms:
Rectal
Rectosigmoid
Segmental
Subtotal
Total form
Clinic forms
Compensated
Subcompensated
Decompensated
Clinic
Of all cases of HD, 80–90% produce clinical symptoms and are
Clinic
Of all cases of HD, 80–90% produce clinical symptoms and are
A full-term neonate has bilious emesis during first and second days
A full-term neonate has bilious emesis during first and second days
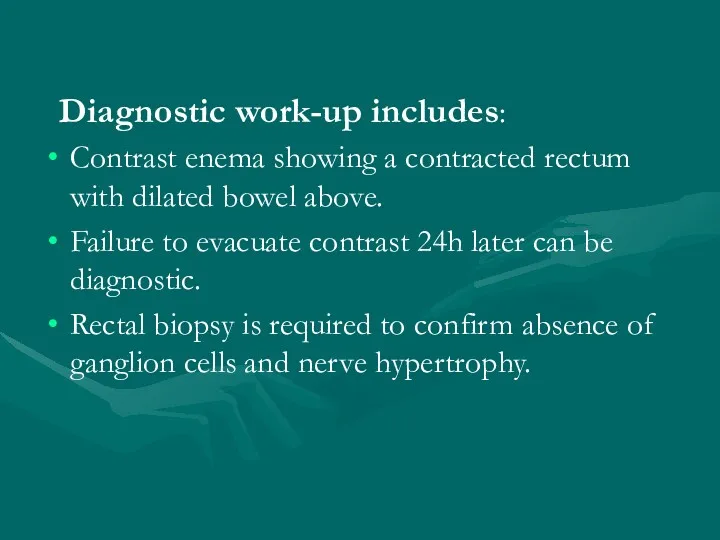
Diagnostic work-up includes:
Contrast enema showing a contracted rectum with dilated
Diagnostic work-up includes:
Contrast enema showing a contracted rectum with dilated
Surgical treatment
Soave endo-rectal pull through with removal of the diseased distal
Surgical treatment
Soave endo-rectal pull through with removal of the diseased distal
Anorectal anomalies
Anorectal malformations, represent a wide spectrum of defects. Surgical techniques
Anorectal anomalies
Anorectal malformations, represent a wide spectrum of defects. Surgical techniques
Сlassification
Сlassification
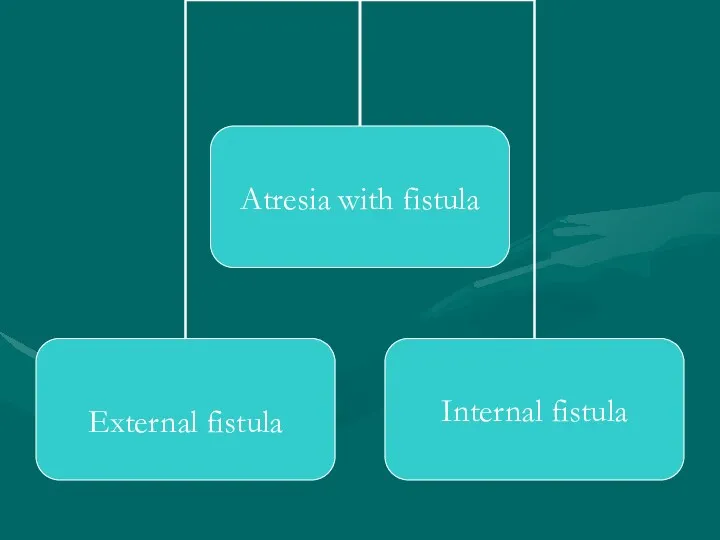
External fistula:
Vaginal fistula
Perineal fistula
Scrotal fistula
Internal fistula:
Vaginal fistula
Fistula in the urinary blader
Fistula
External fistula:
Vaginal fistula
Perineal fistula
Scrotal fistula
Internal fistula:
Vaginal fistula
Fistula in the urinary blader
Fistula
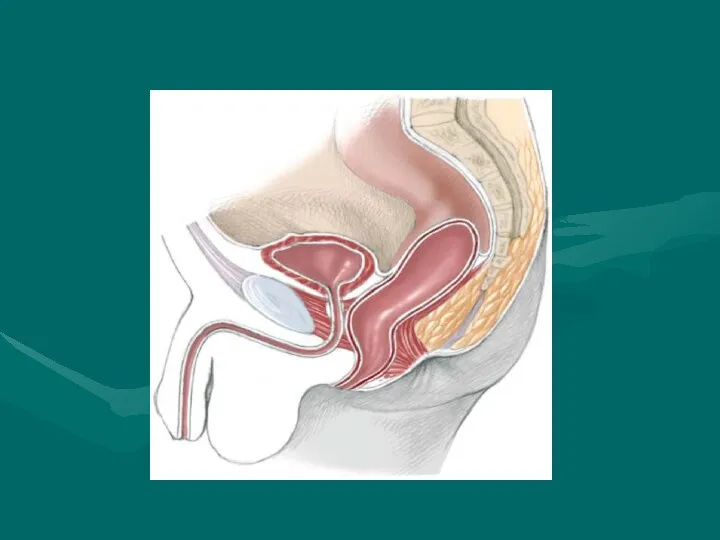
Perineal Fistula
This malformation represents the simplest of the spectrum. In
Perineal Fistula
This malformation represents the simplest of the spectrum. In
Rectourethral Fistula.
This group of patients include two specific categories: (a) rectourethral
Rectourethral Fistula.
This group of patients include two specific categories: (a) rectourethral
Imperforate Anus Without Fistula
This particular malformation is unique.When we say imperforated
Imperforate Anus Without Fistula
This particular malformation is unique.When we say imperforated
Rectoperineal Fistula.
This defect is equivalent to the recto-perineal fistula in males
Rectoperineal Fistula.
This defect is equivalent to the recto-perineal fistula in males
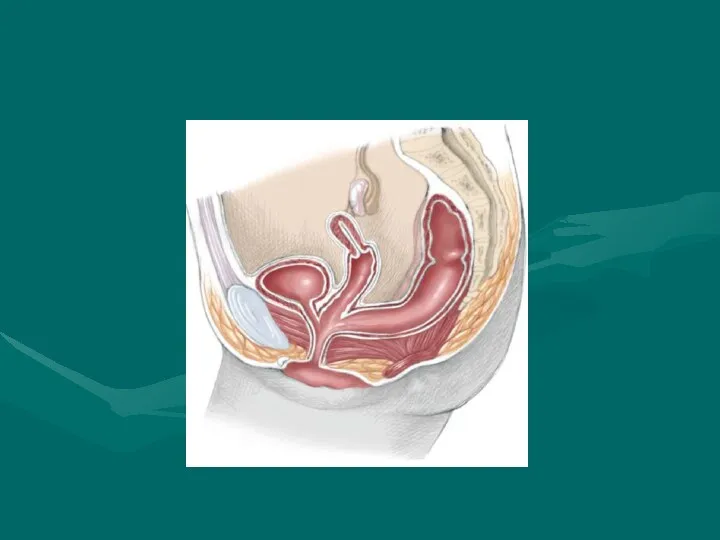
Cloaca.
A cloaca is defined as a malformation in which the rectum,
Cloaca.
A cloaca is defined as a malformation in which the rectum,
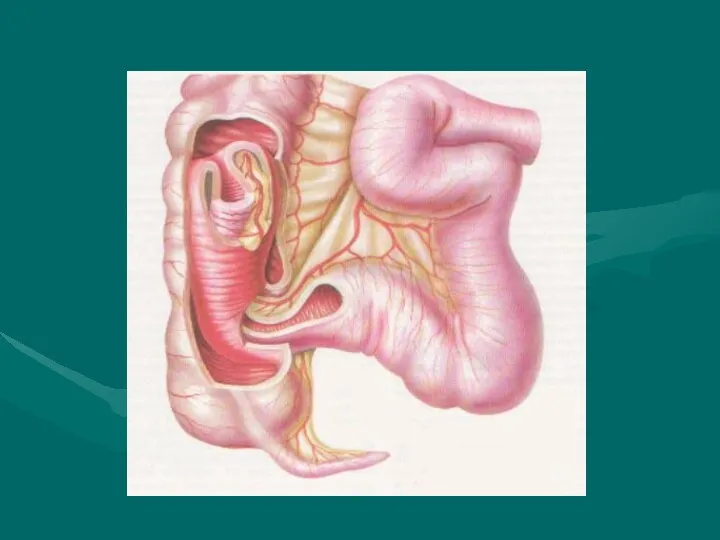
INTUSSUSCEPTION
INTUSSUSCEPTION
INTUSSUSCEPTION
DEFINITION
Telescoping of a proximal segment of the intestine (intussusceptum) into
INTUSSUSCEPTION
DEFINITION
Telescoping of a proximal segment of the intestine (intussusceptum) into
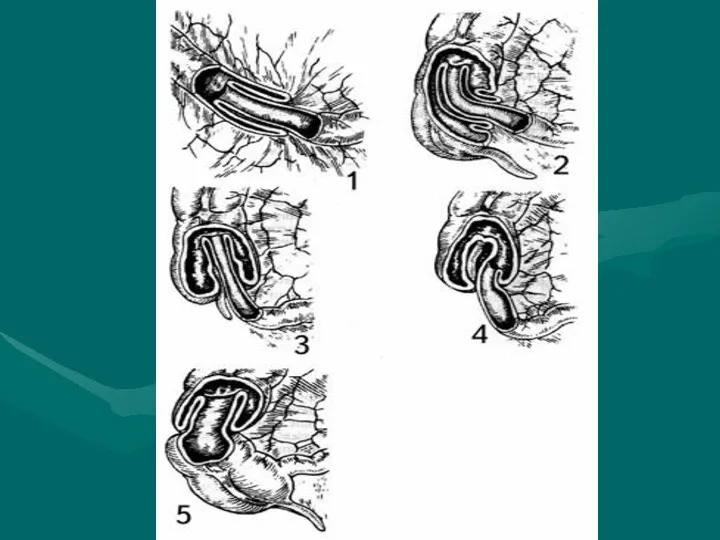
INTUSSUSCEPTION
ANATOMIC LOCATIONS
ILEOCOLIC
MOST COMMON IN CHILDREN
ILEO-ILEOCOLIC
SECOND MOST COMMON
ENTEROENTERIC
ILEO-ILEAL, JEJUNO-JEJUNAL
MORE COMMON IN
INTUSSUSCEPTION
ANATOMIC LOCATIONS
ILEOCOLIC
MOST COMMON IN CHILDREN
ILEO-ILEOCOLIC
SECOND MOST COMMON
ENTEROENTERIC
ILEO-ILEAL, JEJUNO-JEJUNAL
MORE COMMON IN
PATHOPHYSIOLOGY
Precipitating mechanism unknown
Obstruction of intussusceptum mesentery
Venous and lymphatic obstruction
Ischemic necrosis occurs
PATHOPHYSIOLOGY
Precipitating mechanism unknown
Obstruction of intussusceptum mesentery
Venous and lymphatic obstruction
Ischemic necrosis occurs
ETIOLOGIES
Majority of pediatric intussusceptions idiopathic (85-90%)
LYMPHOID HYPERPLASIA POSSIBLE ETIOLOGY
Mechanical abnormalities
ETIOLOGIES
Majority of pediatric intussusceptions idiopathic (85-90%)
LYMPHOID HYPERPLASIA POSSIBLE ETIOLOGY
Mechanical abnormalities
EPIDEMIOLOGY
Incidence 2 - 4 / 1000 live births
Usual age group
EPIDEMIOLOGY
Incidence 2 - 4 / 1000 live births
Usual age group
INTUSSUSCEPTION
CLINICAL CHARACTERISTICS
Early Symptoms
PAROXYSMAL ABDOMINAL PAIN
SEPARATED BY PERIODS OF APATHY
POOR FEEDING AND
INTUSSUSCEPTION
CLINICAL CHARACTERISTICS
Early Symptoms
PAROXYSMAL ABDOMINAL PAIN
SEPARATED BY PERIODS OF APATHY
POOR FEEDING AND
PHYSICAL EVALUATION
Moderately to severely ill
Irritable, limited movement
Most are at least
PHYSICAL EVALUATION
Moderately to severely ill
Irritable, limited movement
Most are at least
INTUSSUSCEPTION
STAGES
I. Bright clinical manifestation
II. Pseudodysenteric stage
III. Peritonitis
INTUSSUSCEPTION
STAGES
I. Bright clinical manifestation
II. Pseudodysenteric stage
III. Peritonitis
Ultrasonic diagnostics
Ultrasonic diagnostics
RADIOGRAPHIC EVALUATION
Plain radiographs (acute abdominal series)
Plain films suggestive in majority,
RADIOGRAPHIC EVALUATION
Plain radiographs (acute abdominal series)
Plain films suggestive in majority,

TREATMENT
Obstructive surgical emergency
Pediatric surgeon notified immediately
Supportive Therapy
AGGRESSIVE FLUID RESUSCITATION
ELECTROLYTES
NASOGASTRIC TUBE PLACEMENT
TREATMENT
Obstructive surgical emergency
Pediatric surgeon notified immediately
Supportive Therapy
AGGRESSIVE FLUID RESUSCITATION
ELECTROLYTES
NASOGASTRIC TUBE PLACEMENT
INTUSSUSCEPTION
PNEUMATIC REDUCTION
Theoretical Advantages
LESS INFLAMMATION IF PERFORATION OCCURS
Method
AIR INSUFFLATION LIMITED TO MAXIMUM
INTUSSUSCEPTION
PNEUMATIC REDUCTION
Theoretical Advantages
LESS INFLAMMATION IF PERFORATION OCCURS
Method
AIR INSUFFLATION LIMITED TO MAXIMUM
INTUSSUSCEPTION
NON-OPERATIVE REDUCTION CONTRAINDICATIONS
Absolute Contraindications
PERITONEAL SIGNS
SUSPECTED PERFORATION
Relative Contraindications
SYMPTOMS > 24-48 HRS
RECTAL
INTUSSUSCEPTION
NON-OPERATIVE REDUCTION CONTRAINDICATIONS
Absolute Contraindications
PERITONEAL SIGNS
SUSPECTED PERFORATION
Relative Contraindications
SYMPTOMS > 24-48 HRS
RECTAL
INTUSSUSCEPTION FAILURE OF NON-OPERATIVE REDUCTION
Factors associated with failure
SYMPTOMS > 48 HRS
RECTAL
INTUSSUSCEPTION FAILURE OF NON-OPERATIVE REDUCTION
Factors associated with failure
SYMPTOMS > 48 HRS
RECTAL
Acquired intestinal obstruction
Acquired intestinal obstructions are a partial or complete
Acquired intestinal obstruction
Acquired intestinal obstructions are a partial or complete
Intestinal obstructions can be mechanical or nonmechanical.
Mechanical obstruction is caused
Intestinal obstructions can be mechanical or nonmechanical.
Mechanical obstruction is caused
Clinic
1. Abdominal pain
2. Vomiting
3. Constipation
4. Intoxication syndrome
Clinic
1. Abdominal pain
2. Vomiting
3. Constipation
4. Intoxication syndrome
Diagnosis
X-ray examination
Ultrasonic diagnostics
Computed tomography
Diagnostic testing will include a complete blood
Diagnosis
X-ray examination
Ultrasonic diagnostics
Computed tomography
Diagnostic testing will include a complete blood
Treatment
Preoperative preparation:
a. inserting a nasogastric tube to suction out the
Treatment
Preoperative preparation:
a. inserting a nasogastric tube to suction out the
 Комбинаторные задачи в школьном курсе математики
Комбинаторные задачи в школьном курсе математики Презентация ВПК России
Презентация ВПК России Мы - за здоровый образ жизни!
Мы - за здоровый образ жизни! Воображение у детей дошкольного возраста в онтогенезе
Воображение у детей дошкольного возраста в онтогенезе Мир накануне Первой мировой войны. Индустриальная цивилизация в начале ХХ века
Мир накануне Первой мировой войны. Индустриальная цивилизация в начале ХХ века Знаем правила движения, как таблицу умножения
Знаем правила движения, как таблицу умножения Исправление нарушений произношения звука р
Исправление нарушений произношения звука р Презентация Мысли и поступки. Слова и речь, ОРКСЭ, урок № 24, к учебнику Шемшуриной А.(Дрофа), 4 класс
Презентация Мысли и поступки. Слова и речь, ОРКСЭ, урок № 24, к учебнику Шемшуриной А.(Дрофа), 4 класс Молодежній совет управления Росреестра по Тверской области. Итоги деятельности в 1 полугодии 2018
Молодежній совет управления Росреестра по Тверской области. Итоги деятельности в 1 полугодии 2018 Бутерброды и горячие напитки
Бутерброды и горячие напитки Человек Божий
Человек Божий Air Cargo Overview
Air Cargo Overview С праздником 8 марта
С праздником 8 марта Роль пейзажа в сказке К.Г. Паустовского Тёплый хлеб. Нравственные проблемы произведения
Роль пейзажа в сказке К.Г. Паустовского Тёплый хлеб. Нравственные проблемы произведения Символы моей Родины. ДНР
Символы моей Родины. ДНР Виды замков (по способу крепления)
Виды замков (по способу крепления) Организация работы среднего медицинского персонала в амбулаторно-поликлинических учреждениях
Организация работы среднего медицинского персонала в амбулаторно-поликлинических учреждениях Урок по ОРКСЭ (модуль основы светской этики) по теме Семья
Урок по ОРКСЭ (модуль основы светской этики) по теме Семья Презентация 13
Презентация 13 Интернет в жизни старшеклассника: за или против
Интернет в жизни старшеклассника: за или против Строительство малых мостов
Строительство малых мостов Обязательное страхование автогражданской ответственности (ОСАГО)
Обязательное страхование автогражданской ответственности (ОСАГО) Презентация к интегрированному занятию По следам невиданных животных
Презентация к интегрированному занятию По следам невиданных животных Пусть планета будет чистой. Проблема бытового мусора
Пусть планета будет чистой. Проблема бытового мусора Геморрой
Геморрой Определённый артикль. Неопределённый артикль. Нулевой артикль
Определённый артикль. Неопределённый артикль. Нулевой артикль Система работы с одарёнными детьми
Система работы с одарёнными детьми Франция на пути к абсолютизму
Франция на пути к абсолютизму