- Idiopathic (Immune) Thrombocytopenic Purpura

Содержание
- 2. Idiopathic (Immune) Thrombocytopenic Purpura Thrombocytopenia in the absence of other blood cell abnormalities (normal RBC &
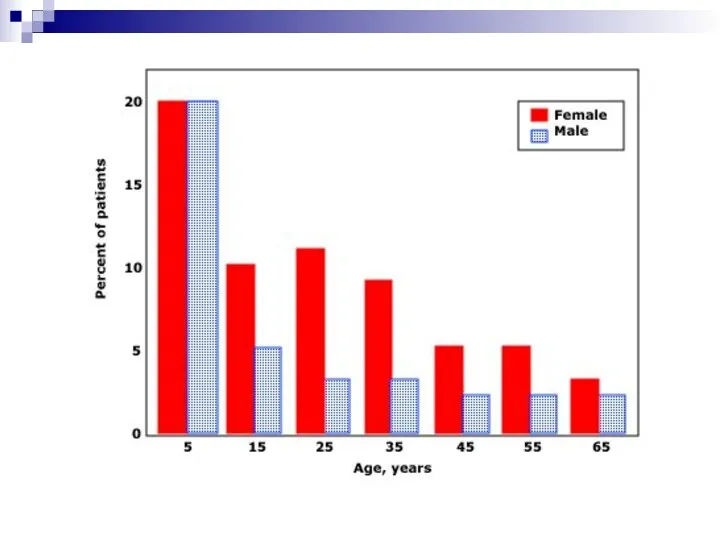
- 3. Statistics of ITP Incidence of 22 million/year in one study Prevalence greater as often chronic *Segal
- 5. Clinical Manifestations May be acute or insidious onset Mucocutaneous Bleeding *petechiae, purpura, ecchymosis *epistaxis, gum bleeding
- 8. Etiology of ITP : Children Often after infection (viral or bacterial) Theories: *antibody cross-reactivity *H. pylori
- 9. Diagnosis (of Exclusion) Rule out other causes: *lab error / PLT clumping *drug / medication interaction
- 10. Diagnosis (of Exclusion) Rule out other causes: *lab error / PLT clumping *drug / medication interaction
- 11. To Marrow or Not to Marrow? Bone marrow aspiration & biopsy if… Patient 60 yrs. or
- 12. Anti-Platelet Antibody Testing NOT recommended by ASH Practice Guidelines Poor positive/negative predictive values, poor sensitivity with
- 13. Management of ITP Goal = prevention of bleeding, NOT cure!
- 14. General Principles of Therapy Major bleeding rare if PLT > 10,000 Goal = get PLT count
- 15. “Safe” Platelet Counts “moderately” t-penic = 30-50,000 Probably safe if asymptomatic Caution with elderly (CNS bleeds)
- 16. When Planning Therapy… Tailor therapy and decision to treat to the individual patient Weigh bleeding vs.
- 17. Initial Therapy Prednisone 1 mg/kg/day *usually response within 2 weeks Taper off after PLT response Duration
- 18. Second-Line Therapy IV Immune Globulin (IVIg) 1 gram/kg/day x 2 days WinRho (anti-D) – if pt
- 19. Treatment Side-Effects Steroids *bone density loss *GI effects *muscle weakness *weight gain IVIG/anti-D *hypersensitivity *headache *renal
- 20. Splenectomy Usually reserved for treatment failure Consider risk of bleeding, pt lifestyle RISKS *surgical procedure *loss
- 21. Data from George, JN, Woolf, SH, Raskob, GE, et al. Blood 1996; 88:3. When to do
- 22. Response Post-Splenectomy Usually normalized PLTs within 2 weeks (often immediately) Younger pts do better Kojouri et
- 23. Data from Fabris, F, et al. Br J Haematol 2001; 112:637.
- 24. Chronic Refractory ITP Persistent > 3 months PLT Failure to respond to splenectomy
- 25. When all else fails… Steroids IVIg / anti-D Rituximab (anti-CD20) Cyclophosphamide Danazol Accessory splenectomy H. pylori
- 26. Wrapping it up… ITP is often a chronic disease in adults Multiple therapies may be needed
- 29. Скачать презентацию
Idiopathic (Immune) Thrombocytopenic Purpura
Thrombocytopenia in the absence of other blood cell
Idiopathic (Immune) Thrombocytopenic Purpura
Thrombocytopenia in the absence of other blood cell
Statistics of ITP
Incidence of 22 million/year in one study
Prevalence greater as
Statistics of ITP
Incidence of 22 million/year in one study
Prevalence greater as
Clinical Manifestations
May be acute or insidious onset
Mucocutaneous Bleeding
*petechiae, purpura, ecchymosis
Clinical Manifestations
May be acute or insidious onset
Mucocutaneous Bleeding
*petechiae, purpura, ecchymosis


Etiology of ITP : Children
Often after infection (viral or bacterial)
Theories:
*antibody
Etiology of ITP : Children
Often after infection (viral or bacterial)
Theories:
*antibody
Diagnosis (of Exclusion)
Rule out other causes:
*lab error / PLT clumping
Diagnosis (of Exclusion)
Rule out other causes:
*lab error / PLT clumping
Diagnosis (of Exclusion)
Rule out other causes:
*lab error / PLT clumping
Diagnosis (of Exclusion)
Rule out other causes:
*lab error / PLT clumping
To Marrow or Not to Marrow?
Bone marrow aspiration & biopsy if…
Patient
To Marrow or Not to Marrow?
Bone marrow aspiration & biopsy if…
Patient
Anti-Platelet Antibody Testing
NOT recommended by ASH Practice Guidelines
Poor positive/negative predictive values,
Anti-Platelet Antibody Testing
NOT recommended by ASH Practice Guidelines
Poor positive/negative predictive values,
Management of ITP
Goal = prevention of bleeding, NOT cure!
Management of ITP
Goal = prevention of bleeding, NOT cure!
General Principles of Therapy
Major bleeding rare if PLT > 10,000
Goal =
General Principles of Therapy
Major bleeding rare if PLT > 10,000
Goal =
“Safe” Platelet Counts
“moderately” t-penic = 30-50,000
Probably safe if asymptomatic
Caution with elderly
“Safe” Platelet Counts
“moderately” t-penic = 30-50,000
Probably safe if asymptomatic
Caution with elderly
When Planning Therapy…
Tailor therapy and decision to treat to the individual
When Planning Therapy…
Tailor therapy and decision to treat to the individual
Initial Therapy
Prednisone 1 mg/kg/day
*usually response within 2 weeks
Taper off after
Initial Therapy
Prednisone 1 mg/kg/day
*usually response within 2 weeks
Taper off after
Second-Line Therapy
IV Immune Globulin (IVIg)
1 gram/kg/day x 2 days
WinRho (anti-D)
Second-Line Therapy
IV Immune Globulin (IVIg)
1 gram/kg/day x 2 days
WinRho (anti-D)
Treatment Side-Effects
Steroids
*bone density loss *GI effects
*muscle weakness *weight gain
IVIG/anti-D
Treatment Side-Effects
Steroids
*bone density loss *GI effects
*muscle weakness *weight gain
IVIG/anti-D
Splenectomy
Usually reserved for treatment failure
Consider risk of bleeding, pt lifestyle
RISKS
*surgical
Splenectomy
Usually reserved for treatment failure
Consider risk of bleeding, pt lifestyle
RISKS
*surgical
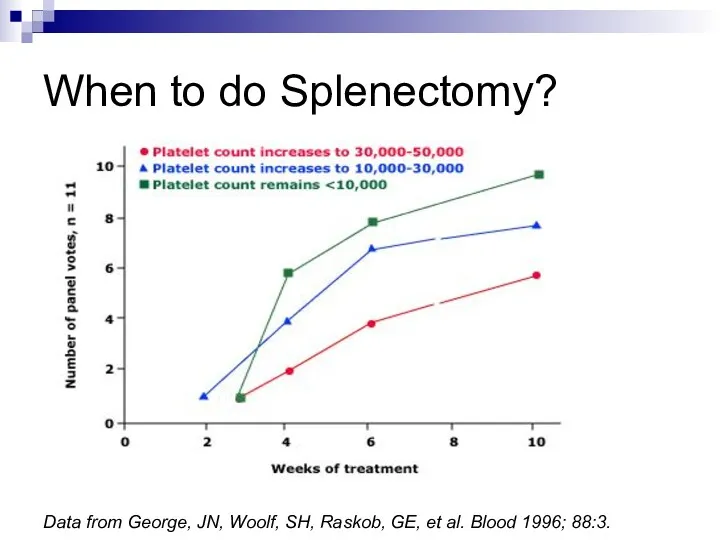
Data from George, JN, Woolf, SH, Raskob, GE, et al. Blood
Data from George, JN, Woolf, SH, Raskob, GE, et al. Blood
Response Post-Splenectomy
Usually normalized PLTs within 2 weeks (often immediately)
Younger pts do
Response Post-Splenectomy
Usually normalized PLTs within 2 weeks (often immediately)
Younger pts do
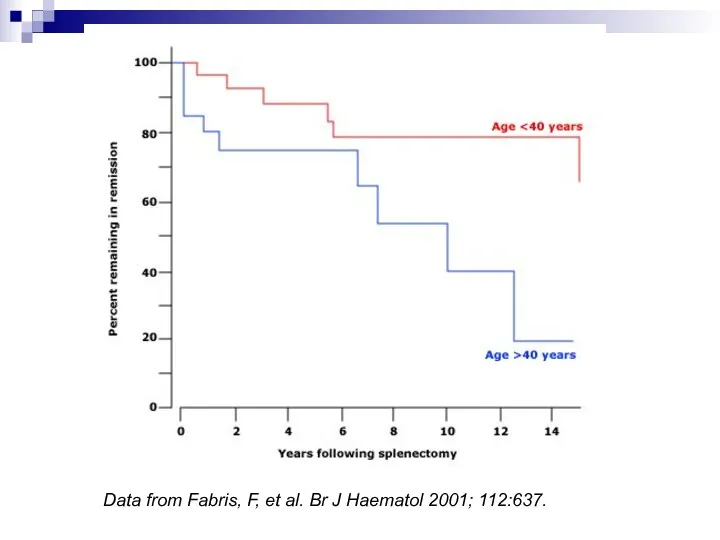
Data from Fabris, F, et al. Br J Haematol 2001; 112:637.
Data from Fabris, F, et al. Br J Haematol 2001; 112:637.
Chronic Refractory ITP
Persistent > 3 months
PLT < 50,000
Failure to respond to
Chronic Refractory ITP
Persistent > 3 months
PLT < 50,000
Failure to respond to
When all else fails…
Steroids
IVIg / anti-D
Rituximab (anti-CD20)
Cyclophosphamide
Danazol
Accessory splenectomy
H. pylori eradication
When all else fails…
Steroids
IVIg / anti-D
Rituximab (anti-CD20)
Cyclophosphamide
Danazol
Accessory splenectomy
H. pylori eradication
Wrapping it up…
ITP is often a chronic disease in adults
Multiple therapies
Wrapping it up…
ITP is often a chronic disease in adults
Multiple therapies

 Художники-пейзажисты
Художники-пейзажисты Технологии рефлексии в педагогическом процессе
Технологии рефлексии в педагогическом процессе Послідовне з’єднання провідників
Послідовне з’єднання провідників Мавзу. Жамият тараккиётининг гоя ва Мафкура Билан ўзаро богликлиги
Мавзу. Жамият тараккиётининг гоя ва Мафкура Билан ўзаро богликлиги Алюминий
Алюминий Каталог дидактическ игр по нравственно- патриотическому воспитанию детей дошкольного возраста
Каталог дидактическ игр по нравственно- патриотическому воспитанию детей дошкольного возраста Коммунальные ресурсы на общедомовые нужды
Коммунальные ресурсы на общедомовые нужды How to Introduce Yourself in English. Как рассказать о себе на англ.языке
How to Introduce Yourself in English. Как рассказать о себе на англ.языке FinFactor. Решение кейса от Changellenge
FinFactor. Решение кейса от Changellenge Урок Периодический закон Д.И. Менделеева 9 класс.
Урок Периодический закон Д.И. Менделеева 9 класс. Первая оценка и как к ней относится
Первая оценка и как к ней относится Презентация Одаренные дети
Презентация Одаренные дети Презентация Познавательно - исследовательская деятельность детей старшего дошкольного возраста
Презентация Познавательно - исследовательская деятельность детей старшего дошкольного возраста Хирургическая анатомия суставов
Хирургическая анатомия суставов ВКР: Имидж гостиничного предприятия (планирование, формирование, продвижение)
ВКР: Имидж гостиничного предприятия (планирование, формирование, продвижение) Музыкально - дидактическая игра Угадай, на чём играю?
Музыкально - дидактическая игра Угадай, на чём играю? Матрицы. Свойства операций над матрицами. Теорема о ранге матрицы
Матрицы. Свойства операций над матрицами. Теорема о ранге матрицы Применение смазочно-охлаждающих жидкостей (СОЖ)
Применение смазочно-охлаждающих жидкостей (СОЖ) Логопедическое занятие-игра. Драматизация сказки Репка Тема: Слоговой анализ и синтез
Логопедическое занятие-игра. Драматизация сказки Репка Тема: Слоговой анализ и синтез  Внеурочная и проектная деятельность учащихся
Внеурочная и проектная деятельность учащихся Часть 2. Фотоотчёт. Дорогою Добра.Летний городской лагерь.
Часть 2. Фотоотчёт. Дорогою Добра.Летний городской лагерь. Герб Санкт-Петербурга
Герб Санкт-Петербурга 20231022_dif._podhod
20231022_dif._podhod История туризма и гостеприимства
История туризма и гостеприимства Модернизация устройства РЗиА на электрической подстанции 110/35/10 кВ
Модернизация устройства РЗиА на электрической подстанции 110/35/10 кВ Ясли-это серьезно!
Ясли-это серьезно! Пристрої компютера. Фотоальбом
Пристрої компютера. Фотоальбом Роль религии в жизни общества
Роль религии в жизни общества