- Origin, differential diagnosis and thrapy of jaundices in neonates

Содержание
- 2. Hemoglobin Myoglobin Hem-contained Enzymes and pyrrols Hb+albumin DGB MGB Isomers of UB Vena cava inferior Hepatic
- 3. Catabolism of heme to bilirubin by microsomal heme oxygenase and biliverdin reductase. (From Tenhunen R et
- 4. The pathways of bilirubin synthesis, transport, and metabolism. Hgb, hemoglobin; RBCs, red blood cells. (From Assali
- 5. Mean total serum bilirubin (TSB) concentrations in 22 full-term normal white and African-American infants during the
- 6. Developmental pattern of hepatic bilirubin uridine diphosphoglucuronate glucuronosyltransferase (UGT) activity in humans. (From Kawade N, Onishi
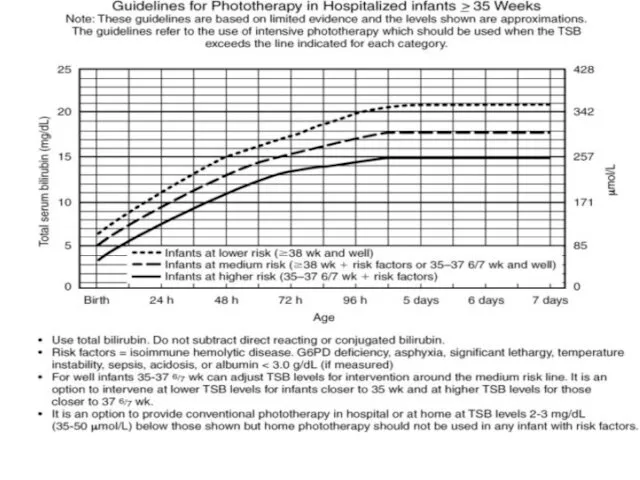
- 7. Zones of risk for pathologic hyperbilirubinemia based on hour-specific serum bilirubin levels. (From Bhutani VK et
- 8. Healthy state Conjugated jaundice Hemolytic jaundice Parenchymatouse jaundice Mechanic jaundice НБ GlA GT GA GT UB
- 9. Hour-specific bilirubin nomogram with the predictive ability of the predischarge bilirubin value for subsequent severe hyperbilirubinemia,
- 10. Clinical and serologic differences of hemolytic disease among ABO and Rh sensibilisation 1. a - и
- 11. The basic principles of change blood transfusion. 1.The tip of correctly fixed umbilical vein catheter must
- 12. Indication for change blood transfusion 0 5 10 15 25 20 24 48 72 96 120
- 16. Скачать презентацию
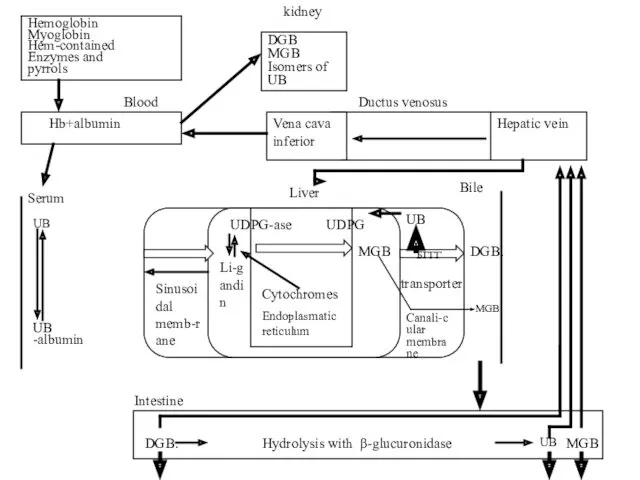
Hemoglobin
Myoglobin
Hem-contained
Enzymes and
pyrrols
Hb+albumin
DGB
MGB
Isomers of
UB
Vena cava inferior
Hepatic vein
DGB.
UB
MGB
MGB
DGB.
MGB
Ductus venosus
Liver
Bile
Serum
UB
UB -albumin
Hydrolysis with β-glucuronidase
БГГГ
UB
UDPG
UDPG-ase
Li-gandin
Sinusoidal memb-rane
transporter
Canali-cular
Hemoglobin
Myoglobin
Hem-contained
Enzymes and
pyrrols
Hb+albumin
DGB
MGB
Isomers of
UB
Vena cava inferior
Hepatic vein
DGB.
UB
MGB
MGB
DGB.
MGB
Ductus venosus
Liver
Bile
Serum
UB
UB -albumin
Hydrolysis with β-glucuronidase
БГГГ
UB
UDPG
UDPG-ase
Li-gandin
Sinusoidal memb-rane
transporter
Canali-cular
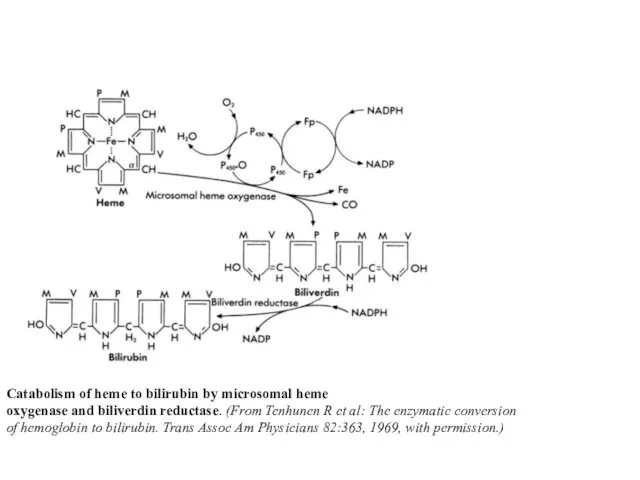
Catabolism of heme to bilirubin by microsomal heme
oxygenase and biliverdin
Catabolism of heme to bilirubin by microsomal heme
oxygenase and biliverdin
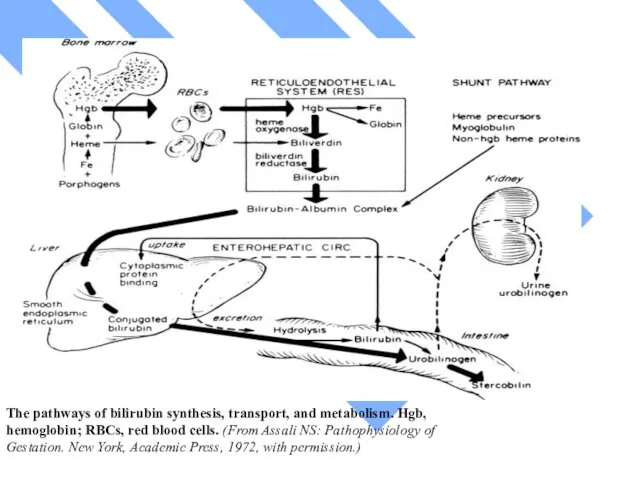
The pathways of bilirubin synthesis, transport, and metabolism. Hgb, hemoglobin; RBCs,
The pathways of bilirubin synthesis, transport, and metabolism. Hgb, hemoglobin; RBCs,
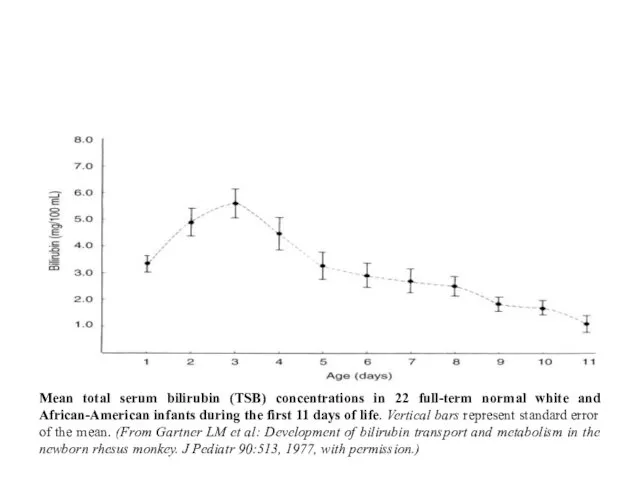
Mean total serum bilirubin (TSB) concentrations in 22 full-term normal white
Mean total serum bilirubin (TSB) concentrations in 22 full-term normal white
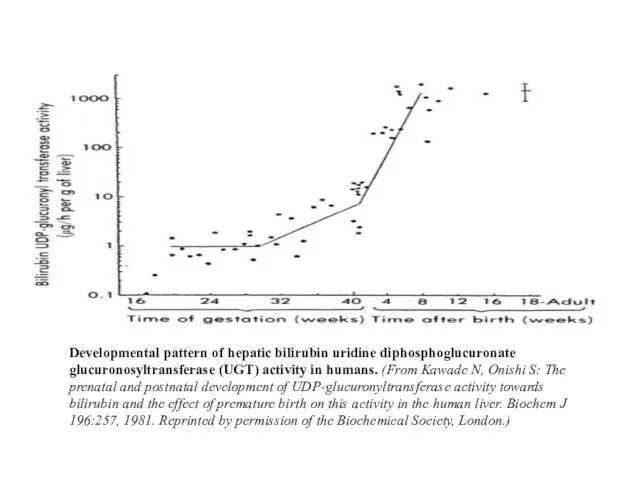
Developmental pattern of hepatic bilirubin uridine diphosphoglucuronate glucuronosyltransferase (UGT) activity in
Developmental pattern of hepatic bilirubin uridine diphosphoglucuronate glucuronosyltransferase (UGT) activity in
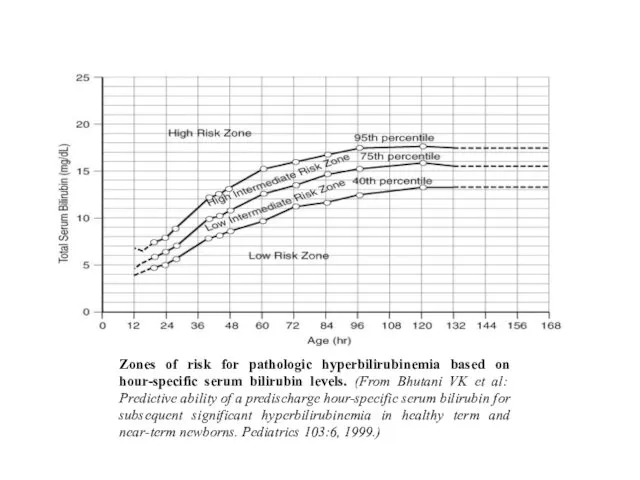
Zones of risk for pathologic hyperbilirubinemia based on hour-specific serum bilirubin
Zones of risk for pathologic hyperbilirubinemia based on hour-specific serum bilirubin
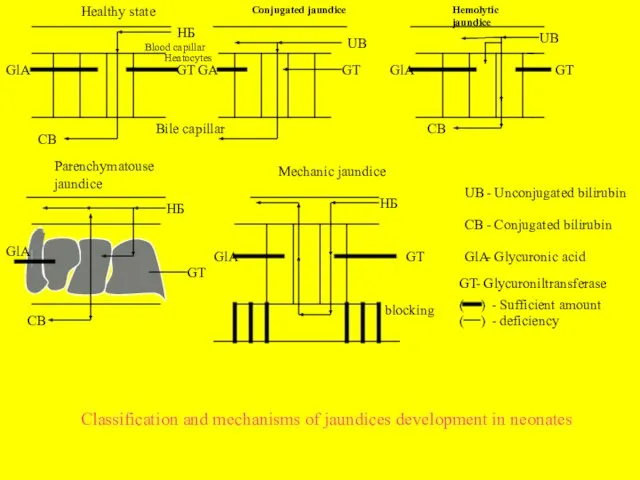
Healthy state
Conjugated jaundice
Hemolytic jaundice
Parenchymatouse jaundice
Mechanic jaundice
НБ
GlA
GT
GA
GT
UB
UB
НБ
НБ
GlA
GlA
GlA
GT
GT
GT
CB
CB
CB
Blood capillar
Heatocytes
Bile capillar
UB
CB
GlA
GT
(
(
)
)
blocking
- Unconjugated bilirubin
- Conjugated
Healthy state
Conjugated jaundice
Hemolytic jaundice
Parenchymatouse jaundice
Mechanic jaundice
НБ
GlA
GT
GA
GT
UB
UB
НБ
НБ
GlA
GlA
GlA
GT
GT
GT
CB
CB
CB
Blood capillar
Heatocytes
Bile capillar
UB
CB
GlA
GT
(
(
)
)
blocking
- Unconjugated bilirubin
- Conjugated
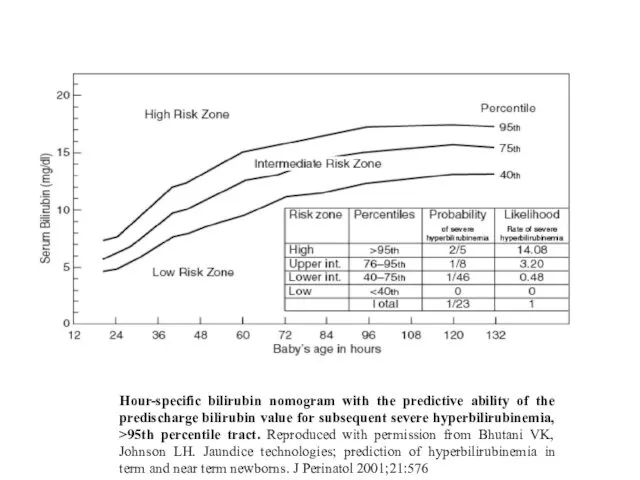
Hour-specific bilirubin nomogram with the predictive ability of the predischarge bilirubin
Hour-specific bilirubin nomogram with the predictive ability of the predischarge bilirubin
Clinical and serologic differences of hemolytic disease among ABO and Rh
Clinical and serologic differences of hemolytic disease among ABO and Rh
The basic principles of change blood transfusion.
1.The tip of correctly fixed
The basic principles of change blood transfusion.
1.The tip of correctly fixed
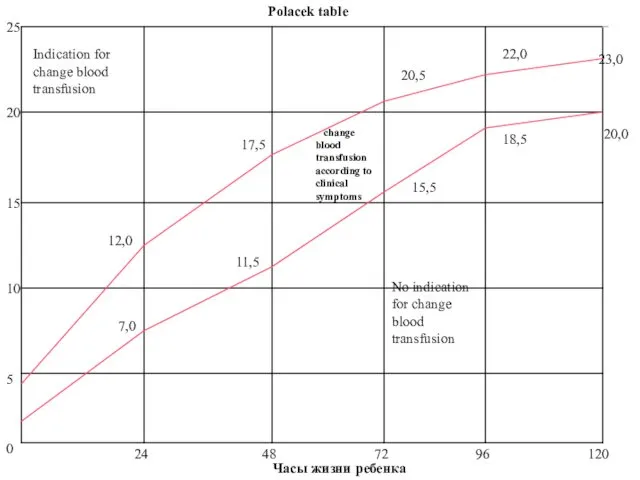
Indication for change blood transfusion
0
5
10
15
25
20
24
48
72
96
120
7,0
12,0
11,5
17,5
20,5
15,5
22,0
18,5
23,0
20,0
change blood transfusion according to clinical
Indication for change blood transfusion
0
5
10
15
25
20
24
48
72
96
120
7,0
12,0
11,5
17,5
20,5
15,5
22,0
18,5
23,0
20,0
change blood transfusion according to clinical
 Технико-экономический анализ деятельности Свердловской дистанции электроснабжения. Разработка мероприятий по снижению издержек
Технико-экономический анализ деятельности Свердловской дистанции электроснабжения. Разработка мероприятий по снижению издержек Нравственная культура личности
Нравственная культура личности Треугольник. Равенство и подобие треугольников
Треугольник. Равенство и подобие треугольников 1_fevralya_dlya_DO
1_fevralya_dlya_DO Скульптура первой половины XIX века
Скульптура первой половины XIX века Основы физиологии труда и комфортные условия жизнедеятельности
Основы физиологии труда и комфортные условия жизнедеятельности презентация к курсу История и культура Санкт- Петербурга
презентация к курсу История и культура Санкт- Петербурга Мультимедийная викторина Природа родного края
Мультимедийная викторина Природа родного края Эталоны единиц величин бесконтактных средств измерений температуры
Эталоны единиц величин бесконтактных средств измерений температуры Разминки-пятиминутки
Разминки-пятиминутки Формирование универсальных учебных действий на уроках в начальной школе
Формирование универсальных учебных действий на уроках в начальной школе Завершающий период Великой Отечественной войны
Завершающий период Великой Отечественной войны Сүйек-буын туберкулезі
Сүйек-буын туберкулезі Презентация: Стихийные природные явления России
Презентация: Стихийные природные явления России Чрезвычайные ситуации экологического характера
Чрезвычайные ситуации экологического характера Архітектура комп'ютера
Архітектура комп'ютера Социально-коммуникативное развитие НОД Путешествие в весенний лес-1 младшая группа
Социально-коммуникативное развитие НОД Путешествие в весенний лес-1 младшая группа Урок географии в 7 классе коррекционной школы VIII вида на тему Животный мир тундры
Урок географии в 7 классе коррекционной школы VIII вида на тему Животный мир тундры Wall Calendar 2017: NASA
Wall Calendar 2017: NASA Оздоровительная физическая культура и ее формы. Влияние оздоровительной физической культуры на организм человека
Оздоровительная физическая культура и ее формы. Влияние оздоровительной физической культуры на организм человека Презентации к урокам
Презентации к урокам Правила поведения за столом. Занятие 1.
Правила поведения за столом. Занятие 1. Презентация Метод учебного проекта
Презентация Метод учебного проекта Новый фитнес с бассейном
Новый фитнес с бассейном Древний Китай
Древний Китай Lubrication
Lubrication Административный центр Уральского федерального округа Екатеринбург
Административный центр Уральского федерального округа Екатеринбург Окислительно-восстановительные процессы и реакции
Окислительно-восстановительные процессы и реакции