- Traumatic shock

Содержание
- 2. DEFINITION Shock it is a severe disturbance of hemodynamic in which the circulatory system fails to
- 3. SHOCK IN TRAUMA Classification Hypovolemic Distributive Cardiogenic
- 4. HYPOVOLEMIC SHOCK MOST COMMON CAUSE OF SHOCK IN THE TRAUMA PATIENT DUE TO HEMORRHAGE ( LOSS
- 5. DISTRIBUTIVE SHOCK NEUROGENIC SHOCK DECREASED SYSTEMIC VASCULAR RESISTANCE DUE TO VASODILATION MOST COMMON CAUSE IN SPINAL
- 6. CARDIOGENIC SHOCK INTRINSIC BLUNT CARDIAC TRAUMA LEADING TO MUSCLE DAMAGE AND DYSRHYTHMIA VALVULAR DISCRUPTION EXTRINSIC PERICARDIAL
- 7. TRAUMATIC SHOCK MECHANISM Microcirculation –Systemic vascular resistance rises to maintain a level of systemic pressure that
- 8. TRAUMATIC SHOCK MECHANISM Cellular response –Decline of intracellular high energy phosphate stores (decreased amount of ATP)
- 9. TRAUMATIC SHOCK MECHANISM Cardiovascular response –Decreased ventricular filling (decreased preload). The increased heart rate is a
- 10. TRAUMATIC SHOCK MECHANISM Pulmonary response –Increased pulmonary vascular resistance (particularly in septic shock) –Tachypnoe, but restricted
- 11. TRAUMATIC SHOCK MECHANISM Renal response –Consequences of hypo perfusion: reduced renal blood flow, increased afferent arteriolar
- 12. TRAUMATIC SHOCK MECHANISM Inflammatory responses –Activation of an extensive network of proinflammatory mediator systems plays a
- 13. CLINICAL MANIFESTATION PRESENCE OF PERIPHERAL AND PULMONARY EDEMA INFUSION OF LARGE VOLUME FLUID WHICH MAY BE
- 14. TREATMENT AND MANAGEMENT PRE-HOSPITAL CARE: EXTERNAL BLEEDING SHOULD BE CONTROLLED BY DIRECT PRESSURE IMMOBILIZATION PATIENT SECURING
- 16. Скачать презентацию
DEFINITION
Shock it is a severe disturbance of hemodynamic in which the
DEFINITION
Shock it is a severe disturbance of hemodynamic in which the
SHOCK IN TRAUMA
Classification
Hypovolemic
Distributive
Cardiogenic
SHOCK IN TRAUMA
Classification
Hypovolemic
Distributive
Cardiogenic
HYPOVOLEMIC SHOCK
MOST COMMON CAUSE OF SHOCK IN THE TRAUMA PATIENT
DUE TO
HYPOVOLEMIC SHOCK
MOST COMMON CAUSE OF SHOCK IN THE TRAUMA PATIENT
DUE TO
DISTRIBUTIVE SHOCK
NEUROGENIC SHOCK
DECREASED SYSTEMIC VASCULAR RESISTANCE DUE TO VASODILATION
MOST
DISTRIBUTIVE SHOCK
NEUROGENIC SHOCK
DECREASED SYSTEMIC VASCULAR RESISTANCE DUE TO VASODILATION
MOST
CARDIOGENIC SHOCK
INTRINSIC
BLUNT CARDIAC TRAUMA LEADING TO MUSCLE DAMAGE AND DYSRHYTHMIA
VALVULAR DISCRUPTION
EXTRINSIC
CARDIOGENIC SHOCK
INTRINSIC
BLUNT CARDIAC TRAUMA LEADING TO MUSCLE DAMAGE AND DYSRHYTHMIA
VALVULAR DISCRUPTION
EXTRINSIC
TRAUMATIC SHOCK MECHANISM
Microcirculation –Systemic vascular resistance rises to maintain a
TRAUMATIC SHOCK MECHANISM
Microcirculation –Systemic vascular resistance rises to maintain a
TRAUMATIC SHOCK MECHANISM
Cellular response –Decline of intracellular high energy phosphate
TRAUMATIC SHOCK MECHANISM
Cellular response –Decline of intracellular high energy phosphate
TRAUMATIC SHOCK MECHANISM
Cardiovascular response –Decreased ventricular filling (decreased preload). The
TRAUMATIC SHOCK MECHANISM
Cardiovascular response –Decreased ventricular filling (decreased preload). The
TRAUMATIC SHOCK MECHANISM
Pulmonary response –Increased pulmonary vascular resistance (particularly in
TRAUMATIC SHOCK MECHANISM
Pulmonary response –Increased pulmonary vascular resistance (particularly in
TRAUMATIC SHOCK MECHANISM
Renal response –Consequences of hypo perfusion: reduced renal
TRAUMATIC SHOCK MECHANISM
Renal response –Consequences of hypo perfusion: reduced renal
TRAUMATIC SHOCK MECHANISM
Inflammatory responses –Activation of an extensive network of
TRAUMATIC SHOCK MECHANISM
Inflammatory responses –Activation of an extensive network of
CLINICAL MANIFESTATION
PRESENCE OF PERIPHERAL AND PULMONARY EDEMA
INFUSION OF LARGE
CLINICAL MANIFESTATION
PRESENCE OF PERIPHERAL AND PULMONARY EDEMA
INFUSION OF LARGE
TREATMENT AND MANAGEMENT
PRE-HOSPITAL CARE:
EXTERNAL BLEEDING SHOULD BE CONTROLLED BY DIRECT PRESSURE
TREATMENT AND MANAGEMENT
PRE-HOSPITAL CARE:
EXTERNAL BLEEDING SHOULD BE CONTROLLED BY DIRECT PRESSURE
 Презентация Мой класс- это мое отражение
Презентация Мой класс- это мое отражение Времена группы Continuous
Времена группы Continuous Произведения М.Ю. Лермонтова в творчестве М. Врубеля
Произведения М.Ю. Лермонтова в творчестве М. Врубеля Вейвлеты при анализе скважинных данных
Вейвлеты при анализе скважинных данных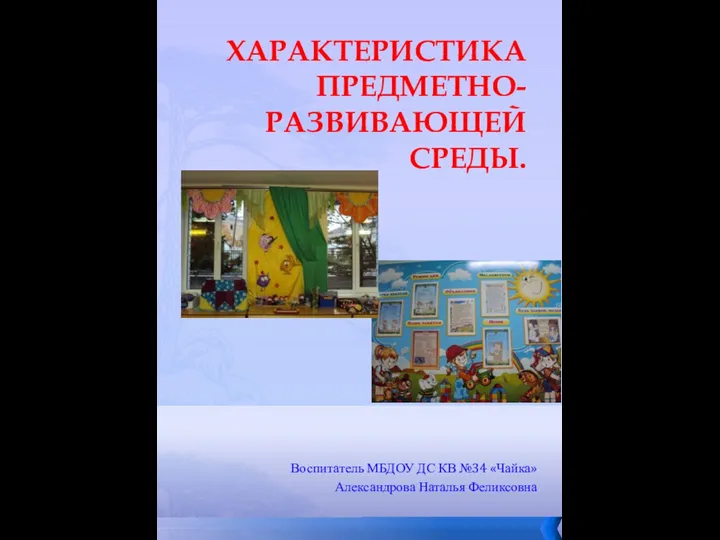 Отчет о создании развивающей среды.
Отчет о создании развивающей среды. Антуан де Сент-Экзюпери
Антуан де Сент-Экзюпери Автоматизация смешения светлых нефтепродуктов
Автоматизация смешения светлых нефтепродуктов Купола над белым безмолвием.
Купола над белым безмолвием. Искусство 16 века в Нидерландах и Германии. (Тема 7)
Искусство 16 века в Нидерландах и Германии. (Тема 7) Творческий проект здоровые зубы - всякому любы
Творческий проект здоровые зубы - всякому любы Будущий мужчина, или Как правильно воспитывать мальчика (консультация для родителей)
Будущий мужчина, или Как правильно воспитывать мальчика (консультация для родителей) Графический интерфейс операционных систем
Графический интерфейс операционных систем Игра Подбери одежду по сезону
Игра Подбери одежду по сезону Колокола в музыке
Колокола в музыке Тема 1. Место и роль вооруженных сил Российской Федерации в структуре государства
Тема 1. Место и роль вооруженных сил Российской Федерации в структуре государства Хищные звери
Хищные звери Лекция 5__
Лекция 5__ Скульпту́ра. Объект изображения в скульптуре
Скульпту́ра. Объект изображения в скульптуре Значение и употребление глаголов в речи
Значение и употребление глаголов в речи Асептика и антисептика
Асептика и антисептика ВКР: Проект мини-цеха производства колбасных изделий и полуфабрикатов мощностью 1,5 т/смену
ВКР: Проект мини-цеха производства колбасных изделий и полуфабрикатов мощностью 1,5 т/смену Оригами Сонобе
Оригами Сонобе Презентация по технологии Портрет в сырной рамке
Презентация по технологии Портрет в сырной рамке Москва во главе объединения русских земель
Москва во главе объединения русских земель Шаблон Россия
Шаблон Россия Разработка проекта наладки РТК на базе станка с ЧПУ на обработку детали Шестерня VIII оси 1к62-02-119
Разработка проекта наладки РТК на базе станка с ЧПУ на обработку детали Шестерня VIII оси 1к62-02-119 Мое портфолио Диск Диск
Мое портфолио Диск Диск 20002
20002