- Try-in and correction of the PRD. Remodeling and repair of removable dentures

Содержание
- 2. Content Try-in and correction of the PRD. Remodeling of denture Repair of removable dentures. Prosthetic stomatitis.
- 3. Try-in and correction of the PRD. Doctor have to evaluate: the quality of polishing, faults after
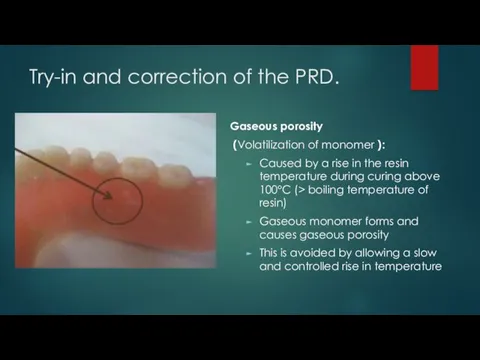
- 4. Try-in and correction of the PRD. Gaseous porosity (Volatilization of monomer ): Caused by a rise
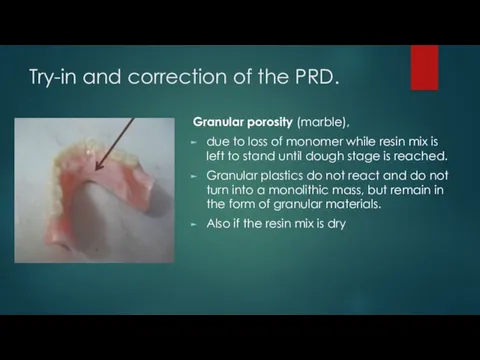
- 5. Try-in and correction of the PRD. Granular porosity (marble), due to loss of monomer while resin
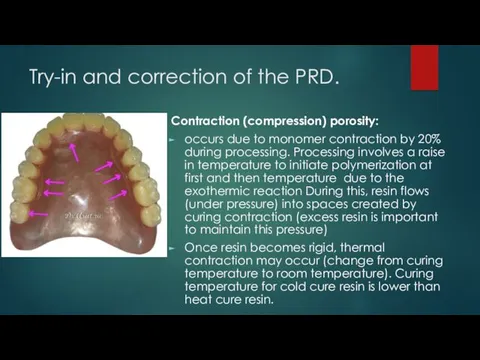
- 6. Try-in and correction of the PRD. Contraction (compression) porosity: occurs due to monomer contraction by 20%
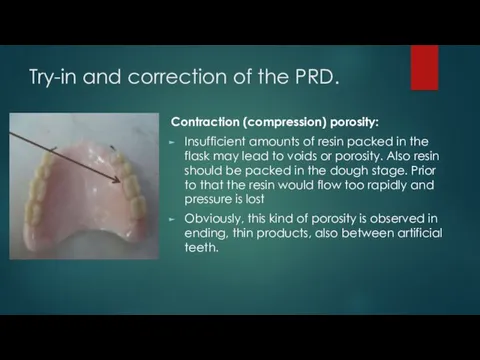
- 7. Try-in and correction of the PRD. Contraction (compression) porosity: Insufficient amounts of resin packed in the
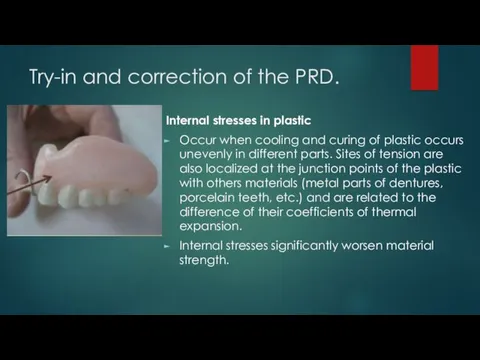
- 8. Try-in and correction of the PRD. Internal stresses in plastic Occur when cooling and curing of
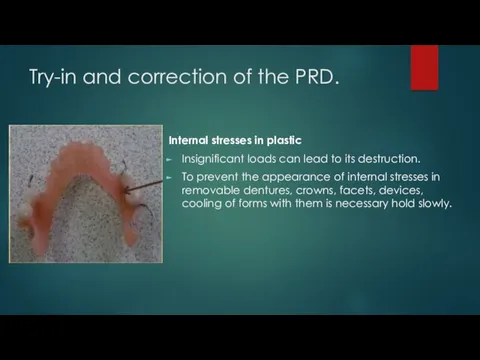
- 9. Try-in and correction of the PRD. Internal stresses in plastic Insignificant loads can lead to its
- 10. Relining of denture Relining and rebasingrelining is the resurfacing of the tissue surface of a denture
- 11. Relining of denture Relining - recreation of the inner surface of the denture. One that lies
- 12. Relining of denture When else is the doctor doing a soft reassignment? - If exostoses or
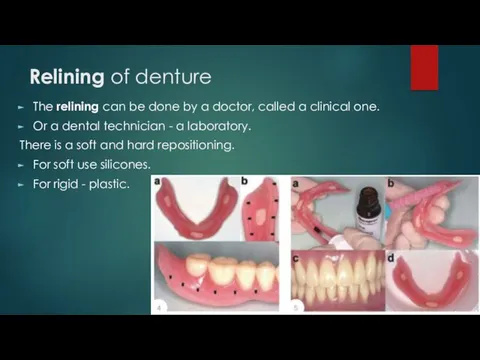
- 13. Relining of denture The relining can be done by a doctor, called a clinical one. Or
- 14. Relining of denture Why is laboratory relocation better than clinical? The technician uses hot polymerization plastic,
- 15. Relining of denture But, there are methods of temporary clinical relining. When you need to cure
- 16. Repair of removable dentures. Reasons: Poorly made (poorly constructed). The patient mechanically break. The lifetime of
- 17. Repair of removable dentures. Other causes of denture fracture 1. Deep labial frenal notch
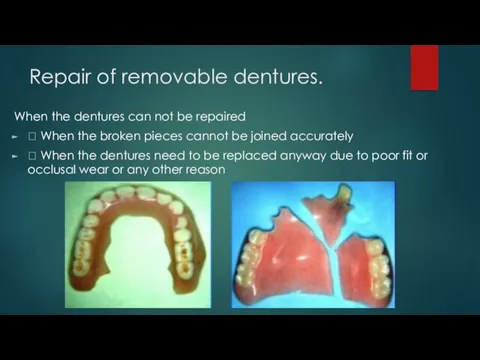
- 18. Repair of removable dentures. When the dentures can not be repaired When the broken pieces
- 19. Repair of removable dentures. Types Of materials used in repairs 1.Chemical-Cured acrylic 2.Visible Light Cured (VLC)
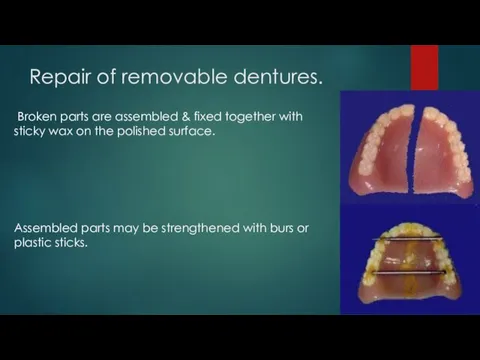
- 20. Repair of removable dentures. Broken parts are assembled & fixed together with sticky wax on the
- 21. Repair of removable dentures. Any undercut on the fitting surface is blocked out with wax or
- 22. Repair of removable dentures. Fractured edges are widened along the fracture line and beveled towards the
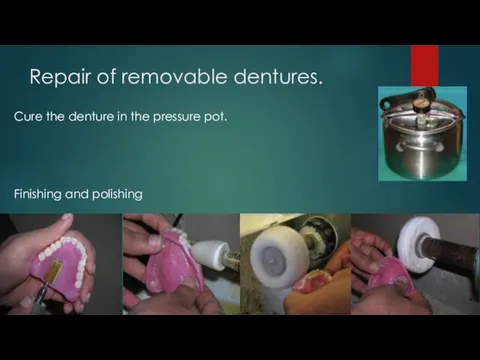
- 23. Repair of removable dentures. Cure the denture in the pressure pot. Finishing and polishing
- 24. Prosthetic stomatitis. Factors of prosthetic stomatitis (inflammation of mucosa of the prosthetic bedcaused by denture) Violation
- 25. Prosthetic stomatitis. Toxic effect. 1) Toxins of germs. 2) And the residual monomer is methyl methacrylic
- 26. Prosthetic stomatitis. Traumatic stomatitis. Toxic stomatitis (bacterial or chemical). Contact stomatitis.
- 27. Adaptation to the partial removable dentures. The adequacy of denture retention on the jaws and the
- 28. Adaptation to the partial removable dentures. To become accustomed to the dentures within a shorter time
- 29. Adaptation to the partial removable dentures. 5. Dentures that cause pain should be removed and the
- 30. Adaptation to the partial removable dentures. Three phases (by Kurlyandsky) should be distinguished in the adaptation
- 31. Adaptation to the partial removable dentures. The second phase, the phase of partial inhibition, occurs between
- 33. Скачать презентацию
Content
Try-in and correction of the PRD.
Remodeling of denture
Repair of removable dentures.
Prosthetic
Content
Try-in and correction of the PRD.
Remodeling of denture
Repair of removable dentures.
Prosthetic
Try-in and correction of the PRD.
Doctor have to evaluate:
the quality of
Try-in and correction of the PRD.
Doctor have to evaluate:
the quality of
Try-in and correction of the PRD.
Gaseous porosity
(Volatilization of monomer ):
Caused by
Try-in and correction of the PRD.
Gaseous porosity
(Volatilization of monomer ):
Caused by
Try-in and correction of the PRD.
Granular porosity (marble),
due to loss of
Try-in and correction of the PRD.
Granular porosity (marble),
due to loss of
Try-in and correction of the PRD.
Contraction (compression) porosity:
occurs due to monomer
Try-in and correction of the PRD.
Contraction (compression) porosity:
occurs due to monomer
Try-in and correction of the PRD.
Contraction (compression) porosity:
Insufficient amounts of resin
Try-in and correction of the PRD.
Contraction (compression) porosity:
Insufficient amounts of resin
Try-in and correction of the PRD.
Internal stresses in plastic
Occur when cooling and
Try-in and correction of the PRD.
Internal stresses in plastic
Occur when cooling and
Try-in and correction of the PRD.
Internal stresses in plastic
Insignificant loads can lead
Try-in and correction of the PRD.
Internal stresses in plastic
Insignificant loads can lead
Relining of denture
Relining and rebasingrelining is the resurfacing of the tissue surface of
Relining of denture
Relining and rebasingrelining is the resurfacing of the tissue surface of
Relining of denture
Relining - recreation of the inner surface of the denture. One
Relining of denture
Relining - recreation of the inner surface of the denture. One
Relining of denture
When else is the doctor doing a soft reassignment?
- If exostoses
Relining of denture
When else is the doctor doing a soft reassignment?
- If exostoses
Relining of denture
The relining can be done by a doctor, called a clinical
Relining of denture
The relining can be done by a doctor, called a clinical
Relining of denture
Why is laboratory relocation better than clinical?
The technician uses hot polymerization
Relining of denture
Why is laboratory relocation better than clinical?
The technician uses hot polymerization
Relining of denture
But, there are methods of temporary clinical relining. When you need
Relining of denture
But, there are methods of temporary clinical relining. When you need
Repair of removable dentures.
Reasons:
Poorly made (poorly constructed).
The patient mechanically break.
The lifetime of
Repair of removable dentures.
Reasons:
Poorly made (poorly constructed).
The patient mechanically break.
The lifetime of
Repair of removable dentures.
Other causes of denture fracture
1. Deep labial
Repair of removable dentures.
Other causes of denture fracture
1. Deep labial
Repair of removable dentures.
When the dentures can not be repaired
When
Repair of removable dentures.
When the dentures can not be repaired
When
Repair of removable dentures.
Types Of materials used in repairs
1.Chemical-Cured acrylic
2.Visible
Repair of removable dentures.
Types Of materials used in repairs
1.Chemical-Cured acrylic
2.Visible
Repair of removable dentures.
Broken parts are assembled & fixed together with sticky
Repair of removable dentures.
Broken parts are assembled & fixed together with sticky
Repair of removable dentures.
Any undercut on the fitting surface is blocked out
Repair of removable dentures.
Any undercut on the fitting surface is blocked out

Repair of removable dentures.
Fractured edges are widened along the fracture line and
Repair of removable dentures.
Fractured edges are widened along the fracture line and

Repair of removable dentures.
Cure the denture in the pressure pot.
Finishing and polishing
Repair of removable dentures.
Cure the denture in the pressure pot.
Finishing and polishing
Prosthetic stomatitis.
Factors of prosthetic stomatitis (inflammation of mucosa of the prosthetic bedcaused
Prosthetic stomatitis.
Factors of prosthetic stomatitis (inflammation of mucosa of the prosthetic bedcaused
Prosthetic stomatitis.
Toxic effect. 1) Toxins of germs. 2) And the residual monomer
Prosthetic stomatitis.
Toxic effect. 1) Toxins of germs. 2) And the residual monomer
Prosthetic stomatitis.
Traumatic stomatitis.
Toxic stomatitis (bacterial or chemical).
Contact stomatitis.
Prosthetic stomatitis.
Traumatic stomatitis.
Toxic stomatitis (bacterial or chemical).
Contact stomatitis.

Adaptation to the partial removable dentures.
The adequacy of denture retention on the jaws
Adaptation to the partial removable dentures.
The adequacy of denture retention on the jaws
Adaptation to the partial removable dentures.
To become accustomed to the dentures within a
Adaptation to the partial removable dentures.
To become accustomed to the dentures within a
Adaptation to the partial removable dentures.
5. Dentures that cause pain should be removed
Adaptation to the partial removable dentures.
5. Dentures that cause pain should be removed
Adaptation to the partial removable dentures.
Three phases (by Kurlyandsky) should be distinguished in
Adaptation to the partial removable dentures.
Three phases (by Kurlyandsky) should be distinguished in
Adaptation to the partial removable dentures.
The second phase, the phase of partial inhibition,
Adaptation to the partial removable dentures.
The second phase, the phase of partial inhibition,
 11 сынып ата - аналарымен өткізілген №4 жиналыс
11 сынып ата - аналарымен өткізілген №4 жиналыс Басни И.А. Крылова
Басни И.А. Крылова Индекс цитирования
Индекс цитирования Правовое регулирование закупок товаров, работ, услуг отдельными видами юридических лиц
Правовое регулирование закупок товаров, работ, услуг отдельными видами юридических лиц Проектирование календарного плана производства работ при строительстве общественного здания в городе Калуга
Проектирование календарного плана производства работ при строительстве общественного здания в городе Калуга Ацетиленовый генератор
Ацетиленовый генератор Презентация Национальный парк Паанаярви к уроку географии 8 класс
Презентация Национальный парк Паанаярви к уроку географии 8 класс Презентация о жизни и творчестве Мусы Джалиля
Презентация о жизни и творчестве Мусы Джалиля Следственные и оперативно-розыскные ошибки: их профмлактика и устранение в состязательном процессе
Следственные и оперативно-розыскные ошибки: их профмлактика и устранение в состязательном процессе Углеводы. Классификация углеводов
Углеводы. Классификация углеводов Курская дуга
Курская дуга Биологические мембраны
Биологические мембраны Natural Disasters
Natural Disasters Промежутки возрастания и убывания, наибольшее и наименьшее значения, точки экстремума
Промежутки возрастания и убывания, наибольшее и наименьшее значения, точки экстремума Презентация Братский район в годы ВОВ (1941-1945г)
Презентация Братский район в годы ВОВ (1941-1945г) Экономические связи России с зарубежными странами
Экономические связи России с зарубежными странами Отчет о проведении городской экологической операции Ёлочка
Отчет о проведении городской экологической операции Ёлочка Древесные ресурсы леса и эффективность их использования
Древесные ресурсы леса и эффективность их использования Солнце - ближайшая звезда
Солнце - ближайшая звезда Асинхронные машины. Конструкция и принцип действия. (Лекция 1)
Асинхронные машины. Конструкция и принцип действия. (Лекция 1) Эндометриоз. Классификация
Эндометриоз. Классификация Проектирование, строительство и эксплуатация автомобильных дорог. Исследование характеристик колейности по Башкортостану
Проектирование, строительство и эксплуатация автомобильных дорог. Исследование характеристик колейности по Башкортостану How are you feeling?
How are you feeling? Собираем урожай. Игры для дошкольников
Собираем урожай. Игры для дошкольников Основы объективно-ориентированного программирования в среде Lazarus
Основы объективно-ориентированного программирования в среде Lazarus Портфолио воспитателя ГПД
Портфолио воспитателя ГПД История развития цифро-аналогового преобразователя (ЦАП)
История развития цифро-аналогового преобразователя (ЦАП) Колебательные процессы (лекция 16)
Колебательные процессы (лекция 16)