- Uterine sarcoma

Содержание
- 2. The uterine sarcomas form a group of malignant tumors that arises from the smooth muscle or
- 4. Risk factors Exposure to estrogen is a key risk factor Risk is increased with dose and
- 5. Homologous consisting of uterine cells. Heterologous composed of tissue elements are not inherent in the uterus.
- 6. (THE HISTOLOGICAL SUBTYPE) If the lesion originates from the stroma of the uterine lining it is
- 7. ESS /LMS/Adenosarcoma FIGO 2009 staging IVB distant metastasis (including intraabdominal or inguinal lymph nodes; excluding adnexa,
- 9. Stage I-II – rapid growth of the uterus, bleeding from the genital tract (acyclic, contact, in
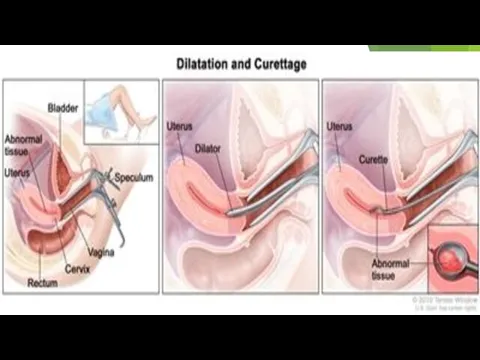
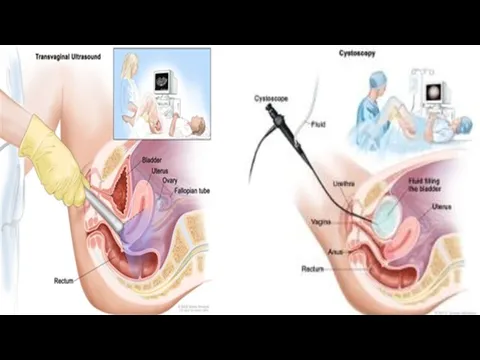
- 10. DIAGNOSTICS Anamnesis (complaints, an objective examination) General blood analysis, blood chemistry, CA 125 assay Gynecological examination
- 11. Pelvic exam PAP test
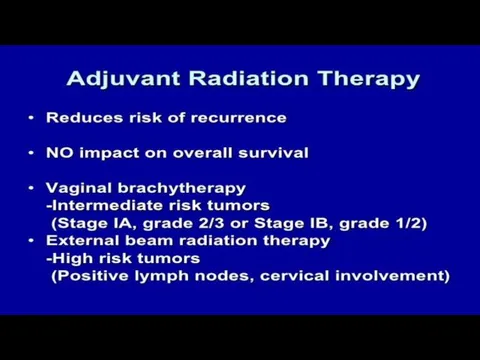
- 14. Treatment Treatment for this disease will vary, based on: • The size and location of the
- 15. Treatment for leiomyosarcoma Stage I - radical therapy, total abdominal hysterectomy with appendages Stage II, III
- 16. Treatment for endometrial stromal sarcoma Stage I - hysterectomy with appendages of the upper third of
- 17. Operations Leiomyosarcoma of reproductive age - hysterectomy without appendages pre and postmenopause - hysterectomy with appendages
- 18. Hormone terapy Appropriate in patients that desire fertility preservation - young parient - well differentiated cancer
- 22. REFERENCES * Zagouri F, Dimopoulos AM, Fotiou S, Kouloulias V, Papadimitriou CA (2009). "Treatment of early
- 24. Скачать презентацию
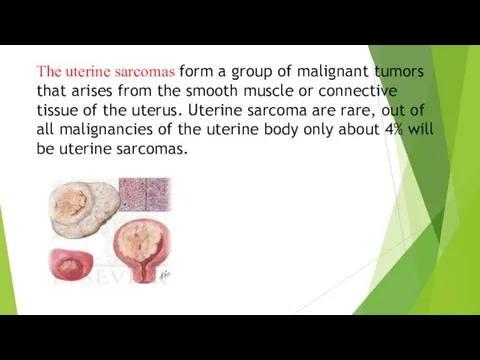
The uterine sarcomas form a group of malignant tumors that arises
The uterine sarcomas form a group of malignant tumors that arises

Risk factors
Exposure to estrogen is a key risk factor
Risk is
Risk factors
Exposure to estrogen is a key risk factor
Risk is
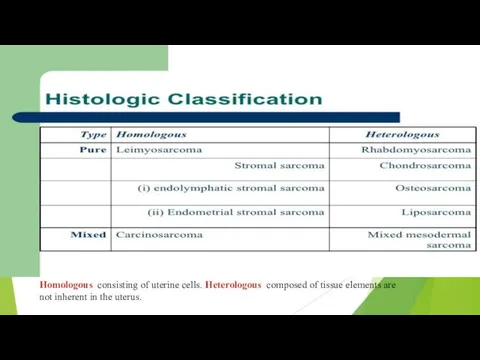
Homologous consisting of uterine cells. Heterologous composed of tissue elements are
Homologous consisting of uterine cells. Heterologous composed of tissue elements are
(THE HISTOLOGICAL SUBTYPE)
If the lesion originates from the stroma of
(THE HISTOLOGICAL SUBTYPE)
If the lesion originates from the stroma of
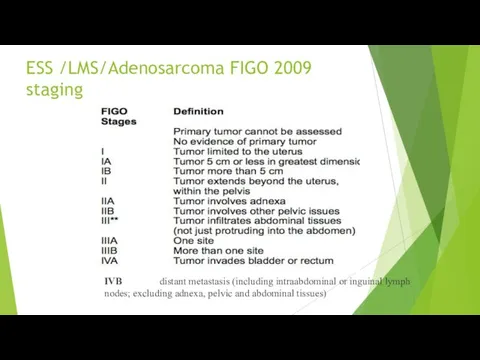
ESS /LMS/Adenosarcoma FIGO 2009 staging
IVB distant metastasis (including intraabdominal or inguinal
ESS /LMS/Adenosarcoma FIGO 2009 staging
IVB distant metastasis (including intraabdominal or inguinal
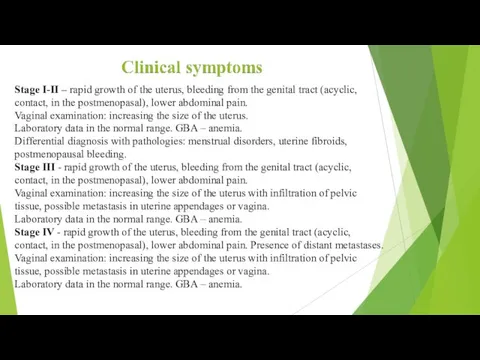
Stage I-II – rapid growth of the uterus, bleeding from the
Stage I-II – rapid growth of the uterus, bleeding from the

DIAGNOSTICS
Anamnesis (complaints, an objective examination)
General blood analysis, blood chemistry, CA 125
DIAGNOSTICS
Anamnesis (complaints, an objective examination)
General blood analysis, blood chemistry, CA 125
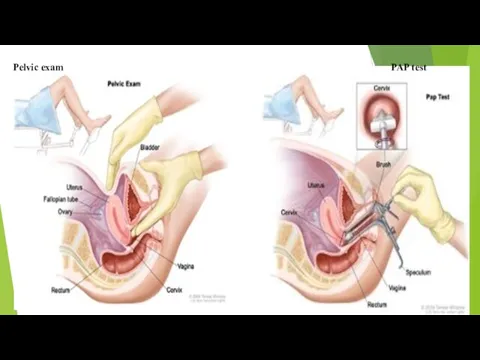
Pelvic exam PAP test
Pelvic exam PAP test
Treatment
Treatment for this disease will vary, based on:
• The size and location
Treatment
Treatment for this disease will vary, based on:
• The size and location
Treatment for leiomyosarcoma
Stage I - radical therapy, total abdominal hysterectomy
Treatment for leiomyosarcoma
Stage I - radical therapy, total abdominal hysterectomy
Treatment for endometrial stromal sarcoma
Stage I - hysterectomy with appendages
Treatment for endometrial stromal sarcoma
Stage I - hysterectomy with appendages
Operations
Leiomyosarcoma
of reproductive age - hysterectomy without appendages
pre and postmenopause -
Operations
Leiomyosarcoma
of reproductive age - hysterectomy without appendages
pre and postmenopause -
Hormone terapy
Appropriate in patients that desire fertility preservation
- young parient
- well
Hormone terapy Appropriate in patients that desire fertility preservation - young parient - well
REFERENCES
* Zagouri F, Dimopoulos AM, Fotiou S, Kouloulias V, Papadimitriou CA
REFERENCES * Zagouri F, Dimopoulos AM, Fotiou S, Kouloulias V, Papadimitriou CA
 Посвящение в пешеходы. 1 класс
Посвящение в пешеходы. 1 класс Возникновение жизни на Земле
Возникновение жизни на Земле Шаблон для презентации Правила дорожного движения
Шаблон для презентации Правила дорожного движения урок химии в 9 классе Азот
урок химии в 9 классе Азот Ата аналар жиналысына
Ата аналар жиналысына Принцип работы профилемеров
Принцип работы профилемеров Чем отличается рояль от пианино
Чем отличается рояль от пианино первый узкофюзеляжный гражданский самолёт SSJ100
первый узкофюзеляжный гражданский самолёт SSJ100 Циклические алгоритмы
Циклические алгоритмы Описание опыта
Описание опыта Деколонізація. Японія. Китай. Індія (Письмова робота, Всесвітня історія 11 клас )
Деколонізація. Японія. Китай. Індія (Письмова робота, Всесвітня історія 11 клас ) Коррекция дислексии. Методика Рональда Дэйвиса
Коррекция дислексии. Методика Рональда Дэйвиса Презентация:Развитие оптико - пространственных представлений у детей дошкольного возраста
Презентация:Развитие оптико - пространственных представлений у детей дошкольного возраста Членство в Федерации Альпинизма
Членство в Федерации Альпинизма Выступление на педагогическом совете Эффективный урок
Выступление на педагогическом совете Эффективный урок Сервировка стола к дню смеха
Сервировка стола к дню смеха Техническое обслуживание и ремонт теплообменных аппаратов
Техническое обслуживание и ремонт теплообменных аппаратов Электрические провода. Разновидность проводов. 8 класс
Электрические провода. Разновидность проводов. 8 класс Презентация Интервью
Презентация Интервью Русский иконостас
Русский иконостас Правило светофора
Правило светофора Морфологические формы слова. ЕГЭ. Задание 6
Морфологические формы слова. ЕГЭ. Задание 6 Сладкое и полезное лакомство
Сладкое и полезное лакомство Оценка достижения показателей стратегических документов
Оценка достижения показателей стратегических документов Имена героев в названиях улиц Екатеринбурга: улица Бажова
Имена героев в названиях улиц Екатеринбурга: улица Бажова Как происходило объединение Франции
Как происходило объединение Франции Теоретические и коррекционные подходы в работе с аутичными детьми
Теоретические и коррекционные подходы в работе с аутичными детьми Презентация Разработки по созданию развивающей среды в группе детского сада
Презентация Разработки по созданию развивающей среды в группе детского сада