- The Renal Transplant Patient

Содержание
- 2. Introduction Renal transplantation is the preferred treatment for patients with end-stage renal disease. It offers better
- 3. EMPs encounter transplant pts at 2 critical stages: Initial doctors to identify potential donors from a
- 4. Diabetic nephropathy accounts for 40% of the diseases resulting in renal transplantation. This subgroup of pts
- 5. The Transplantation Process Transplant coordinators should be called early for any pt who may meet brain
- 6. Following brain death, a number of physiological changes occur that need to be rectified if donor
- 7. About 75% of organ donors develop diabetes insipidus due to pituitary necrosis and this leads to
- 8. Definitions Allograft : graft between genetically dissimilar individuals of the same species. Autograft : graft in
- 9. The Surgical Procedure Wet ischaemia time (time from cessation of circulation to removal of organ and
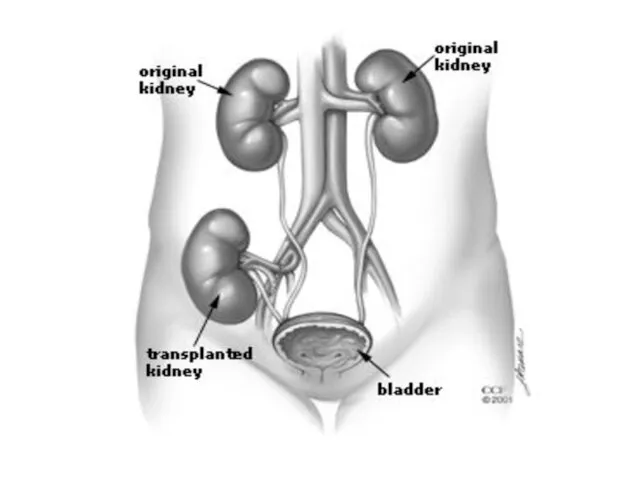
- 10. The transplant renal a is anastomosed to the ipsilateral internal or external iliac a, the renal
- 11. Living donor transplants fxn immediately after transplant, +/- 30% of cadaveric transplants have delayed graft fxn
- 14. Graft Prognosis Directly related to source of donor kidney. Recipients of cadaveric kidneys have more episodes
- 15. Morbidity Infection (most common cause of M&M in first year post transplantation) and graft failure occur.
- 16. Osteoporosis 60% Malignant neoplasm 14% - related to the degree of immunosupression.
- 17. Mortality Survival of pts after transplantation from a liver donor is 98% at 1 yr and
- 18. Hx of a pt with organ transplant presenting to ED Current symptoms (esp. fever) Transplant age
- 19. Immunosuppressive Rx Compliance with Rx Previous infections Recent exposure to ill pts
- 20. Examination of the Patient Inspect, palpate and auscultate the graft site. Graft tenderness and swelling is
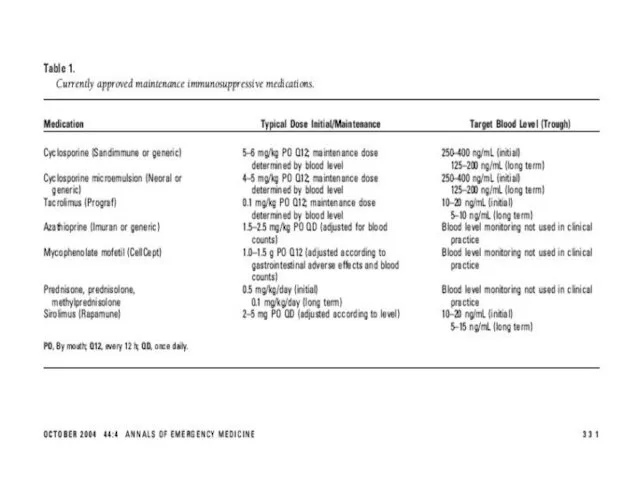
- 21. Immunosuppressive Therapy Renal transplant pts require lifelong immunosuppression to prevent rejection. Current “triple” regimes include cyclosporine-microemulsion
- 22. Cyclosporine: inhibits both cellular and humoral immunity by binding to cyclophilins which block cytokine transcription and
- 23. Azathioprine: antimetabolite derivative of 6-mercatopurine. Inhibits DNA + RNA synthesis, resulting in suppression of lymphocyte proliferation.
- 24. Tacrolimus: newer macrolide compound that binds to lymphocyte proteins and inhibits cytokine synthesis. Used as either
- 25. Immunosuppressant minimisation protocols are becoming more popular. Triple Rx for 3-12 months after transplantation followed by
- 26. The initial Rx of rejection involves the administration of IVI corticosteroids (methylpred 250-1000mg daily for 3/7
- 30. Surgical Complications affecting Allografts Usual postop generic complications: atelectasis, pneumonia, wound infection, ileus, bleeding and venous
- 31. 2. Peritransplant haematoma Early postop complication or in setting of perioperative anticoagulation (2-3%) Severe pain over
- 32. 3. Urinary Leak First transplant month. (2-5%) Presents with urine extravasation and ARF, fever, pain and
- 33. 4. Lymphocoele Occurs within the first 3 post transplant months and is due to lymph leaking
- 34. 5. Obstructive Uropathy Occurs in early post transplant period (3-6%). The commonest causes are extrinsic compression
- 35. 6. Renal artery stenosis Late presentation. Pts present with uncontrolled HT, allograft dysfunction and peripheral oedema.
- 36. Fever in the Transplant Pt Commom problem. Opportunistic infections occur frequently. Remember that fever may be
- 37. Infections in the 1st post transplant month Usual post op infections: pneumonia, wound infection, line sepsis,
- 38. Infections in the remainder of the 1st post transplant year Opportunistic infections are most common after
- 39. Most reliable diagnosis is PCR for viral DNA in blood. Untreated CMV has a mortality as
- 40. Infections after the 1st post transplant year Community-acquired infections unrelated to immune suppression are more common.
- 41. Non-infectious causes of fever Pulmonary atelectasis (early post op) Severe acute rejection Administration of antilymphocyte Abs
- 42. Initial Work-up for febrile post transplant pt FBC + diff Serum creatinine Urine dipstix and analysis
- 43. Cardiovascular disorders The risk of CVS disease is increased 3 to 5 fold in kidney transplant
- 44. HT Complications Prevalence is 70-90% in renal transplant recipients. None of the parentarel or oral antiHT
- 45. Pulmonary Complications Most common pulmonary problem is pneumonia. Nonopportunistic post op pneumonia in the 1st month,
- 46. GIT Problems Abnormalities in LFTs occur frequently. The clinical presentation of acute cholecystitis may be blunted
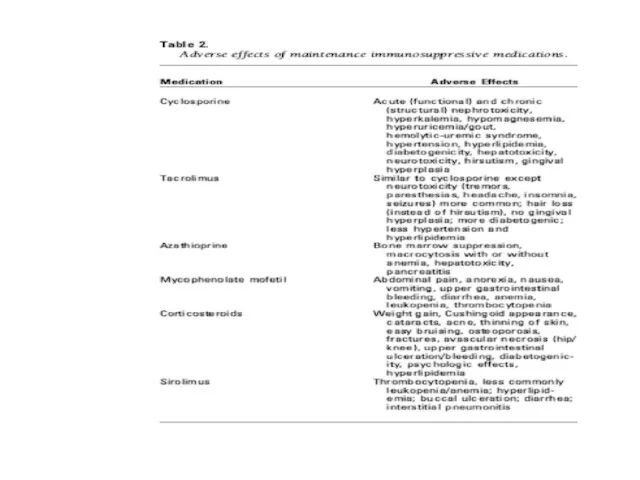
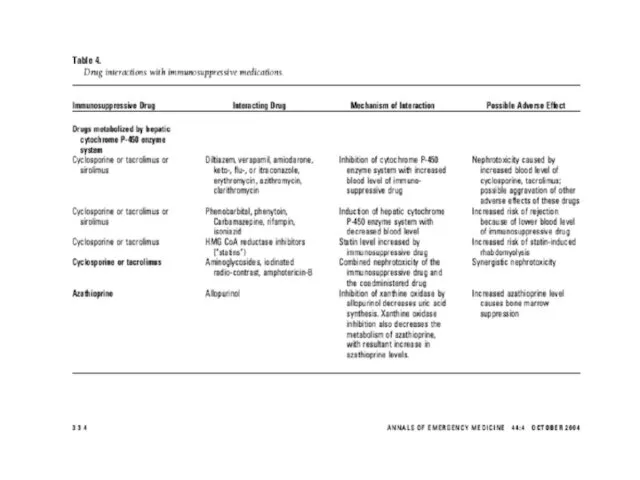
- 47. Neurologic + Psychiatric Disorders Cyclosporine and tacrolimus cause similar neurological S/Es (headache, insomnia, tremors, parasthesias, cramp
- 48. Meningitis: Listeria monocytogenes, cryptococcus + TB. Encephalitis or meningoencephalitis: CMV, toxoplasma or HSV. Post transplant lymphoma
- 49. Haematological Disorders Anaemia, leukopaenia, thrombocytopaenia alone or in combination is common. Often due to drugs. HUS:
- 50. Post transplant erythrocytosis occurs in 10-20% of pts during the first post transplant year + persists
- 51. Musculoskeletal Disorders Corticosteroids, and to a lesser extent cyclosporine + tacrolimus predispose to osteoporosis. Cyclosporine +
- 52. With pts on azothioprine, the use of allopurinol can cause severe bone marrow suppression unless the
- 53. Dermatological Disorders A variety of disorders can occur: acne,herpes zoster, human papilloma virus, squamous cell Ca
- 54. Electrolyte Abnormalities Cyclosporin + tacrolimus cause hyperkalaemia (decreased K excretion in urine) and hypomagnesemia (increased Mg
- 55. New Onset DM De nova DM occurs in 5-20% of renal transplant recipients. Contributing to this
- 56. Malignancy Transplant recipients are at significantly higher risk for cancers than the general population because of
- 57. Stress-dose Corticosteroid Coverage Severely ill renal transplant pts presenting to ED will require stress-dose corticosteroid coverage
- 58. Acute Rejection Indirect pathway: soluble donor Ag that is processed by recipient APC + then presented
- 59. Acute rejection appears within the first 3 posttransplant months and affects 30% of cadaveric transplants and
- 60. Chronic Rejection Usually apparent from 3 months onwards and detected clinically by gradual deteriation in graft
- 61. Take Home Massage 1. If a transplant pt presents the ED, always consider the possibility of
- 63. Скачать презентацию
Introduction
Renal transplantation is the preferred treatment for patients with end-stage renal
Introduction
Renal transplantation is the preferred treatment for patients with end-stage renal
EMPs encounter transplant pts at 2 critical stages:
Initial doctors to identify
EMPs encounter transplant pts at 2 critical stages:
Initial doctors to identify
Diabetic nephropathy accounts for 40% of the diseases resulting in renal
Diabetic nephropathy accounts for 40% of the diseases resulting in renal
The Transplantation Process
Transplant coordinators should be called early for any pt
The Transplantation Process
Transplant coordinators should be called early for any pt
Following brain death, a number of physiological changes occur that need
Following brain death, a number of physiological changes occur that need
About 75% of organ donors develop diabetes insipidus due to pituitary
About 75% of organ donors develop diabetes insipidus due to pituitary
Definitions
Allograft : graft between genetically dissimilar individuals of the same species.
Autograft
Definitions
Allograft : graft between genetically dissimilar individuals of the same species.
Autograft
The Surgical Procedure
Wet ischaemia time (time from cessation of circulation to
The Surgical Procedure
Wet ischaemia time (time from cessation of circulation to
The transplant renal a is anastomosed to the ipsilateral internal or
The transplant renal a is anastomosed to the ipsilateral internal or
Living donor transplants fxn immediately after transplant, +/- 30% of cadaveric
Living donor transplants fxn immediately after transplant, +/- 30% of cadaveric
Graft Prognosis
Directly related to source of donor kidney.
Recipients of cadaveric kidneys
Graft Prognosis
Directly related to source of donor kidney.
Recipients of cadaveric kidneys
Morbidity
Infection (most common cause of M&M in first year post transplantation)
Morbidity
Infection (most common cause of M&M in first year post transplantation)
Osteoporosis 60%
Malignant neoplasm 14% - related to the degree of immunosupression.
Osteoporosis 60%
Malignant neoplasm 14% - related to the degree of immunosupression.
Mortality
Survival of pts after transplantation from a liver donor is 98%
Mortality
Survival of pts after transplantation from a liver donor is 98%
Hx of a pt with organ transplant presenting to ED
Current symptoms
Hx of a pt with organ transplant presenting to ED
Current symptoms
Immunosuppressive Rx
Compliance with Rx
Previous infections
Recent exposure to ill pts
Immunosuppressive Rx
Compliance with Rx
Previous infections
Recent exposure to ill pts
Examination of the Patient
Inspect, palpate and auscultate the graft site.
Graft tenderness
Examination of the Patient
Inspect, palpate and auscultate the graft site.
Graft tenderness
Immunosuppressive Therapy
Renal transplant pts require lifelong immunosuppression to prevent rejection.
Current “triple”
Immunosuppressive Therapy
Renal transplant pts require lifelong immunosuppression to prevent rejection.
Current “triple”
Cyclosporine: inhibits both cellular and humoral immunity by binding to cyclophilins
Cyclosporine: inhibits both cellular and humoral immunity by binding to cyclophilins
Azathioprine: antimetabolite derivative of 6-mercatopurine. Inhibits DNA + RNA synthesis, resulting
Azathioprine: antimetabolite derivative of 6-mercatopurine. Inhibits DNA + RNA synthesis, resulting
Tacrolimus: newer macrolide compound that binds to lymphocyte proteins and inhibits
Tacrolimus: newer macrolide compound that binds to lymphocyte proteins and inhibits
Immunosuppressant minimisation protocols are becoming more popular.
Triple Rx for 3-12 months
Immunosuppressant minimisation protocols are becoming more popular.
Triple Rx for 3-12 months
The initial Rx of rejection involves the administration of IVI corticosteroids
The initial Rx of rejection involves the administration of IVI corticosteroids
Surgical Complications affecting Allografts
Usual postop generic complications: atelectasis, pneumonia, wound infection,
Surgical Complications affecting Allografts
Usual postop generic complications: atelectasis, pneumonia, wound infection,
2. Peritransplant haematoma
Early postop complication or in setting of perioperative
2. Peritransplant haematoma
Early postop complication or in setting of perioperative
3. Urinary Leak
First transplant month. (2-5%)
Presents with urine extravasation
3. Urinary Leak
First transplant month. (2-5%)
Presents with urine extravasation
4. Lymphocoele
Occurs within the first 3 post transplant months and
4. Lymphocoele
Occurs within the first 3 post transplant months and
5. Obstructive Uropathy
Occurs in early post transplant period (3-6%). The
5. Obstructive Uropathy
Occurs in early post transplant period (3-6%). The
6. Renal artery stenosis
Late presentation.
Pts present with uncontrolled
6. Renal artery stenosis
Late presentation.
Pts present with uncontrolled
Fever in the Transplant Pt
Commom problem.
Opportunistic infections occur frequently.
Remember that fever
Fever in the Transplant Pt
Commom problem.
Opportunistic infections occur frequently.
Remember that fever
Infections in the 1st post transplant month
Usual post op infections: pneumonia,
Infections in the 1st post transplant month
Usual post op infections: pneumonia,
Infections in the remainder of the 1st post transplant year
Opportunistic infections
Infections in the remainder of the 1st post transplant year
Opportunistic infections
Most reliable diagnosis is PCR for viral DNA in blood.
Untreated
Most reliable diagnosis is PCR for viral DNA in blood.
Untreated
Infections after the 1st post transplant year
Community-acquired infections unrelated to immune
Infections after the 1st post transplant year
Community-acquired infections unrelated to immune
Non-infectious causes of fever
Pulmonary atelectasis (early post op)
Severe acute rejection
Administration of
Non-infectious causes of fever
Pulmonary atelectasis (early post op)
Severe acute rejection
Administration of
Initial Work-up for febrile post transplant pt
FBC + diff
Serum creatinine
Urine dipstix
Initial Work-up for febrile post transplant pt
FBC + diff
Serum creatinine
Urine dipstix
Cardiovascular disorders
The risk of CVS disease is increased 3 to 5
Cardiovascular disorders
The risk of CVS disease is increased 3 to 5
HT Complications
Prevalence is 70-90% in renal transplant recipients.
None of the parentarel
HT Complications
Prevalence is 70-90% in renal transplant recipients.
None of the parentarel
Pulmonary Complications
Most common pulmonary problem is pneumonia.
Nonopportunistic post op pneumonia in
Pulmonary Complications
Most common pulmonary problem is pneumonia.
Nonopportunistic post op pneumonia in
GIT Problems
Abnormalities in LFTs occur frequently.
The clinical presentation of acute cholecystitis
GIT Problems
Abnormalities in LFTs occur frequently.
The clinical presentation of acute cholecystitis
Neurologic + Psychiatric Disorders
Cyclosporine and tacrolimus cause similar neurological S/Es (headache,
Neurologic + Psychiatric Disorders
Cyclosporine and tacrolimus cause similar neurological S/Es (headache,
Meningitis: Listeria monocytogenes, cryptococcus + TB.
Encephalitis or meningoencephalitis: CMV, toxoplasma or
Meningitis: Listeria monocytogenes, cryptococcus + TB.
Encephalitis or meningoencephalitis: CMV, toxoplasma or
Haematological Disorders
Anaemia, leukopaenia, thrombocytopaenia alone or in combination is common. Often
Haematological Disorders
Anaemia, leukopaenia, thrombocytopaenia alone or in combination is common. Often
Post transplant erythrocytosis occurs in 10-20% of pts during the first
Post transplant erythrocytosis occurs in 10-20% of pts during the first
Musculoskeletal Disorders
Corticosteroids, and to a lesser extent cyclosporine + tacrolimus predispose
Musculoskeletal Disorders
Corticosteroids, and to a lesser extent cyclosporine + tacrolimus predispose
With pts on azothioprine, the use of allopurinol can cause severe
With pts on azothioprine, the use of allopurinol can cause severe
Dermatological Disorders
A variety of disorders can occur: acne,herpes zoster, human papilloma
Dermatological Disorders
A variety of disorders can occur: acne,herpes zoster, human papilloma
Electrolyte Abnormalities
Cyclosporin + tacrolimus cause hyperkalaemia (decreased K excretion in urine)
Electrolyte Abnormalities
Cyclosporin + tacrolimus cause hyperkalaemia (decreased K excretion in urine)
New Onset DM
De nova DM occurs in 5-20% of renal transplant
New Onset DM
De nova DM occurs in 5-20% of renal transplant
Malignancy
Transplant recipients are at significantly higher risk for cancers than the
Malignancy
Transplant recipients are at significantly higher risk for cancers than the
Stress-dose Corticosteroid Coverage
Severely ill renal transplant pts presenting to ED will
Stress-dose Corticosteroid Coverage
Severely ill renal transplant pts presenting to ED will
Acute Rejection
Indirect pathway: soluble donor Ag that is processed by recipient
Acute Rejection
Indirect pathway: soluble donor Ag that is processed by recipient
Acute rejection appears within the first 3 posttransplant months and affects
Acute rejection appears within the first 3 posttransplant months and affects
Chronic Rejection
Usually apparent from 3 months onwards and detected clinically by
Chronic Rejection
Usually apparent from 3 months onwards and detected clinically by
Take Home Massage
1. If a transplant pt presents the ED, always
Take Home Massage
1. If a transplant pt presents the ED, always
 Madrid. It is big and busy city in the center of spain
Madrid. It is big and busy city in the center of spain Active voice
Active voice Основы английского языка (3 класс)
Основы английского языка (3 класс) In the jungle
In the jungle The history of the olympic games
The history of the olympic games Russian Federation
Russian Federation Indian cuisine
Indian cuisine The art of genuine communication
The art of genuine communication Relative pronouns who, why, when, which, whose, where, what
Relative pronouns who, why, when, which, whose, where, what Subject and Aims of the History of English
Subject and Aims of the History of English Space News
Space News Food and Cooking
Food and Cooking Check vocabulary
Check vocabulary Tornado Alley is the most dangerous disaster in the USA. Life after
Tornado Alley is the most dangerous disaster in the USA. Life after The Essay Topic Selection Guidelines. Week 1. Lesson 2
The Essay Topic Selection Guidelines. Week 1. Lesson 2 The secrets of the nature
The secrets of the nature Fast food
Fast food Gubin Andrey Terentyevich
Gubin Andrey Terentyevich Sport in our life
Sport in our life My day
My day christmas vocabulary
christmas vocabulary Indefinite article (a / an)
Indefinite article (a / an) Буквосочетание th. Числительные (numbers)
Буквосочетание th. Числительные (numbers) Friends and friendship
Friends and friendship Structuralism as a concept of language and as linguistic methodology
Structuralism as a concept of language and as linguistic methodology English Tea
English Tea The Republic of Kazakhstan in civil proceedings
The Republic of Kazakhstan in civil proceedings The United kingdom of great Britain and northern Ireland
The United kingdom of great Britain and northern Ireland