- VITAMIN “D”

Содержание
- 2. Content Source Physiology & metabolism Deficiency & resistance Requirements & Treatment ‘Extra-skeletal’ effects
- 3. History 1600s 1st description of rickets by Whistler & Glisson 1918 Sir Edward Mellanby linked with
- 4. Modern Day Interest Vitamin D & metabolites Significant role in calcium homeostasis & bone metabolism Deficiency
- 5. Vitamin D Deficiency Subclinical deficiency Silent epidemic. Present in approximately 30% to 50% of the general
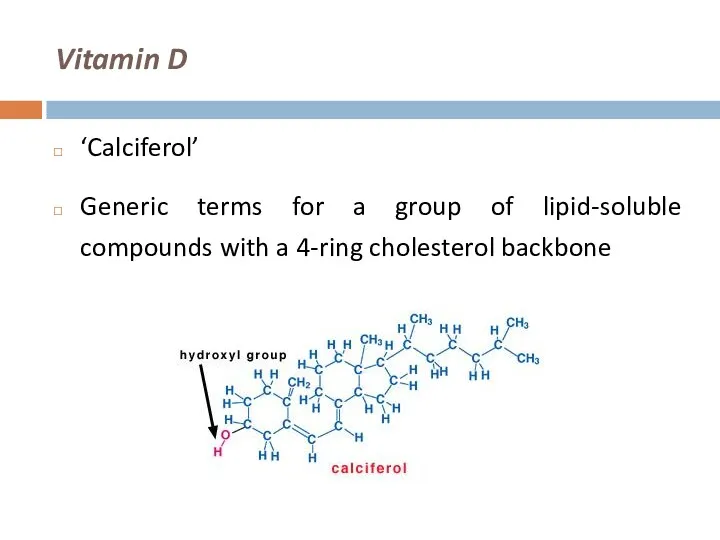
- 6. Vitamin D ‘Calciferol’ Generic terms for a group of lipid-soluble compounds with a 4-ring cholesterol backbone
- 7. Sources Of Vitamin D Sunlight (UV) Intestinal absorption (only ~20%) Oily fish Fortified milk / bread
- 8. Absorption & Metabolism Affected by fat malabsorption Pancreatic insufficiency CF Cholestatic liver disease Coeliac Crohn’s
- 9. Vitamin D Metabolism Skin UV light photo-isomerises provitamin D to D3 (cholecalciferol) Transported by Vit D
- 10. Vitamin D Metabolism
- 11. Deficiency & Resistance Impaired availability of Vit D Lack of sun exposure, can be seasonal Fat
- 12. Consequences of Vitamin D Deficiency Reduced intestinal absorption of calcium & phosphorus Hypophosphataemia precedes hypocalciaemia Secondary
- 13. Rickets
- 14. Osteomalacia After closure of epiphyseal plates Impaired mineralisation Fractures Lab tests Low calcium & phosphate High
- 15. Associated Clinical Conditions Muscle Weakness and Falls Proximal muscle weakness Chronic muscle aches Myopathy Increase in
- 16. Associated Clinical Conditions Bone Density and Fractures Risk of osteoporosis may be reduced with adequate intake
- 17. Associated Clinical Conditions Role in Cancer Prevention Low intake of vitamin D and calcium has been
- 18. Associated Clinical Conditions Autoimmune Disease Vitamin D supplementation is associated with a lower risk of autoimmune
- 19. Associated Clinical Conditions Role in Cardiovascular Diseases Vitamin D deficiency activates the renin-angiotensin-aldosterone system and can
- 20. Associated Clinical Conditions Role in Reproductive Health Vitamin D deficiency early in pregnancy is associated with
- 21. At-Risk Groups Elderly Stores decline with age Winter House-bound or institutionalised Poor nutritional intake Impaired absorption
- 22. At-Risk Groups Children Exclusively breast-fed infants Variable dietary intake Vegetarian or fish-free diet Ethnic background Women
- 23. At-Risk Groups Healthy adults Immigrants Winter (1 in 6 UK adults) Boston study – Holick et
- 24. At-Risk Groups Hospitalised patients Age Sun exposure Intake Renal injury Burns victims 22-42% prevalence in US
- 25. Assessment
- 26. Investigations
- 27. Diagnosis
- 28. Vitamin D Measurements
- 29. Vitamin D Preparations (assuming normal renal function) Cholecalciferol D3 Natural molecule in man Ergocalciferol D2 Plant-derived
- 30. Vitamin D Preparations
- 31. Vitamin D Supplementation Deficiency ( Oral Therapy 1st line agent: Fultium-D3 ® (Cholecalciferol) 800 iu capsules
- 32. Vitamin D Supplementation Deficiency ( Oral Therapy 1st line agent: Fultium-D3 ® (Cholecalciferol) 800 iu capsules
- 33. Vitamin D Supplementation Insufficiency (25-50 nmol/l or 10-20 mcg/l) or for long-term maintenance following rx of
- 34. Combined calcium & vitamin D supplements Calcium component usually unnecessary in primary vitamin D deficiency Less
- 35. Alfacalcidol/Calcitriol Alfacalcidol (1 alpha- vitamin D) and Calcitriol have no routine place in the management of
- 36. Monitoring 1 month Bone and renal profile 3 months Bone and renal profile, vitamin D, and
- 37. Conclusion Commoner than we think! Can be prevented: Promote awareness, especially in high-risk groups Sun-exposure Safe,
- 39. Скачать презентацию
Content
Source
Physiology & metabolism
Deficiency & resistance
Requirements & Treatment
‘Extra-skeletal’ effects
Content
Source
Physiology & metabolism
Deficiency & resistance
Requirements & Treatment
‘Extra-skeletal’ effects
History
1600s 1st description of rickets by Whistler & Glisson
1918 Sir Edward Mellanby linked
History
1600s 1st description of rickets by Whistler & Glisson
1918 Sir Edward Mellanby linked
Modern Day Interest
Vitamin D & metabolites
Significant role in calcium homeostasis &
Modern Day Interest
Vitamin D & metabolites
Significant role in calcium homeostasis &
Vitamin D Deficiency
Subclinical deficiency
Silent epidemic.
Present in approximately 30% to 50% of
Vitamin D Deficiency
Subclinical deficiency
Silent epidemic.
Present in approximately 30% to 50% of
Vitamin D
‘Calciferol’
Generic terms for a group of lipid-soluble compounds with a
Vitamin D
‘Calciferol’
Generic terms for a group of lipid-soluble compounds with a

Sources Of Vitamin D
Sunlight (UV)
Intestinal absorption (only ~20%)
Oily fish
Fortified milk /
Sources Of Vitamin D
Sunlight (UV)
Intestinal absorption (only ~20%)
Oily fish
Fortified milk /
Absorption & Metabolism
Affected by fat malabsorption
Pancreatic insufficiency
CF
Cholestatic liver disease
Coeliac
Crohn’s
Absorption & Metabolism
Affected by fat malabsorption
Pancreatic insufficiency
CF
Cholestatic liver disease
Coeliac
Crohn’s
Vitamin D Metabolism
Skin
UV light photo-isomerises provitamin D to D3 (cholecalciferol)
Transported by
Vitamin D Metabolism
Skin
UV light photo-isomerises provitamin D to D3 (cholecalciferol)
Transported by
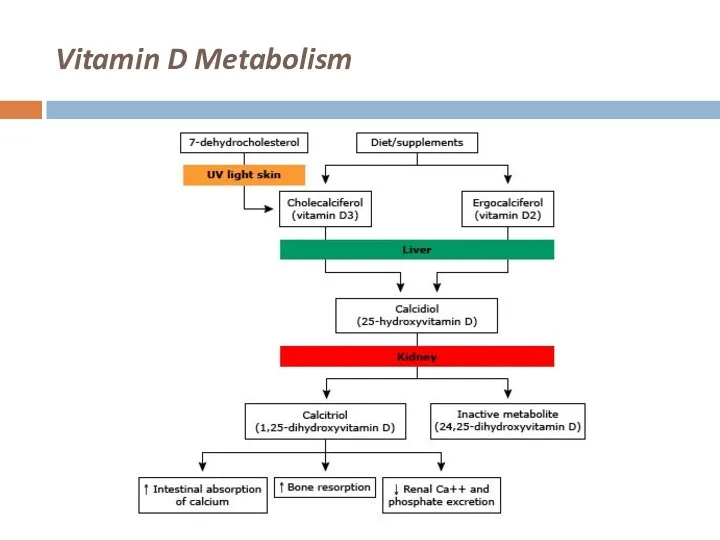
Vitamin D Metabolism
Vitamin D Metabolism
Deficiency & Resistance
Impaired availability of Vit D
Lack of sun exposure, can
Deficiency & Resistance
Impaired availability of Vit D
Lack of sun exposure, can
Consequences of Vitamin D Deficiency
Reduced intestinal absorption of calcium & phosphorus
Hypophosphataemia
Consequences of Vitamin D Deficiency
Reduced intestinal absorption of calcium & phosphorus
Hypophosphataemia
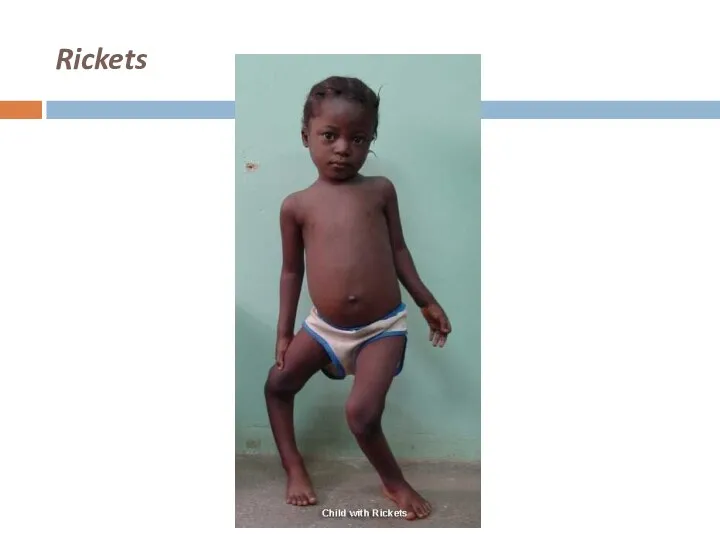
Rickets
Rickets
Osteomalacia
After closure of epiphyseal plates
Impaired mineralisation
Fractures
Lab tests
Low calcium & phosphate
High ALP
X-rays
Diffuse
Osteomalacia
After closure of epiphyseal plates
Impaired mineralisation
Fractures
Lab tests
Low calcium & phosphate
High ALP
X-rays
Diffuse
Associated Clinical Conditions
Muscle Weakness and Falls
Proximal muscle weakness
Chronic muscle aches
Myopathy
Increase in
Associated Clinical Conditions
Muscle Weakness and Falls
Proximal muscle weakness
Chronic muscle aches
Myopathy
Increase in
Associated Clinical Conditions
Bone Density and Fractures
Risk of osteoporosis may be reduced
Associated Clinical Conditions
Bone Density and Fractures
Risk of osteoporosis may be reduced
Associated Clinical Conditions
Role in Cancer Prevention
Low intake of vitamin D and
Associated Clinical Conditions
Role in Cancer Prevention
Low intake of vitamin D and
Associated Clinical Conditions
Autoimmune Disease
Vitamin D supplementation is associated with a lower
Associated Clinical Conditions
Autoimmune Disease
Vitamin D supplementation is associated with a lower
Associated Clinical Conditions
Role in Cardiovascular Diseases
Vitamin D deficiency activates the renin-angiotensin-aldosterone
Associated Clinical Conditions
Role in Cardiovascular Diseases
Vitamin D deficiency activates the renin-angiotensin-aldosterone
Associated Clinical Conditions
Role in Reproductive Health
Vitamin D deficiency early in pregnancy
Associated Clinical Conditions
Role in Reproductive Health
Vitamin D deficiency early in pregnancy
At-Risk Groups
Elderly
Stores decline with age
Winter
House-bound or institutionalised
Poor nutritional intake
Impaired absorption
CKD
At-Risk Groups
Elderly
Stores decline with age
Winter
House-bound or institutionalised
Poor nutritional intake
Impaired absorption
CKD
At-Risk Groups
Children
Exclusively breast-fed infants
Variable dietary intake
Vegetarian or fish-free diet
Ethnic background
Women treated
At-Risk Groups
Children
Exclusively breast-fed infants
Variable dietary intake
Vegetarian or fish-free diet
Ethnic background
Women treated
At-Risk Groups
Healthy adults
Immigrants
Winter (1 in 6 UK adults)
Boston study –
At-Risk Groups
Healthy adults
Immigrants
Winter (1 in 6 UK adults)
Boston study –
At-Risk Groups
Hospitalised patients
Age
Sun exposure
Intake
Renal injury
Burns victims
22-42% prevalence in US studies
At-Risk Groups
Hospitalised patients
Age
Sun exposure
Intake
Renal injury
Burns victims
22-42% prevalence in US studies
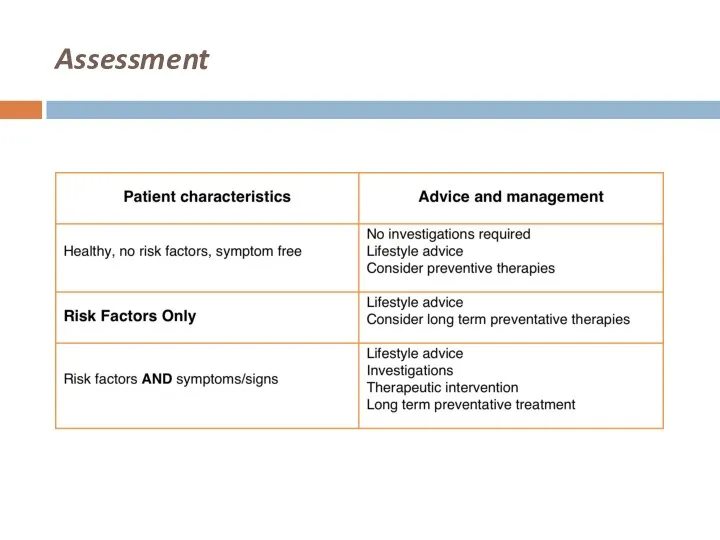
Assessment
Assessment
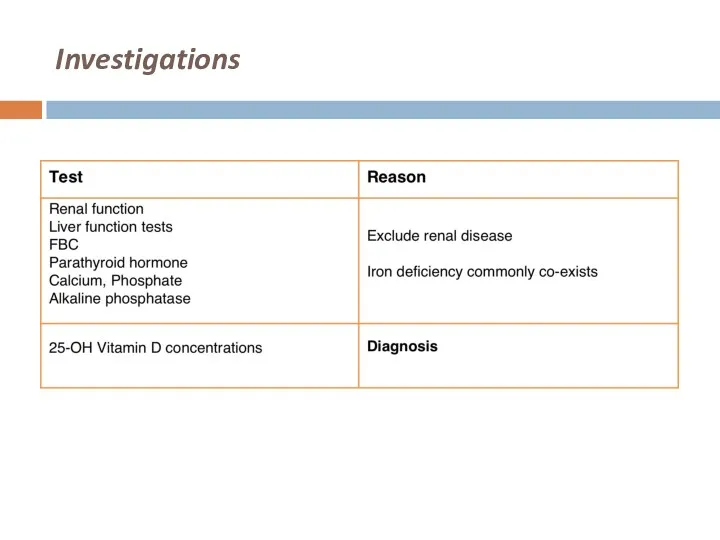
Investigations
Investigations
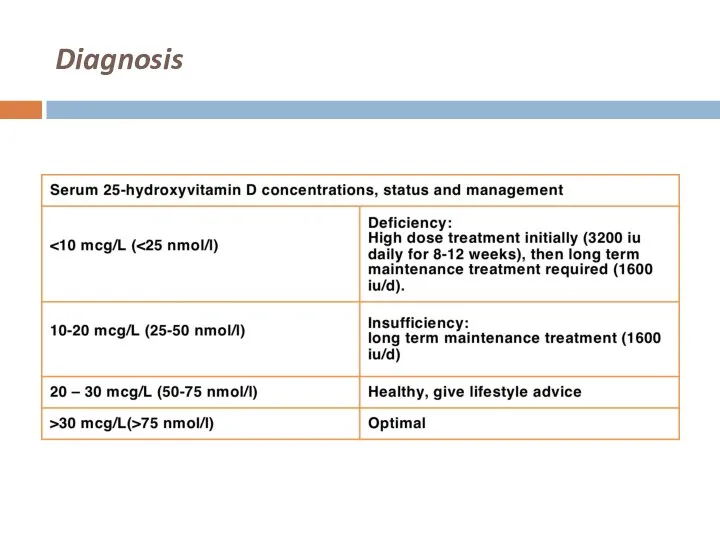
Diagnosis
Diagnosis

Vitamin D Measurements
Vitamin D Measurements
Vitamin D Preparations
(assuming normal renal function)
Cholecalciferol
D3
Natural molecule in man
Ergocalciferol
D2
Plant-derived
Less effective than
Vitamin D Preparations
(assuming normal renal function)
Cholecalciferol
D3
Natural molecule in man
Ergocalciferol
D2
Plant-derived
Less effective than
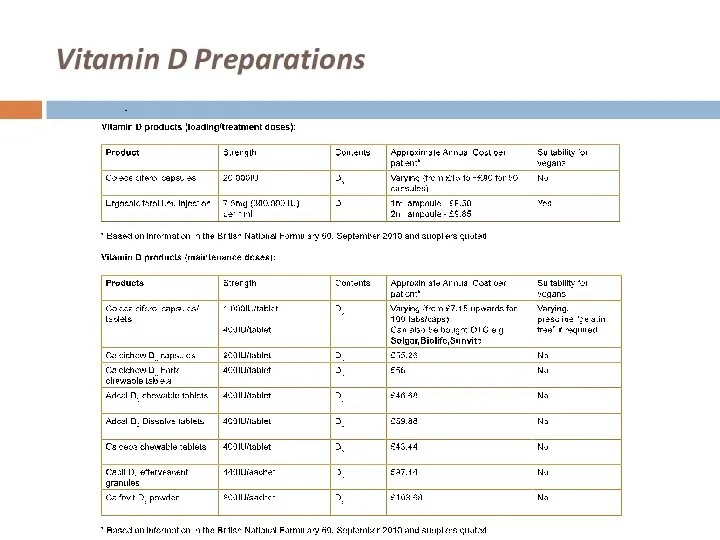
Vitamin D Preparations
Vitamin D Preparations

Vitamin D Supplementation
Deficiency (<25 nmol/l or 10 mcg/l)
Oral Therapy
1st line agent:
Vitamin D Supplementation
Deficiency (<25 nmol/l or 10 mcg/l)
Oral Therapy
1st line agent:
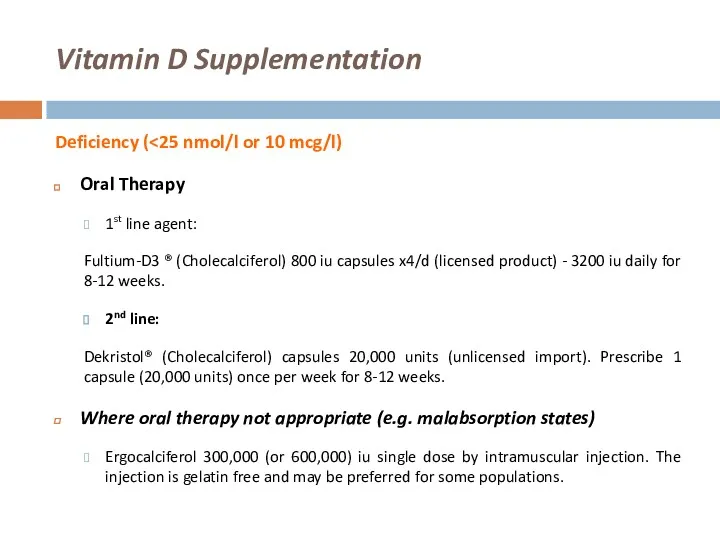
Vitamin D Supplementation
Deficiency (<25 nmol/l or 10 mcg/l)
Oral Therapy
1st line agent:
Vitamin D Supplementation
Deficiency (<25 nmol/l or 10 mcg/l)
Oral Therapy
1st line agent:
Vitamin D Supplementation
Insufficiency (25-50 nmol/l or 10-20 mcg/l) or for long-term
Vitamin D Supplementation
Insufficiency (25-50 nmol/l or 10-20 mcg/l) or for long-term
Combined calcium & vitamin D supplements
Calcium component usually unnecessary in primary
Combined calcium & vitamin D supplements
Calcium component usually unnecessary in primary
Alfacalcidol/Calcitriol
Alfacalcidol (1 alpha- vitamin D) and Calcitriol have no routine place
Alfacalcidol/Calcitriol
Alfacalcidol (1 alpha- vitamin D) and Calcitriol have no routine place
Monitoring
1 month
Bone and renal profile
3 months
Bone and renal profile, vitamin D,
Monitoring
1 month
Bone and renal profile
3 months
Bone and renal profile, vitamin D,

Conclusion
Commoner than we think!
Can be prevented:
Promote awareness, especially in high-risk groups
Sun-exposure
Safe,
Conclusion
Commoner than we think!
Can be prevented:
Promote awareness, especially in high-risk groups
Sun-exposure
Safe,
 The scientific picture of the world
The scientific picture of the world Роль учителя в развитии навыков говорения на уроках английского языка в начальной школе
Роль учителя в развитии навыков говорения на уроках английского языка в начальной школе The History of the U.S. Customs Service
The History of the U.S. Customs Service Higher Education in England
Higher Education in England Reasons for learning English
Reasons for learning English Cupcake in a cup
Cupcake in a cup In harmony with myself
In harmony with myself Weather
Weather Действительный залог (Active Voice). Страдательный залог (Passive Voice)
Действительный залог (Active Voice). Страдательный залог (Passive Voice) Identify barriers to learning
Identify barriers to learning The weather
The weather What’s the weather
What’s the weather Thanksgiving Day
Thanksgiving Day Present Simple
Present Simple My summer holidays
My summer holidays Main cities of the Usa
Main cities of the Usa Language and speech. Types of speech
Language and speech. Types of speech The present simple Tense
The present simple Tense Employee health & hygiene. (Chapter 3)
Employee health & hygiene. (Chapter 3) Придаточные предложения
Придаточные предложения My home
My home English. Geographic position
English. Geographic position Promotion ideas for your company
Promotion ideas for your company Present Perfect vs Past Past Perfect. Lesson 5
Present Perfect vs Past Past Perfect. Lesson 5 Features of British cuisine
Features of British cuisine My personality and choice of future profession
My personality and choice of future profession Shortcomings and negative influence of the media
Shortcomings and negative influence of the media Famous-birthdays activities
Famous-birthdays activities