- Esophagus. Esophageal Structure

Содержание
- 2. Esophagus Esophageal anatomy and physiology Esophageal symptoms Diagnostic procedures GERD Dysphagia
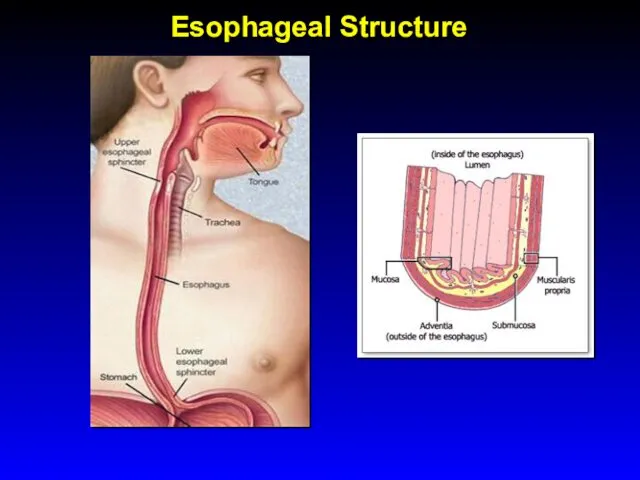
- 3. Esophageal Structure
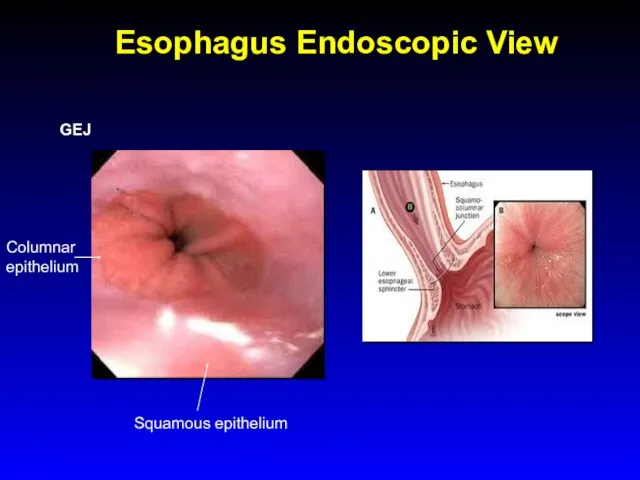
- 4. Esophagus Endoscopic View GEJ Columnar epithelium Squamous epithelium
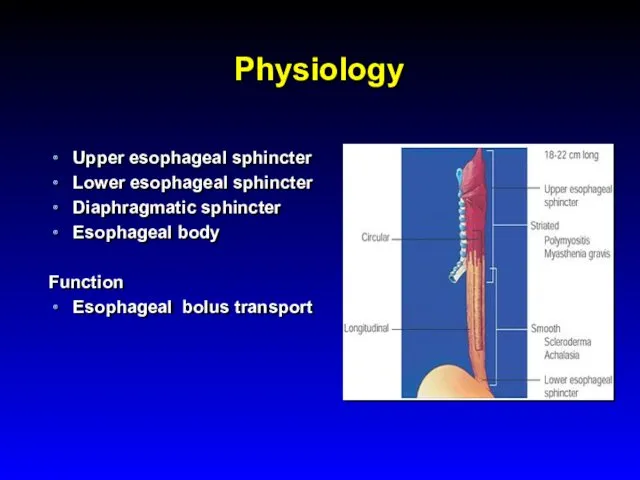
- 5. Physiology Upper esophageal sphincter Lower esophageal sphincter Diaphragmatic sphincter Esophageal body Function Esophageal bolus transport
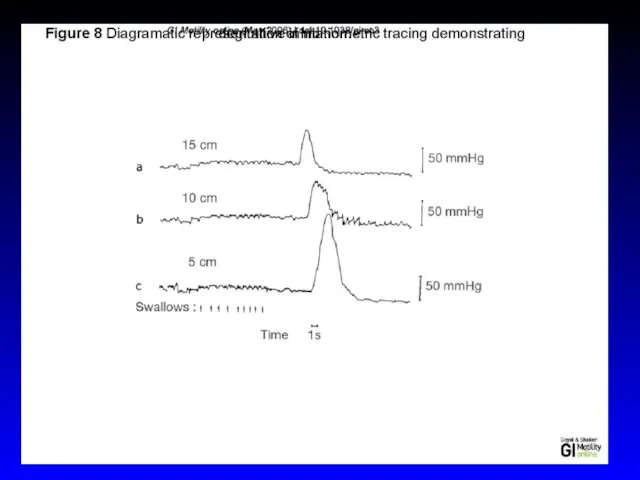
- 7. Physiology- Deglutitive Inhibition The swallow-evoked peristaltic contraction consist of wave of inhibition followed by that of
- 9. Physiology Primary peristalsis esophageal peristaltic contraction wave associated with swallowing Secondary peristalsis It is a reflex
- 10. Transient Lower Esophageal Sphincter Relaxations LES relaxation during belching, retching, vomiting, and rumination TLESR are not
- 12. Physiology The esophagus is innervated by both parasympathetic and sympathetic nerves The parasympathetics control peristalsis via
- 13. Symptoms Heartburn (pyrosis)- the most common esophageal symptom Discomfort or burning sensation behind the sternum that
- 14. Symptoms Regurgitation - effortless return of food or fluid into the pharynx without nausea or retching
- 15. Symptoms Chest pain - common esophageal symptom with characteristics similar to cardiac pain pressure type sensation
- 16. Symptoms Dysphagia - feeling of food "sticking" or lodging in the chest Solid food dysphagia /liquid
- 17. Symptoms Odynophagia - pain caused by swallowing common with pill or infectious esophagitis, esophageal ulcer /erosions
- 18. Diagnostic Studies Endoscopy Radiography Endoscopic Ultrasound Esophageal Manometry Video swallow study Reflux Testing
- 19. ENDOSCOPY Endoscopy
- 20. Radiography- Barium Swallow Normal barium swallow Esophageal spasm Cork screw esophagus Hiatal hernia
- 21. Esophageal manometry
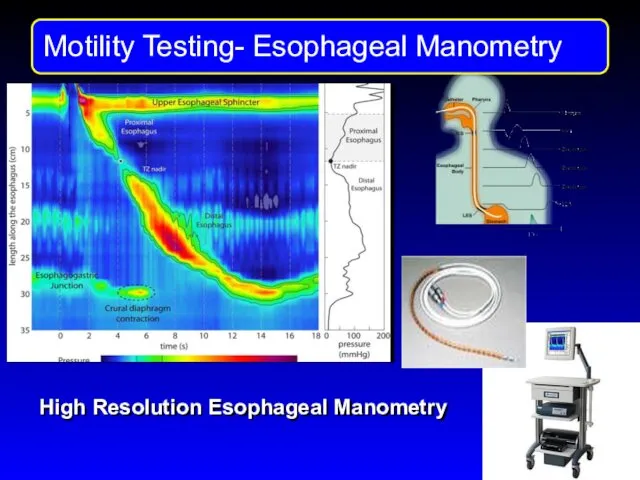
- 22. Motility Testng High Resolution Esophageal Manometry
- 23. 24-hour transnasally positioned wire electrode with the tip stationed in the distal esophagus 48-hour esophageal pH
- 24. pH study: intranasal wire electrode with the sensor in the distal esophagus.
- 25. Wireless Bravo pH Capsule for acid reflux detection
- 28. Acid and non-acid acid reflux detection Gold standard of reflux testing PH-MII detects intraesophageal bolus movement
- 29. Gastroesophageal Reflux Disease (GERD)
- 30. GERD- definitions Physiologic reflux episodes typically occur postprandially, are short-lived, asymptomatic, and rarely occur during sleep
- 31. Pathophysiology of GERD Castell Do et al. Aliment Pharmacol Ther 2004; 20 (Suppl 9):14 Lower esophageal
- 32. Pathophysiology of GERD Hiatal hernia
- 33. GERD Epidemiology Prevalence : 10 -20 % in the Western world , Incidence : 5 per
- 34. GERD Symptoms Common: Heartburn and regurgitation Less common: dysphagia and chest pain Extraesophageal manifestations of GERD:
- 35. GERD- Ds Ds is usually based on clinical symptoms Utilization of diagnostic tests: the goal is
- 37. GERD Differential Diagnosis Infectious, pill, or eosinophilic esophagitis Peptic ulcer disease Dyspepsia Biliary colic Coronary artery
- 38. GERD Treatment Lifestyle modifications Avoidance of Foods that reduce LES pressure -"refluxogenic" (fatty foods, alcohol, spearmint,
- 39. GERD Treatment Inhibitors of gastric acid secretion Reducing the acidity of gastric juice does not prevent
- 40. bv
- 42. GERD Treatment- surgical Nissen fundoplication the proximal stomach is wrapped around the distal esophagus to create
- 43. GERD Complications Chronic esophagitis (bleeding and stricture) increasingly rare due to potent antisecretory medications Esophageal adenocarcinoma
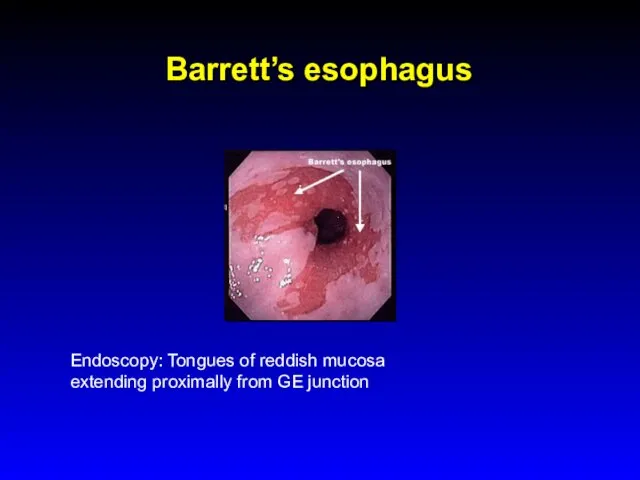
- 44. Barrett’s esophagus Endoscopy: Tongues of reddish mucosa extending proximally from GE junction
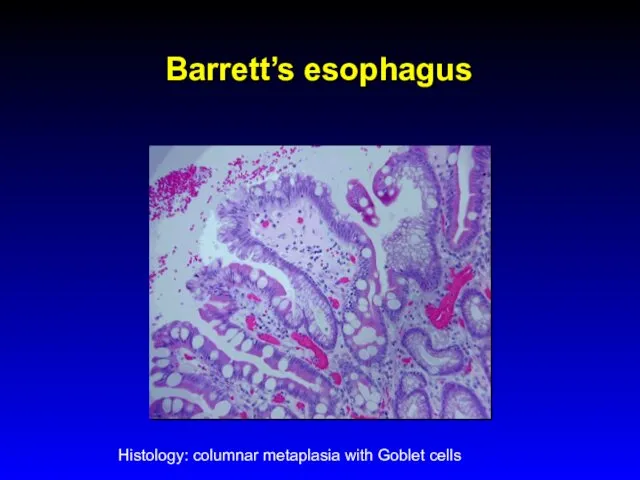
- 45. Barrett’s esophagus Histology: columnar metaplasia with Goblet cells
- 46. GERD Complications- Barrett’s Obese white males in 6th decade of lie are at greatest risk for
- 47. Dysphagia
- 48. Approach to Dysphagia Dysphagia Oropharyngeal Esophageal Video swallow study Type of Bolus Abnormal Address specific cause
- 49. Oropharyngeal Dysphagia Etiology Neurogenic - major source of morbidity related to aspiration and malnutrition CVA Parkinson's
- 50. Zenker's diverticulum Elderly Prevalence 1:1000 - 1:10,000 Symptoms: dysphagia, regurgitation of particulate food debris, aspiration, halitosis
- 51. Esophageal Dysphagia Solid food dysphagia appears when the lumen is Circumferential lesions are more likely to
- 52. Esophageal Dysphagia Structural causes Schatzki's rings Eosinophilic esophagitis Peptic strictures Neoplasia GERD without a stricture, perhaps
- 53. Esophageal Dysphagia Upper endoscopy Dysphagia is an alarm symptom Esophageal manometry Barium swallow
- 54. Esophageal Dysphagia- Schatzki's ring Distal esophagus Mucosal ring Intermittent dysphagia Treatment ( if symptomatic): dilatation +/-
- 55. Achalasia Incidence 1-3:100,000 Age - 25 to 60 yo Symptoms Dysphagia: solid and liquid food Regurgitation:
- 56. Achalasia Etiology: Loss of ganglion cells- inhibitory (nitric oxide) ganglionic neurons within the esophageal myenteric plexus.
- 57. Achalasia Differential diagnosis Diffuse esopghageal spasm (DES) Chagas' disease (Trypanosoma cruzi) -The chronic phase of the
- 58. Achalasia Diagnosis Endoscopy - rarely diagnostic, to exclude pseudo-achalasia Manometry - most sensitive diagnostic test Barium
- 59. Achalasia Conventional manometry - Impaired LES relaxation - Absent peristalsis of esophageal body
- 60. Achalasia Normal High Resolution Manometry
- 61. Three Subtypes of Achalasia on High Resolution Manometry Alexander J. Eckardt & Volker F. Eckardt Nature
- 62. Three Subtypes of Achalasia on High Resolution Manometry Peter J Kahrilas, The Am J Gastro 105,
- 63. Achalasia Barium swallow x-ray dilated esophagus with poor emptying air-fluid level tapering at the LES -
- 64. Achalasia Treatment Therapy is directed at reducing LES pressure Pharmacologicals therapies are relatively ineffective Botulinum toxin,
- 65. Pneumatic balloon dilation of LES
- 67. Achalasia- Complications Squamous cell carcinoma risk increased 17-fold in inadequately treated achalasia most probably due to
- 68. Diffuse Esophageal Spasm (DES) Episodes of dysphagia and chest pain attributable to abnormal esophageal contractions. Diagnosis
- 69. Diffuse Esophageal Spasm Corkscrew esophagus
- 70. Dysphagia Diffuse Esophageal Spasm (DES) Diffferntial diagnosis: angina pectoris peptic or infectious esophagitis Achalasia Treatment -
- 71. Scleroderma - Dilated esophagus - Ineffective peristalsis - Low LES pressure - Severe GERD
- 72. Eosinophilic Esophagitis Prevalence 1:1000 with a predilection for white males, incidence is increasing Symptoms: dysphagia, food
- 73. Eosinophilic Esophagitis Endoscopy: multiple esophageal rings, linear furrows, and punctate exudates Histology: increased eosinophils in the
- 74. Eosinophilic Esophagitis Complications: food impaction and esophageal perforation Treatment: Dietary restrictions PPIs Systemic or topical (fluticasone)
- 75. Infectious Esophagitis Common infections in Immunocompromized pts (organ transplantation, chronic inflammatory diseases, chemotherapy, AIDS) Candida species
- 76. Infectious Esophagitis Candida Esophagitis C. albicans is the most common. Endoscopy with biopsy is diagnostic Endoscopic
- 77. Infectious Esophagitis Herpetic Esophagitis Herpes simplex virus type 1 or 2 may cause esophagitis Endoscopy: vesicles
- 78. Other Types of Esopahgitis Radiation esopahgitis Pill- induced esophagitis doxyclin, tertacyclin, minocycline, peniciliin, clindamycin, NSAIDs, KCl,
- 79. Esophageal Cancer Squamous cell carcinoma Adenocarcinoma
- 80. Esophageal Cancer Squamous cell carcinoma risk factors: excess alcohol consumption and/or cigarette smoking ingestion of nitrites
- 82. Esophageal Cancer incidence of squamous cell cancer decreases over the past 30 years incidence of adenocarcinoma
- 83. Esophageal Cancer Adenocarcinomas arise in the distal esophagus in the presence of chronic gastric reflux and
- 84. Esophageal Cancer Location 10% upper third of the sophagus 35% in the middle third 55% in
- 85. Clinical features Progressive dysphagia (solids) Weight loss When these symptoms develop, the disease is usually incurable
- 86. Esophageal carcinoma Endoscopic and cytologic screening for carcinoma in patients with Barrett’s esophagus Prognosis is poor:
- 88. Скачать презентацию
Esophagus
Esophageal anatomy and physiology
Esophageal symptoms
Diagnostic procedures
GERD
Dysphagia
Esophagus
Esophageal anatomy and physiology
Esophageal symptoms
Diagnostic procedures
GERD
Dysphagia
Esophageal Structure
Esophageal Structure
Esophagus Endoscopic View
GEJ
Columnar epithelium
Squamous epithelium
Esophagus Endoscopic View
GEJ
Columnar epithelium
Squamous epithelium
Physiology
Upper esophageal sphincter
Lower esophageal sphincter
Diaphragmatic sphincter
Esophageal body
Function
Esophageal bolus transport
Physiology
Upper esophageal sphincter
Lower esophageal sphincter
Diaphragmatic sphincter
Esophageal body
Function
Esophageal bolus transport
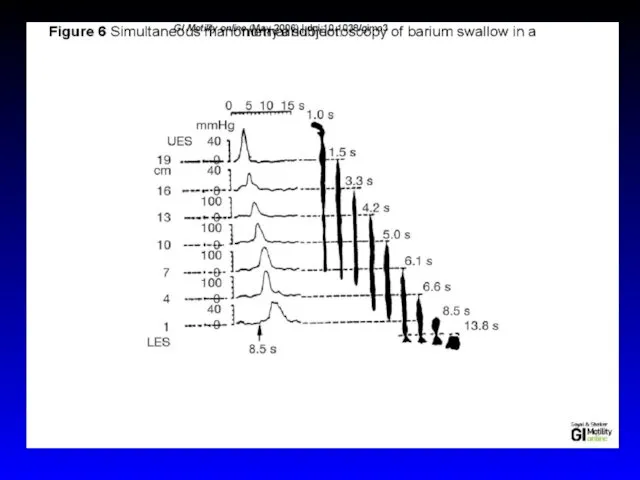
Physiology- Deglutitive Inhibition
The swallow-evoked peristaltic contraction consist of wave of
Physiology- Deglutitive Inhibition
The swallow-evoked peristaltic contraction consist of wave of
Physiology
Primary peristalsis
esophageal peristaltic contraction wave associated with swallowing
Secondary peristalsis
It
Physiology
Primary peristalsis
esophageal peristaltic contraction wave associated with swallowing
Secondary peristalsis
It
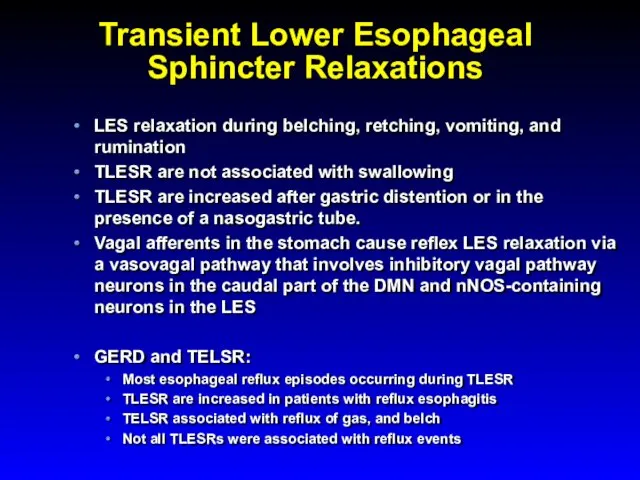
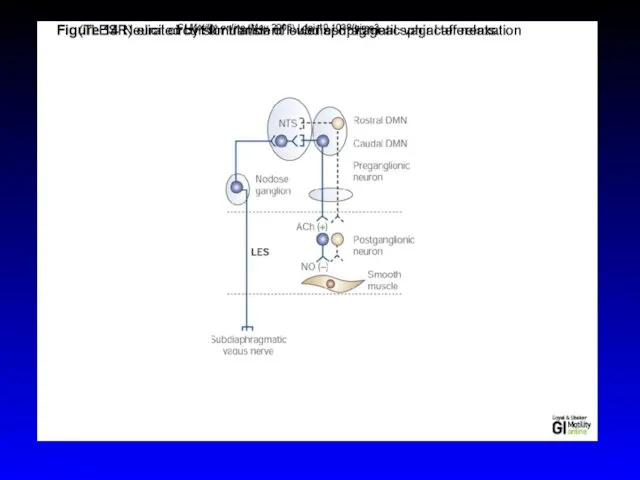
Transient Lower Esophageal Sphincter Relaxations
LES relaxation during belching, retching, vomiting, and
Transient Lower Esophageal Sphincter Relaxations
LES relaxation during belching, retching, vomiting, and
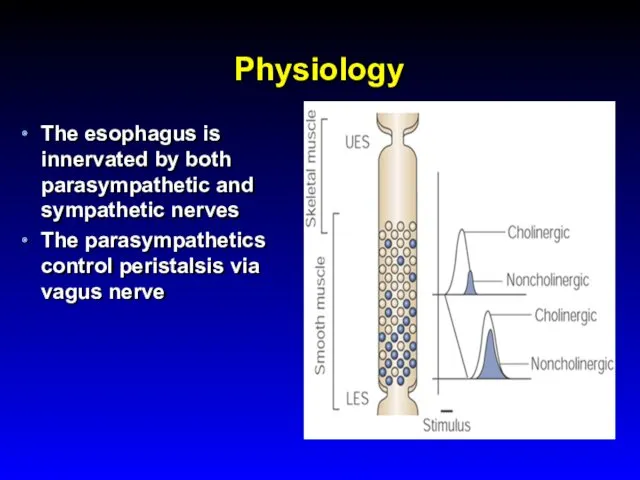
Physiology
The esophagus is innervated by both parasympathetic and sympathetic nerves
The
Physiology
The esophagus is innervated by both parasympathetic and sympathetic nerves
The
Symptoms
Heartburn (pyrosis)- the most common esophageal symptom
Discomfort or burning sensation behind
Symptoms
Heartburn (pyrosis)- the most common esophageal symptom
Discomfort or burning sensation behind
Symptoms
Regurgitation - effortless return of food or fluid into the pharynx
Symptoms
Regurgitation - effortless return of food or fluid into the pharynx
Symptoms
Chest pain - common esophageal symptom with characteristics similar to cardiac
Symptoms
Chest pain - common esophageal symptom with characteristics similar to cardiac
Symptoms
Dysphagia - feeling of food "sticking" or lodging in the chest
Solid
Symptoms
Dysphagia - feeling of food "sticking" or lodging in the chest
Solid
Symptoms
Odynophagia - pain caused by swallowing
common with pill or infectious esophagitis,
Symptoms
Odynophagia - pain caused by swallowing
common with pill or infectious esophagitis,
Diagnostic Studies
Endoscopy
Radiography
Endoscopic Ultrasound
Esophageal Manometry
Video swallow study
Reflux Testing
Diagnostic Studies
Endoscopy
Radiography
Endoscopic Ultrasound
Esophageal Manometry
Video swallow study
Reflux Testing
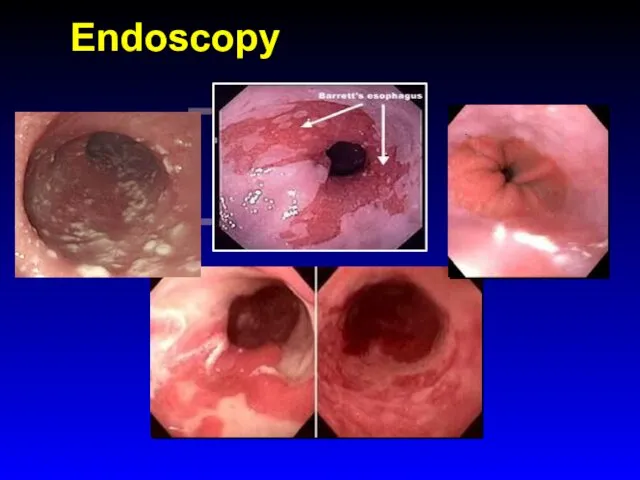
ENDOSCOPY
Endoscopy
ENDOSCOPY
Endoscopy
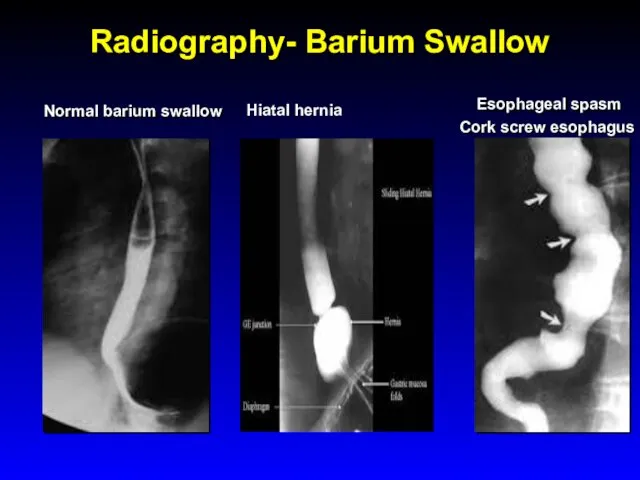
Radiography- Barium Swallow
Normal barium swallow
Esophageal spasm
Cork screw esophagus
Hiatal hernia
Radiography- Barium Swallow
Normal barium swallow
Esophageal spasm
Cork screw esophagus
Hiatal hernia
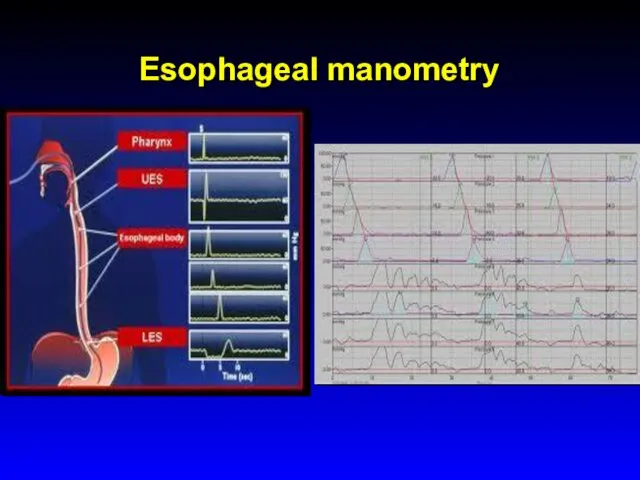
Esophageal manometry
Esophageal manometry
Motility Testng
High Resolution Esophageal Manometry
Motility Testng
High Resolution Esophageal Manometry
24-hour transnasally positioned wire electrode with the tip stationed in the
24-hour transnasally positioned wire electrode with the tip stationed in the
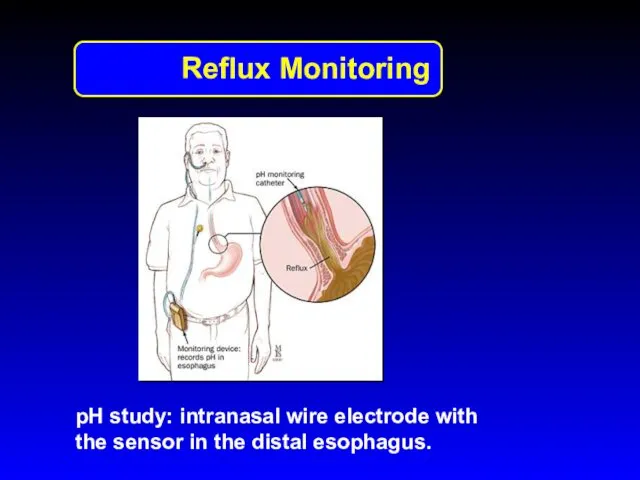
pH study: intranasal wire electrode with the sensor in the distal
pH study: intranasal wire electrode with the sensor in the distal
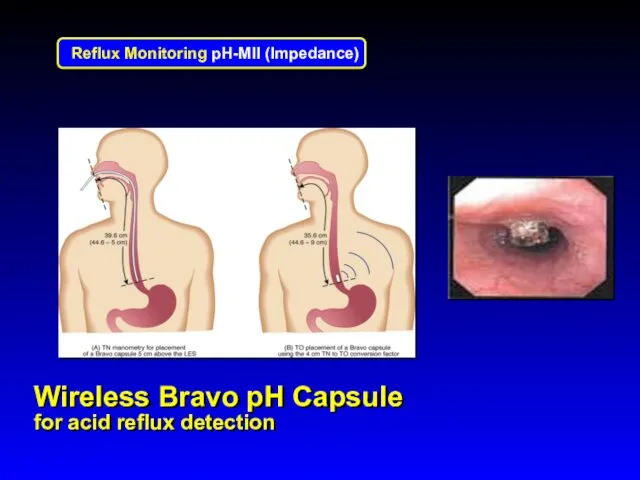
Wireless Bravo pH Capsule
for acid reflux detection
Wireless Bravo pH Capsule
for acid reflux detection
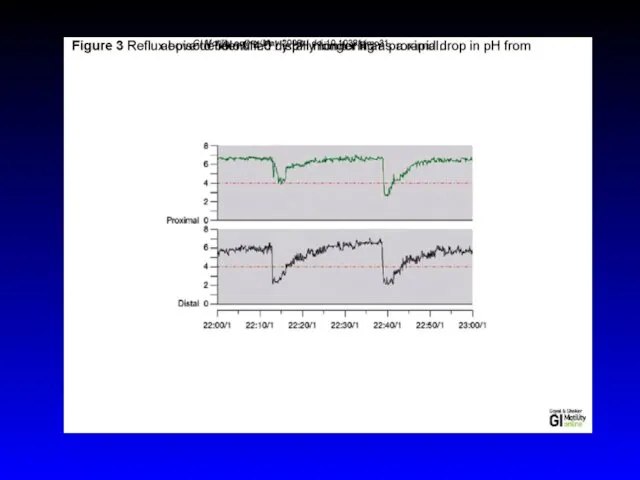

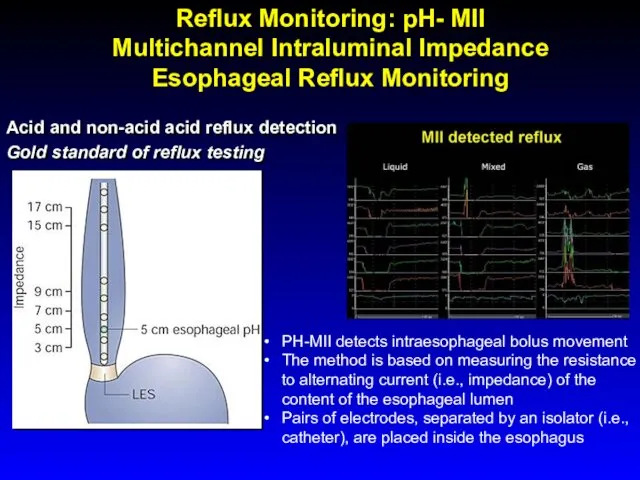
Acid and non-acid acid reflux detection
Gold standard of reflux testing
PH-MII detects
Acid and non-acid acid reflux detection
Gold standard of reflux testing
PH-MII detects
Gastroesophageal
Reflux Disease
(GERD)
Gastroesophageal
Reflux Disease
(GERD)
GERD- definitions
Physiologic reflux episodes typically occur postprandially, are short-lived, asymptomatic, and
GERD- definitions
Physiologic reflux episodes typically occur postprandially, are short-lived, asymptomatic, and
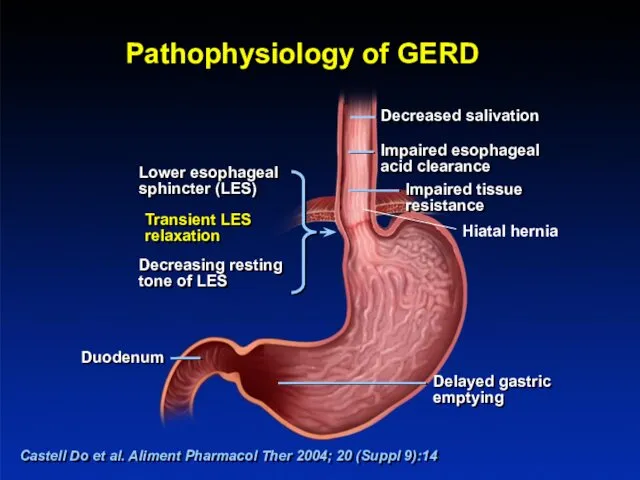
Pathophysiology of GERD
Castell Do et al. Aliment Pharmacol Ther 2004; 20
Pathophysiology of GERD
Castell Do et al. Aliment Pharmacol Ther 2004; 20
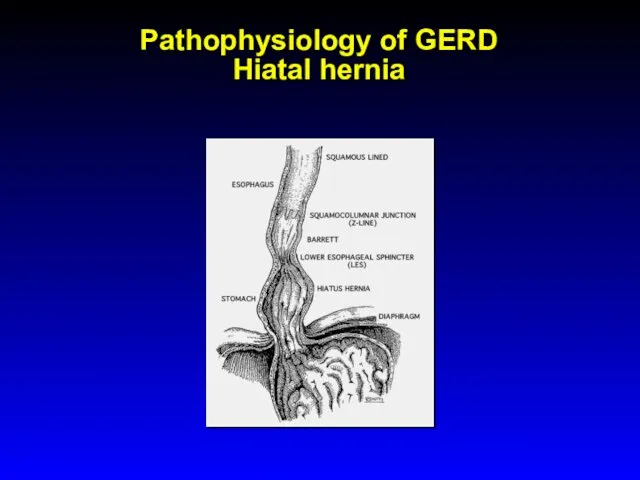
Pathophysiology of GERD
Hiatal hernia
Pathophysiology of GERD
Hiatal hernia
GERD
Epidemiology
Prevalence : 10 -20 % in the Western world , <
GERD
Epidemiology
Prevalence : 10 -20 % in the Western world , <
GERD Symptoms
Common: Heartburn and regurgitation
Less common: dysphagia and chest pain
Extraesophageal manifestations
GERD Symptoms
Common: Heartburn and regurgitation
Less common: dysphagia and chest pain
Extraesophageal manifestations
GERD- Ds
Ds is usually based on clinical symptoms
Utilization of
GERD- Ds
Ds is usually based on clinical symptoms
Utilization of

GERD Differential Diagnosis
Infectious, pill, or eosinophilic esophagitis
Peptic ulcer disease
Dyspepsia
Biliary colic
Coronary artery
GERD Differential Diagnosis
Infectious, pill, or eosinophilic esophagitis
Peptic ulcer disease
Dyspepsia
Biliary colic
Coronary artery
GERD Treatment
Lifestyle modifications
Avoidance of
Foods that reduce LES pressure -"refluxogenic" (fatty
GERD Treatment
Lifestyle modifications
Avoidance of
Foods that reduce LES pressure -"refluxogenic" (fatty
GERD Treatment
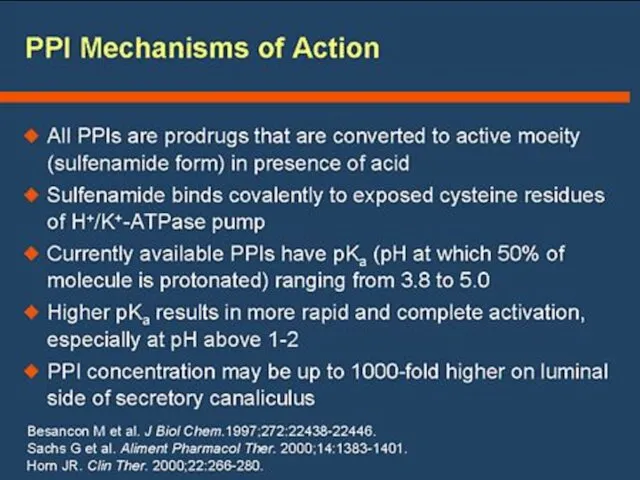
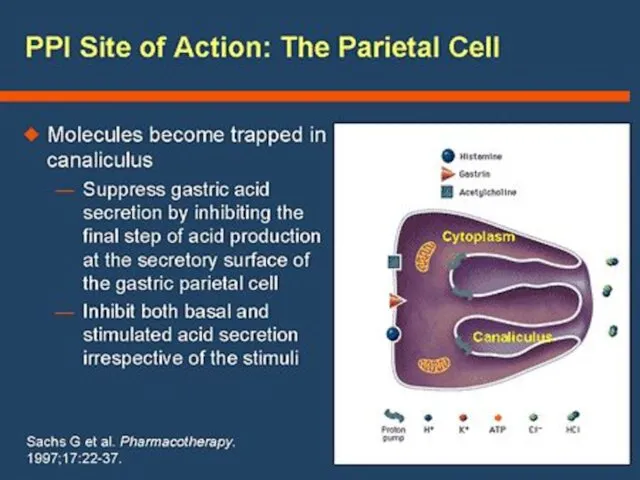
Inhibitors of gastric acid secretion
Reducing the acidity of gastric juice
GERD Treatment
Inhibitors of gastric acid secretion
Reducing the acidity of gastric juice
bv
bv
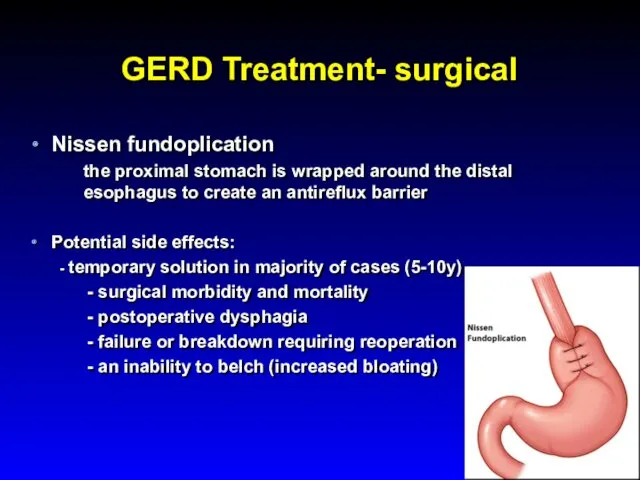
GERD Treatment- surgical
Nissen fundoplication
the proximal stomach is wrapped around the distal
GERD Treatment- surgical
Nissen fundoplication
the proximal stomach is wrapped around the distal
GERD Complications
Chronic esophagitis (bleeding and stricture)
increasingly rare due to potent
GERD Complications
Chronic esophagitis (bleeding and stricture)
increasingly rare due to potent
Barrett’s esophagus
Endoscopy: Tongues of reddish mucosa extending proximally from GE junction
Barrett’s esophagus
Endoscopy: Tongues of reddish mucosa extending proximally from GE junction
Barrett’s esophagus
Histology: columnar metaplasia with Goblet cells
Barrett’s esophagus
Histology: columnar metaplasia with Goblet cells
GERD Complications- Barrett’s
Obese white males in 6th decade of lie are
GERD Complications- Barrett’s
Obese white males in 6th decade of lie are
Dysphagia
Dysphagia
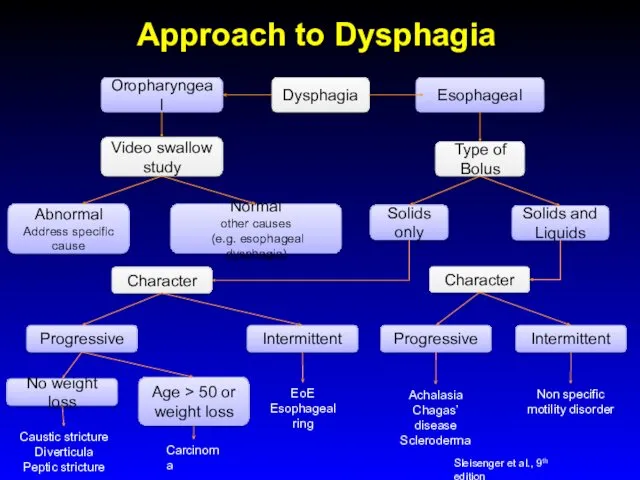
Approach to Dysphagia
Dysphagia
Oropharyngeal
Esophageal
Video swallow study
Type of Bolus
Abnormal
Address specific cause
Normal
other causes
(e.g.
Approach to Dysphagia
Dysphagia
Oropharyngeal
Esophageal
Video swallow study
Type of Bolus
Abnormal
Address specific cause
Normal
other causes
(e.g.
Oropharyngeal Dysphagia
Etiology
Neurogenic - major source of morbidity related to aspiration and
Oropharyngeal Dysphagia
Etiology
Neurogenic - major source of morbidity related to aspiration and
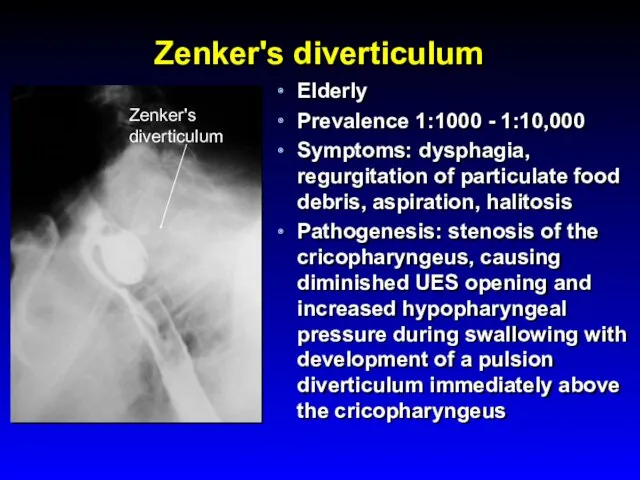
Zenker's diverticulum
Elderly
Prevalence 1:1000 - 1:10,000
Symptoms: dysphagia, regurgitation of
Zenker's diverticulum
Elderly
Prevalence 1:1000 - 1:10,000
Symptoms: dysphagia, regurgitation of
Esophageal Dysphagia
Solid food dysphagia appears when the lumen is <13 mm
Circumferential
Esophageal Dysphagia
Solid food dysphagia appears when the lumen is <13 mm
Circumferential
Esophageal Dysphagia
Structural causes
Schatzki's rings
Eosinophilic esophagitis
Peptic strictures
Neoplasia
GERD without a stricture, perhaps on
Esophageal Dysphagia
Structural causes
Schatzki's rings
Eosinophilic esophagitis
Peptic strictures
Neoplasia
GERD without a stricture, perhaps on
Esophageal Dysphagia
Upper endoscopy
Dysphagia is an alarm symptom
Esophageal manometry
Barium swallow
Esophageal Dysphagia
Upper endoscopy
Dysphagia is an alarm symptom
Esophageal manometry
Barium swallow
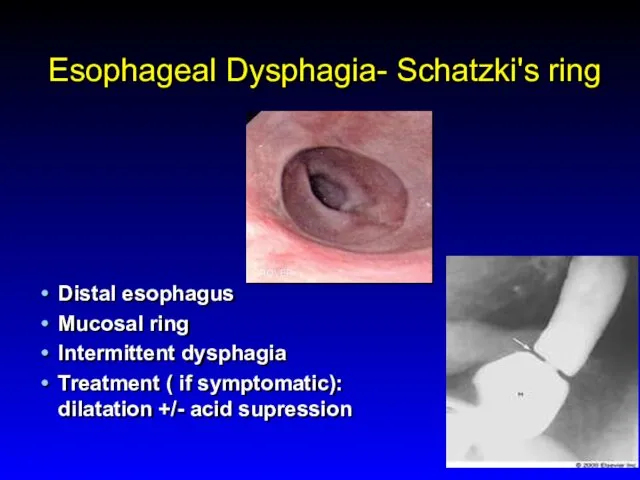
Esophageal Dysphagia- Schatzki's ring
Distal esophagus
Mucosal ring
Intermittent dysphagia
Treatment ( if symptomatic): dilatation
Esophageal Dysphagia- Schatzki's ring
Distal esophagus
Mucosal ring
Intermittent dysphagia
Treatment ( if symptomatic): dilatation
Achalasia
Incidence 1-3:100,000
Age - 25 to 60 yo
Symptoms
Dysphagia: solid and liquid
Achalasia
Incidence 1-3:100,000
Age - 25 to 60 yo
Symptoms
Dysphagia: solid and liquid
Achalasia
Etiology:
Loss of ganglion cells- inhibitory (nitric oxide) ganglionic neurons
Achalasia
Etiology:
Loss of ganglion cells- inhibitory (nitric oxide) ganglionic neurons
Achalasia
Differential diagnosis
Diffuse esopghageal spasm (DES)
Chagas' disease (Trypanosoma cruzi)
-The
Achalasia
Differential diagnosis
Diffuse esopghageal spasm (DES)
Chagas' disease (Trypanosoma cruzi)
-The
Achalasia Diagnosis
Endoscopy
- rarely diagnostic, to exclude pseudo-achalasia
Manometry
- most
Achalasia Diagnosis
Endoscopy
- rarely diagnostic, to exclude pseudo-achalasia
Manometry
- most
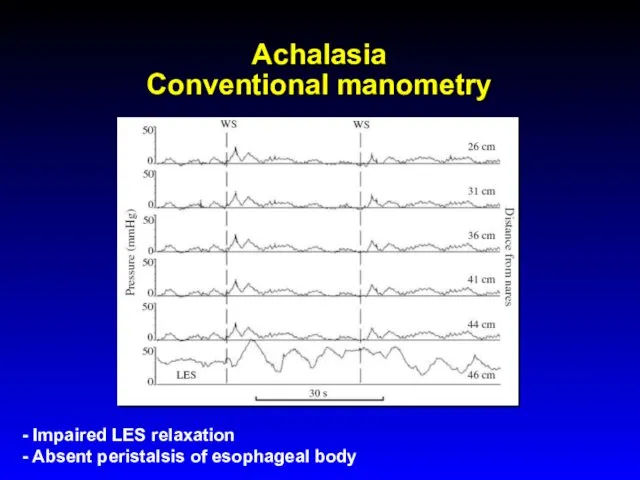
Achalasia
Conventional manometry
- Impaired LES relaxation
- Absent peristalsis of esophageal body
Achalasia
Conventional manometry
- Impaired LES relaxation
- Absent peristalsis of esophageal body
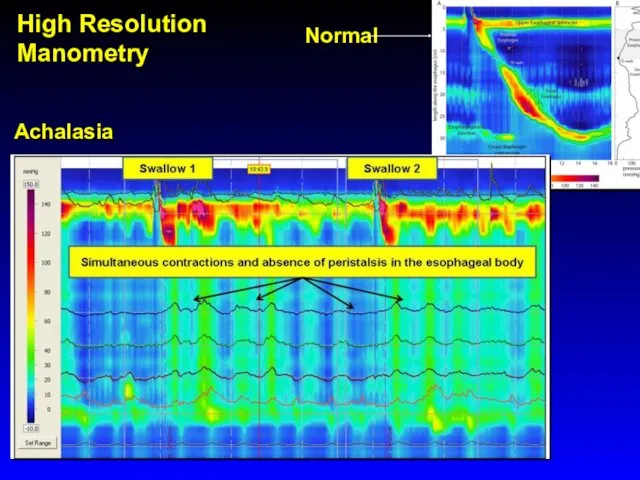
Achalasia
Normal
High Resolution Manometry
Achalasia
Normal
High Resolution Manometry
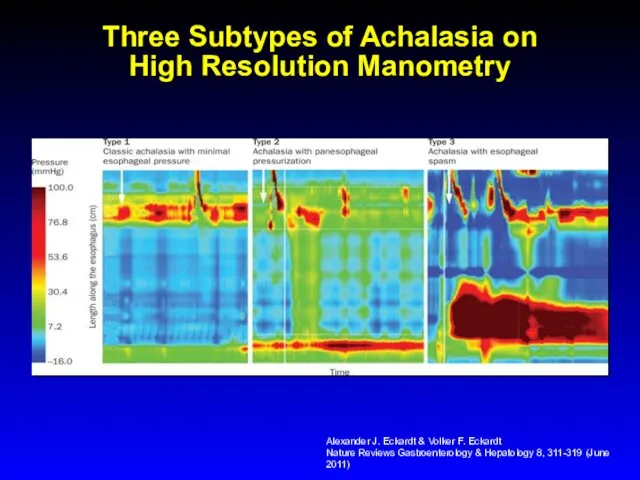
Three Subtypes of Achalasia on
High Resolution Manometry
Alexander J. Eckardt & Volker
Three Subtypes of Achalasia on
High Resolution Manometry
Alexander J. Eckardt & Volker
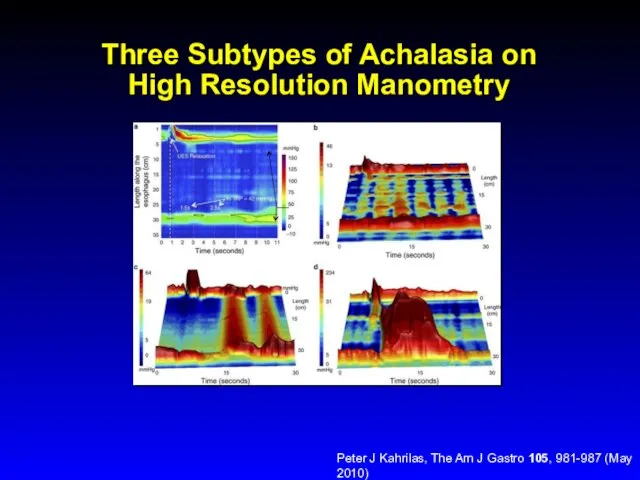
Three Subtypes of Achalasia on
High Resolution Manometry
Peter J Kahrilas, The Am
Three Subtypes of Achalasia on
High Resolution Manometry
Peter J Kahrilas, The Am
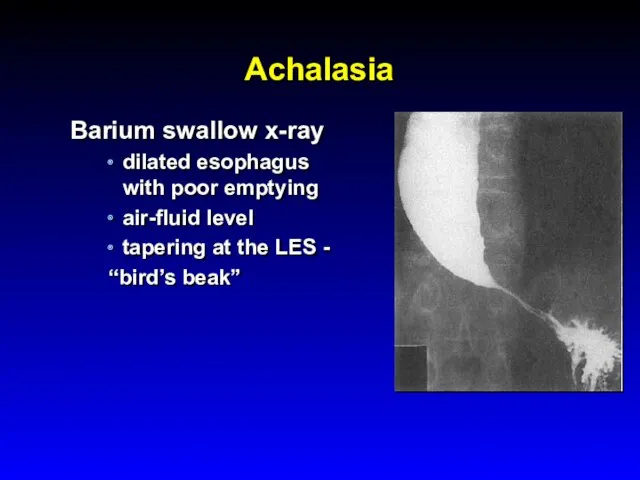
Achalasia
Barium swallow x-ray
dilated esophagus with poor emptying
air-fluid level
tapering at the LES
Achalasia
Barium swallow x-ray
dilated esophagus with poor emptying
air-fluid level
tapering at the LES
Achalasia Treatment
Therapy is directed at reducing LES pressure
Pharmacologicals therapies are
Achalasia Treatment
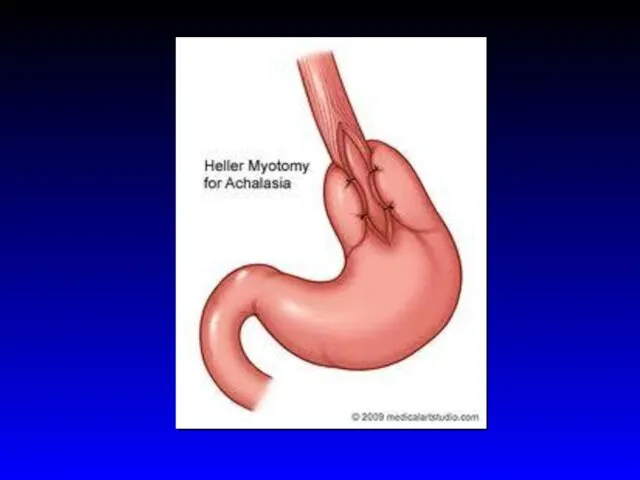
Therapy is directed at reducing LES pressure
Pharmacologicals therapies are
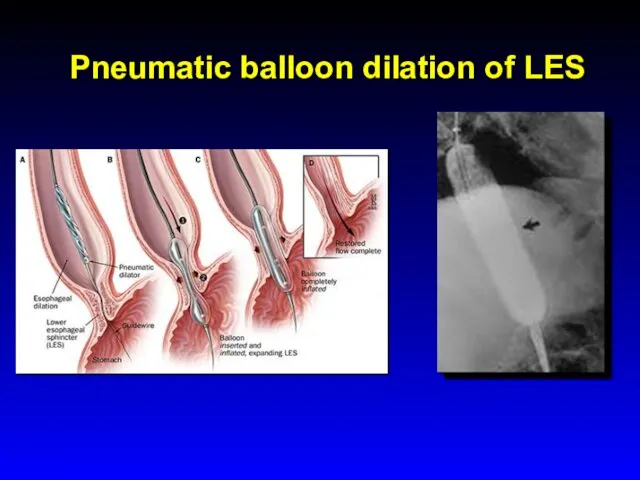
Pneumatic balloon dilation of LES
Pneumatic balloon dilation of LES
Achalasia- Complications
Squamous cell carcinoma risk increased 17-fold in inadequately treated achalasia
Achalasia- Complications
Squamous cell carcinoma risk increased 17-fold in inadequately treated achalasia
Diffuse Esophageal Spasm (DES)
Episodes of dysphagia and chest pain attributable to
Diffuse Esophageal Spasm (DES)
Episodes of dysphagia and chest pain attributable to
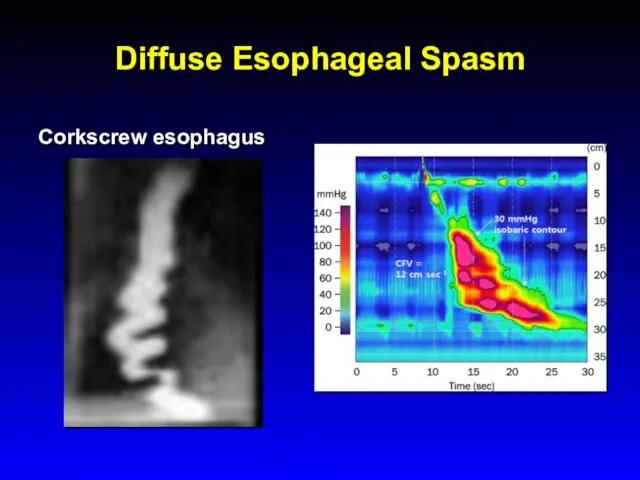
Diffuse Esophageal Spasm
Corkscrew esophagus
Diffuse Esophageal Spasm
Corkscrew esophagus
Dysphagia
Diffuse Esophageal Spasm (DES)
Diffferntial diagnosis:
angina pectoris
peptic or infectious esophagitis
Achalasia
Treatment
- Partial
Dysphagia
Diffuse Esophageal Spasm (DES)
Diffferntial diagnosis:
angina pectoris
peptic or infectious esophagitis
Achalasia
Treatment
- Partial
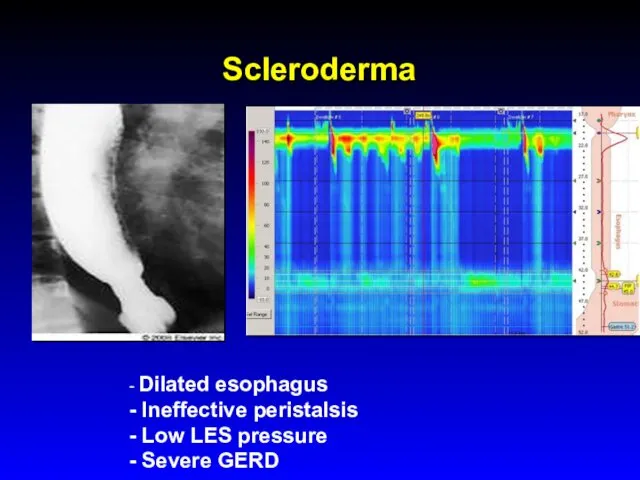
Scleroderma
- Dilated esophagus
- Ineffective peristalsis
- Low LES pressure
- Severe GERD
Scleroderma
- Dilated esophagus
- Ineffective peristalsis
- Low LES pressure
- Severe GERD
Eosinophilic Esophagitis
Prevalence 1:1000 with a predilection for white males, incidence is
Eosinophilic Esophagitis
Prevalence 1:1000 with a predilection for white males, incidence is
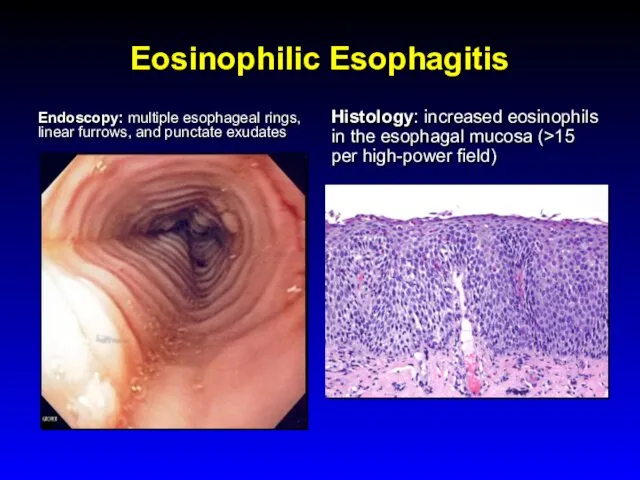
Eosinophilic Esophagitis
Endoscopy: multiple esophageal rings, linear furrows, and punctate exudates
Histology:
Eosinophilic Esophagitis
Endoscopy: multiple esophageal rings, linear furrows, and punctate exudates
Histology:
Eosinophilic Esophagitis
Complications: food impaction and esophageal perforation
Treatment:
Dietary restrictions
PPIs
Systemic or topical
Eosinophilic Esophagitis
Complications: food impaction and esophageal perforation
Treatment:
Dietary restrictions
PPIs
Systemic or topical
Infectious Esophagitis
Common infections in Immunocompromized pts (organ transplantation, chronic inflammatory diseases,
Infectious Esophagitis
Common infections in Immunocompromized pts (organ transplantation, chronic inflammatory diseases,
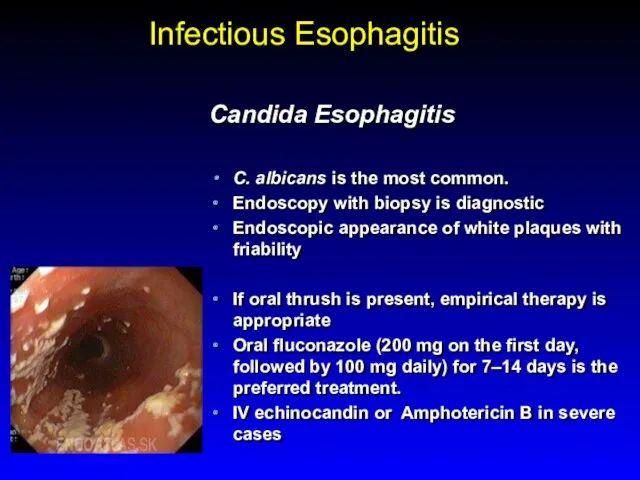
Infectious Esophagitis
Candida Esophagitis
C. albicans is the most common.
Endoscopy with biopsy
Infectious Esophagitis
Candida Esophagitis
C. albicans is the most common.
Endoscopy with biopsy
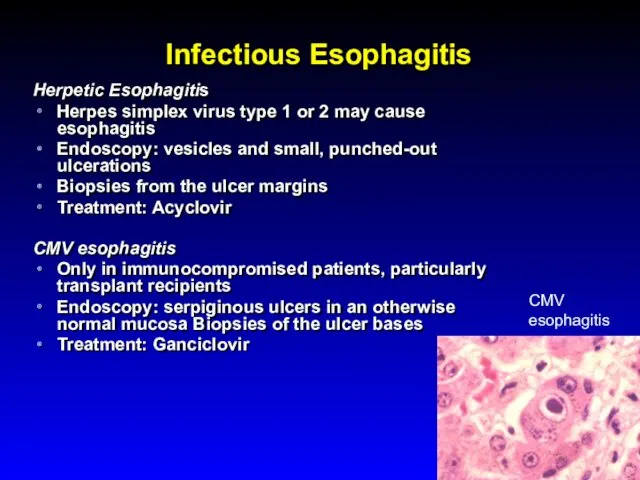
Infectious Esophagitis
Herpetic Esophagitis
Herpes simplex virus type 1 or 2 may cause
Infectious Esophagitis
Herpetic Esophagitis
Herpes simplex virus type 1 or 2 may cause
Other Types of Esopahgitis
Radiation esopahgitis
Pill- induced esophagitis
doxyclin, tertacyclin, minocycline, peniciliin, clindamycin,
Other Types of Esopahgitis
Radiation esopahgitis
Pill- induced esophagitis
doxyclin, tertacyclin, minocycline, peniciliin, clindamycin,
Esophageal Cancer
Squamous cell carcinoma
Adenocarcinoma
Esophageal Cancer
Squamous cell carcinoma
Adenocarcinoma
Esophageal Cancer
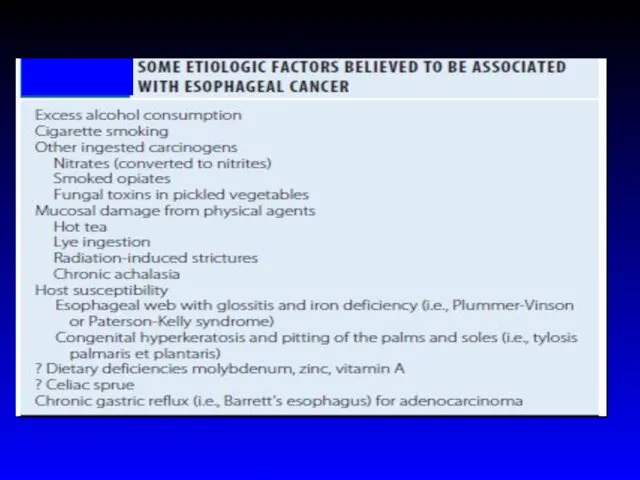
Squamous cell carcinoma risk factors:
excess alcohol consumption and/or cigarette smoking
ingestion
Esophageal Cancer
Squamous cell carcinoma risk factors:
excess alcohol consumption and/or cigarette smoking
ingestion
Esophageal Cancer
incidence of squamous cell cancer decreases over the past 30
Esophageal Cancer
incidence of squamous cell cancer decreases over the past 30
Esophageal Cancer
Adenocarcinomas arise in the distal esophagus in the presence of
Esophageal Cancer
Adenocarcinomas arise in the distal esophagus in the presence of
Esophageal Cancer
Location
10% upper third of the sophagus
35% in the middle
Esophageal Cancer
Location
10% upper third of the sophagus
35% in the middle
Clinical features
Progressive dysphagia (solids)
Weight loss
When these symptoms develop, the disease is
Clinical features
Progressive dysphagia (solids)
Weight loss
When these symptoms develop, the disease is
Esophageal carcinoma
Endoscopic and cytologic screening for carcinoma in patients with Barrett’s
Esophageal carcinoma
Endoscopic and cytologic screening for carcinoma in patients with Barrett’s
 Природные сообщества
Природные сообщества Удобрения, их свойства и применение
Удобрения, их свойства и применение Цитология. Строение биомембраны
Цитология. Строение биомембраны Фитонцидная активность комнатных растений
Фитонцидная активность комнатных растений Ствол мозга и мозжечок
Ствол мозга и мозжечок Пищеварительные железы
Пищеварительные железы Презентация к уроку биологии по теме Основные систематические группы рыб
Презентация к уроку биологии по теме Основные систематические группы рыб Антропогенез. Этапы эволюции человека
Антропогенез. Этапы эволюции человека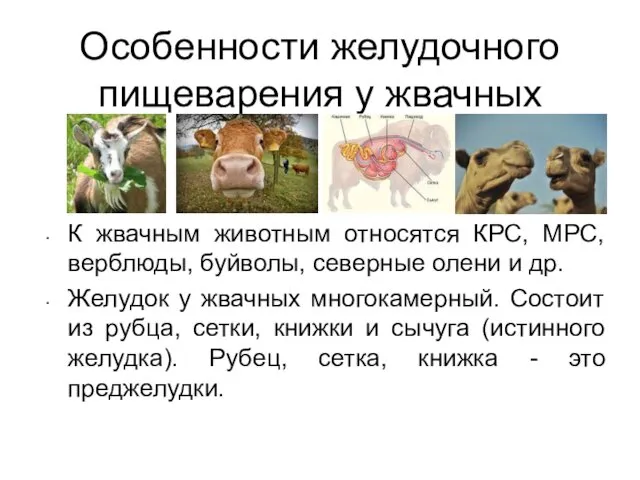 Особенности желудочного пищеварения у жвачных
Особенности желудочного пищеварения у жвачных Внутренняя среда организма. Значение крови и ее состав. 8 класс
Внутренняя среда организма. Значение крови и ее состав. 8 класс Природа в опасности. Многообразие растительного и животного мира
Природа в опасности. Многообразие растительного и животного мира Презентация к уроку 10 класс. Онтогенез. Постэмбриональное развитие
Презентация к уроку 10 класс. Онтогенез. Постэмбриональное развитие Внутренняя среда организма
Внутренняя среда организма Строение голосового аппарата
Строение голосового аппарата Экологическая викторина. Чудеса природы
Экологическая викторина. Чудеса природы Королевский попугай, бигль, померанский щпиц, хомяк, шиншилла, крыса, кошка, суматранский барбус
Королевский попугай, бигль, померанский щпиц, хомяк, шиншилла, крыса, кошка, суматранский барбус Основные элементы биотехнологических процессов
Основные элементы биотехнологических процессов Мочеполовой аппарат. Органы мочеотделения. (Лекция 5)
Мочеполовой аппарат. Органы мочеотделения. (Лекция 5) Характерные особенности строения головы человека
Характерные особенности строения головы человека Екологічні групи рослин по відношенню до вологи
Екологічні групи рослин по відношенню до вологи Гүлдің құрылысы
Гүлдің құрылысы Презентация к уроку Общая характеристика класса Млекопитающих
Презентация к уроку Общая характеристика класса Млекопитающих Вегетативне розмноження рослин
Вегетативне розмноження рослин Влияние спиртов на организм человека
Влияние спиртов на организм человека Отряды млекопитающих
Отряды млекопитающих презентация 9 класс идея развития органического мира
презентация 9 класс идея развития органического мира Многообразие растений семейства сложноцветных
Многообразие растений семейства сложноцветных Рослинні тканини
Рослинні тканини