- General Musculoskeletal Screening: Upper Extremities

Содержание
- 2. 8/27/02 Gregory Crovetti, M.D. General Approach History Inspection Range of Motion (ROM) Palpation Muscular and neurological
- 3. 8/27/02 Gregory Crovetti, M.D. History An accurate history is essential Will give you diagnosis 80-90% of
- 4. 8/27/02 Gregory Crovetti, M.D. General Inspection Observe how the patient moves as they go into the
- 5. 8/27/02 Gregory Crovetti, M.D. Inspection of Specific Area Look for asymmetry between sides Swelling Deformities Atrophy
- 6. 8/27/02 Gregory Crovetti, M.D. Range of Motion (Active) Have patient range the joints Watch for decreased
- 7. 8/27/02 Gregory Crovetti, M.D. Range of Motion (Passive) Next range the joints passively, comparing the end
- 8. 8/27/02 Gregory Crovetti, M.D. Palpation When palpating a structure, you need to know the anatomy of
- 9. 8/27/02 Gregory Crovetti, M.D. Muscular and Neurological Check the following comparing one side to the other:
- 10. 8/27/02 Gregory Crovetti, M.D. Generalized Screening Exam If any abnormalities, a more thorough exam of the
- 11. 8/27/02 Gregory Crovetti, M.D. Neck: Active Range of Motion Chin to chest (flexion) “look at ceiling”
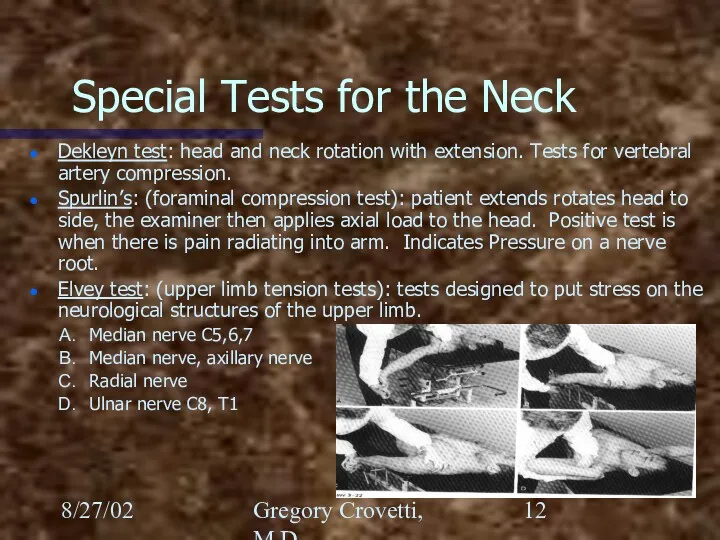
- 12. 8/27/02 Gregory Crovetti, M.D. Special Tests for the Neck Dekleyn test: head and neck rotation with
- 13. 8/27/02 Gregory Crovetti, M.D. Shoulder Exam Inspection Palpation Passive Range of Motion Active Range of Motion
- 14. 8/27/02 Gregory Crovetti, M.D. The Shoulder Joints of the shoulder Glenohumeral Sternoclavicular Acromioclavicular Scapular thoracic (not
- 15. 8/27/02 Gregory Crovetti, M.D. Glenohumeral Joint
- 16. 8/27/02 Gregory Crovetti, M.D. Glenohumeral Ligaments Folds in the anterior capsule produce the superior, middle and
- 17. 8/27/02 Gregory Crovetti, M.D. Glenoid Labrum Glenoid labrum: a fibrocartilaginous rim to increase the contact area
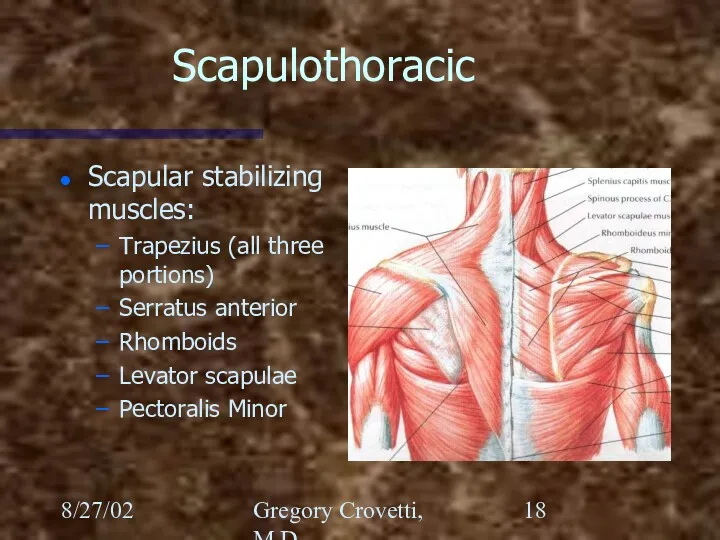
- 18. 8/27/02 Gregory Crovetti, M.D. Scapulothoracic Scapular stabilizing muscles: Trapezius (all three portions) Serratus anterior Rhomboids Levator
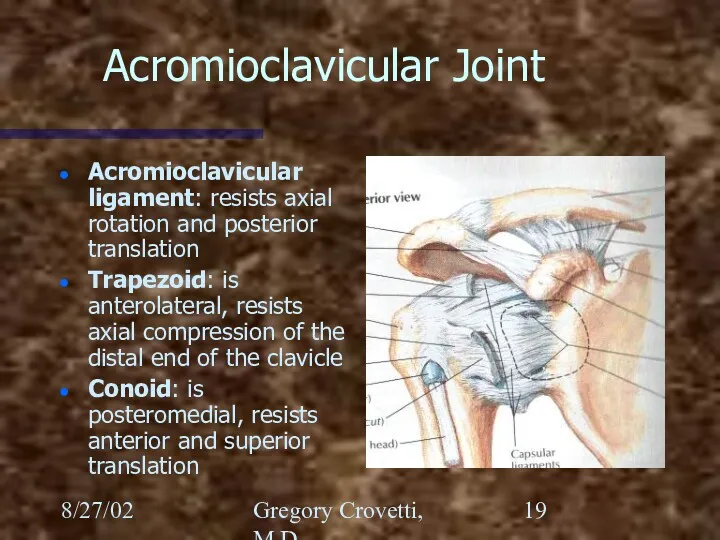
- 19. 8/27/02 Gregory Crovetti, M.D. Acromioclavicular Joint Acromioclavicular ligament: resists axial rotation and posterior translation Trapezoid: is
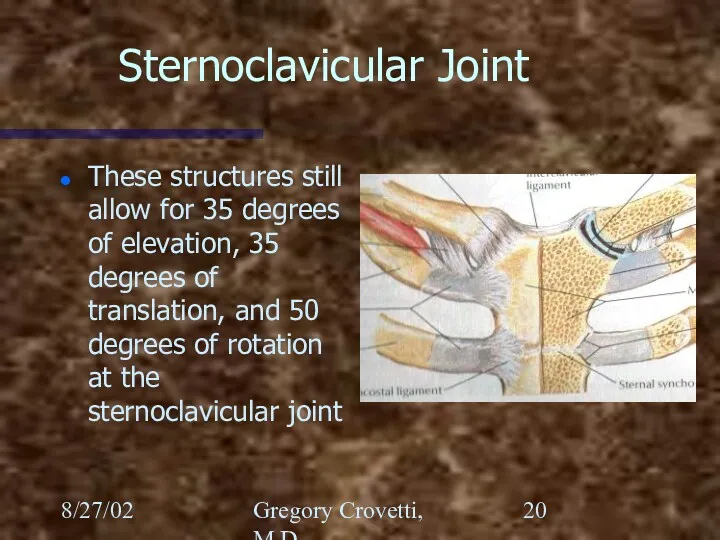
- 20. 8/27/02 Gregory Crovetti, M.D. Sternoclavicular Joint These structures still allow for 35 degrees of elevation, 35
- 21. 8/27/02 Gregory Crovetti, M.D. Shoulder Palpation of the shoulder includes: Sternoclavicular joint Acromioclavicular joint Subacromial area
- 22. 8/27/02 Gregory Crovetti, M.D. Shoulder Rotator cuff: Supraspinatus Infraspinatus Teres Minor Subscapularis
- 23. 8/27/02 Gregory Crovetti, M.D.
- 24. 8/27/02 Gregory Crovetti, M.D. Special Tests for the Shoulder Apprehension (crank) test: The arm is abducted
- 25. 8/27/02 Gregory Crovetti, M.D. Special Tests for the Shoulder Feagin test: arm abducted to 90 elbow
- 26. 8/27/02 Gregory Crovetti, M.D. Special Tests for the Shoulder Yergason’s test: Elbow flexed to 90 degrees,
- 27. 8/27/02 Gregory Crovetti, M.D. Special Tests for the Shoulder Impingement test: Arm is abducted to 90
- 28. 8/27/02 Gregory Crovetti, M.D. The Elbow Palpation: lateral and medial epicondyles, olecranon, radial head, groove on
- 29. 8/27/02 Gregory Crovetti, M.D.
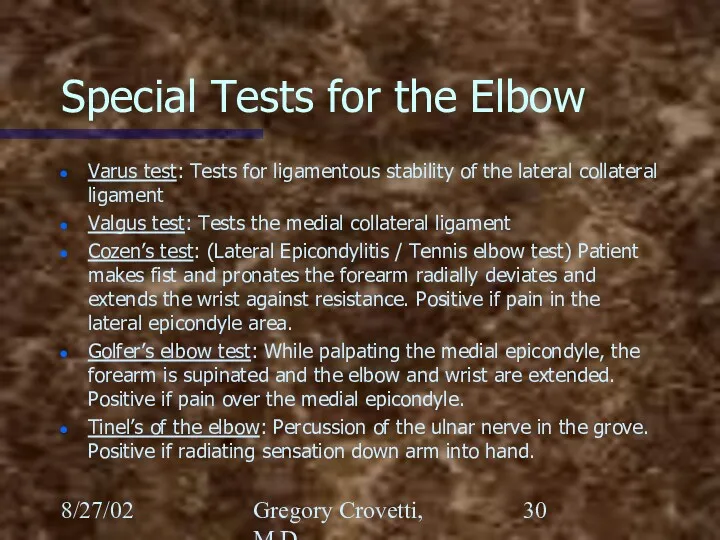
- 30. 8/27/02 Gregory Crovetti, M.D. Special Tests for the Elbow Varus test: Tests for ligamentous stability of
- 31. 8/27/02 Gregory Crovetti, M.D. Wrist and Hand Inspect for swelling or deformities Palpate: anatomic snuff box,
- 32. 8/27/02 Gregory Crovetti, M.D. Bones of the Wrist Scaphoid Lunate Triquetrum Pisiform Trapezium Trapezoid Capitate Hamate
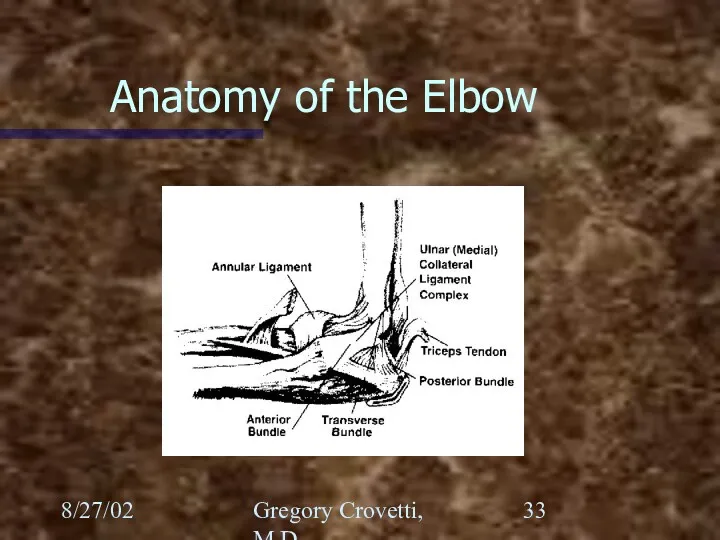
- 33. 8/27/02 Gregory Crovetti, M.D. Anatomy of the Elbow
- 34. 8/27/02 Gregory Crovetti, M.D. Nerves of the Hand Ulnar Radial Median Palmar branch of the median
- 35. 8/27/02 Gregory Crovetti, M.D.
- 36. 8/27/02 Gregory Crovetti, M.D.
- 37. 8/27/02 Gregory Crovetti, M.D.
- 38. 8/27/02 Gregory Crovetti, M.D. Special Tests of Hand and Wrist Cascade sign: Patient flexes the fingers,
- 39. 8/27/02 Gregory Crovetti, M.D. Special Tests of Hand and Wrist Trigger finger: Results from a thickening
- 40. 8/27/02 Gregory Crovetti, M.D. Special Tests of Hand and Wrist Ganglion cyst: Localized swelling usually on
- 41. 8/27/02 Gregory Crovetti, M.D. Special Tests of Hand and Wrist Guyon’s canal: (pisohamate) Through this canal
- 42. 8/27/02 Gregory Crovetti, M.D. Special Tests of Hand and Wrist Watson (scaphoid shift) test: The patient’s
- 43. 8/27/02 Gregory Crovetti, M.D. Special Tests of Hand and Wrist Finkelstein test: Tests for De Quervain’s
- 45. Скачать презентацию
8/27/02
Gregory Crovetti, M.D.
General Approach
History
Inspection
Range of Motion (ROM)
Palpation
Muscular and neurological exams
8/27/02
Gregory Crovetti, M.D.
General Approach
History
Inspection
Range of Motion (ROM)
Palpation
Muscular and neurological exams
8/27/02
Gregory Crovetti, M.D.
History
An accurate history is essential
Will give you diagnosis 80-90%
8/27/02
Gregory Crovetti, M.D.
History
An accurate history is essential
Will give you diagnosis 80-90%
8/27/02
Gregory Crovetti, M.D.
General Inspection
Observe how the patient moves as they go
8/27/02
Gregory Crovetti, M.D.
General Inspection
Observe how the patient moves as they go
8/27/02
Gregory Crovetti, M.D.
Inspection of Specific Area
Look for asymmetry between sides
Swelling
Deformities
Atrophy
Erythema
8/27/02
Gregory Crovetti, M.D.
Inspection of Specific Area
Look for asymmetry between sides
Swelling
Deformities
Atrophy
Erythema
8/27/02
Gregory Crovetti, M.D.
Range of Motion (Active)
Have patient range the joints
Watch for
8/27/02
Gregory Crovetti, M.D.
Range of Motion (Active)
Have patient range the joints
Watch for
8/27/02
Gregory Crovetti, M.D.
Range of Motion (Passive)
Next range the joints passively, comparing
8/27/02
Gregory Crovetti, M.D.
Range of Motion (Passive)
Next range the joints passively, comparing
8/27/02
Gregory Crovetti, M.D.
Palpation
When palpating a structure, you need to know the
8/27/02
Gregory Crovetti, M.D.
Palpation
When palpating a structure, you need to know the
8/27/02
Gregory Crovetti, M.D.
Muscular and Neurological
Check the following comparing one side to
8/27/02
Gregory Crovetti, M.D.
Muscular and Neurological
Check the following comparing one side to
8/27/02
Gregory Crovetti, M.D.
Generalized Screening Exam
If any abnormalities, a more thorough exam
8/27/02
Gregory Crovetti, M.D.
Generalized Screening Exam
If any abnormalities, a more thorough exam
8/27/02
Gregory Crovetti, M.D.
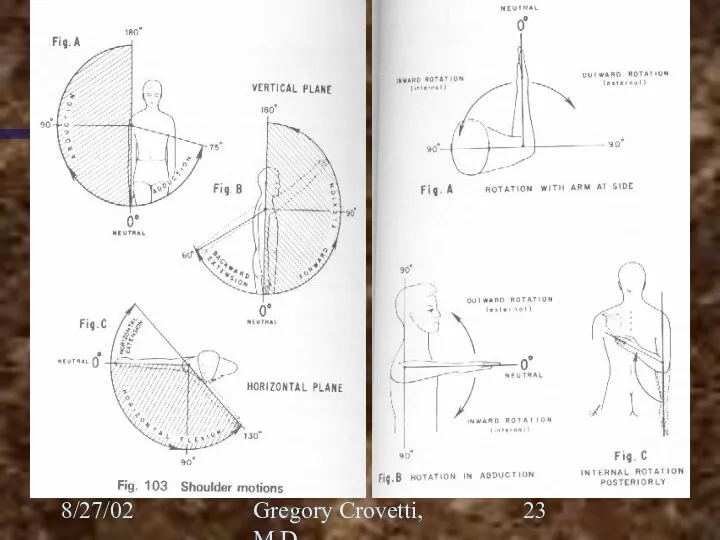
Neck: Active Range of Motion
Chin to chest (flexion)
“look at
8/27/02
Gregory Crovetti, M.D.
Neck: Active Range of Motion
Chin to chest (flexion)
“look at
8/27/02
Gregory Crovetti, M.D.
Special Tests for the Neck
Dekleyn test: head and neck
8/27/02
Gregory Crovetti, M.D.
Special Tests for the Neck
Dekleyn test: head and neck
8/27/02
Gregory Crovetti, M.D.
Shoulder Exam
Inspection
Palpation
Passive Range of Motion
Active Range of Motion
Appley scratch
8/27/02
Gregory Crovetti, M.D.
Shoulder Exam
Inspection
Palpation
Passive Range of Motion
Active Range of Motion
Appley scratch
8/27/02
Gregory Crovetti, M.D.
The Shoulder
Joints of the shoulder
Glenohumeral
Sternoclavicular
Acromioclavicular
Scapular thoracic (not a true
8/27/02
Gregory Crovetti, M.D.
The Shoulder
Joints of the shoulder
Glenohumeral
Sternoclavicular
Acromioclavicular
Scapular thoracic (not a true
8/27/02
Gregory Crovetti, M.D.
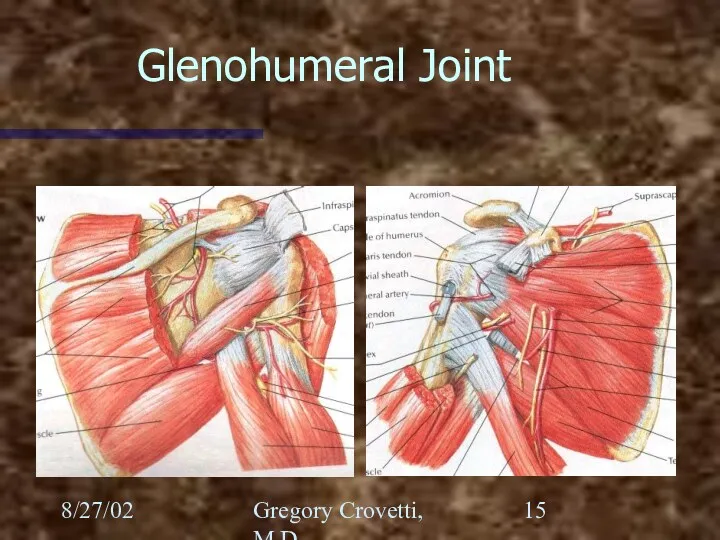
Glenohumeral Joint
8/27/02
Gregory Crovetti, M.D.
Glenohumeral Joint
8/27/02
Gregory Crovetti, M.D.
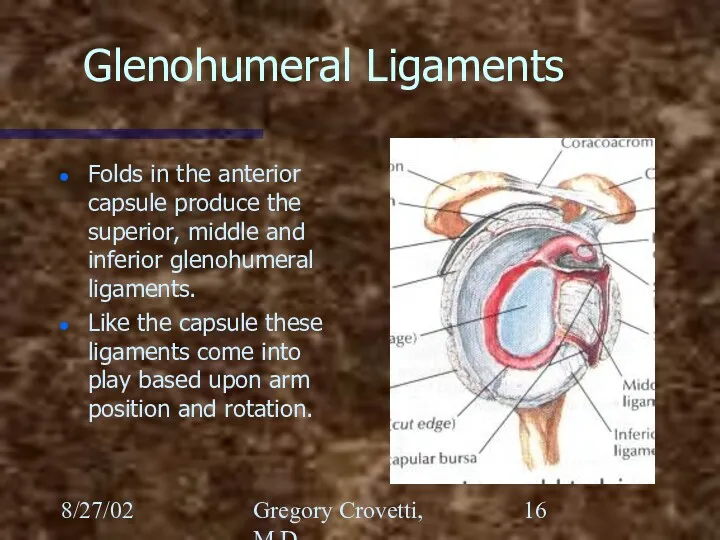
Glenohumeral Ligaments
Folds in the anterior capsule produce the superior,
8/27/02
Gregory Crovetti, M.D.
Glenohumeral Ligaments
Folds in the anterior capsule produce the superior,
8/27/02
Gregory Crovetti, M.D.
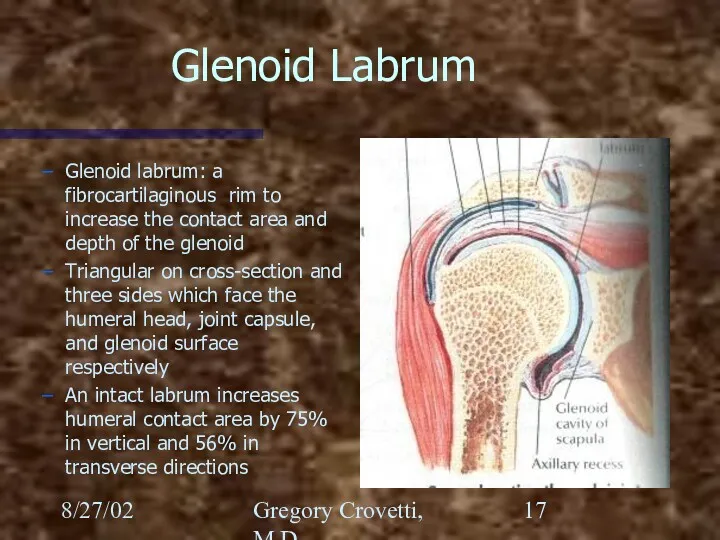
Glenoid Labrum
Glenoid labrum: a fibrocartilaginous rim to increase the
8/27/02
Gregory Crovetti, M.D.
Glenoid Labrum
Glenoid labrum: a fibrocartilaginous rim to increase the
8/27/02
Gregory Crovetti, M.D.
Scapulothoracic
Scapular stabilizing muscles:
Trapezius (all three portions)
Serratus anterior
Rhomboids
Levator scapulae
Pectoralis Minor
8/27/02
Gregory Crovetti, M.D.
Scapulothoracic
Scapular stabilizing muscles:
Trapezius (all three portions)
Serratus anterior
Rhomboids
Levator scapulae
Pectoralis Minor
8/27/02
Gregory Crovetti, M.D.
Acromioclavicular Joint
Acromioclavicular ligament: resists axial rotation and posterior translation
Trapezoid:
8/27/02
Gregory Crovetti, M.D.
Acromioclavicular Joint
Acromioclavicular ligament: resists axial rotation and posterior translation
Trapezoid:
8/27/02
Gregory Crovetti, M.D.
Sternoclavicular Joint
These structures still allow for 35 degrees of
8/27/02
Gregory Crovetti, M.D.
Sternoclavicular Joint
These structures still allow for 35 degrees of
8/27/02
Gregory Crovetti, M.D.
Shoulder
Palpation of the shoulder includes:
Sternoclavicular joint
Acromioclavicular joint
Subacromial area
Bicipital
8/27/02
Gregory Crovetti, M.D.
Shoulder
Palpation of the shoulder includes:
Sternoclavicular joint
Acromioclavicular joint
Subacromial area
Bicipital
8/27/02
Gregory Crovetti, M.D.
Shoulder
Rotator cuff:
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis
8/27/02
Gregory Crovetti, M.D.
Shoulder
Rotator cuff:
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis
8/27/02
Gregory Crovetti, M.D.
8/27/02
Gregory Crovetti, M.D.
8/27/02
Gregory Crovetti, M.D.
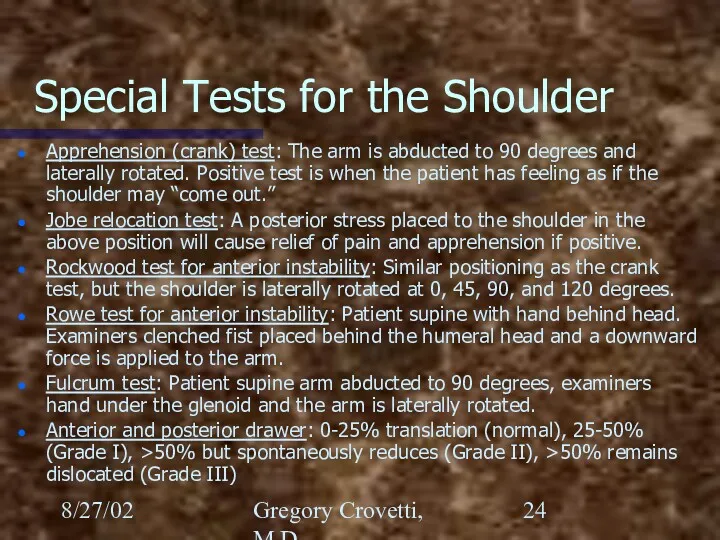
Special Tests for the Shoulder
Apprehension (crank) test: The arm
8/27/02
Gregory Crovetti, M.D.
Special Tests for the Shoulder
Apprehension (crank) test: The arm
8/27/02
Gregory Crovetti, M.D.
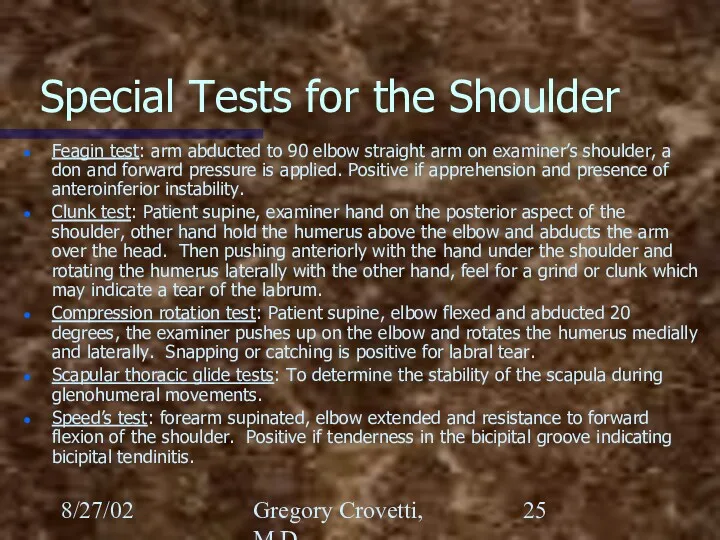
Special Tests for the Shoulder
Feagin test: arm abducted to
8/27/02
Gregory Crovetti, M.D.
Special Tests for the Shoulder
Feagin test: arm abducted to
8/27/02
Gregory Crovetti, M.D.
Special Tests for the Shoulder
Yergason’s test: Elbow flexed to
8/27/02
Gregory Crovetti, M.D.
Special Tests for the Shoulder
Yergason’s test: Elbow flexed to
8/27/02
Gregory Crovetti, M.D.
Special Tests for the Shoulder
Impingement test: Arm is abducted
8/27/02
Gregory Crovetti, M.D.
Special Tests for the Shoulder
Impingement test: Arm is abducted
8/27/02
Gregory Crovetti, M.D.
The Elbow
Palpation: lateral and medial epicondyles, olecranon, radial head,
8/27/02
Gregory Crovetti, M.D.
The Elbow
Palpation: lateral and medial epicondyles, olecranon, radial head,
8/27/02
Gregory Crovetti, M.D.
8/27/02
Gregory Crovetti, M.D.
8/27/02
Gregory Crovetti, M.D.
Special Tests for the Elbow
Varus test: Tests for ligamentous
8/27/02
Gregory Crovetti, M.D.
Special Tests for the Elbow
Varus test: Tests for ligamentous
8/27/02
Gregory Crovetti, M.D.
Wrist and Hand
Inspect for swelling or deformities
Palpate: anatomic snuff
8/27/02
Gregory Crovetti, M.D.
Wrist and Hand
Inspect for swelling or deformities
Palpate: anatomic snuff
8/27/02
Gregory Crovetti, M.D.
Bones of the Wrist
Scaphoid
Lunate
Triquetrum
Pisiform
Trapezium
Trapezoid
Capitate
Hamate
8/27/02
Gregory Crovetti, M.D.
Bones of the Wrist
Scaphoid
Lunate
Triquetrum
Pisiform
Trapezium
Trapezoid
Capitate
Hamate
8/27/02
Gregory Crovetti, M.D.
Anatomy of the Elbow
8/27/02
Gregory Crovetti, M.D.
Anatomy of the Elbow
8/27/02
Gregory Crovetti, M.D.
Nerves of the Hand
Ulnar
Radial
Median
Palmar branch of the median
8/27/02
Gregory Crovetti, M.D.
Nerves of the Hand
Ulnar
Radial
Median
Palmar branch of the median
8/27/02
Gregory Crovetti, M.D.
8/27/02
Gregory Crovetti, M.D.
8/27/02
Gregory Crovetti, M.D.
8/27/02
Gregory Crovetti, M.D.
8/27/02
Gregory Crovetti, M.D.
8/27/02
Gregory Crovetti, M.D.
8/27/02
Gregory Crovetti, M.D.
Special Tests of Hand and Wrist
Cascade sign: Patient flexes
8/27/02
Gregory Crovetti, M.D.
Special Tests of Hand and Wrist
Cascade sign: Patient flexes
8/27/02
Gregory Crovetti, M.D.
Special Tests of Hand and Wrist
Trigger finger: Results from
8/27/02
Gregory Crovetti, M.D.
Special Tests of Hand and Wrist
Trigger finger: Results from
8/27/02
Gregory Crovetti, M.D.
Special Tests of Hand and Wrist
Ganglion cyst: Localized swelling
8/27/02
Gregory Crovetti, M.D.
Special Tests of Hand and Wrist
Ganglion cyst: Localized swelling
8/27/02
Gregory Crovetti, M.D.
Special Tests of Hand and Wrist
Guyon’s canal: (pisohamate) Through
8/27/02
Gregory Crovetti, M.D.
Special Tests of Hand and Wrist
Guyon’s canal: (pisohamate) Through
8/27/02
Gregory Crovetti, M.D.
Special Tests of Hand and Wrist
Watson (scaphoid shift) test:
8/27/02
Gregory Crovetti, M.D.
Special Tests of Hand and Wrist
Watson (scaphoid shift) test:
8/27/02
Gregory Crovetti, M.D.
Special Tests of Hand and Wrist
Finkelstein test: Tests for
8/27/02
Gregory Crovetti, M.D.
Special Tests of Hand and Wrist
Finkelstein test: Tests for
 Класс Птицы
Класс Птицы Виноград. Види винограда
Виноград. Види винограда Урок по биологии в 5 классе Жизнь в мировом океане
Урок по биологии в 5 классе Жизнь в мировом океане Мутационная изменчивость. Закон гомологических рядов
Мутационная изменчивость. Закон гомологических рядов Влияние человека на экосистемы
Влияние человека на экосистемы Животные Австралии
Животные Австралии Органическое вещество почв. (Лекция 8)
Органическое вещество почв. (Лекция 8) Исследовательская работа
Исследовательская работа Взаимосвязи компонентов природы. Природный комплекс. (проект Урок в Москве)
Взаимосвязи компонентов природы. Природный комплекс. (проект Урок в Москве) Местообитание и экологические ниши
Местообитание и экологические ниши Учение об эволюции
Учение об эволюции Основные этапы развития генетики
Основные этапы развития генетики Презентация Человек как житель биосферы
Презентация Человек как житель биосферы Строение и функции головного мозга
Строение и функции головного мозга Хризантема овощная
Хризантема овощная Группа праголосеменные растения
Группа праголосеменные растения тема Водоросли
тема Водоросли Клетка – элементарная единица жизни на земле
Клетка – элементарная единица жизни на земле Мал өсіру әдістері
Мал өсіру әдістері Tissue system in plants
Tissue system in plants Як змінюється восени життя птахів. Перелітні та осілі птахи
Як змінюється восени життя птахів. Перелітні та осілі птахи Строение нейрона. Синапс
Строение нейрона. Синапс Творческое объединение Друзья природы
Творческое объединение Друзья природы Семя - орган размножения и расселения растений
Семя - орган размножения и расселения растений Тимофеев-Ресовский Н.В (1900-1981)
Тимофеев-Ресовский Н.В (1900-1981) Значение комнатных растений в жизни человека
Значение комнатных растений в жизни человека Физиология высшей нервной деятельности
Физиология высшей нервной деятельности Выделительная система
Выделительная система