- Spirochaetales. Treponema Borrelia & Leptospira

Содержание
- 3. Order: Spirochaetales Family: Spirochaetaceae Genus: Treponema Borrelia Family: Leptospiraceae Genus: Leptospira Taxonomy
- 4. General Overview of Spirochaetales Gram-negative spirochetes Spirochete from Greek for “coiled hair” Extremely thin and can
- 5. Periplasmic Flagella Diagram
- 6. Tightly Coiled Spirochete
- 7. Cross-Section of Spirochete with Periplasmic Flagella NOTE: a.k.a., endoflagella, axial fibrils or axial filaments. (Outer sheath)
- 8. Spirochaetales Associated Human Diseases
- 10. Treponema spp.
- 11. Nonvenereal Treponemal Diseases Bejel, Yaws & Pinta Primitive tropical and subtropical regions Primarily in impoverished children
- 12. Treponema pallidum ssp. endemicum Bejel (a.k.a. endemic syphilis) Initial lesions: nondescript oral lesions Secondary lesions: oral
- 13. Treponema pallidum ssp. pertenue (May also see T. pertenue) Papillomatous Lesions of Yaws: painless nodules widely
- 14. Treponema carateum Pinta: primarily restricted to skin 1-3 week incubation period Initial lesions: small pruritic papules
- 16. Treponema pallidum ssp. pallidum
- 17. Venereal Treponemal Disease Syphilis Primarily sexually transmitted disease (STD) May be transmitted congenitally
- 18. Darkfield Microscopy of Treponema pallidum
- 19. Too thin to be seen with light microscopy in specimens stained with Gram stain or Giemsa
- 20. Epidemiology of T. pallidum Transmitted from direct sexual contact or from mother to fetus Not highly
- 21. Incidence of Syphilis in USA
- 22. Geographical Distribution of Syphilis in USA
- 23. Pathogenesis of T. pallidum Tissue destruction and lesions are primarily a consequence of patient’s immune response
- 24. Virulence Factors of T. pallidum Outer membrane proteins promote adherence Hyaluronidase may facilitate perivascular infiltration Antiphagocytic
- 25. Primary disease process involves invasion of mucus membranes, rapid multiplication & wide dissemination through perivascular lymphatics
- 26. Secondary disease 2-10 weeks after primary lesion Widely disseminated mucocutaneous rash Secondary lesions of the skin
- 27. Generalized Mucocutaneous Rash of Secondary Syphilis
- 28. Following secondary disease, host enters latent period First 4 years = early latent Subsequent period =
- 29. Tertiary syphilis characterized by localized granulomatous dermal lesions (gummas) in which few organisms are present Granulomas
- 30. Diagram of a Granuloma (a.k.a. gumma in skin or soft tissue) NOTE: ultimately a fibrin layer
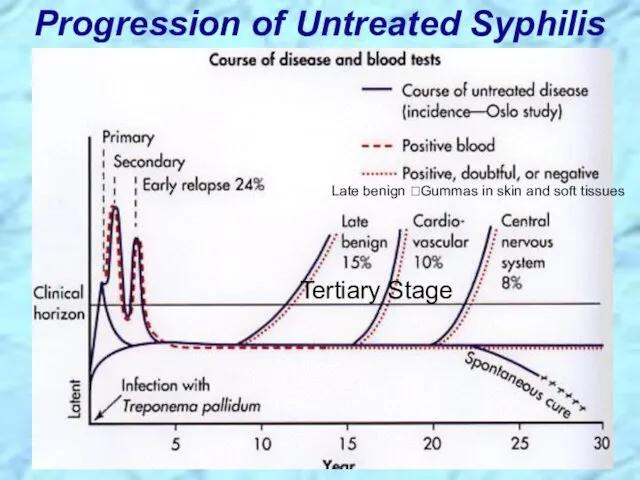
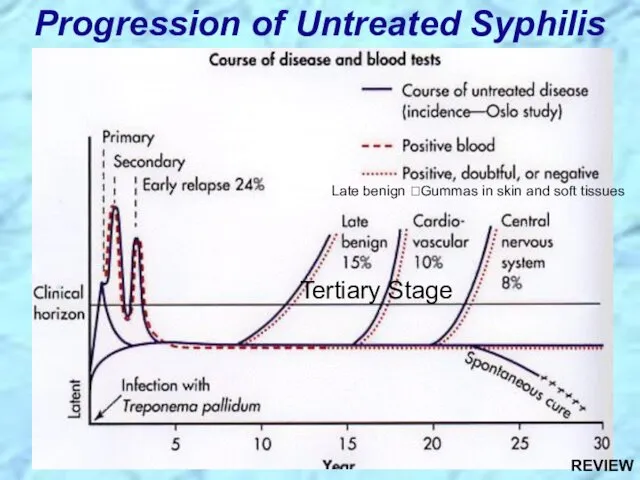
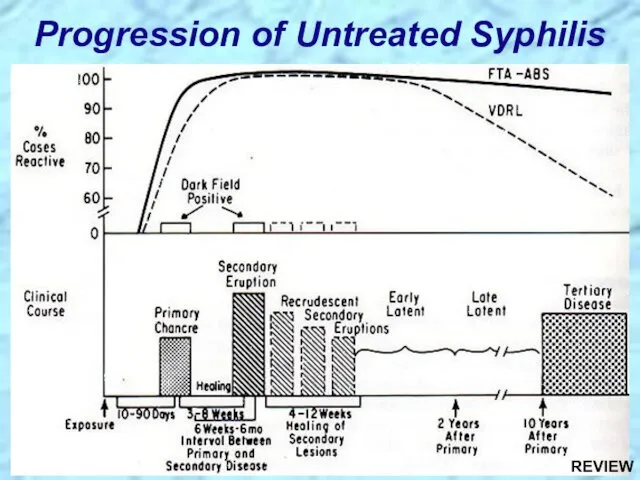
- 31. Progression of Untreated Syphilis Tertiary Stage Late benign ?Gummas in skin and soft tissues
- 32. Congenital syphilis results from transplacental infection T. pallidum septicemia in the developing fetus and widespread dissemination
- 33. Comparison of Incidence of 1o & 2o Syphilis in Women and Congenital Syphilis
- 34. Prevention & Treatment of Syphilis Penicillin remains drug of choice WHO monitors treatment recommendations 7-10 days
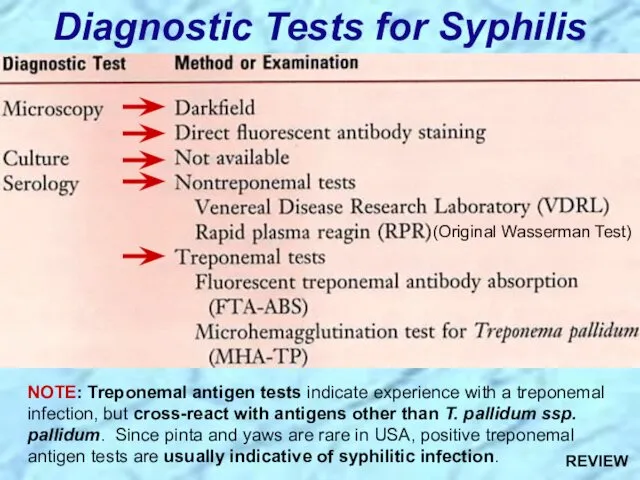
- 35. Diagnostic Tests for Syphilis NOTE: Treponemal antigen tests indicate experience with a treponemal infection, but cross-react
- 36. Sensitivity & Specificity of Serologic Tests for Syphillis
- 37. Review Handout on Sensitivity & Specificity of Diagnostic Tests
- 38. Conditions Associated with False Positive Serological Tests for Syphillis
- 39. Effect of Treatment for Syphillis on Rapid Plasma Reagin Test Reactivity
- 41. Borrelia spp.
- 42. Giemsa Stain of Borrelia recurrentis in Blood Light Microscopy Phase Contrast Microscopy
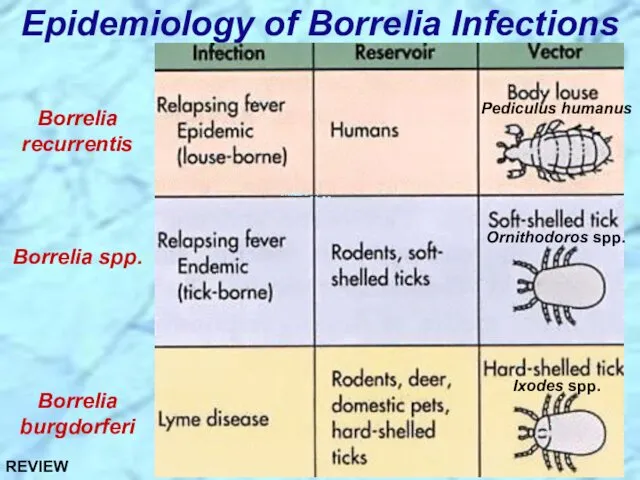
- 43. Epidemiology of Borrelia Infections Borrelia recurrentis Borrelia spp. Borrelia burgdorferi Ixodes spp. Ornithodoros spp. Pediculus humanus
- 44. Borrelia recurrentis & other Borrelia spp.
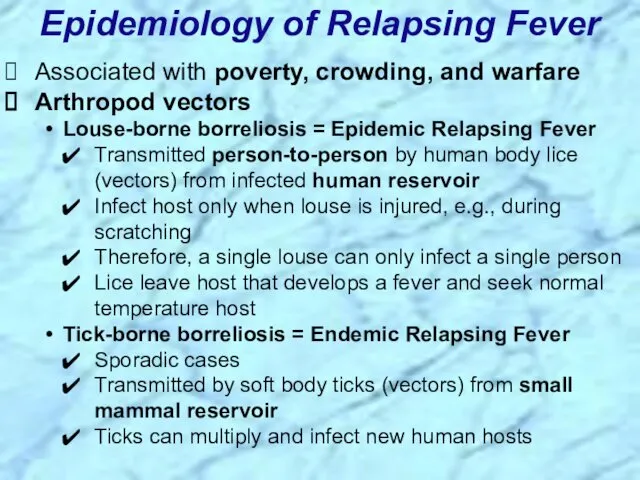
- 45. Associated with poverty, crowding, and warfare Arthropod vectors Louse-borne borreliosis = Epidemic Relapsing Fever Transmitted person-to-person
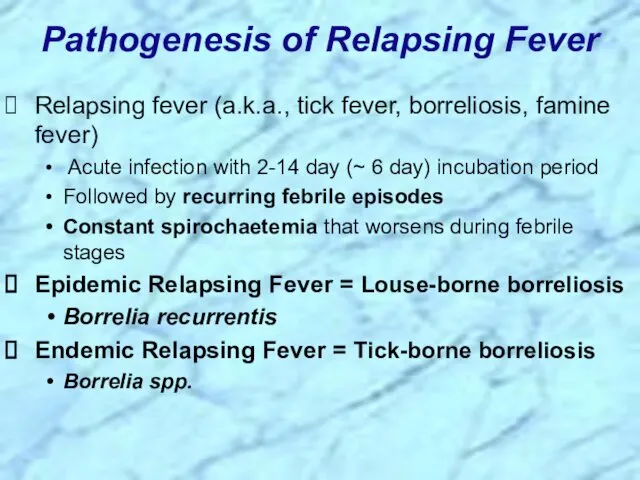
- 46. Pathogenesis of Relapsing Fever Relapsing fever (a.k.a., tick fever, borreliosis, famine fever) Acute infection with 2-14
- 47. Clinical Progression of Relapsing Fever
- 48. Borrelia burgdorferi
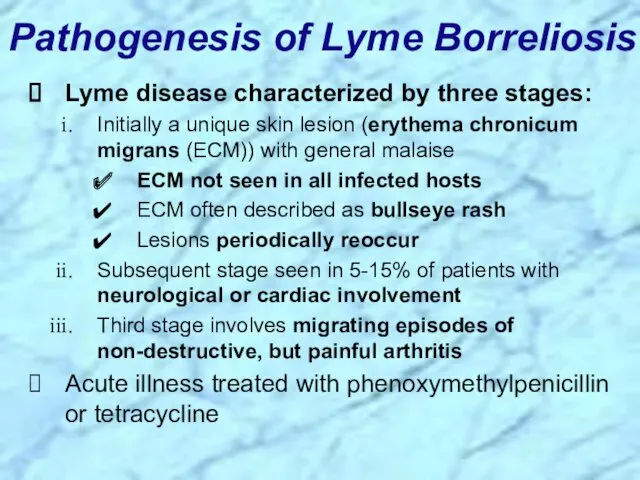
- 49. Pathogenesis of Lyme Borreliosis Lyme disease characterized by three stages: Initially a unique skin lesion (erythema
- 50. Erythema chronicum migrans of Lyme Borreliosis Bullseye rash
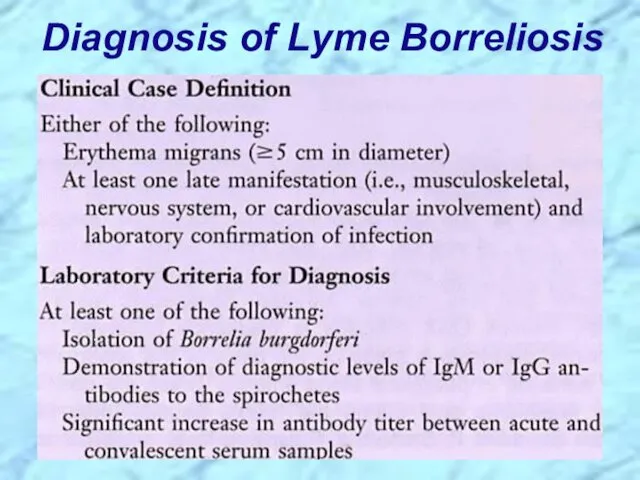
- 51. Diagnosis of Lyme Borreliosis
- 52. Bacteria and Syndromes that Cause Cross-Reactions with Lyme Borreliosis Serological Tests
- 53. Lyme disease was recognized as a syndrome in 1975 with outbreak in Lyme, Connecticut Transmitted by
- 54. Incidence of Lyme Borreliosis in USA
- 56. Leptospira interrogans
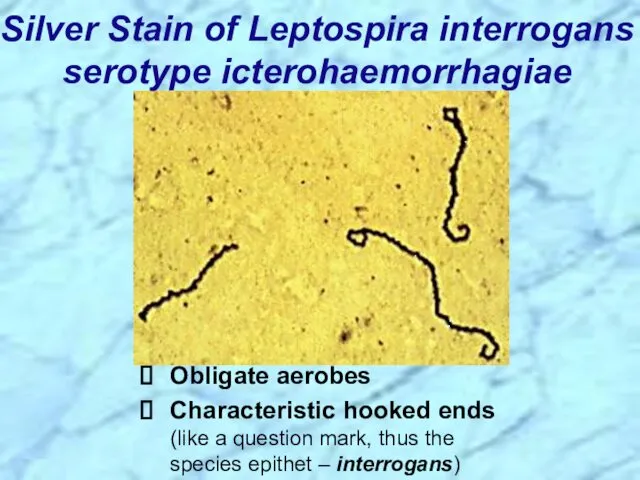
- 57. Silver Stain of Leptospira interrogans serotype icterohaemorrhagiae Obligate aerobes Characteristic hooked ends (like a question mark,
- 58. Leptospirosis Clinical Syndromes Mild virus-like syndrome (Anicteric leptospirosis) Systemic with aseptic meningitis (Icteric leptospirosis) Overwhelming disease
- 59. Leptospirosis, also called Weil’s disease in humans Direct invasion and replication in tissues Characterized by an
- 60. Clinical Progression of Icteric (Weil’s Disease) and Anicteric Leptospirosis (pigmented part of eye)
- 61. Epidemiology of Leptospirosis Mainly a zoonotic disease Transmitted to humans from a variety of wild and
- 62. Comparison of Diagnostic Tests for Leptospirosis
- 64. REVIEW of Spirochaetales
- 65. General Overview of Spirochaetales Gram-negative spirochetes Spirochete from Greek for “coiled hair” Extremely thin and can
- 66. Periplasmic Flagella Diagram REVIEW
- 67. Spirochaetales Associated Human Diseases REVIEW
- 68. Review of Treponema
- 69. Summary of Treponema Infections REVIEW
- 70. Summary of Treponema Infections (cont.) REVIEW
- 71. Nonvenereal Treponemal Diseases Bejel, Yaws & Pinta Primitive tropical and subtropical regions Primarily in impoverished children
- 72. Review of Treponema pallidum ssp. pallidum
- 73. Too thin to be seen with light microscopy in specimens stained with Gram stain or Giemsa
- 74. Epidemiology of T. pallidum Transmitted from direct sexual contact or from mother to fetus Not highly
- 75. Pathogenesis of T. pallidum Tissue destruction and lesions are primarily a consequence of patient’s immune response
- 76. Virulence Factors of T. pallidum Outer membrane proteins promote adherence Hyaluronidase may facilitate perivascular infiltration Antiphagocytic
- 77. Primary disease process involves invasion of mucus membranes, rapid multiplication & wide dissemination through perivascular lymphatics
- 78. Secondary disease 2-10 weeks after primary lesion Widely disseminated mucocutaneous rash Secondary lesions of the skin
- 79. Following secondary disease, host enters latent period First 4 years = early latent Subsequent period =
- 80. Tertiary syphilis characterized by localized granulomatous dermal lesions (gummas) in which few organisms are present Granulomas
- 81. Diagram of a Granuloma (a.k.a. gumma in skin or soft tissue) NOTE: ultimately a fibrin layer
- 82. Progression of Untreated Syphilis Tertiary Stage Late benign ?Gummas in skin and soft tissues REVIEW
- 83. Progression of Untreated Syphilis REVIEW
- 84. Congenital syphilis results from transplacental infection T. pallidum septicemia in the developing fetus and widespread dissemination
- 85. Prevention & Treatment of Syphilis Penicillin remains drug of choice WHO monitors treatment recommendations 7-10 days
- 86. Diagnostic Tests for Syphilis NOTE: Treponemal antigen tests indicate experience with a treponemal infection, but cross-react
- 87. Review Handout on Sensitivity & Specificity of Diagnostic Tests
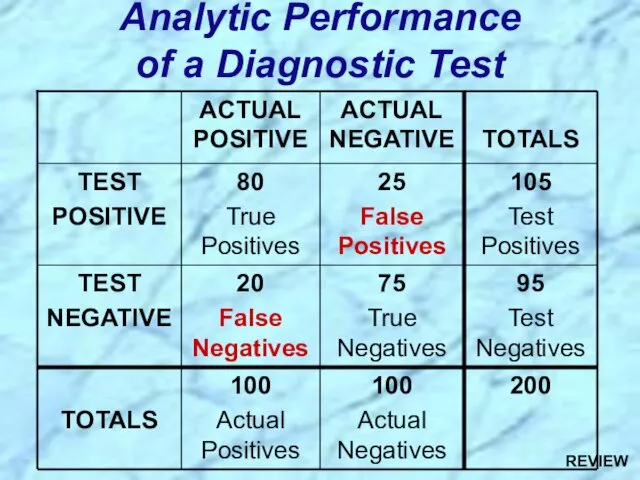
- 88. Analytic Performance of a Diagnostic Test REVIEW
- 89. Sensitivity = Measure of True Positive Rate (TPR) = No. of True Pos. = No. of
- 90. Review of Borrelia
- 91. Summary of Borellia Infections REVIEW
- 92. Summary of Borellia Infections (cont.) REVIEW
- 93. Epidemiology of Borrelia Infections Borrelia recurrentis Borrelia spp. Borrelia burgdorferi Ixodes spp. Ornithodoros spp. Pediculus humanus
- 94. Review of Borrelia recurrentis & other Borrelia spp.
- 95. Associated with poverty, crowding, and warfare Arthropod vectors Louse-borne borreliosis = Epidemic Relapsing Fever Transmitted person-to-person
- 96. Pathogenesis of Relapsing Fever Relapsing fever (a.k.a., tick fever, borreliosis, famine fever) Acute infection with 2-14
- 97. Review of Borrelia burgdorferi
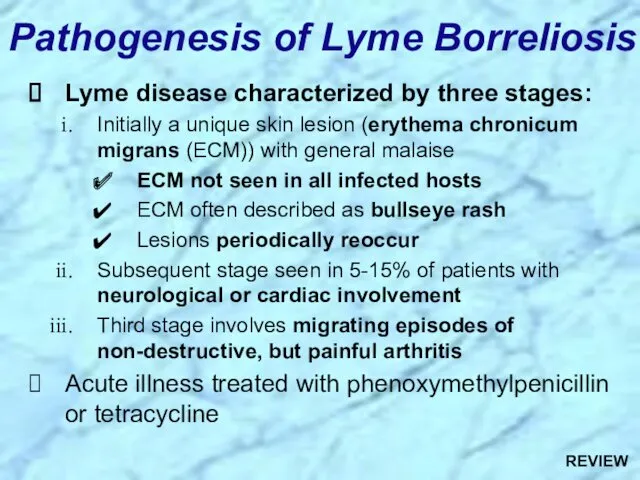
- 98. Pathogenesis of Lyme Borreliosis Lyme disease characterized by three stages: Initially a unique skin lesion (erythema
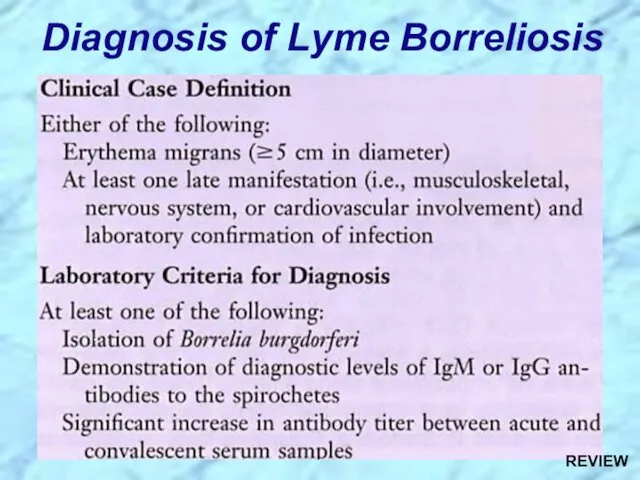
- 99. Diagnosis of Lyme Borreliosis REVIEW
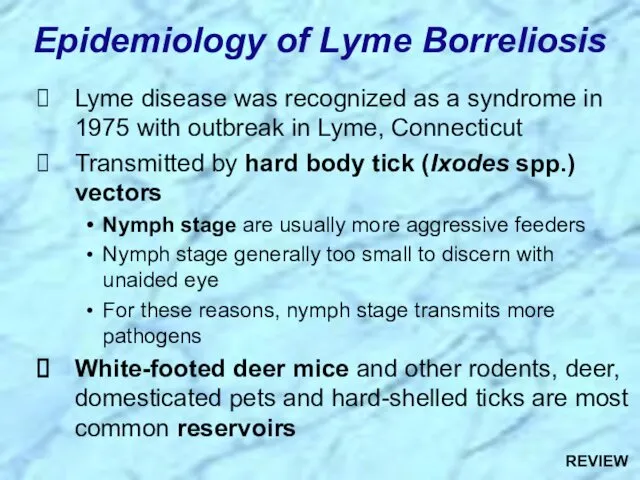
- 100. Lyme disease was recognized as a syndrome in 1975 with outbreak in Lyme, Connecticut Transmitted by
- 101. Review of Leptospira
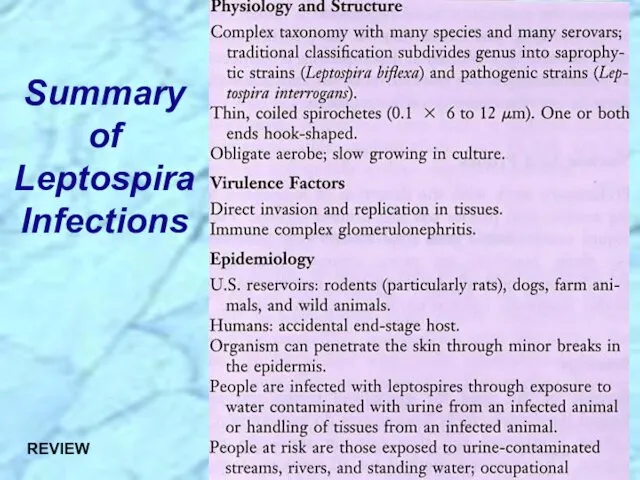
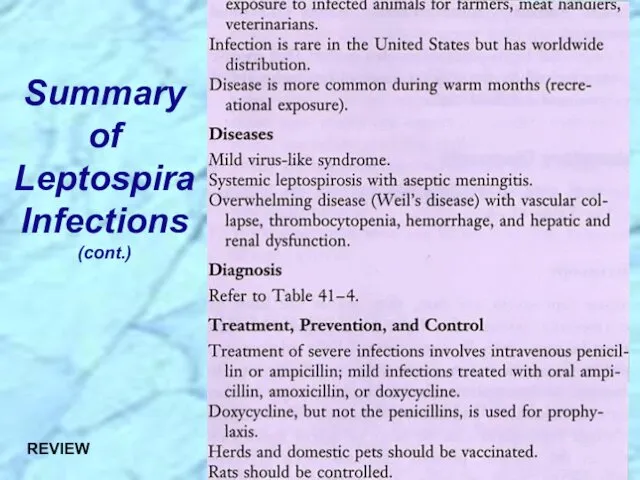
- 102. Summary of Leptospira Infections REVIEW
- 103. Summary of Leptospira Infections (cont.) REVIEW
- 104. Leptospirosis Clinical Syndromes Mild virus-like syndrome (Anicteric leptospirosis) Systemic with aseptic meningitis (Icteric leptospirosis) Overwhelming disease
- 105. Leptospirosis, also called Weil’s disease in humans Direct invasion and replication in tissues Characterized by an
- 106. Epidemiology of Leptospirosis Mainly a zoonotic disease Transmitted to humans from a variety of wild and
- 108. Скачать презентацию

Order: Spirochaetales
Family: Spirochaetaceae
Genus: Treponema
Borrelia
Family: Leptospiraceae
Genus: Leptospira
Taxonomy
Order: Spirochaetales
Family: Spirochaetaceae
Genus: Treponema
Borrelia
Family: Leptospiraceae
Genus: Leptospira
Taxonomy
General Overview of Spirochaetales
Gram-negative spirochetes
Spirochete from Greek for “coiled
General Overview of Spirochaetales
Gram-negative spirochetes
Spirochete from Greek for “coiled

Periplasmic Flagella Diagram
Periplasmic Flagella Diagram
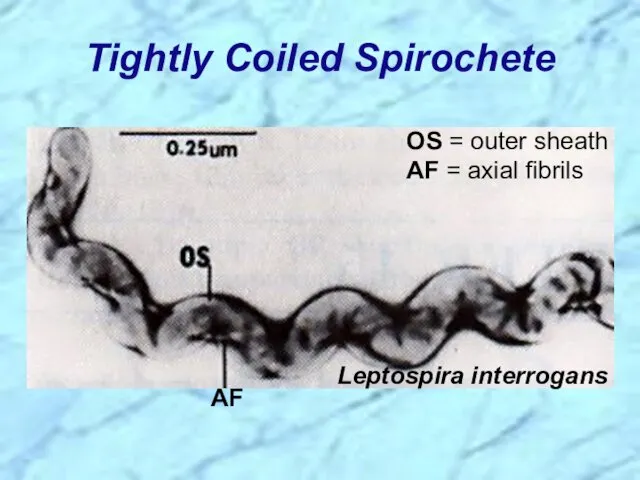
Tightly Coiled Spirochete
Tightly Coiled Spirochete
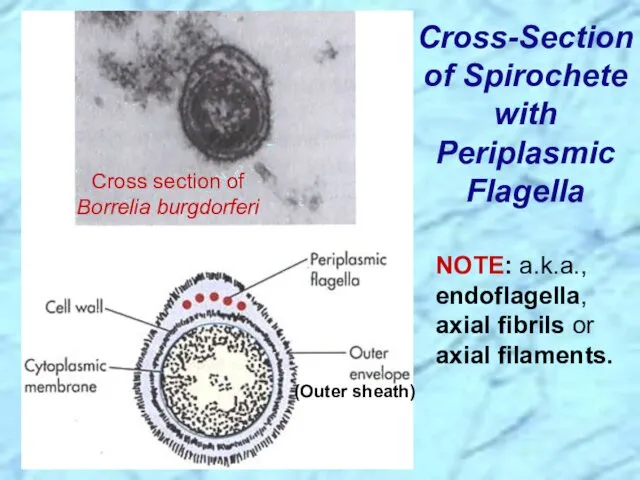
Cross-Section of Spirochete with Periplasmic Flagella
NOTE: a.k.a., endoflagella, axial fibrils or
Cross-Section of Spirochete with Periplasmic Flagella
NOTE: a.k.a., endoflagella, axial fibrils or
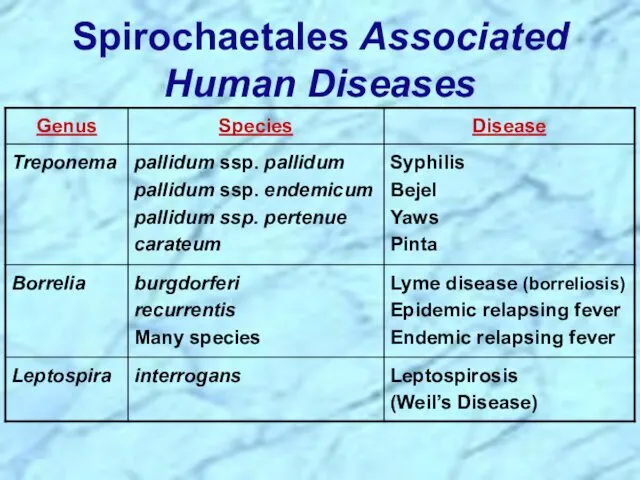
Spirochaetales Associated Human Diseases
Spirochaetales Associated Human Diseases
Treponema spp.
Treponema spp.
Nonvenereal Treponemal Diseases
Bejel, Yaws & Pinta
Primitive tropical and subtropical regions
Primarily in
Nonvenereal Treponemal Diseases
Bejel, Yaws & Pinta
Primitive tropical and subtropical regions
Primarily in
Treponema pallidum ssp. endemicum
Bejel (a.k.a. endemic syphilis)
Initial lesions: nondescript oral
Treponema pallidum ssp. endemicum
Bejel (a.k.a. endemic syphilis)
Initial lesions: nondescript oral
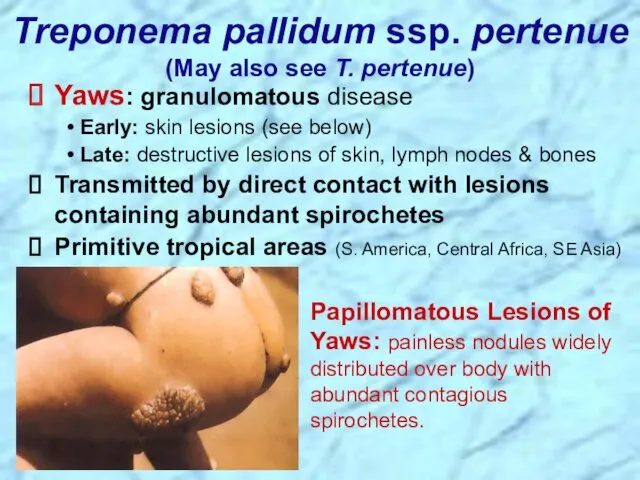
Treponema pallidum ssp. pertenue
(May also see T. pertenue)
Papillomatous Lesions of Yaws:
Treponema pallidum ssp. pertenue
(May also see T. pertenue)
Papillomatous Lesions of Yaws:
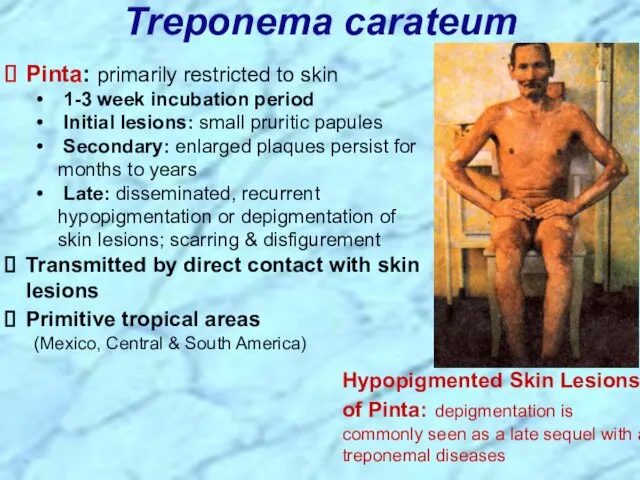
Treponema carateum
Pinta: primarily restricted to skin
1-3 week incubation period
Initial
Treponema carateum
Pinta: primarily restricted to skin
1-3 week incubation period
Initial
Treponema pallidum ssp. pallidum
Treponema pallidum ssp. pallidum
Venereal Treponemal Disease
Syphilis
Primarily sexually transmitted disease (STD)
May be transmitted congenitally
Venereal Treponemal Disease
Syphilis
Primarily sexually transmitted disease (STD)
May be transmitted congenitally
Darkfield Microscopy of Treponema pallidum
Darkfield Microscopy of Treponema pallidum
Too thin to be seen with light microscopy in specimens stained
Too thin to be seen with light microscopy in specimens stained
Epidemiology of T. pallidum
Transmitted from direct sexual contact or from mother
Epidemiology of T. pallidum
Transmitted from direct sexual contact or from mother
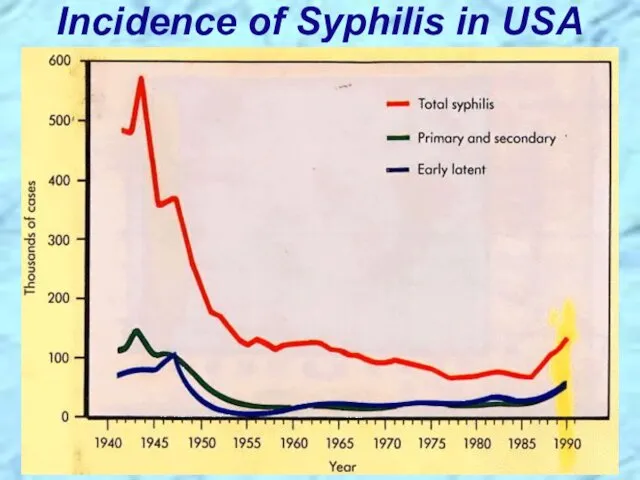
Incidence of Syphilis in USA
Incidence of Syphilis in USA
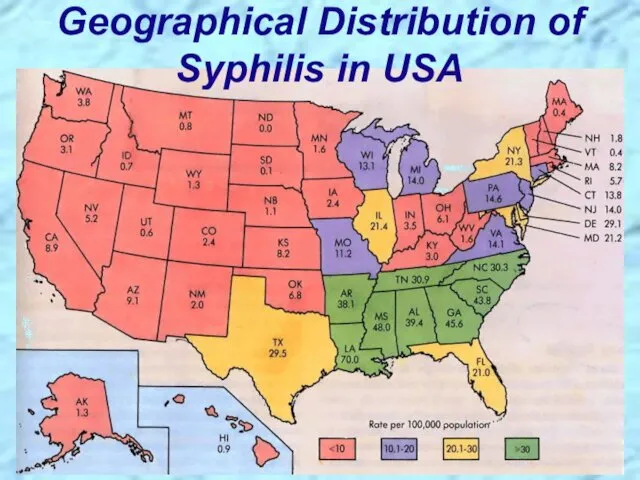
Geographical Distribution of Syphilis in USA
Geographical Distribution of Syphilis in USA
Pathogenesis of T. pallidum
Tissue destruction and lesions are primarily a consequence
Pathogenesis of T. pallidum
Tissue destruction and lesions are primarily a consequence
Virulence Factors of T. pallidum
Outer membrane proteins promote adherence
Hyaluronidase may facilitate
Virulence Factors of T. pallidum
Outer membrane proteins promote adherence
Hyaluronidase may facilitate
Primary disease process involves invasion of mucus membranes, rapid multiplication &
Primary disease process involves invasion of mucus membranes, rapid multiplication &
Secondary disease 2-10 weeks after primary lesion
Widely disseminated mucocutaneous rash
Secondary lesions
Secondary disease 2-10 weeks after primary lesion
Widely disseminated mucocutaneous rash
Secondary lesions
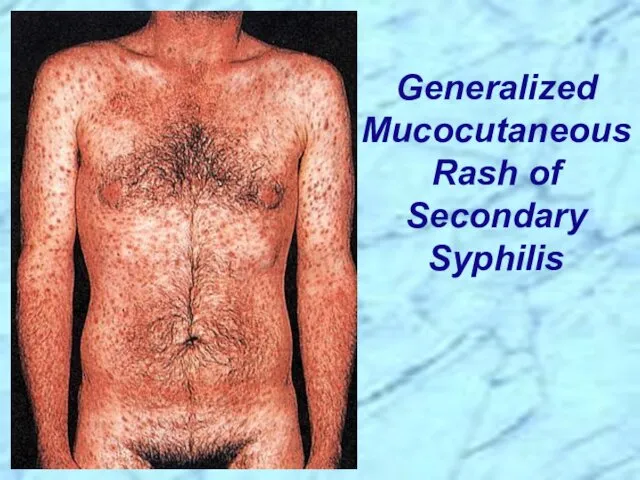
Generalized Mucocutaneous Rash of Secondary Syphilis
Generalized Mucocutaneous Rash of Secondary Syphilis
Following secondary disease, host enters latent period
First 4 years = early
Following secondary disease, host enters latent period
First 4 years = early
Tertiary syphilis characterized by localized granulomatous dermal lesions (gummas) in which
Tertiary syphilis characterized by localized granulomatous dermal lesions (gummas) in which
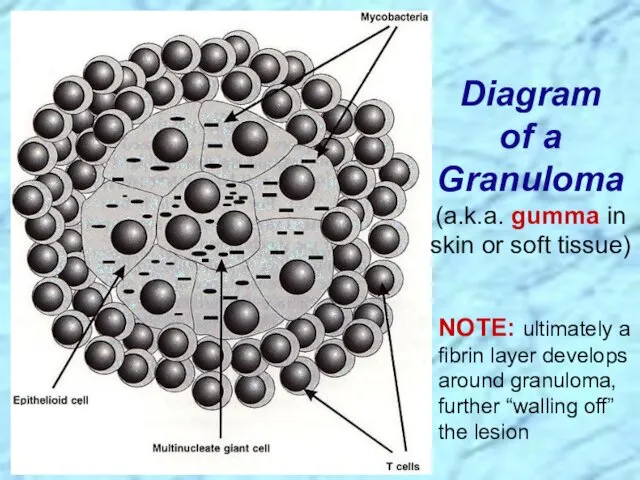
Diagram of a Granuloma
(a.k.a. gumma in skin or soft tissue)
NOTE: ultimately
Diagram of a Granuloma
(a.k.a. gumma in skin or soft tissue)
NOTE: ultimately
Progression of Untreated Syphilis
Tertiary Stage
Late benign ?Gummas in skin and soft
Progression of Untreated Syphilis
Tertiary Stage
Late benign ?Gummas in skin and soft
Congenital syphilis results from transplacental infection
T. pallidum septicemia in the developing
Congenital syphilis results from transplacental infection
T. pallidum septicemia in the developing
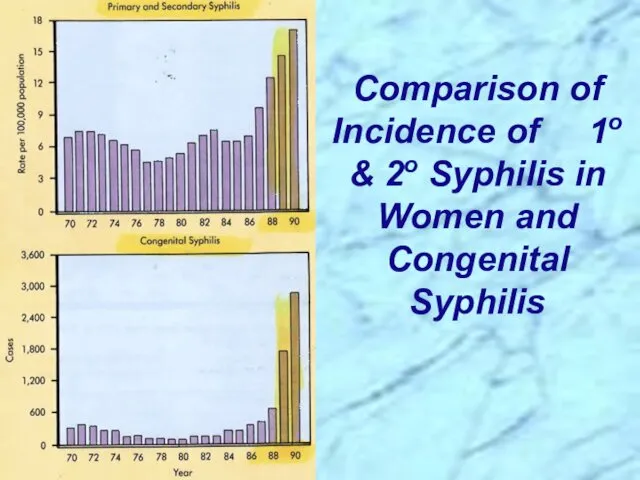
Comparison of Incidence of 1o & 2o Syphilis in Women and
Comparison of Incidence of 1o & 2o Syphilis in Women and
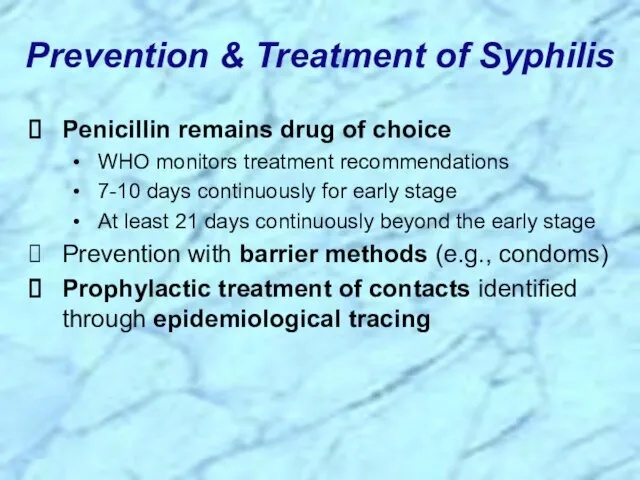
Prevention & Treatment of Syphilis
Penicillin remains drug of choice
WHO monitors treatment
Prevention & Treatment of Syphilis
Penicillin remains drug of choice
WHO monitors treatment
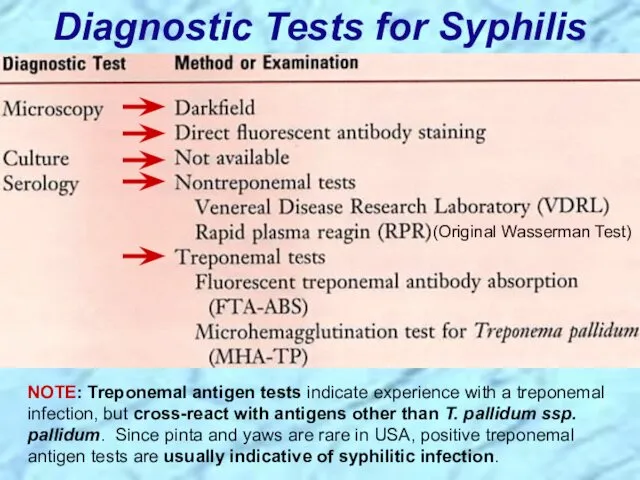
Diagnostic Tests for Syphilis
NOTE: Treponemal antigen tests indicate experience with a
Diagnostic Tests for Syphilis
NOTE: Treponemal antigen tests indicate experience with a
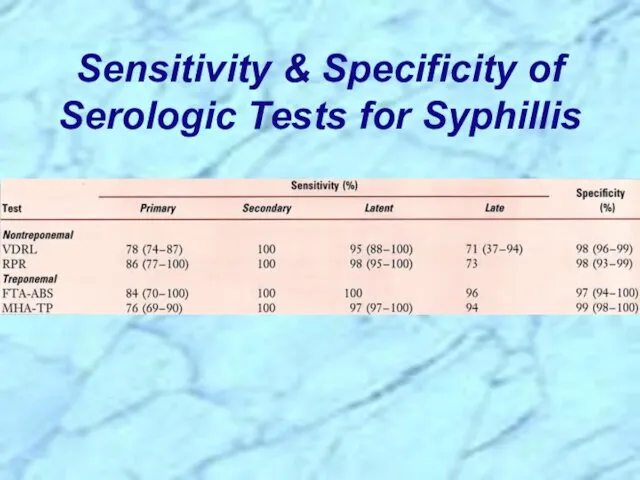
Sensitivity & Specificity of Serologic Tests for Syphillis
Sensitivity & Specificity of Serologic Tests for Syphillis
Review Handout on Sensitivity & Specificity of Diagnostic Tests
Review Handout on Sensitivity & Specificity of Diagnostic Tests
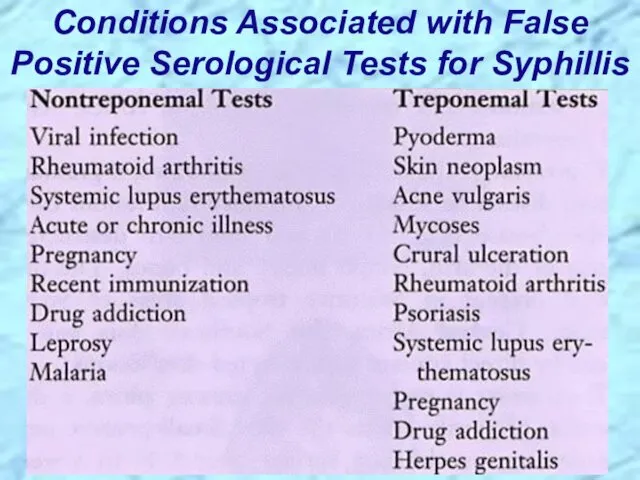
Conditions Associated with False Positive Serological Tests for Syphillis
Conditions Associated with False Positive Serological Tests for Syphillis
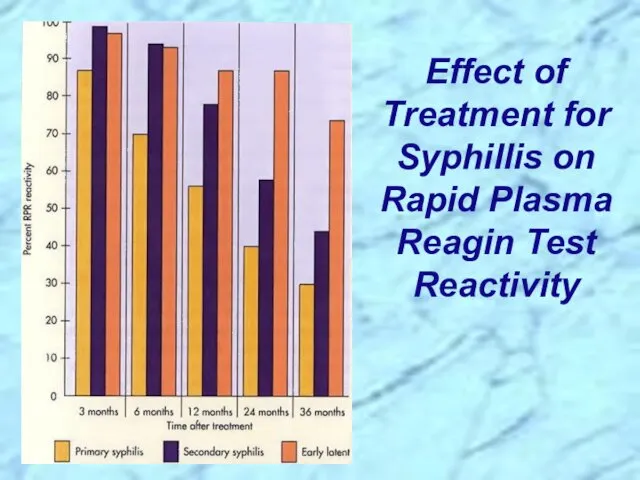
Effect of Treatment for Syphillis on Rapid Plasma Reagin Test Reactivity
Effect of Treatment for Syphillis on Rapid Plasma Reagin Test Reactivity
Borrelia spp.
Borrelia spp.
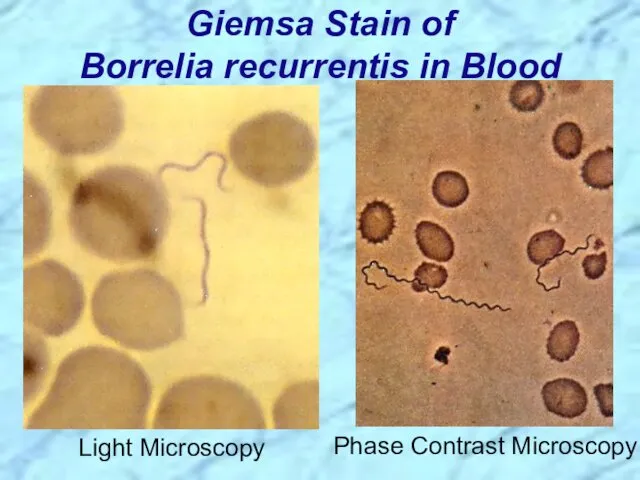
Giemsa Stain of Borrelia recurrentis in Blood
Light Microscopy
Phase Contrast Microscopy
Giemsa Stain of Borrelia recurrentis in Blood
Light Microscopy
Phase Contrast Microscopy
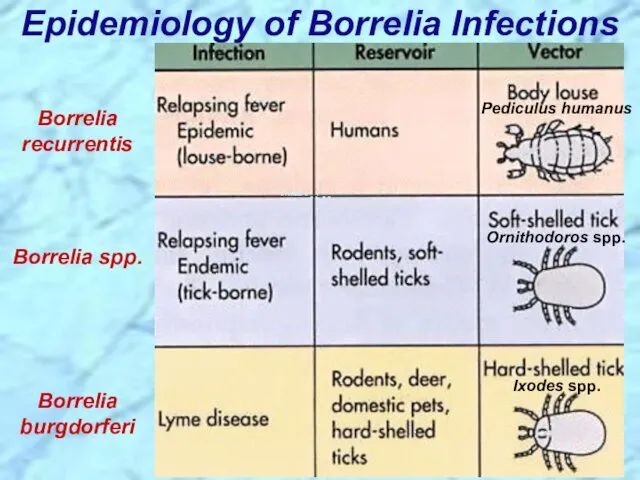
Epidemiology of Borrelia Infections
Borrelia recurrentis
Borrelia spp.
Borrelia burgdorferi
Ixodes spp.
Ornithodoros spp.
Pediculus humanus
Epidemiology of Borrelia Infections
Borrelia recurrentis
Borrelia spp.
Borrelia burgdorferi
Ixodes spp.
Ornithodoros spp.
Pediculus humanus
Borrelia recurrentis & other Borrelia spp.
Borrelia recurrentis & other Borrelia spp.
Associated with poverty, crowding, and warfare
Arthropod vectors
Louse-borne borreliosis = Epidemic Relapsing
Associated with poverty, crowding, and warfare
Arthropod vectors
Louse-borne borreliosis = Epidemic Relapsing
Pathogenesis of Relapsing Fever
Relapsing fever (a.k.a., tick fever, borreliosis, famine fever)
Pathogenesis of Relapsing Fever
Relapsing fever (a.k.a., tick fever, borreliosis, famine fever)
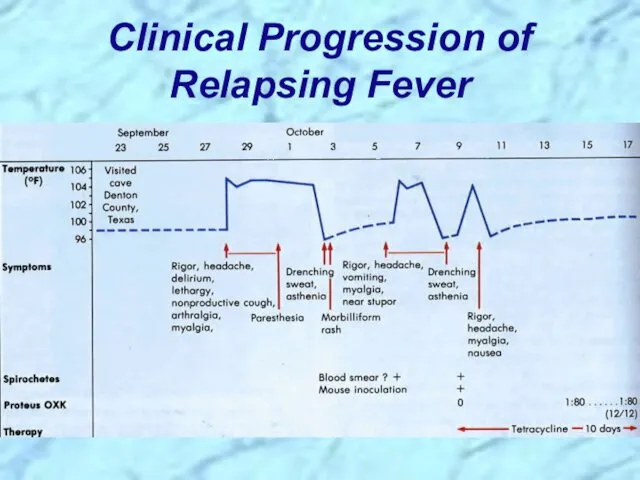
Clinical Progression of Relapsing Fever
Clinical Progression of Relapsing Fever
Borrelia burgdorferi
Borrelia burgdorferi
Pathogenesis of Lyme Borreliosis
Lyme disease characterized by three stages:
Initially a unique
Pathogenesis of Lyme Borreliosis
Lyme disease characterized by three stages:
Initially a unique
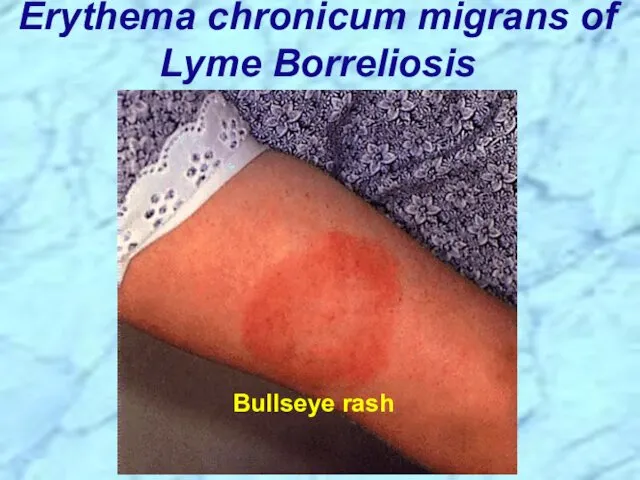
Erythema chronicum migrans of Lyme Borreliosis
Bullseye rash
Erythema chronicum migrans of Lyme Borreliosis
Bullseye rash
Diagnosis of Lyme Borreliosis
Diagnosis of Lyme Borreliosis
Bacteria and Syndromes that Cause Cross-Reactions with Lyme Borreliosis Serological Tests
Bacteria and Syndromes that Cause Cross-Reactions with Lyme Borreliosis Serological Tests
Lyme disease was recognized as a syndrome in 1975 with outbreak
Lyme disease was recognized as a syndrome in 1975 with outbreak
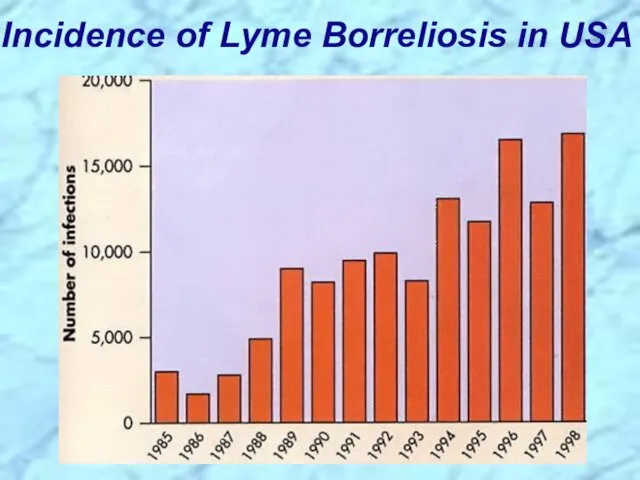
Incidence of Lyme Borreliosis in USA
Incidence of Lyme Borreliosis in USA
Leptospira interrogans
Leptospira interrogans
Silver Stain of Leptospira interrogans serotype icterohaemorrhagiae
Obligate aerobes
Characteristic hooked ends (like
Silver Stain of Leptospira interrogans serotype icterohaemorrhagiae
Obligate aerobes
Characteristic hooked ends (like
Leptospirosis Clinical Syndromes
Mild virus-like syndrome
(Anicteric leptospirosis) Systemic with aseptic meningitis
(Icteric leptospirosis)
Leptospirosis Clinical Syndromes
Mild virus-like syndrome
(Anicteric leptospirosis) Systemic with aseptic meningitis
(Icteric leptospirosis)
Leptospirosis, also called Weil’s disease in humans
Direct invasion and replication in
Leptospirosis, also called Weil’s disease in humans
Direct invasion and replication in
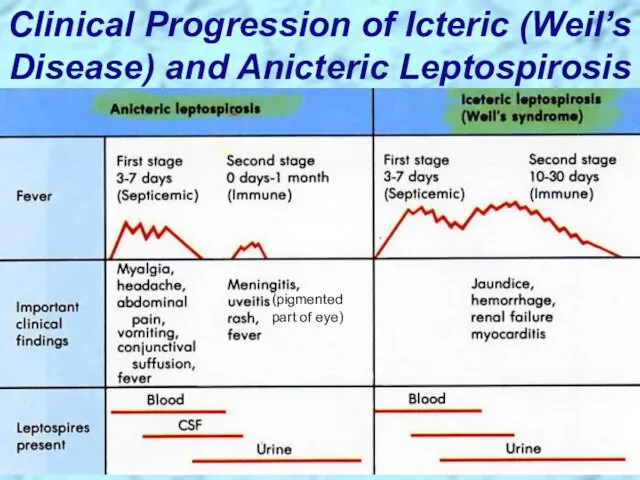
Clinical Progression of Icteric (Weil’s Disease) and Anicteric Leptospirosis
(pigmented part of
Clinical Progression of Icteric (Weil’s Disease) and Anicteric Leptospirosis
(pigmented part of
Epidemiology of Leptospirosis
Mainly a zoonotic disease
Transmitted to humans from a
Epidemiology of Leptospirosis
Mainly a zoonotic disease
Transmitted to humans from a
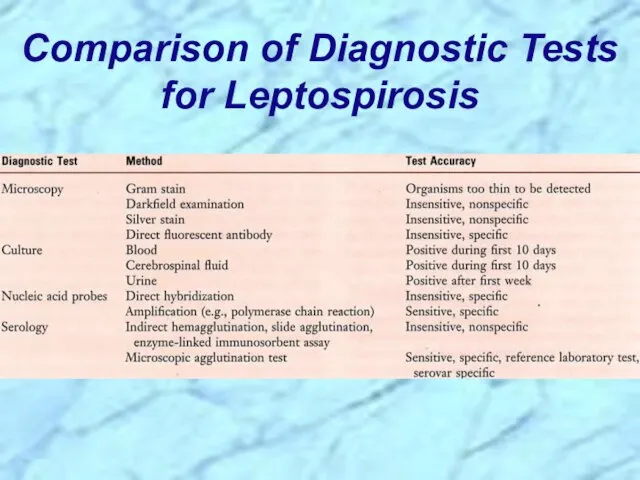
Comparison of Diagnostic Tests for Leptospirosis
Comparison of Diagnostic Tests for Leptospirosis
REVIEW
of
Spirochaetales
REVIEW
of
Spirochaetales
General Overview of Spirochaetales
Gram-negative spirochetes
Spirochete from Greek for “coiled
General Overview of Spirochaetales
Gram-negative spirochetes
Spirochete from Greek for “coiled
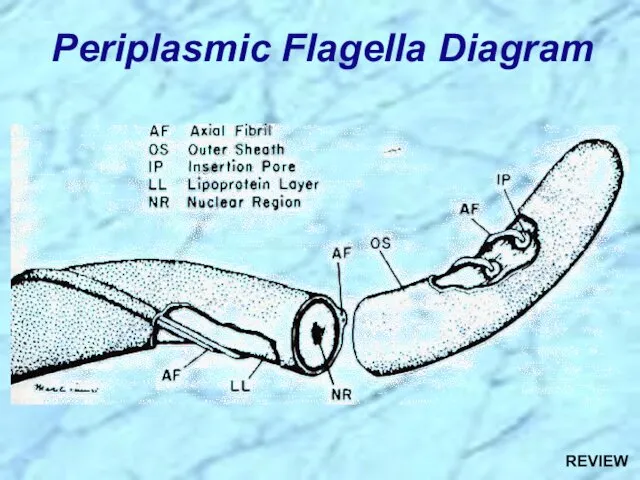
Periplasmic Flagella Diagram
REVIEW
Periplasmic Flagella Diagram
REVIEW
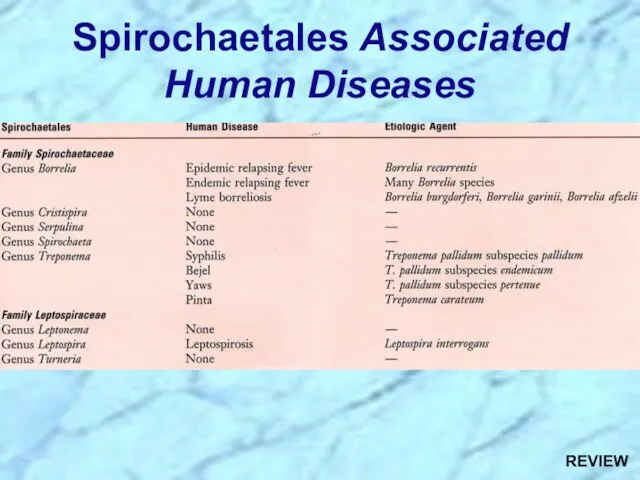
Spirochaetales Associated Human Diseases
REVIEW
Spirochaetales Associated Human Diseases
REVIEW
Review of Treponema
Review of Treponema
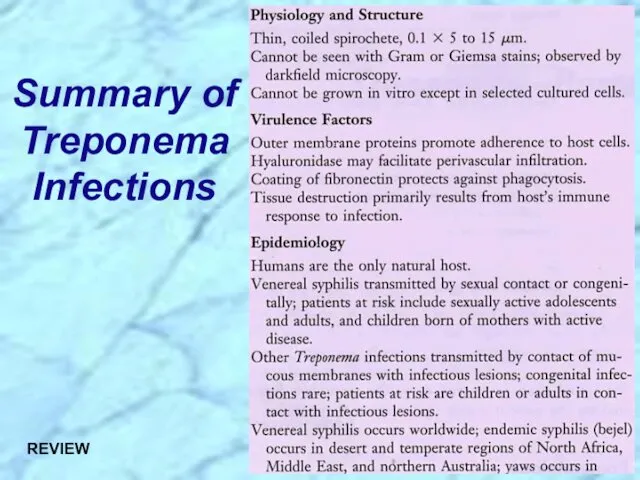
Summary of Treponema Infections
REVIEW
Summary of Treponema Infections
REVIEW
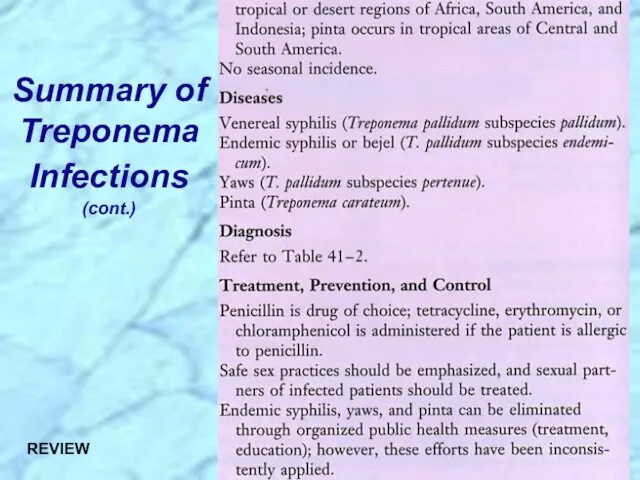
Summary of Treponema Infections (cont.)
REVIEW
Summary of Treponema Infections (cont.)
REVIEW
Nonvenereal Treponemal Diseases
Bejel, Yaws & Pinta
Primitive tropical and subtropical regions
Primarily in
Nonvenereal Treponemal Diseases
Bejel, Yaws & Pinta
Primitive tropical and subtropical regions
Primarily in
Review of Treponema pallidum ssp. pallidum
Review of Treponema pallidum ssp. pallidum
Too thin to be seen with light microscopy in specimens stained
Too thin to be seen with light microscopy in specimens stained
Epidemiology of T. pallidum
Transmitted from direct sexual contact or from mother
Epidemiology of T. pallidum
Transmitted from direct sexual contact or from mother
Pathogenesis of T. pallidum
Tissue destruction and lesions are primarily a consequence
Pathogenesis of T. pallidum
Tissue destruction and lesions are primarily a consequence

Virulence Factors of T. pallidum
Outer membrane proteins promote adherence
Hyaluronidase may facilitate
Virulence Factors of T. pallidum
Outer membrane proteins promote adherence
Hyaluronidase may facilitate
Primary disease process involves invasion of mucus membranes, rapid multiplication &
Primary disease process involves invasion of mucus membranes, rapid multiplication &
Secondary disease 2-10 weeks after primary lesion
Widely disseminated mucocutaneous rash
Secondary lesions
Secondary disease 2-10 weeks after primary lesion
Widely disseminated mucocutaneous rash
Secondary lesions
Following secondary disease, host enters latent period
First 4 years = early
Following secondary disease, host enters latent period
First 4 years = early
Tertiary syphilis characterized by localized granulomatous dermal lesions (gummas) in which
Tertiary syphilis characterized by localized granulomatous dermal lesions (gummas) in which
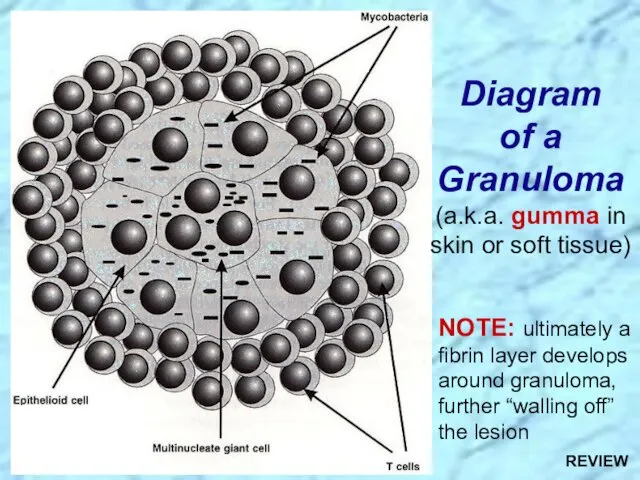
Diagram of a Granuloma
(a.k.a. gumma in skin or soft tissue)
NOTE: ultimately
Diagram of a Granuloma
(a.k.a. gumma in skin or soft tissue)
NOTE: ultimately
Progression of Untreated Syphilis
Tertiary Stage
Late benign ?Gummas in skin and soft
Progression of Untreated Syphilis
Tertiary Stage
Late benign ?Gummas in skin and soft
Progression of Untreated Syphilis
REVIEW
Progression of Untreated Syphilis
REVIEW
Congenital syphilis results from transplacental infection
T. pallidum septicemia in the developing
Congenital syphilis results from transplacental infection
T. pallidum septicemia in the developing
Prevention & Treatment of Syphilis
Penicillin remains drug of choice
WHO monitors treatment
Prevention & Treatment of Syphilis
Penicillin remains drug of choice
WHO monitors treatment
Diagnostic Tests for Syphilis
NOTE: Treponemal antigen tests indicate experience with a
Diagnostic Tests for Syphilis
NOTE: Treponemal antigen tests indicate experience with a
Review Handout on Sensitivity & Specificity of Diagnostic Tests
Review Handout on Sensitivity & Specificity of Diagnostic Tests
Analytic Performance of a Diagnostic Test
REVIEW
Analytic Performance of a Diagnostic Test
REVIEW
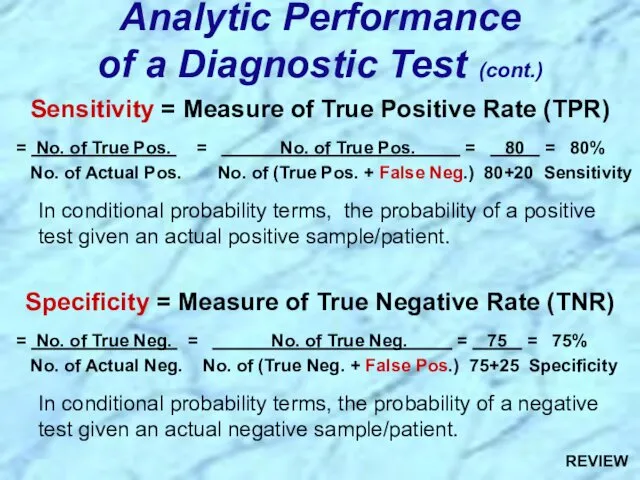
Sensitivity = Measure of True Positive Rate (TPR)
= No. of
Sensitivity = Measure of True Positive Rate (TPR)
= No. of
Review of Borrelia
Review of Borrelia
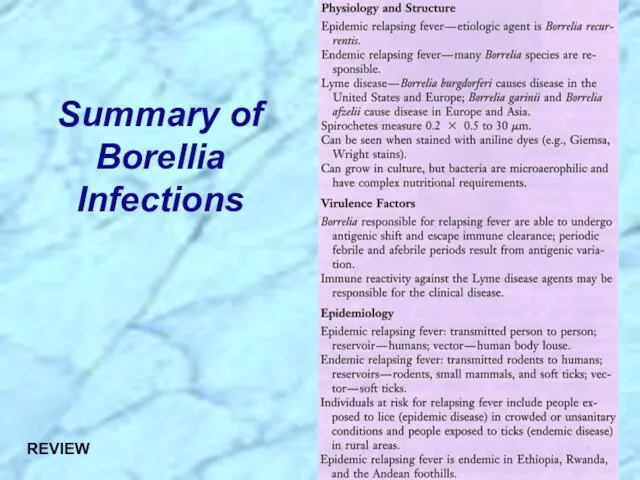
Summary of Borellia Infections
REVIEW
Summary of Borellia Infections
REVIEW
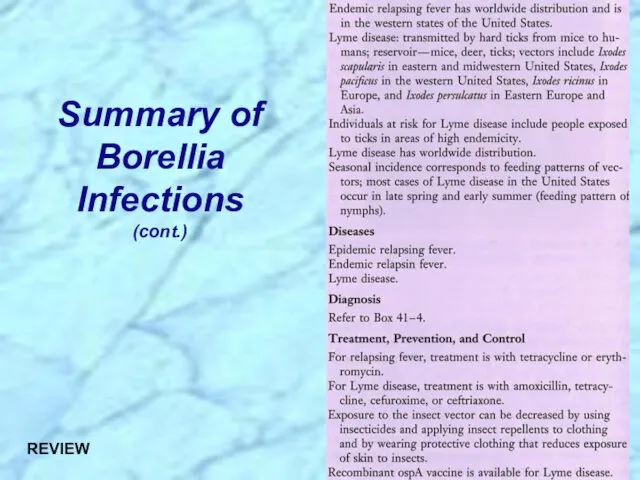
Summary of Borellia Infections (cont.)
REVIEW
Summary of Borellia Infections (cont.)
REVIEW
Epidemiology of Borrelia Infections
Borrelia recurrentis
Borrelia spp.
Borrelia burgdorferi
Ixodes spp.
Ornithodoros spp.
Pediculus humanus
REVIEW
Epidemiology of Borrelia Infections
Borrelia recurrentis
Borrelia spp.
Borrelia burgdorferi
Ixodes spp.
Ornithodoros spp.
Pediculus humanus
REVIEW
Review of Borrelia recurrentis & other Borrelia spp.
Review of Borrelia recurrentis & other Borrelia spp.
Associated with poverty, crowding, and warfare
Arthropod vectors
Louse-borne borreliosis = Epidemic Relapsing
Associated with poverty, crowding, and warfare
Arthropod vectors
Louse-borne borreliosis = Epidemic Relapsing
Pathogenesis of Relapsing Fever
Relapsing fever (a.k.a., tick fever, borreliosis, famine fever)
Pathogenesis of Relapsing Fever
Relapsing fever (a.k.a., tick fever, borreliosis, famine fever)
Review of Borrelia burgdorferi
Review of Borrelia burgdorferi
Pathogenesis of Lyme Borreliosis
Lyme disease characterized by three stages:
Initially a unique
Pathogenesis of Lyme Borreliosis
Lyme disease characterized by three stages:
Initially a unique
Diagnosis of Lyme Borreliosis
REVIEW
Diagnosis of Lyme Borreliosis
REVIEW
Lyme disease was recognized as a syndrome in 1975 with outbreak
Lyme disease was recognized as a syndrome in 1975 with outbreak
Review of Leptospira
Review of Leptospira
Summary of Leptospira Infections
REVIEW
Summary of Leptospira Infections
REVIEW
Summary of Leptospira Infections (cont.)
REVIEW
Summary of Leptospira Infections (cont.)
REVIEW
Leptospirosis Clinical Syndromes
Mild virus-like syndrome
(Anicteric leptospirosis) Systemic with aseptic meningitis
(Icteric leptospirosis)
Leptospirosis Clinical Syndromes
Mild virus-like syndrome
(Anicteric leptospirosis) Systemic with aseptic meningitis
(Icteric leptospirosis)
Leptospirosis, also called Weil’s disease in humans
Direct invasion and replication in
Leptospirosis, also called Weil’s disease in humans
Direct invasion and replication in
Epidemiology of Leptospirosis
Mainly a zoonotic disease
Transmitted to humans from a
Epidemiology of Leptospirosis
Mainly a zoonotic disease
Transmitted to humans from a
 General characteristics of 6 Kingdoms
General characteristics of 6 Kingdoms Биологически активные низкомолекулярные вещества
Биологически активные низкомолекулярные вещества Әр түрлі мөлшердегі минералды тыңайтқыштардың қант қызылшасының өнімділігіне әсерін анықтау барысындағы суреттер
Әр түрлі мөлшердегі минералды тыңайтқыштардың қант қызылшасының өнімділігіне әсерін анықтау барысындағы суреттер Растительная клетка. Лекция 1
Растительная клетка. Лекция 1 Актинидия. Особенности
Актинидия. Особенности Многообразие ракообразных
Многообразие ракообразных Кетоновые тела. Тема 10
Кетоновые тела. Тема 10 Лист. Морфология
Лист. Морфология Строение растительной клетки
Строение растительной клетки Генеративні органи рослини
Генеративні органи рослини Функциональная асимметрия мозга. Лекция 11
Функциональная асимметрия мозга. Лекция 11 Методы микроскопии
Методы микроскопии Самое редкое животное Африки - Окапи
Самое редкое животное Африки - Окапи Презентация, конспект урока, карточки - задания к уроку биологии для 6 класса на тему Фотосинтез.
Презентация, конспект урока, карточки - задания к уроку биологии для 6 класса на тему Фотосинтез. ПрезентацияТурнир по биологии в 8 классе.
ПрезентацияТурнир по биологии в 8 классе. Тема 12.Навоз, воздух, вода
Тема 12.Навоз, воздух, вода Лист — боковой орган побега
Лист — боковой орган побега Фотосинтез. История открытия
Фотосинтез. История открытия Миология. Мышцы тела человека
Миология. Мышцы тела человека Рослини ендеміки Австралії
Рослини ендеміки Австралії Деление клетки – митоз, мейоз
Деление клетки – митоз, мейоз Животные Республики Башкортостан
Животные Республики Башкортостан Физиология растений. Лекция 2
Физиология растений. Лекция 2 Красная книга Сызранского района
Красная книга Сызранского района В Буграх растут деревья и кустарники
В Буграх растут деревья и кустарники Сон и его значение
Сон и его значение Половое поведение животных
Половое поведение животных Ароматерапия. Химия эфирных масел
Ароматерапия. Химия эфирных масел