- Congenital and acquired respiratory disorders in infants

Содержание
- 2. OBJECTIVES Review of Cardio-Pulmonary Development. Define changes that occur during transition to extra-uterine life with emphasis
- 3. STAGES OF NORMAL LUNG GROWTH Embryonic - first 5 weeks; formation of proximal airways Pseudoglandular -
- 4. Pseudoglandular 6-16 weeks
- 5. Canalicular Phase 16-24 weeks
- 6. Saccular Phase 24-34 weeks
- 7. PHYSIOLOGIC MATURATION (Surfactant Production) Type 2 pneumocytes appear at 24-26 weeks Responsible for reduction of alveolar
- 10. Maturational Factors Stimulation Glucorticoids, ACTH Thyroid Hormones, TRF EGF Heroin Aminophyline,cAMP Interferon Estrogens Inhibition Diabetes (insulin,
- 11. FETAL CIRCULATION
- 12. TRANSITION TO EXTRA-UTERINE LIFE Fetal Breathing Instantaneous; liquid filled to air filled lungs Maintenance of FRC
- 13. MECHANICS OF BREATHING Respiratory Control Center...CNS Metabolic Needs Negative pressure breathing Compliance and Resistance Inspiratory Muscles
- 14. Signs of Respiratory Distress Tachypnea Intercostal retractions Nasal Flaring Grunting Cyanosis
- 15. When is it abnormal to show signs of respiratory distress? When tachypnea, retractions, flaring, or grunting
- 16. Causes of Neonatal Respiratory Distress Obstructive/restrictive - mucous, choanal atresia, pneumothorax, diaphragmatic hernia. Primary lung problem
- 17. Infants at Risk for Developing Respiratory Distress Preterm Infants Infants with birth asphyxia Infants of Diabetic
- 18. Evaluation of Respiratory Distress Administer Oxygen and other necessary emergency treatment Vital sign assessment Determine cause--
- 19. Principles of Therapy Improve oxygen delivery to lungs-- supplemental oxygen, CPAP, assisted ventilation, surfactant Improve blood
- 20. DISEASE STATES Respiratory Distress Syndrome Transient Tachypnea of the Newborn Meconium Aspiration Syndrome Persistent Hypertension of
- 21. RESPIRATORY DISTRESS SYNDROME Surfactant Deficiency Tidal Volume Ventilation Pulmonary Injury Sequence
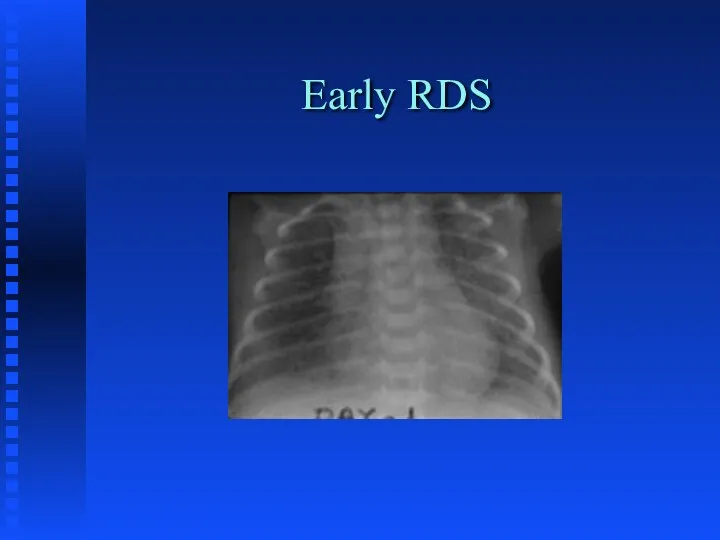
- 22. CLINICAL FEATURES OF RDS Tachypnea/Apnea Dyspnea Grunting/Flaring Hypoxemia Radiographic Features Pulmonary Function Abnormalities
- 23. Early RDS
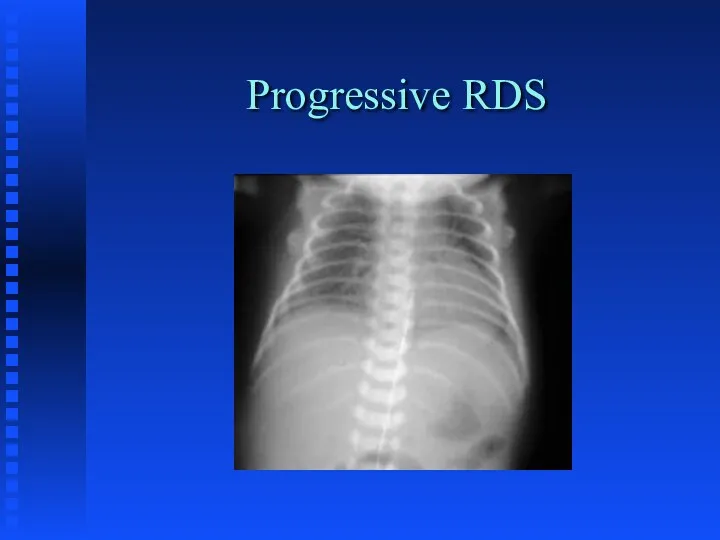
- 24. Progressive RDS
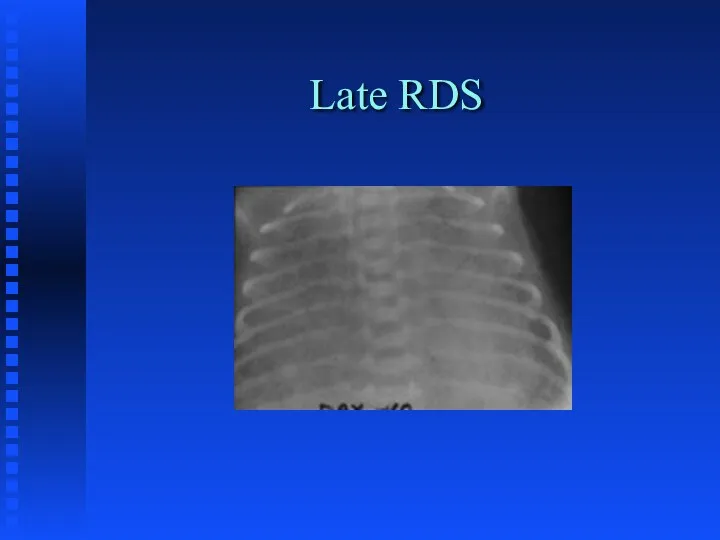
- 25. Late RDS
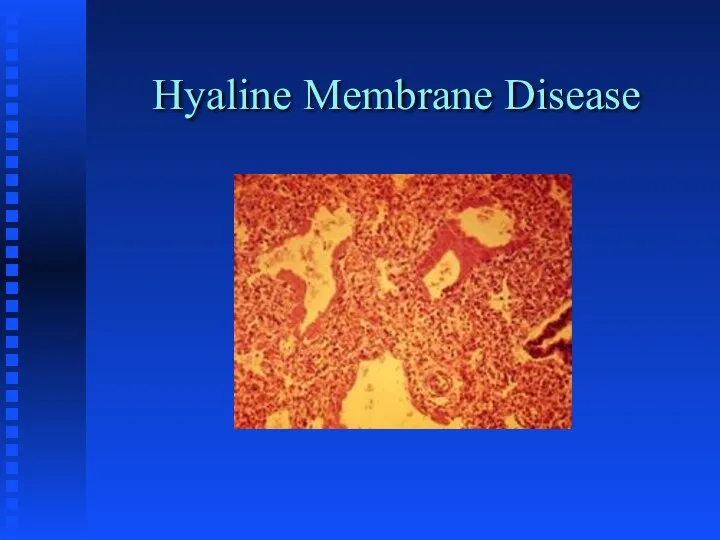
- 26. Hyaline Membrane Disease
- 27. THERAPY FOR RDS Oxygen - maintain PaO2 > 50 torr Nasal CPAP Intermittent Mandatory Ventilation Surfactant
- 28. PIE
- 29. PIE Pathology
- 30. PIE Histology
- 31. Pneumothorax/PIE
- 32. Pneumothorax
- 33. Pneumopericardium
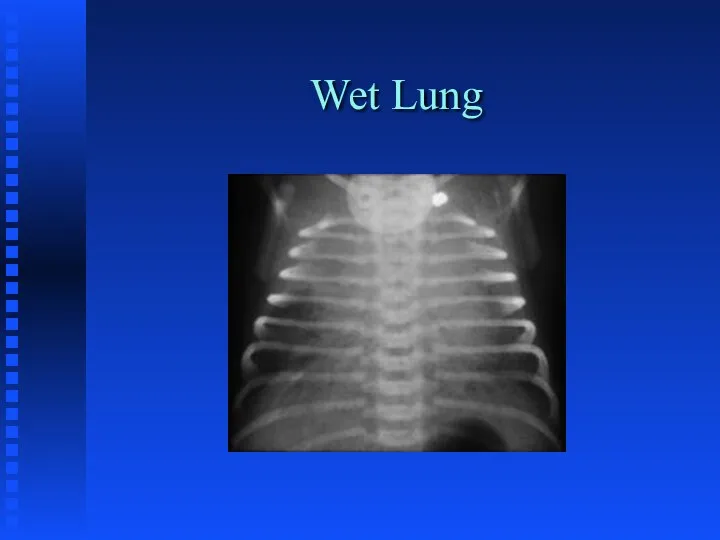
- 34. TRANSIENT TACHYPNEA OF THE NEWBORN Delayed Fluid Resorption Hard to differentiate early on from RDS both
- 35. Wet Lung
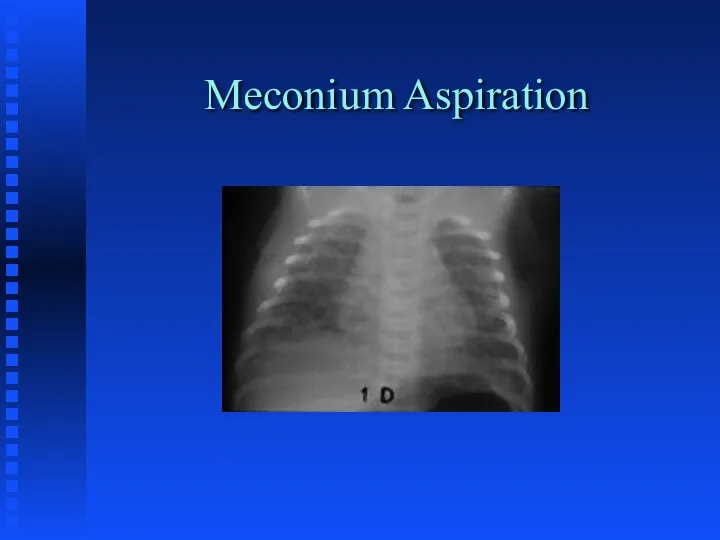
- 36. MECONIUM ASPIRATION SYNDROME Chemical Pneumonitis Surfactant Inactivation Potential for Infection Potential for Pulmonary Hypertension Management varies
- 37. Meconium Aspiration
- 38. PERSISTENT PULMONARY HYPERTENSION Usually secondary to primary pulmonary disease state Pulmonary Vascular Lability Treat the underlying
- 39. PPHN
- 40. CONGENITAL PNEUMONIA Infectious; primarily GBS Amniotic Fluid aspiration Viral etiology Surfactant inactivation
- 41. GBS Pneumonia
- 42. CONGENITAL MALFORMATIONS Choanal Atresia Tracheal Atresia/stenosis Chest Mass Diaphragmatic hernia CCAM Sequestration Lobar emphysema
- 43. CCAM
- 44. Lobar Emphysema
- 45. Diaphragmatic Hernia
- 46. Chylothorax
- 47. Phrenic Nerve Paralysis
- 48. ACQUIRED DISEASES Infections Bronchopulmonary Dysplasia Sub-glottic stenosis Apnea of Prematurity
- 49. Early BPD
- 50. Progressive BPD
- 51. Late BPD
- 52. APNEA Definition: cessation of breathing for longer than a 15 second period or for a shorter
- 53. Babies at Risk for Apnea Preterm Respiratory Distress Metabolic Disorders Infections Cold-stressed babies who are being
- 54. Anticipation and Detection Place at-risk infants on cardio-respiratory monitor Low heart rate limit (80-100) Respiratory alarm
- 55. Treatment Determine cause: x-ray blood sugar body and environmental temperature hematocrit sepsis work up electrolytes cardiac
- 56. Treatment CPAP Theophylline/Caffeine therapy Mechanical ventilation Apnea monitor
- 58. Скачать презентацию
OBJECTIVES
Review of Cardio-Pulmonary Development.
Define changes that occur during transition to
OBJECTIVES
Review of Cardio-Pulmonary Development.
Define changes that occur during transition to
STAGES
OF
NORMAL LUNG GROWTH
Embryonic - first 5 weeks; formation of
STAGES
OF
NORMAL LUNG GROWTH
Embryonic - first 5 weeks; formation of
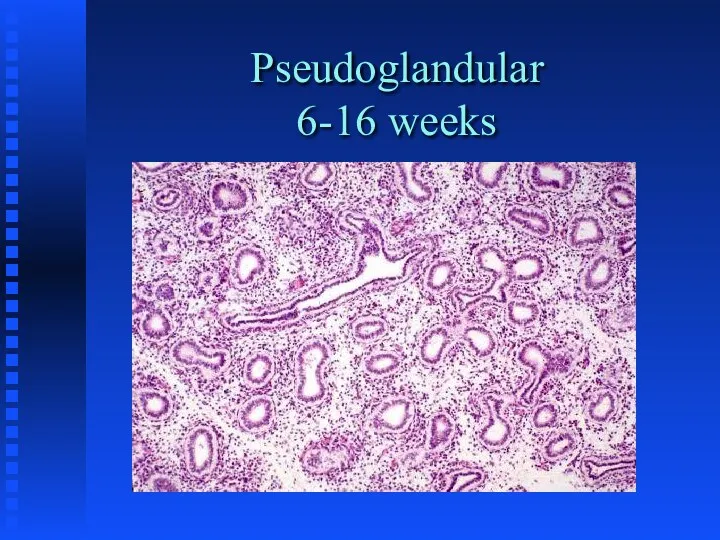
Pseudoglandular
6-16 weeks
Pseudoglandular
6-16 weeks
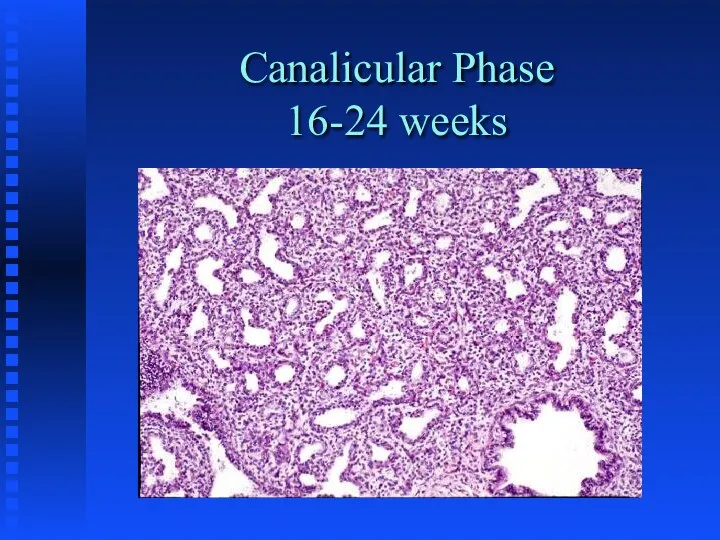
Canalicular Phase
16-24 weeks
Canalicular Phase
16-24 weeks
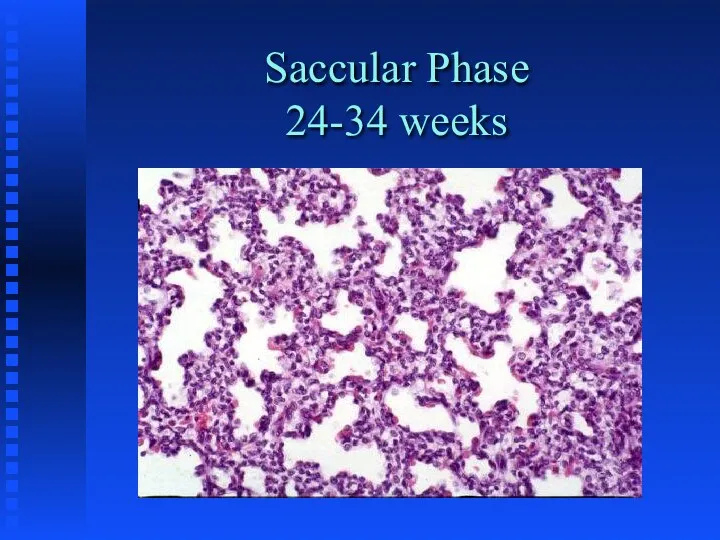
Saccular Phase
24-34 weeks
Saccular Phase
24-34 weeks
PHYSIOLOGIC MATURATION
(Surfactant Production)
Type 2 pneumocytes appear at 24-26 weeks
Responsible for reduction
PHYSIOLOGIC MATURATION
(Surfactant Production)
Type 2 pneumocytes appear at 24-26 weeks
Responsible for reduction
Maturational Factors
Stimulation
Glucorticoids, ACTH
Thyroid Hormones, TRF
EGF
Heroin
Aminophyline,cAMP
Interferon
Estrogens
Inhibition
Diabetes (insulin, hyperglycemia, butyric acid)
Testosterone
TGF-B
Barbiturates
Prolactin
Maturational Factors
Stimulation
Glucorticoids, ACTH
Thyroid Hormones, TRF
EGF
Heroin
Aminophyline,cAMP
Interferon
Estrogens
Inhibition
Diabetes (insulin, hyperglycemia, butyric acid)
Testosterone
TGF-B
Barbiturates
Prolactin
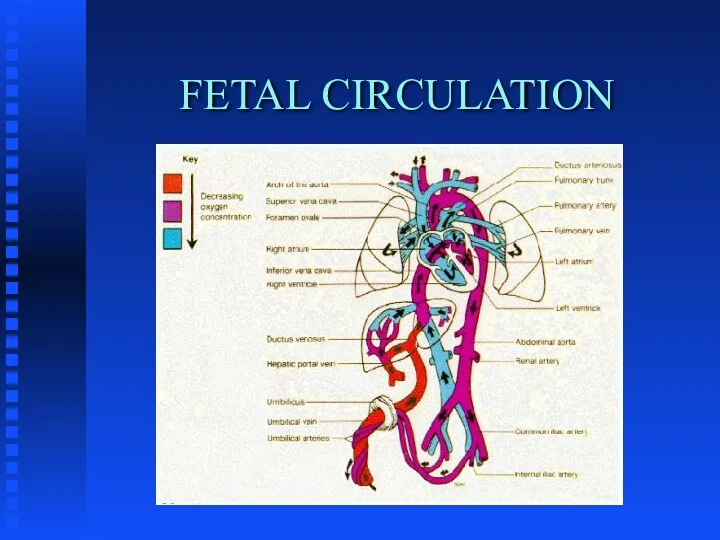
FETAL CIRCULATION
FETAL CIRCULATION
TRANSITION
TO
EXTRA-UTERINE LIFE
Fetal Breathing
Instantaneous; liquid filled to air filled lungs
Maintenance of FRC
Placental
TRANSITION
TO
EXTRA-UTERINE LIFE
Fetal Breathing
Instantaneous; liquid filled to air filled lungs
Maintenance of FRC
Placental
MECHANICS OF BREATHING
Respiratory Control Center...CNS
Metabolic Needs
Negative pressure breathing
Compliance and Resistance
Inspiratory Muscles
Rib
MECHANICS OF BREATHING
Respiratory Control Center...CNS
Metabolic Needs
Negative pressure breathing
Compliance and Resistance
Inspiratory Muscles
Rib
Signs of Respiratory Distress
Tachypnea
Intercostal retractions
Nasal Flaring
Grunting
Cyanosis
Signs of Respiratory Distress
Tachypnea
Intercostal retractions
Nasal Flaring
Grunting
Cyanosis
When is it abnormal to show signs of respiratory distress?
When tachypnea,
When is it abnormal to show signs of respiratory distress?
When tachypnea,
Causes of Neonatal Respiratory Distress
Obstructive/restrictive - mucous, choanal atresia, pneumothorax, diaphragmatic
Causes of Neonatal Respiratory Distress
Obstructive/restrictive - mucous, choanal atresia, pneumothorax, diaphragmatic

Infants at Risk for Developing Respiratory Distress
Preterm Infants
Infants with birth asphyxia
Infants
Infants at Risk for Developing Respiratory Distress
Preterm Infants
Infants with birth asphyxia
Infants
Evaluation of Respiratory Distress
Administer Oxygen and other necessary emergency treatment
Vital sign
Evaluation of Respiratory Distress
Administer Oxygen and other necessary emergency treatment
Vital sign
Principles of Therapy
Improve oxygen delivery to lungs-- supplemental oxygen, CPAP, assisted
Principles of Therapy
Improve oxygen delivery to lungs-- supplemental oxygen, CPAP, assisted
DISEASE STATES
Respiratory Distress Syndrome
Transient Tachypnea of the Newborn
Meconium Aspiration Syndrome
Persistent Hypertension
DISEASE STATES
Respiratory Distress Syndrome
Transient Tachypnea of the Newborn
Meconium Aspiration Syndrome
Persistent Hypertension
RESPIRATORY DISTRESS SYNDROME
Surfactant Deficiency
Tidal Volume Ventilation
Pulmonary Injury Sequence
RESPIRATORY DISTRESS SYNDROME
Surfactant Deficiency
Tidal Volume Ventilation
Pulmonary Injury Sequence
CLINICAL FEATURES OF RDS
Tachypnea/Apnea
Dyspnea
Grunting/Flaring
Hypoxemia
Radiographic Features
Pulmonary Function Abnormalities
CLINICAL FEATURES OF RDS
Tachypnea/Apnea
Dyspnea
Grunting/Flaring
Hypoxemia
Radiographic Features
Pulmonary Function Abnormalities
Early RDS
Early RDS
Progressive RDS
Progressive RDS
Late RDS
Late RDS
Hyaline Membrane Disease
Hyaline Membrane Disease
THERAPY FOR RDS
Oxygen - maintain PaO2 > 50 torr
Nasal CPAP
Intermittent Mandatory
THERAPY FOR RDS
Oxygen - maintain PaO2 > 50 torr
Nasal CPAP
Intermittent Mandatory
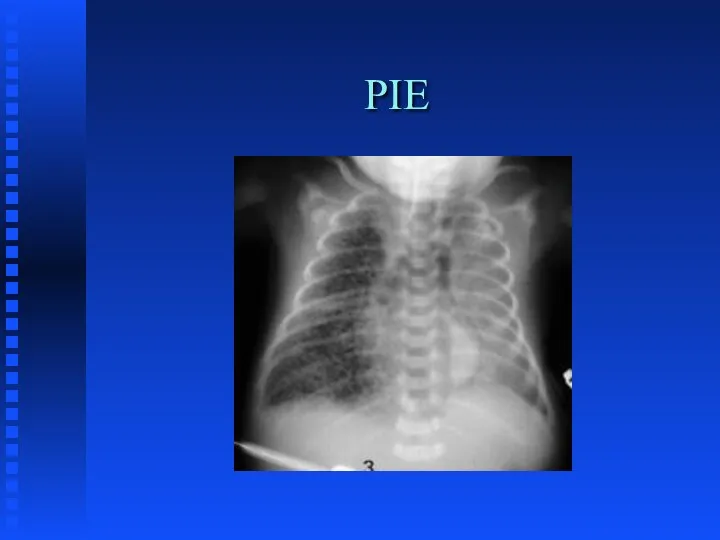
PIE
PIE
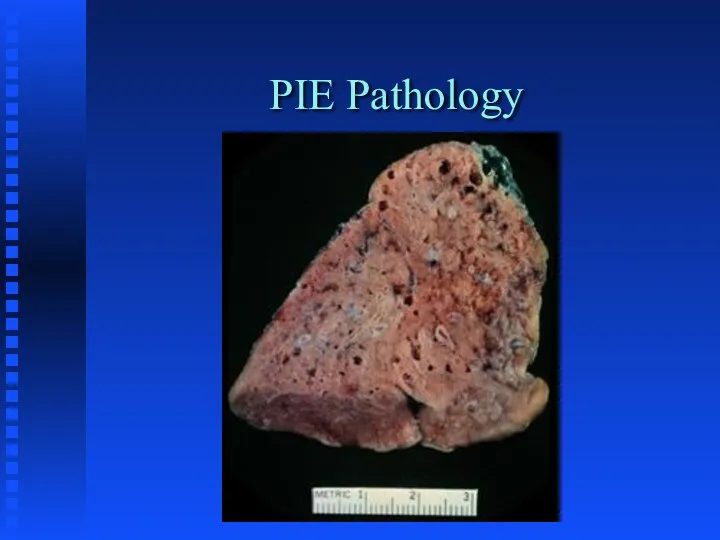
PIE Pathology
PIE Pathology
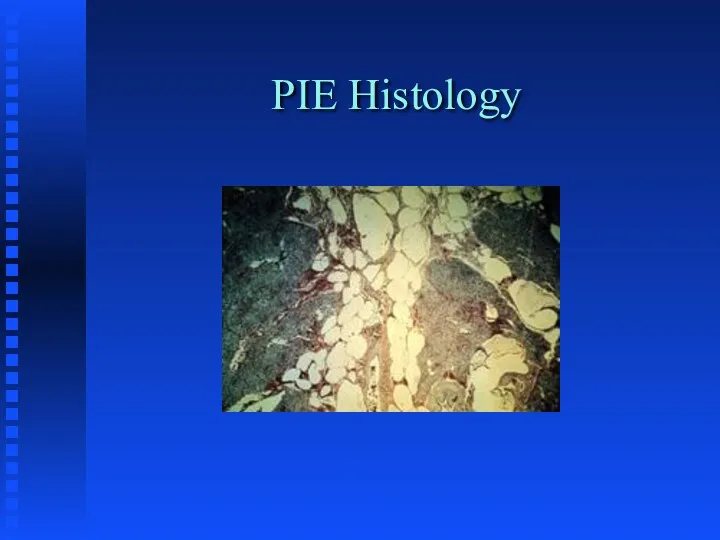
PIE Histology
PIE Histology
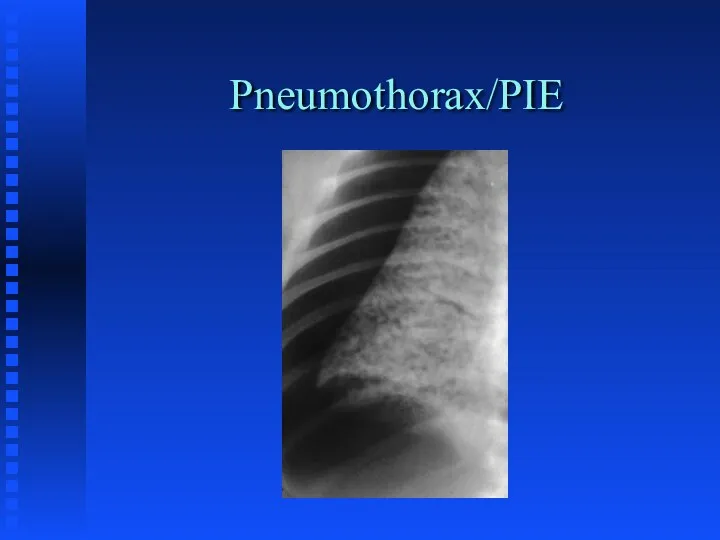
Pneumothorax/PIE
Pneumothorax/PIE
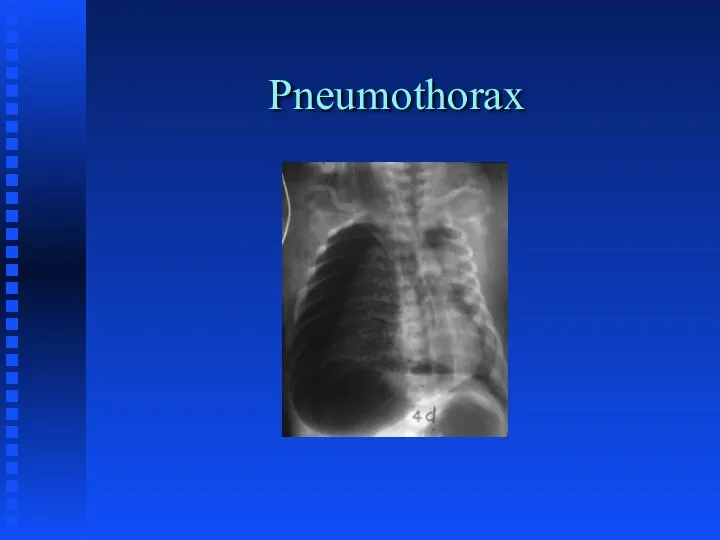
Pneumothorax
Pneumothorax
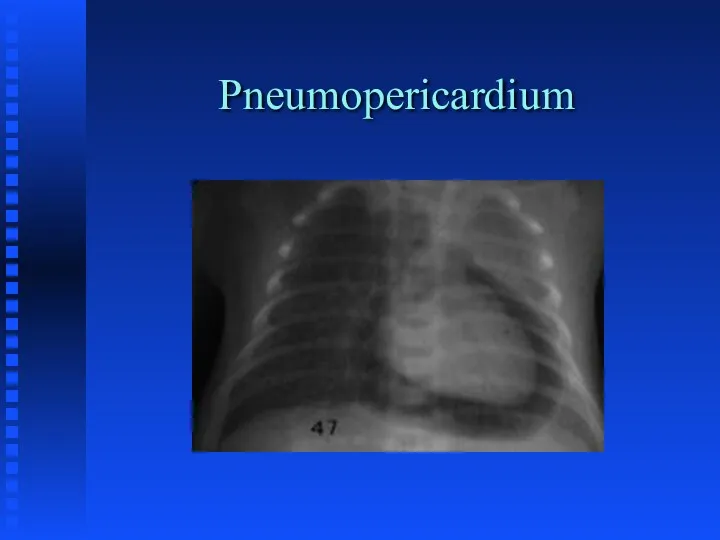
Pneumopericardium
Pneumopericardium
TRANSIENT TACHYPNEA OF THE NEWBORN
Delayed Fluid Resorption
Hard to differentiate early on
TRANSIENT TACHYPNEA OF THE NEWBORN
Delayed Fluid Resorption
Hard to differentiate early on
Wet Lung
Wet Lung
MECONIUM ASPIRATION SYNDROME
Chemical Pneumonitis
Surfactant Inactivation
Potential for Infection
Potential for Pulmonary Hypertension
Management varies
MECONIUM ASPIRATION SYNDROME
Chemical Pneumonitis
Surfactant Inactivation
Potential for Infection
Potential for Pulmonary Hypertension
Management varies
Meconium Aspiration
Meconium Aspiration
PERSISTENT PULMONARY HYPERTENSION
Usually secondary to primary pulmonary disease state
Pulmonary Vascular Lability
Treat
PERSISTENT PULMONARY HYPERTENSION
Usually secondary to primary pulmonary disease state
Pulmonary Vascular Lability
Treat
PPHN
PPHN
CONGENITAL PNEUMONIA
Infectious; primarily GBS
Amniotic Fluid aspiration
Viral etiology
Surfactant inactivation
CONGENITAL PNEUMONIA
Infectious; primarily GBS
Amniotic Fluid aspiration
Viral etiology
Surfactant inactivation
GBS Pneumonia
GBS Pneumonia
CONGENITAL MALFORMATIONS
Choanal Atresia
Tracheal Atresia/stenosis
Chest Mass
Diaphragmatic hernia
CCAM
Sequestration
Lobar emphysema
CONGENITAL MALFORMATIONS
Choanal Atresia
Tracheal Atresia/stenosis
Chest Mass
Diaphragmatic hernia
CCAM
Sequestration
Lobar emphysema
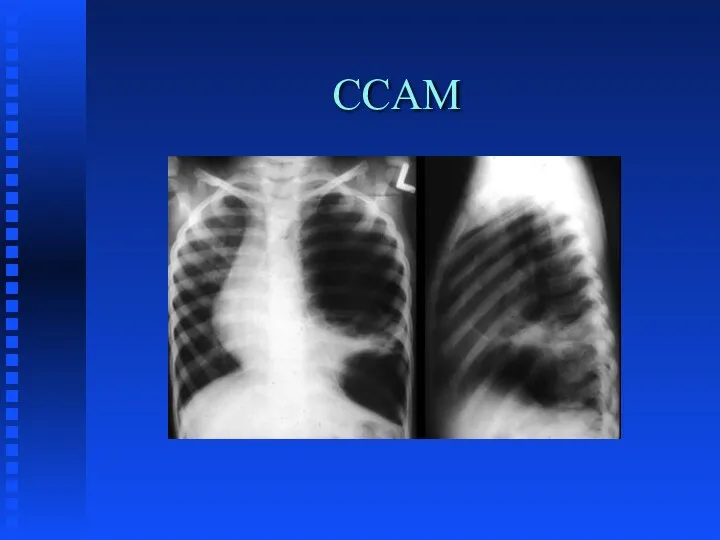
CCAM
CCAM
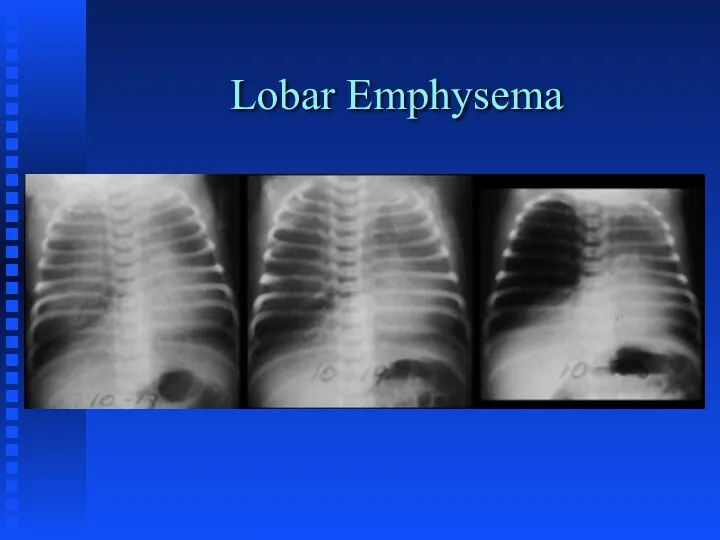
Lobar Emphysema
Lobar Emphysema
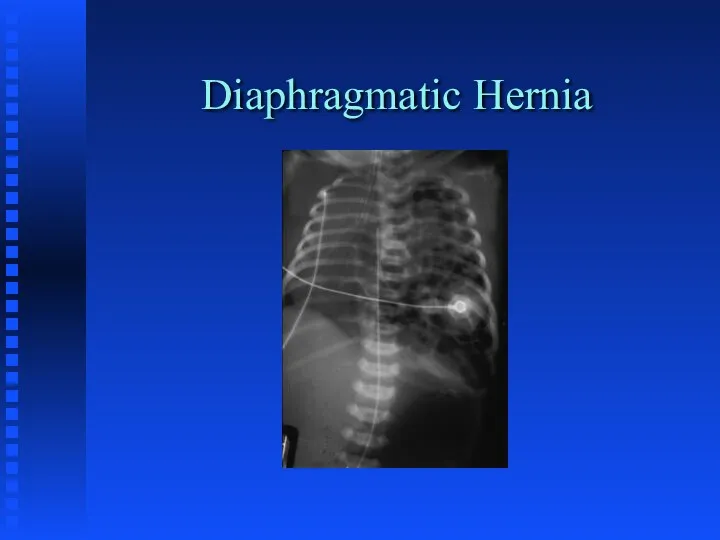
Diaphragmatic Hernia
Diaphragmatic Hernia
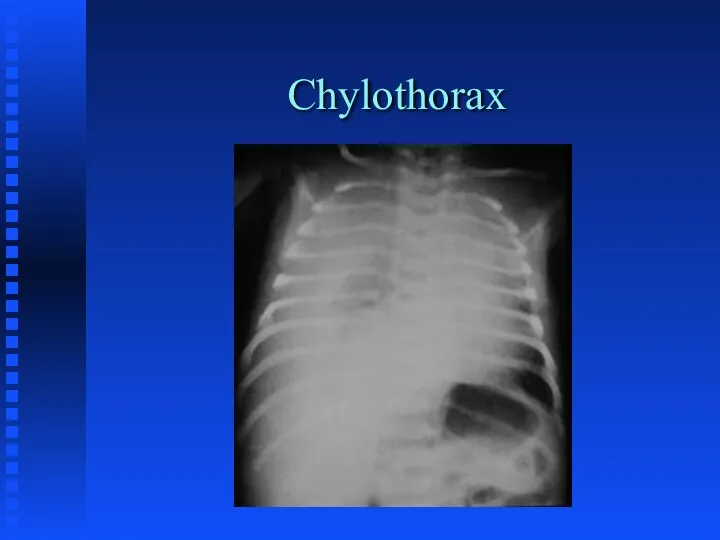
Chylothorax
Chylothorax
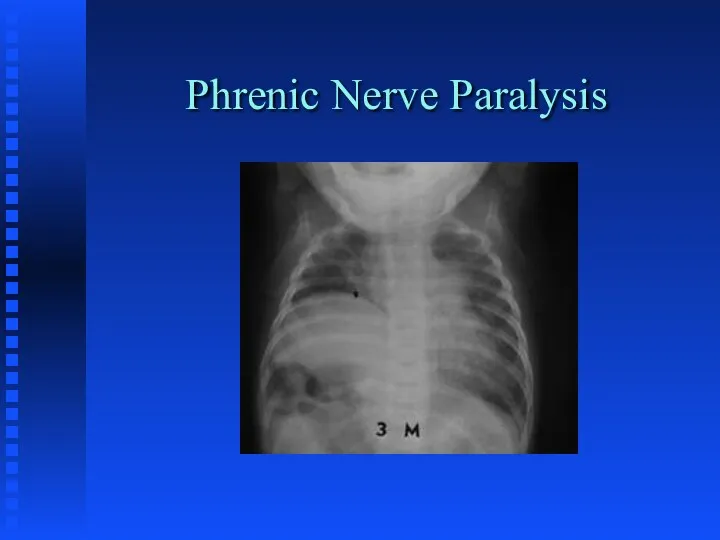
Phrenic Nerve Paralysis
Phrenic Nerve Paralysis
ACQUIRED DISEASES
Infections
Bronchopulmonary Dysplasia
Sub-glottic stenosis
Apnea of Prematurity
ACQUIRED DISEASES
Infections
Bronchopulmonary Dysplasia
Sub-glottic stenosis
Apnea of Prematurity
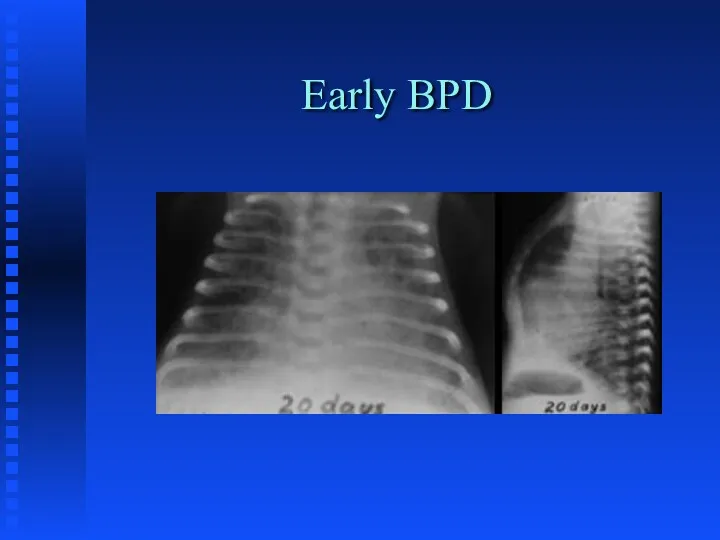
Early BPD
Early BPD
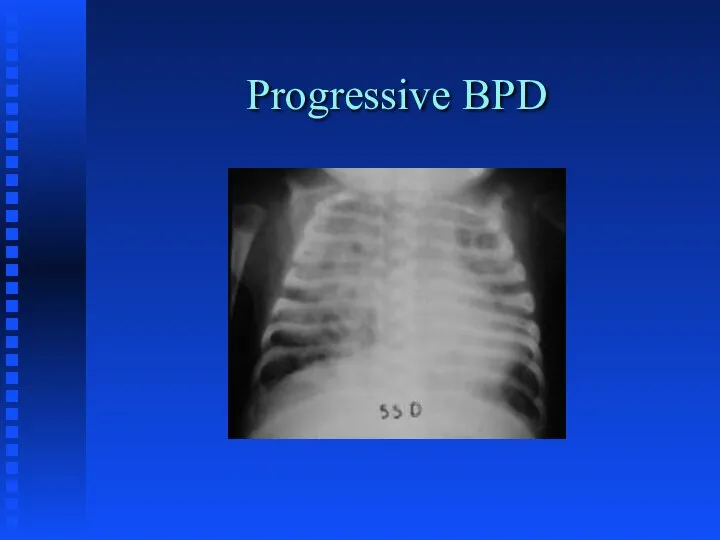
Progressive BPD
Progressive BPD
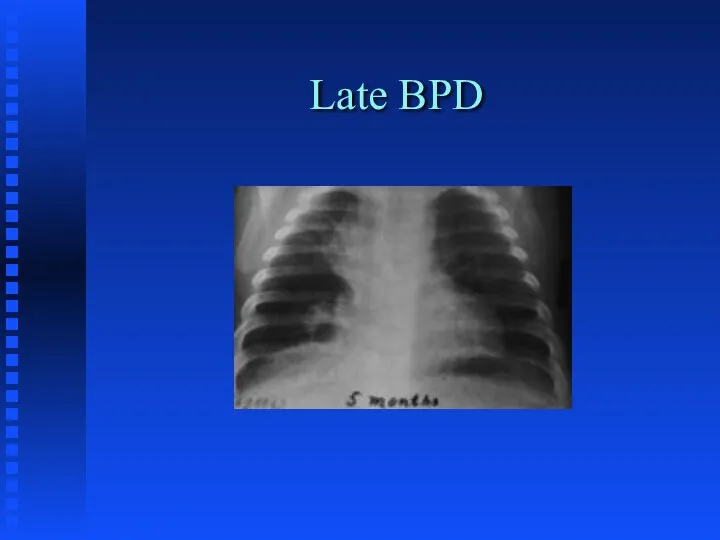
Late BPD
Late BPD
APNEA
Definition: cessation of breathing for longer than a 15 second period
APNEA
Definition: cessation of breathing for longer than a 15 second period
Babies at Risk for Apnea
Preterm
Respiratory Distress
Metabolic Disorders
Infections
Cold-stressed babies who are being
Babies at Risk for Apnea
Preterm
Respiratory Distress
Metabolic Disorders
Infections
Cold-stressed babies who are being
Anticipation and Detection
Place at-risk infants on cardio-respiratory monitor
Low heart rate limit
Anticipation and Detection
Place at-risk infants on cardio-respiratory monitor
Low heart rate limit
Treatment
Determine cause:
x-ray
blood sugar
body and environmental temperature
hematocrit
sepsis work up
electrolytes
cardiac work up
r/o
Treatment
Determine cause:
x-ray
blood sugar
body and environmental temperature
hematocrit
sepsis work up
electrolytes
cardiac work up
r/o
Treatment
CPAP
Theophylline/Caffeine therapy
Mechanical ventilation
Apnea monitor
Treatment
CPAP
Theophylline/Caffeine therapy
Mechanical ventilation
Apnea monitor
 Интегрированный урок математики и окружающего мира в 3 классе Письменное сложение и вычитание трёхзначных чисел( презентация )
Интегрированный урок математики и окружающего мира в 3 классе Письменное сложение и вычитание трёхзначных чисел( презентация ) График производной. Готовимся к ЕГЭ
График производной. Готовимся к ЕГЭ Логарифмическая функция, её свойства и график
Логарифмическая функция, её свойства и график Початкові відомості зі стереометрії. Конус
Початкові відомості зі стереометрії. Конус Дисперсионный анализ
Дисперсионный анализ Системы линейных алгебраических уравнений
Системы линейных алгебраических уравнений Устный счет 1 класс
Устный счет 1 класс Подготовка к ЕГЭ по математике. Решение заданий В3
Подготовка к ЕГЭ по математике. Решение заданий В3 Модуль числа
Модуль числа Счастливый случай. Интеллектуальная игра
Счастливый случай. Интеллектуальная игра Логистиканың даму факторлары. Материалдық ағым
Логистиканың даму факторлары. Материалдық ағым Все действия с положительными и отрицательными числами. 6 класс
Все действия с положительными и отрицательными числами. 6 класс Решение задач с помощью уравнений
Решение задач с помощью уравнений Тригонометрические уравнения
Тригонометрические уравнения Симметрия вокруг нас
Симметрия вокруг нас Отрезок. Измерение отрезков
Отрезок. Измерение отрезков Название чисел в записи действий
Название чисел в записи действий Квадратные уравнения. Решение задач с помощью квадратных уравнений
Квадратные уравнения. Решение задач с помощью квадратных уравнений Численные методы расчета переходных процессов (лекция № 20)
Численные методы расчета переходных процессов (лекция № 20) Пробный тест по математике для 4 класса
Пробный тест по математике для 4 класса Система опорних фактів курсу планіметрії
Система опорних фактів курсу планіметрії Конспект интегрированного занятия по ФЭМП Путешествие по королевству математики Диск
Конспект интегрированного занятия по ФЭМП Путешествие по королевству математики Диск Теория и методы дискретных вычислений
Теория и методы дискретных вычислений Нахождение числа по заданному значению его дроби
Нахождение числа по заданному значению его дроби Решение задач на встречное движение
Решение задач на встречное движение Корень n-й степени
Корень n-й степени Степенная функция и ее график
Степенная функция и ее график Математические задачи
Математические задачи