- Acute Glomerulonephritis

Содержание
- 2. Anatomy of the glomerulus and the juxtaglomerular apparatus All three layers (endothelium, glomerular basement membrane, slit
- 3. Fig. Glomerular basement membrane (GBM)
- 4. Glomerular diseases (glomerulopathy) heterogeneous group of diseases Dividing: Primary glomerulopathy Secondary glomerulopathy – can be manifestation
- 5. Immunopathologic mechanisms Damage of kidney depend on: mechanism and intensity of immune reaction collocation of antigens
- 6. Cytotoxic (Type II) reaction – antibody mediated cytotoxicity (ADCC) These occur when antibodies interact with antigens
- 7. Type III reaction – immune complex-mediated hypersensitivity The reaction of antibody with antigen generates immune complexes.
- 8. The magnitude of the reaction depends on the quantitity of immune complexes as well as distribution
- 9. Location of immune deposits in the glomerular capillary wall
- 10. Delayed – type hypersensitivity (Type IV) T lymphocytes may also recognize antigen When they do, a
- 11. Four major pathogenetic forms of glomerular injury In non-proliferative glomerulopathy: Damage by antibodies Damage mediate by
- 12. Classification of glomerulopathies Clinical: primary x secondary According time period: acute x subacute x chronic According
- 13. Pathogenic mechanisms of glomerular diseases NEPHRITIC NEPHROTIC Chronic glomerulonephritis
- 14. Pathogenesis of nephritic diseases
- 15. Histologic pattern May not correlate with the clinical presentation Various histological types of glomerulonephritis
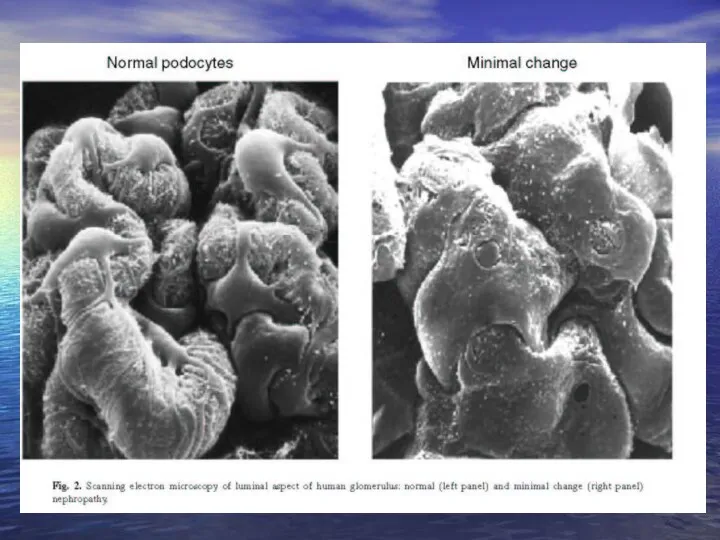
- 16. B: “Minimal changes” GN = lipoid nephrosis: some mesangial proliferation, edematous podocytes, fusion (“loss”) of their
- 17. Acute glomerulonephritis (poststreptococcal GN) Is commonly caused by infection by certain strains of group A beta-hemolytic
- 19. Postinfectional non-streptococcus glomerulonephritis Acute glomerulonephritis can develope also in the course of other infections: - stafylococci
- 20. Focal proliferative glomerulonephritis - different etiology: IgA nefropathy Nephritis in systemic lupus erythematodes (SLE) Nephritis in
- 21. Rapidly progressive glomerulonephritis (RPGN) Heterogeneous group of diseases, it is characterised by intense proliferation of glomerular/capsular
- 22. Three forms of RPGN GN with creation of antiobdies (IgG, IgA) agains GBM (anti-GBM) - linear
- 23. Goodpastures´ syndrome It is charecterised antibodies against basal membrane of glomeruli (alveolocapillary membrane) Etiology: combination of
- 24. Slowly progressive glomerulonephritis Group of GN called membrane-proliferative GN 2 forms: in 1 form : -
- 25. Pathogenesis of nephrotic diseases
- 26. „Minimal changes“ GN (lipoid nephrosis) Especially in children Pathogenesis ambiguous – connection with viral infections, vaccination,
- 28. Focal (segmental) glomerulosclerosis More serious degree - focal: - diffuse: > 50% glomerulů are affected -
- 29. Membranous GN Diffuse thickness of GBM due to deposition of IK in basement membrane Strong association
- 30. Stages of membranous GN
- 31. Idiopatic membranous glomerulopathy
- 32. Membranoproliferative (mesangiocapillary) glomerulopathy Is characterised by hypercellularity of the glomerular cells and basement membrane thickening 2
- 33. IgA nephropathy (Berger´s disease) Mesangioproliferative GN with deposits of IgA, event. C3 Etiology: - unknown, clinical
- 34. Chronic glomerulonephritis Common terminal result of many glomerular diseases („end stage kidney“) It is charecterised by
- 35. Glomerulopathy in connective tissue disorders SLE predominantly affects women, who account for 90% cases The age
- 36. Vasculitis Heterogenous group of diseases characterised by necrotizing inflammation of vessels Etiology: primary x secondary Pathogenesis:
- 37. Henoch-Schönlein purpura systemic vasculitis affecting medium-sized vessels especially in children and younger people It is frequently
- 38. Polyarteritis nodosa is an inflammatory and necrotizing disease involving the medium-sized and small arteries throughout the
- 39. Pauci-immune necrotizing GN Wegener´s granulomatosis is a vasculitis leading to sinus, pulmonary and renal disease glomerulonephritis
- 40. Diabetic nephropathy = diabetic intracapillary glomerulosclerosis (sy Kimmelstielův-Wilsonův) Etiopathogenesis: hyperglycemia affects conformation BM and mesangial matrix
- 41. Schematic demonstration of running diabetic nephropathy
- 42. Amyloidosis Kidney belong to organs most frequently affected by amyloidosis AL amyloidosis – is a complication
- 44. Скачать презентацию
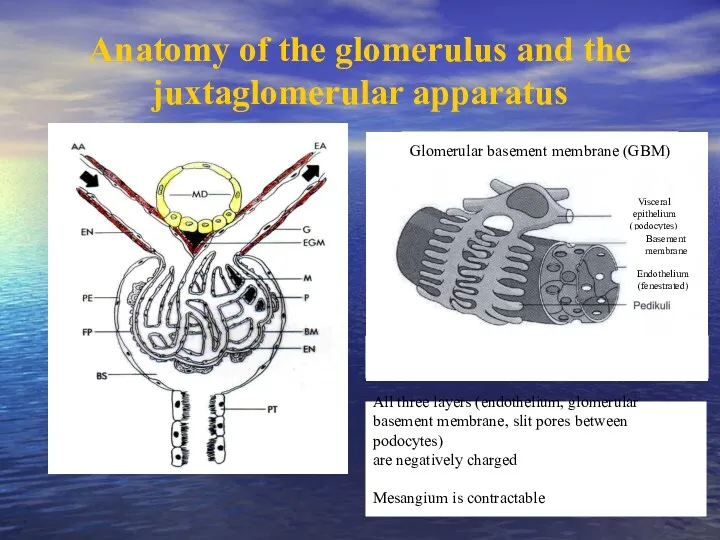
Anatomy of the glomerulus and the juxtaglomerular apparatus
All three layers (endothelium,
Anatomy of the glomerulus and the juxtaglomerular apparatus
All three layers (endothelium,
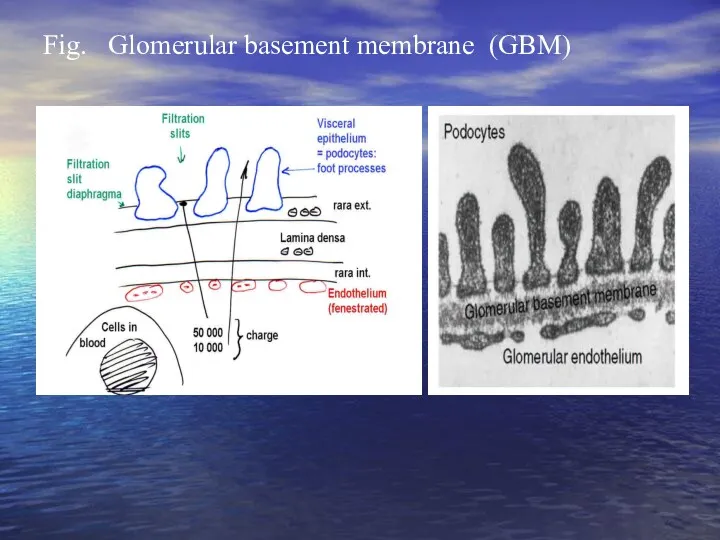
Fig. Glomerular basement membrane (GBM)
Fig. Glomerular basement membrane (GBM)
Glomerular diseases (glomerulopathy)
heterogeneous group of diseases
Dividing:
Primary glomerulopathy
Secondary glomerulopathy
–
Glomerular diseases (glomerulopathy)
heterogeneous group of diseases
Dividing:
Primary glomerulopathy
Secondary glomerulopathy
–
Immunopathologic mechanisms
Damage of kidney depend on:
mechanism and intensity of immune reaction
collocation
Immunopathologic mechanisms
Damage of kidney depend on:
mechanism and intensity of immune reaction
collocation
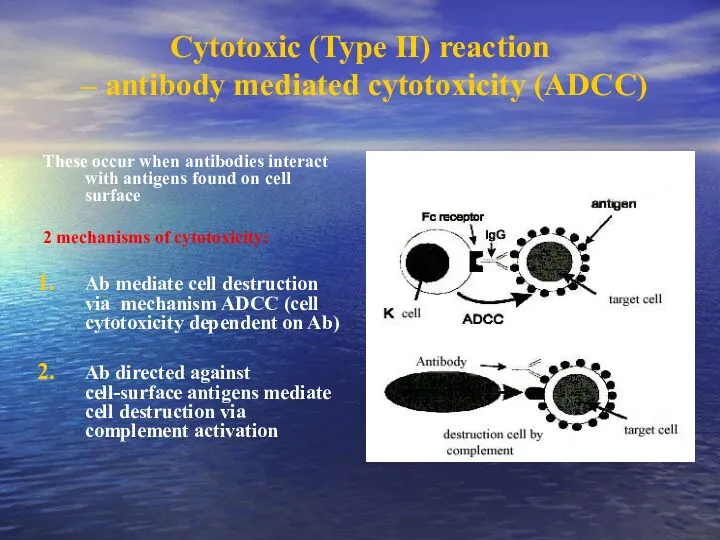
Cytotoxic (Type II) reaction
– antibody mediated cytotoxicity (ADCC)
These occur when
Cytotoxic (Type II) reaction
– antibody mediated cytotoxicity (ADCC)
These occur when
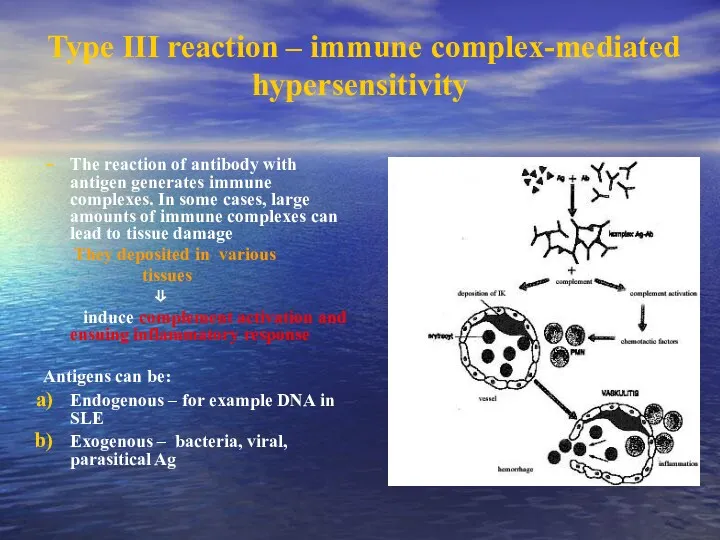
Type III reaction – immune complex-mediated hypersensitivity
The reaction of antibody with
Type III reaction – immune complex-mediated hypersensitivity
The reaction of antibody with
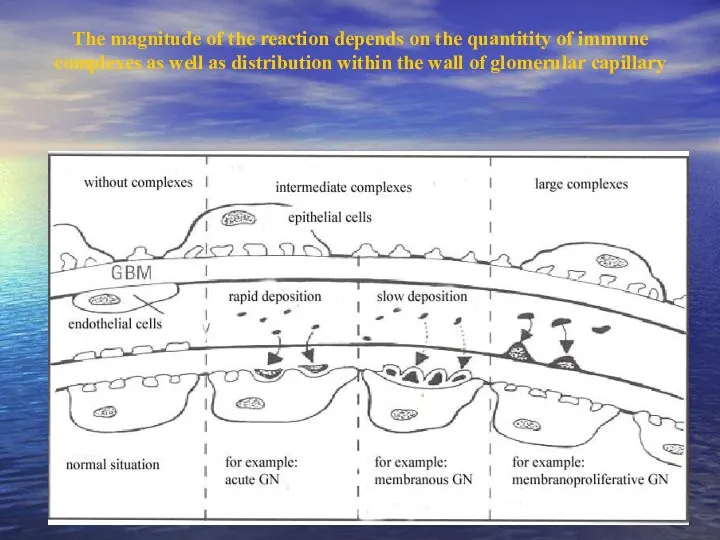
The magnitude of the reaction depends on the quantitity of immune
The magnitude of the reaction depends on the quantitity of immune
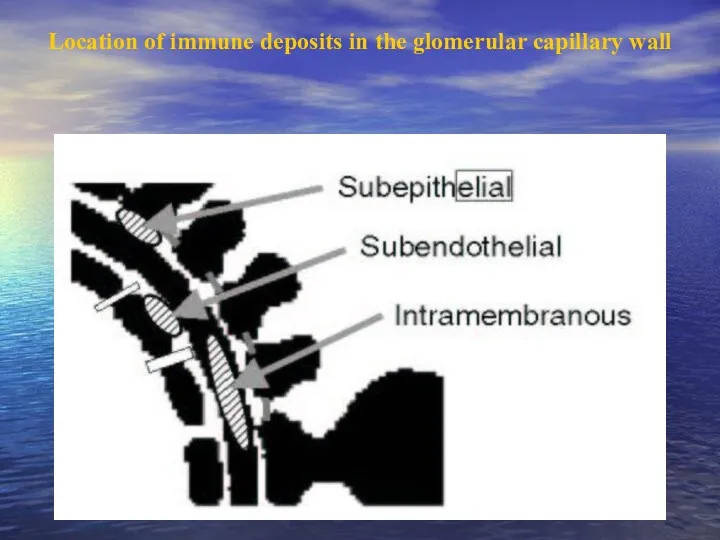
Location of immune deposits in the glomerular capillary wall
Location of immune deposits in the glomerular capillary wall
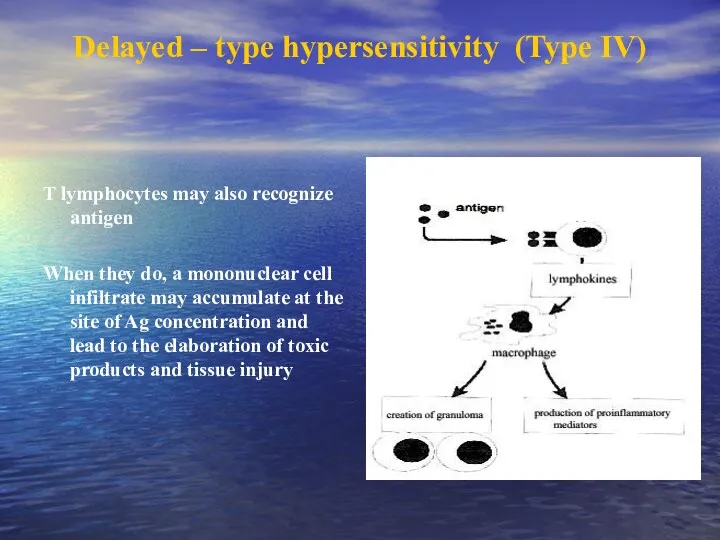
Delayed – type hypersensitivity (Type IV)
T lymphocytes may also recognize antigen
When
Delayed – type hypersensitivity (Type IV)
T lymphocytes may also recognize antigen
When
Four major pathogenetic forms of glomerular injury
In non-proliferative glomerulopathy:
Damage by antibodies
Damage
Four major pathogenetic forms of glomerular injury
In non-proliferative glomerulopathy:
Damage by antibodies
Damage
Classification of glomerulopathies
Clinical: primary x secondary
According time period: acute x subacute
Classification of glomerulopathies
Clinical: primary x secondary
According time period: acute x subacute
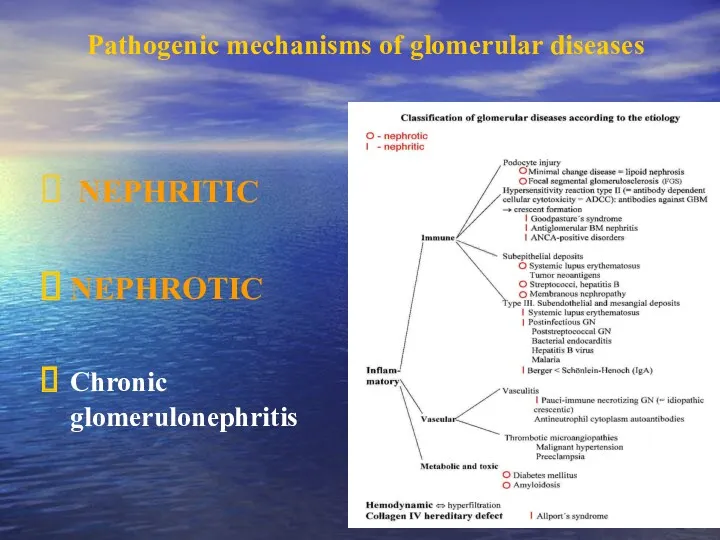
Pathogenic mechanisms of glomerular diseases
NEPHRITIC
NEPHROTIC
Chronic glomerulonephritis
Pathogenic mechanisms of glomerular diseases
NEPHRITIC
NEPHROTIC
Chronic glomerulonephritis
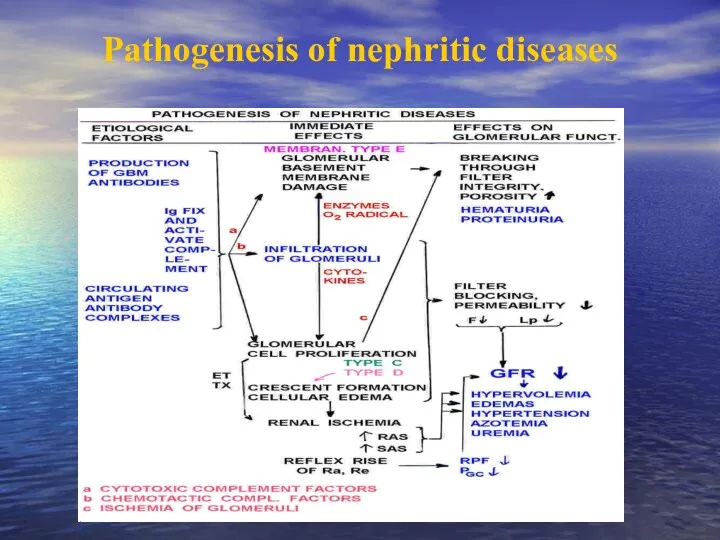
Pathogenesis of nephritic diseases
Pathogenesis of nephritic diseases
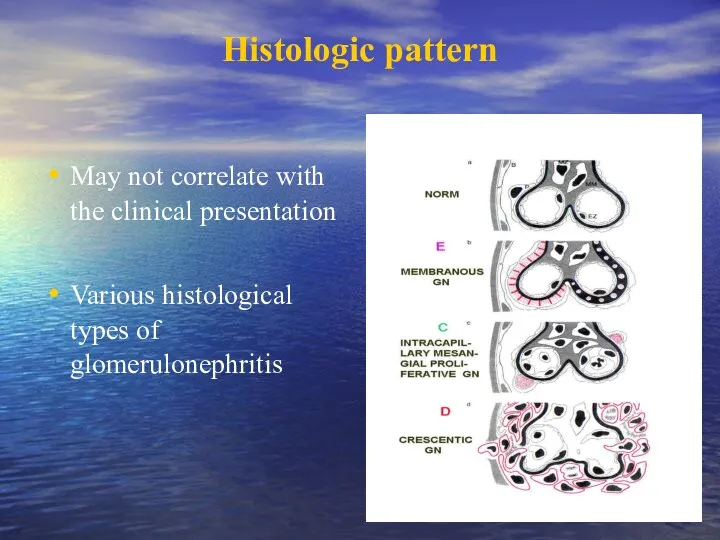
Histologic pattern
May not correlate with the clinical presentation
Various histological types
Histologic pattern
May not correlate with the clinical presentation
Various histological types
B: “Minimal changes” GN = lipoid nephrosis: some mesangial proliferation, edematous
B: “Minimal changes” GN = lipoid nephrosis: some mesangial proliferation, edematous
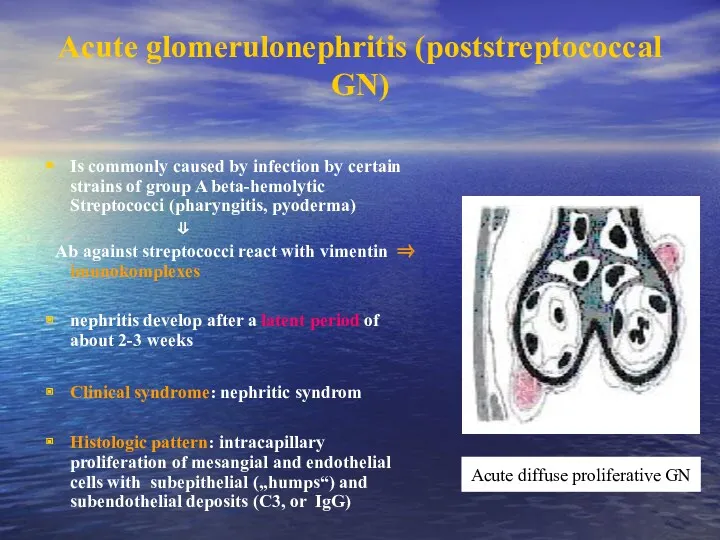
Acute glomerulonephritis (poststreptococcal GN)
Is commonly caused by infection by certain strains
Acute glomerulonephritis (poststreptococcal GN)
Is commonly caused by infection by certain strains
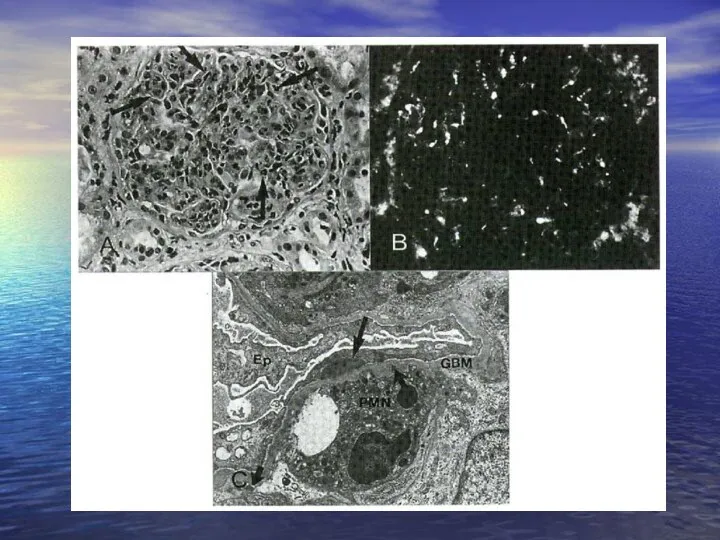
Postinfectional non-streptococcus glomerulonephritis
Acute glomerulonephritis can develope also in the course of
Postinfectional non-streptococcus glomerulonephritis
Acute glomerulonephritis can develope also in the course of

Focal proliferative glomerulonephritis
- different etiology:
IgA nefropathy
Nephritis in systemic lupus erythematodes (SLE)
Nephritis
Focal proliferative glomerulonephritis
- different etiology:
IgA nefropathy
Nephritis in systemic lupus erythematodes (SLE)
Nephritis
Rapidly progressive glomerulonephritis (RPGN)
Heterogeneous group of diseases, it is characterised by
Rapidly progressive glomerulonephritis (RPGN)
Heterogeneous group of diseases, it is characterised by
Three forms of RPGN
GN with creation of antiobdies (IgG, IgA) agains
Three forms of RPGN
GN with creation of antiobdies (IgG, IgA) agains
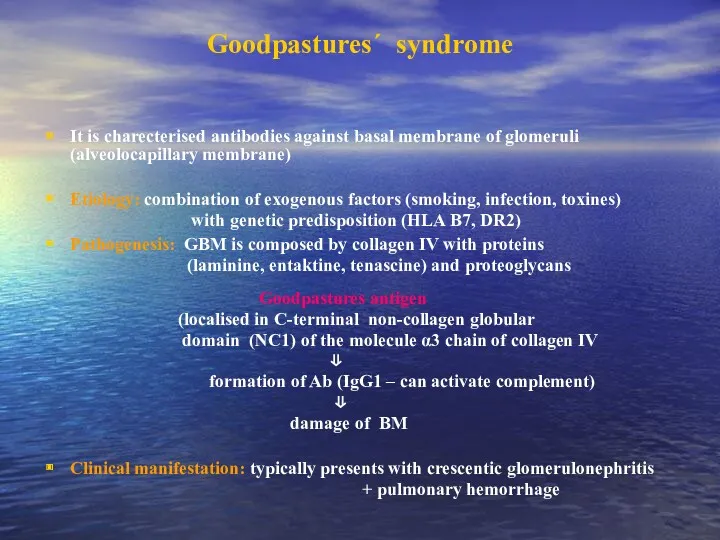
Goodpastures´ syndrome
It is charecterised antibodies against basal membrane of glomeruli (alveolocapillary
Goodpastures´ syndrome
It is charecterised antibodies against basal membrane of glomeruli (alveolocapillary
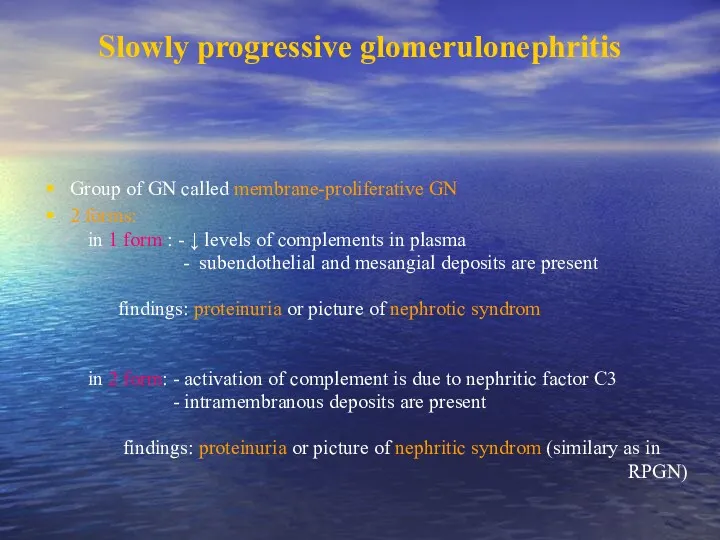
Slowly progressive glomerulonephritis
Group of GN called membrane-proliferative GN
2 forms:
in
Slowly progressive glomerulonephritis
Group of GN called membrane-proliferative GN
2 forms:
in
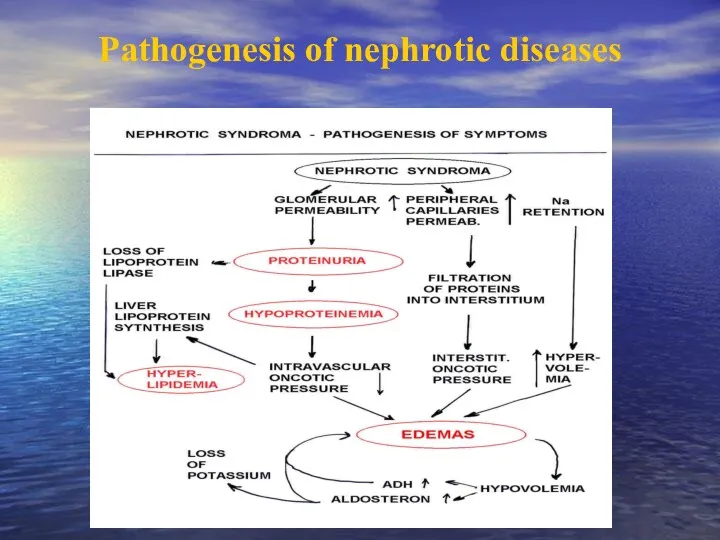
Pathogenesis of nephrotic diseases
Pathogenesis of nephrotic diseases
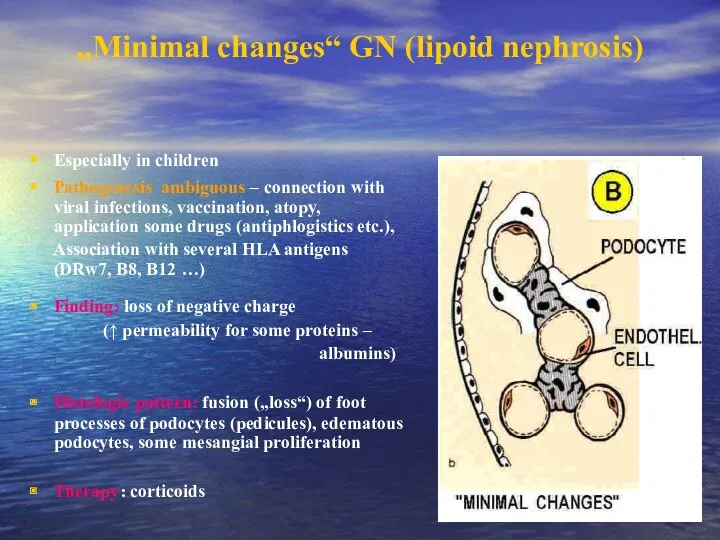
„Minimal changes“ GN (lipoid nephrosis)
Especially in children
Pathogenesis ambiguous – connection with
„Minimal changes“ GN (lipoid nephrosis)
Especially in children
Pathogenesis ambiguous – connection with
Focal (segmental) glomerulosclerosis
More serious degree
- focal: < 50% glomeruli are
Focal (segmental) glomerulosclerosis
More serious degree
- focal: < 50% glomeruli are
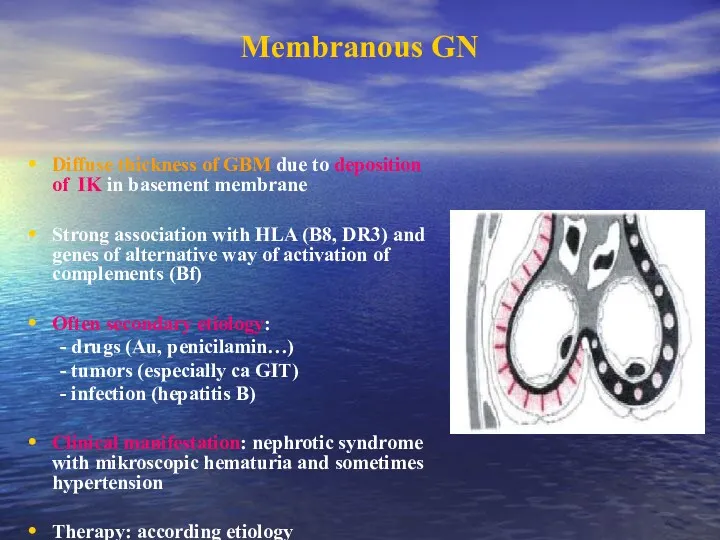
Membranous GN
Diffuse thickness of GBM due to deposition of IK in
Membranous GN
Diffuse thickness of GBM due to deposition of IK in
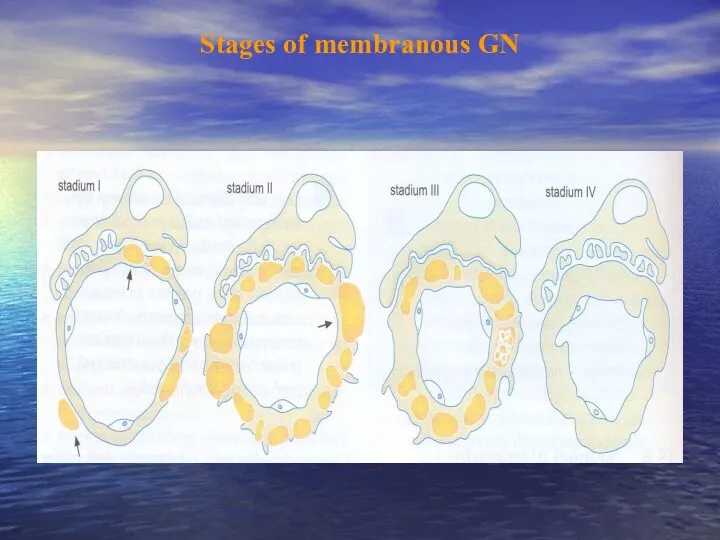
Stages of membranous GN
Stages of membranous GN
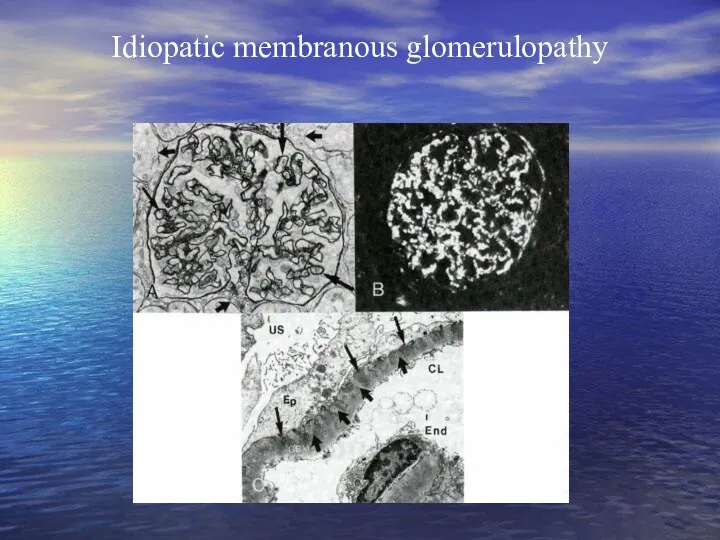
Idiopatic membranous glomerulopathy
Idiopatic membranous glomerulopathy
Membranoproliferative (mesangiocapillary) glomerulopathy
Is characterised by hypercellularity of the glomerular cells and
Membranoproliferative (mesangiocapillary) glomerulopathy
Is characterised by hypercellularity of the glomerular cells and
IgA nephropathy (Berger´s disease)
Mesangioproliferative GN with deposits of IgA, event. C3
Etiology:
IgA nephropathy (Berger´s disease)
Mesangioproliferative GN with deposits of IgA, event. C3
Etiology:
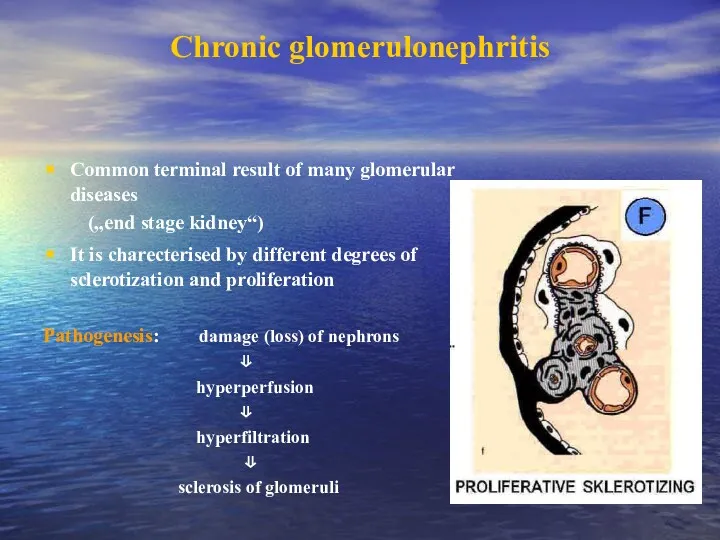
Chronic glomerulonephritis
Common terminal result of many glomerular diseases
(„end stage
Chronic glomerulonephritis
Common terminal result of many glomerular diseases
(„end stage
Glomerulopathy in connective tissue disorders
SLE predominantly affects women, who account for
Glomerulopathy in connective tissue disorders
SLE predominantly affects women, who account for
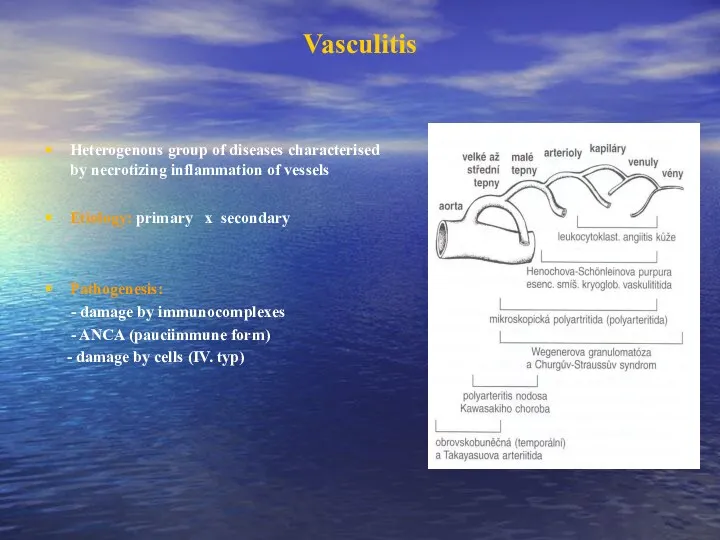
Vasculitis
Heterogenous group of diseases characterised by necrotizing inflammation of vessels
Etiology: primary
Vasculitis
Heterogenous group of diseases characterised by necrotizing inflammation of vessels
Etiology: primary
Henoch-Schönlein purpura
systemic vasculitis affecting medium-sized vessels
especially in children and younger people
It
Henoch-Schönlein purpura
systemic vasculitis affecting medium-sized vessels
especially in children and younger people
It
Polyarteritis nodosa
is an inflammatory and necrotizing disease involving the medium-sized and
Polyarteritis nodosa
is an inflammatory and necrotizing disease involving the medium-sized and
Pauci-immune necrotizing GN
Wegener´s granulomatosis
is a vasculitis leading to sinus, pulmonary and
Pauci-immune necrotizing GN
Wegener´s granulomatosis
is a vasculitis leading to sinus, pulmonary and
Diabetic nephropathy
= diabetic intracapillary glomerulosclerosis (sy Kimmelstielův-Wilsonův)
Etiopathogenesis: hyperglycemia affects conformation BM
Diabetic nephropathy
= diabetic intracapillary glomerulosclerosis (sy Kimmelstielův-Wilsonův)
Etiopathogenesis: hyperglycemia affects conformation BM
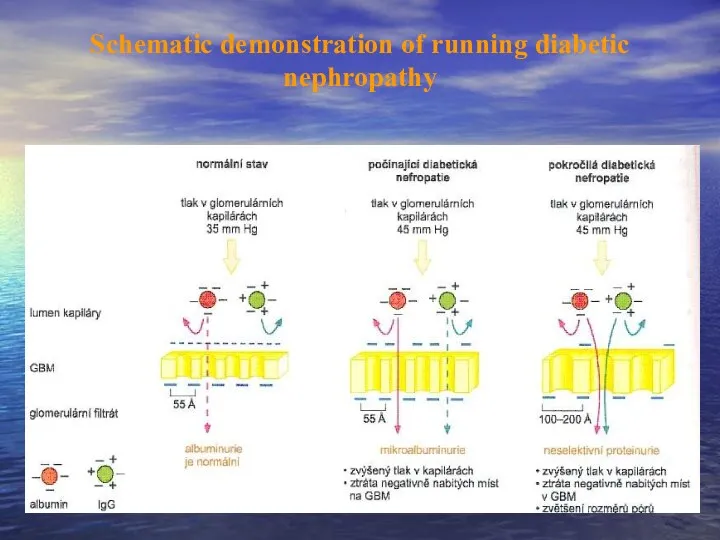
Schematic demonstration of running diabetic nephropathy
Schematic demonstration of running diabetic nephropathy
Amyloidosis
Kidney belong to organs most frequently affected by amyloidosis
AL amyloidosis –
Amyloidosis
Kidney belong to organs most frequently affected by amyloidosis
AL amyloidosis –
 Перикардиты. Анатомия перикарда
Перикардиты. Анатомия перикарда Спадкові захворювання нервової системи
Спадкові захворювання нервової системи ВИЧ: вопросы и ответы
ВИЧ: вопросы и ответы Нейтропении у детей
Нейтропении у детей Николай Иванович Пирогов Русский хирург и анатом
Николай Иванович Пирогов Русский хирург и анатом Информационные технологии для фармацевтов
Информационные технологии для фармацевтов Периоды детства
Периоды детства Антипсихотики (нейролептики)
Антипсихотики (нейролептики) Глобальные риски и новейшие медицинские технологии
Глобальные риски и новейшие медицинские технологии Компрессионные синдромы шейного отдела позвоночника
Компрессионные синдромы шейного отдела позвоночника Жанұямен қарым – қатынаста жеткен жетістіктерді және қиыншылықтарды талдау
Жанұямен қарым – қатынаста жеткен жетістіктерді және қиыншылықтарды талдау Інсульт. Причини, симптоми інсульту, перша допомога, поради
Інсульт. Причини, симптоми інсульту, перша допомога, поради Крон ауруы
Крон ауруы Pancreatic Cancer
Pancreatic Cancer Особенности фармакокинетики и фармакодинамики при лечении аллергий
Особенности фармакокинетики и фармакодинамики при лечении аллергий ИБС. Стенокардия
ИБС. Стенокардия Нәрестелердің асфиксиясы
Нәрестелердің асфиксиясы Опухолевый рост
Опухолевый рост Кілегейлі қабықтар мен мүшелерде эпителий тінінің мамандануы
Кілегейлі қабықтар мен мүшелерде эпителий тінінің мамандануы Нарушения сна у младенцев и детей раннего возраста
Нарушения сна у младенцев и детей раннего возраста Анастезия задних верхних и нижнего луночкого нерва по П.М. Егорову
Анастезия задних верхних и нижнего луночкого нерва по П.М. Егорову Токсикология фосфорорганических соединений (ФОС)
Токсикология фосфорорганических соединений (ФОС) Анатомо-фізіологічні особливості сечовидільної системи у дітей
Анатомо-фізіологічні особливості сечовидільної системи у дітей Өлім, өлім белгілері
Өлім, өлім белгілері Ми қыртысының анатомиялық-гистологиялық құрылымы
Ми қыртысының анатомиялық-гистологиялық құрылымы Воспалительные процессы органов женской половой системы специфической этиологии
Воспалительные процессы органов женской половой системы специфической этиологии Болезнь Крона
Болезнь Крона Respiratory system
Respiratory system