- Amniotic fluid embolism

Содержание
- 2. AMNIOTIC FLUID EMBOLISM AFE is thought to occur when amniotic fluid , fetal cells, hair, or
- 3. AMNIOTIC FLUID EMBOLISM Overall incidence ranges from 1 in 8,000 to 1 in 80,000 pregnancies. 10%
- 4. AMNIOTIC FLUID EMBOLISM Time of event: During labor. During C/S. After normal vaginal delivery. During second
- 5. Risk factors of AFE Advanced maternal age Multiparity Meconium Cervical laceration Intrauterine foetal death Very strong
- 6. Experimental AFE The cardiorespiratory effects of acute intravascular injection of amniotic fluid have been studied in
- 7. Experimental AFE Intravascular injection of amniotic fluid in rhesus monkeys failed to produce cardiovascular changes similar
- 8. Pathophysiology - Poorly understood. - Cotton (1996), has proposed a biphasic model. Phase 1: Amniotic fluid
- 9. Pathophysiology The similar homodynamic derangements seen with AFE syndrome , anaphylactic, and septic shock have led
- 10. Pathophysiology Measurement of tryptase ( a degranulation product of mast cells released with histamine during anaphylactic
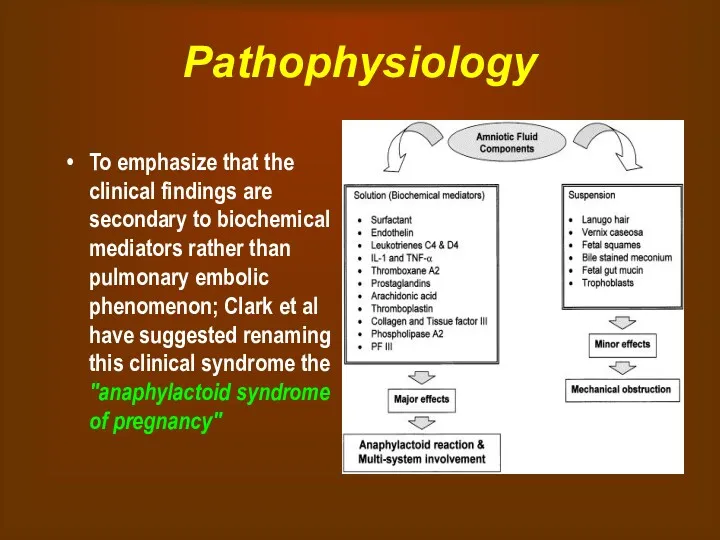
- 11. Pathophysiology To emphasize that the clinical findings are secondary to biochemical mediators rather than pulmonary embolic
- 12. Clinical presentation The classic clinical presentation of the syndrome has been described by five signs that
- 13. Clinical presentation A sudden drop in O2 saturation can be the initial indication of AFE during
- 14. Clinical presentation 10-15% of patients will develop grand mal seizures. CXR may be normal or show
- 15. Diagnosis In 1941, Steiner and Luschbaugh described histopathologic findings in the pulmonary vasculature in 8 multiparous
- 16. Laboratory investigations in suspected AFE Non specific complete blood count coagulation parameters including FDP, fibrinogen arterial
- 17. Differential diagnosis Obviously depends upon presentation Anaphylaxis (Collapse) Pulmonary embolus (Collapse) Aspiration (Hypoxaemia) Pre-eclampsia or eclampsia
- 18. Management of AFE GOALS OF MANAGEMENT: Restoration of cardiovascular and pulmonary equilibrium Maintain systolic blood pressure
- 19. Management of AFE As intubation and CPR may be required it is necessary to have easy
- 20. Management of AFE Treat hypotension, increase the circulating volume and cardiac output with crystalloids. After correction
- 21. Management of AFE In the ICU To assess the effectiveness of treatment and resuscitation, it is
- 22. Management of AFE In the ICU Central venous pressure monitoring is important to diagnose right ventricular
- 23. Management of AFE Coagulopathy DIC results in the depletion of fibrinogen, platelets, and coagulation factors, especially
- 24. Restoration of uterine tone Uterine atony is best treated with massage, uterine packing, and oxytocin or
- 25. Sympathomimetic Vasopressor agent Dopamine Dopamine increases myocardial contractility and systolic BP with little increase in diastolic
- 26. Maternal Mortality in AFE Maternal death usually occurs in one of three ways: (1) sudden cardiac
- 27. Further issues in the Management Transfer: Transfer to a level 3 hospital may be required once
- 28. Medical/Legal Pitfalls Failure to respond emergently is a pitfall. AFE is a clinical diagnosis. Steps must
- 29. SUMMARY AFE is a sudden and unexpected rare but life threatining complication of pregnancy. It has
- 31. Скачать презентацию
AMNIOTIC FLUID EMBOLISM
AFE is thought to occur when amniotic fluid ,
AMNIOTIC FLUID EMBOLISM
AFE is thought to occur when amniotic fluid ,
AMNIOTIC FLUID EMBOLISM
Overall incidence ranges from 1 in 8,000 to 1
AMNIOTIC FLUID EMBOLISM
Overall incidence ranges from 1 in 8,000 to 1
AMNIOTIC FLUID EMBOLISM
Time of event:
During labor.
During C/S.
After normal vaginal delivery.
During second
AMNIOTIC FLUID EMBOLISM
Time of event:
During labor.
During C/S.
After normal vaginal delivery.
During second
Risk factors of AFE
Advanced maternal age
Multiparity
Meconium
Cervical laceration
Intrauterine foetal death
Very strong frequent
Risk factors of AFE
Advanced maternal age
Multiparity
Meconium
Cervical laceration
Intrauterine foetal death
Very strong frequent
Experimental AFE
The cardiorespiratory effects of acute intravascular injection of amniotic fluid
Experimental AFE
The cardiorespiratory effects of acute intravascular injection of amniotic fluid
Experimental AFE
Intravascular injection of amniotic fluid in rhesus monkeys failed to
Experimental AFE
Intravascular injection of amniotic fluid in rhesus monkeys failed to
Pathophysiology
- Poorly understood.
- Cotton (1996), has proposed a biphasic model. Phase
Pathophysiology
- Poorly understood.
- Cotton (1996), has proposed a biphasic model. Phase
Pathophysiology
The similar homodynamic derangements seen with AFE syndrome , anaphylactic, and
Pathophysiology
The similar homodynamic derangements seen with AFE syndrome , anaphylactic, and
Pathophysiology
Measurement of tryptase ( a degranulation product of mast cells released
Pathophysiology
Measurement of tryptase ( a degranulation product of mast cells released
Pathophysiology
To emphasize that the clinical findings are secondary to biochemical mediators
Pathophysiology
To emphasize that the clinical findings are secondary to biochemical mediators
Clinical presentation
The classic clinical presentation of the syndrome has been described
Clinical presentation
The classic clinical presentation of the syndrome has been described
Clinical presentation
A sudden drop in O2 saturation can be the initial
Clinical presentation
A sudden drop in O2 saturation can be the initial
Clinical presentation
10-15% of patients will develop grand mal seizures.
CXR may be
Clinical presentation
10-15% of patients will develop grand mal seizures.
CXR may be
Diagnosis
In 1941, Steiner and Luschbaugh described histopathologic findings in the pulmonary
Diagnosis
In 1941, Steiner and Luschbaugh described histopathologic findings in the pulmonary
Laboratory investigations in suspected AFE
Non specific
complete blood count
coagulation parameters including FDP,
Laboratory investigations in suspected AFE
Non specific
complete blood count
coagulation parameters including FDP,
Differential diagnosis
Obviously depends upon presentation
Anaphylaxis (Collapse)
Pulmonary embolus (Collapse)
Aspiration (Hypoxaemia)
Pre-eclampsia or eclampsia
Differential diagnosis
Obviously depends upon presentation
Anaphylaxis (Collapse)
Pulmonary embolus (Collapse)
Aspiration (Hypoxaemia)
Pre-eclampsia or eclampsia
Management of AFE
GOALS OF MANAGEMENT:
Restoration of cardiovascular and pulmonary equilibrium
Maintain systolic
Management of AFE
GOALS OF MANAGEMENT:
Restoration of cardiovascular and pulmonary equilibrium
Maintain systolic
Management of AFE
As intubation and CPR may be required it is
Management of AFE
As intubation and CPR may be required it is
Management of AFE
Treat hypotension, increase the circulating volume and cardiac output
Management of AFE
Treat hypotension, increase the circulating volume and cardiac output
Management of AFE In the ICU
To assess the effectiveness of treatment
Management of AFE In the ICU
To assess the effectiveness of treatment
Management of AFE In the ICU
Central venous pressure monitoring is important
Management of AFE In the ICU
Central venous pressure monitoring is important
Management of AFE Coagulopathy
DIC results in the depletion of fibrinogen, platelets,
Management of AFE Coagulopathy
DIC results in the depletion of fibrinogen, platelets,
Restoration of uterine tone
Uterine atony is best treated with massage, uterine
Restoration of uterine tone
Uterine atony is best treated with massage, uterine
Sympathomimetic Vasopressor agent
Dopamine
Dopamine increases myocardial contractility and systolic BP with little
Sympathomimetic Vasopressor agent
Dopamine
Dopamine increases myocardial contractility and systolic BP with little
Maternal Mortality in AFE
Maternal death usually occurs in one of three
Maternal Mortality in AFE
Maternal death usually occurs in one of three
Further issues in the Management
Transfer:
Transfer to a level 3 hospital may
Further issues in the Management
Transfer:
Transfer to a level 3 hospital may
Medical/Legal Pitfalls
Failure to respond emergently is a pitfall. AFE is a
Medical/Legal Pitfalls
Failure to respond emergently is a pitfall. AFE is a
SUMMARY
AFE is a sudden and unexpected rare but life threatining complication
SUMMARY
AFE is a sudden and unexpected rare but life threatining complication
 Державна санітарно-епідеміологічна експертиза, як елемент соціально-гігієнічного моніторингу. Основні положення та організація
Державна санітарно-епідеміологічна експертиза, як елемент соціально-гігієнічного моніторингу. Основні положення та організація Операции на органах шеи
Операции на органах шеи Физиология паращитовидных желёз
Физиология паращитовидных желёз Повреждения и заболевания мочеполовых органов
Повреждения и заболевания мочеполовых органов Хирург Н.Н. Бурденко
Хирург Н.Н. Бурденко Арбовирусты инфекциялар. Кенелік энцефалит вирусы
Арбовирусты инфекциялар. Кенелік энцефалит вирусы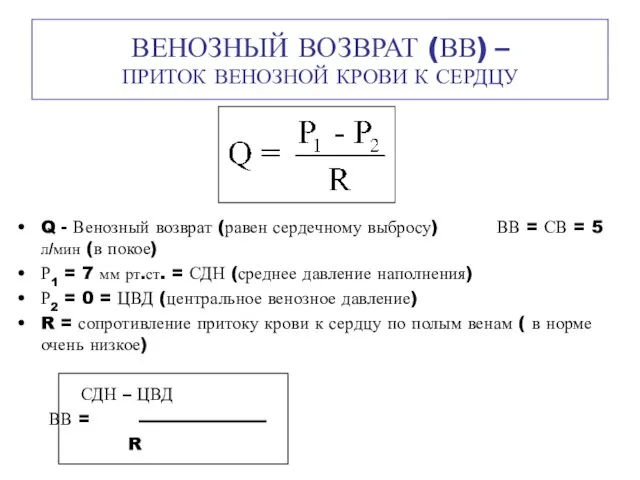 Венозный возврат (ВВ) – приток венозной крови к сердцу
Венозный возврат (ВВ) – приток венозной крови к сердцу Шум и вибрация
Шум и вибрация Алкогольный цирроз
Алкогольный цирроз Возрастные особенности системы крови и иммунитета
Возрастные особенности системы крови и иммунитета Неврозы
Неврозы Противоаритмические лекарственные средства
Противоаритмические лекарственные средства Здоровье на работе. Что должен знать о ВИЧ/СПИДе каждый?
Здоровье на работе. Что должен знать о ВИЧ/СПИДе каждый? Гигиена аптечных заведений
Гигиена аптечных заведений Гиперчувствительность. Иммунодефициты. Аутоиммунные процессы
Гиперчувствительность. Иммунодефициты. Аутоиммунные процессы Послеродовые депрессии
Послеродовые депрессии Аллергия. Стоматология
Аллергия. Стоматология 84-я Всероссийская научная конференция студентов и молодых ученых. Отчет. Секция: Общая хирургия
84-я Всероссийская научная конференция студентов и молодых ученых. Отчет. Секция: Общая хирургия Клинико-экономические исследования
Клинико-экономические исследования Химиотерапевтические лекарственные препараты, макролиды и азалиды
Химиотерапевтические лекарственные препараты, макролиды и азалиды Пороки сердца
Пороки сердца Асқорыту жолдарының қатерлі және қатерсіз ісіктері
Асқорыту жолдарының қатерлі және қатерсіз ісіктері Мировые демографические показатели рождаемость, смертность в развитых и развивающихся странах. Демографическая ситуация в Росси
Мировые демографические показатели рождаемость, смертность в развитых и развивающихся странах. Демографическая ситуация в Росси Классификация геморрагического васкулита
Классификация геморрагического васкулита Белки
Белки ЦМК СД в акушерстве и гинекологии ,
ЦМК СД в акушерстве и гинекологии , Medical Education in Japan
Medical Education in Japan Заболевания органов пищеварения у пожилых людей
Заболевания органов пищеварения у пожилых людей