- Anti-inflammatory drugs

Содержание
- 2. Plan of lecture: Anti-inflammatory agents Anti-allergic drugs Immunomodulators
- 3. Inflammation Inflammation is a complex protective response of the organism to injury caused by damaging agents.
- 4. Mediators of inflammation Prostaglandins Bradykinin Serotonin Histamine Interleukins-2 – 6, 10, 12,13 Platelet activating factor Gamma-Interferon
- 5. The role of some prostaglandins in the body PGE 2 – vasodilation, bronchodilation, inhibition of gastric
- 6. Cyclo-oxygenase (COX) Exists in the tissue as constitutive isoform (COX-1). At site of inflammation, cytokines stim
- 7. NSAIDs – nonsteroidal anti-inflammatory drugs
- 8. 1. Nonsteroidal anti-inflammatory drugs (NSAIDs) Nonselective COX inhibitors 1. Salicylates *Acetylsalicylic acid (Aspirin) * Salicylamide 2.
- 9. Selective COX inhibitors Preferential COX-2 inhibitors Nimesulide Meloxicam Nabumeton Selective COX-2 inhibitors Celecoxib Parecoxib Rofecoxib NB!!!These
- 10. Mechanism of action of NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) • Act by inhibiting CycloOXygenases (COX) => no
- 11. Mechanism of anti-inflammatory drugs’ action
- 12. Pharmacological effects of NSAIDs Anti-inflammatory Analgesic Antipyretic Antiplatelet (Aspirin) Closure of ductus arteriosus in newborn
- 13. Clinical uses of NSAIDs 1. Pain: headache, toothache, myalgia, backpain; 2. Fever; 3. Arthritises: rheumatiod arthritis,
- 15. Side effects of NSAIDs 1. GIT disturbances: epigastric pain, nausea, gastric peptic ulcer (especially aspirin), gastrointestinal
- 16. Contraindications A) Pregnancy B) Haemophilic patients C) Hypersensitivity reactions D) Viral infections mainly in children E)
- 17. Drugs interaction Potentiates the gastric irritant effect of alcohol Potentiates the hypoglycaemic effects of oral hypoglycaemic
- 18. The Salicylates - ASPIRIN Duration of action ~ 4 hr. Orally taken. Weak acid (pKa ~
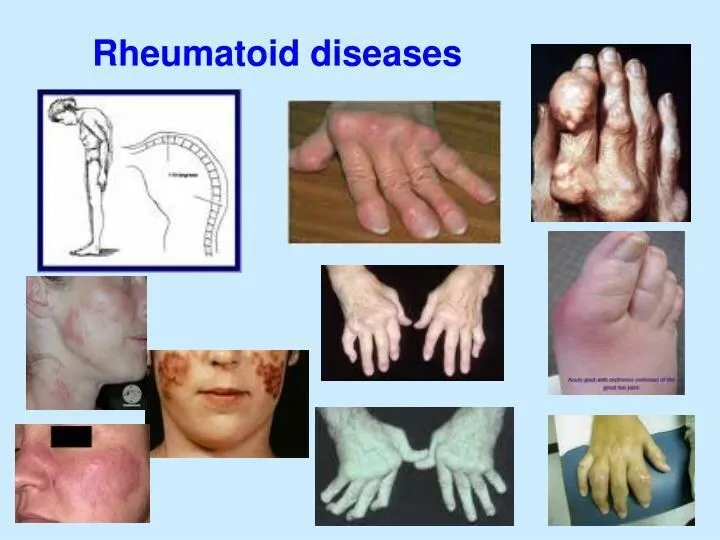
- 19. ASPIRIN - Therapeutic Uses Antipyretic, analgesic. Anti-inflammatory: rheumatic fever, rheumatoid arthritis (joint dis), other rheumatological diseases.
- 20. Propionic acid derivatives IBUPROFEN: Pharmacokinetics Rapidly absorbed after oral ingestion. Half-life 1-2 hours Highly bound to
- 21. IBUPROFEN The same mechanism & pharmacological actions of aspirin Except that it is reversible inhibitor for
- 22. Clinical uses A) Analgesic B) Antipyretic C) Anti-inflammatory D)Acute gouty arthritis E) Patent ductus arteriosus
- 23. Preparations of Ibuprofen Oral preparations. Topical cream for osteoarthritis. A liquid gel for rapid relief of
- 24. Adverse effects 1.Gastric upset (less frequent than aspirin). 2.Fluid retention 3.Hypersensetivity reactions 4.Ocular disturbances 5.Rare hematologic
- 25. Contraindications 1. Peptic ulcer 2. Allergic patients to aspirin 3. Kidney impairment 4.Liver diseases 5.Pregnancy 6.Haemophilic
- 26. Piroxicam Mechanism of actions: A) Non-selective inhibitors to COX1 & COX2 B) Traps free radicals C)
- 27. Pharmacokinetics Well absorbed orally Half- Life 45 hours Given once daily
- 28. Adverse effects Less frequent gastric upset (20%). Dizziness. Tinnitus. Headache. Allergy.
- 29. Acetic acid derivatives DICLOFENAC Mechanism of action Non-selective inhibitor to COX1 & COX2. More potent as
- 30. Clinical uses DICLOFENAC A) Any inflammatory conditions B) Musculoskeletal pain C) Dysmenorrhoea D)Acute gouty arthritis E)
- 31. Adverse effects DICLOFENAC Gastric upset Renal impairment Elevation of serum aminotransferase Salt & water retention
- 32. Preparations of DICLOFENAC Diclofenac with misoprostol decreases upper gastrointestinal ulceration, but result in diarrhea. Diclofenac with
- 33. Selective COX 2 inhibitors Advantages: 1. Highly selective inhibitors to COX2 enzyme. 2. Potent anti-inflammatory. 3.
- 34. Selective Cox 2 inhibitors 5. Lower incidence of gastric upset. 6. No effect on platelet aggregation
- 35. Selective Cox 2 inhibitors 9- They are recommended in postoperative patients undergoing bone repair. 10- Also,
- 36. SAIDs – steroidal anti-inflammatory drugs
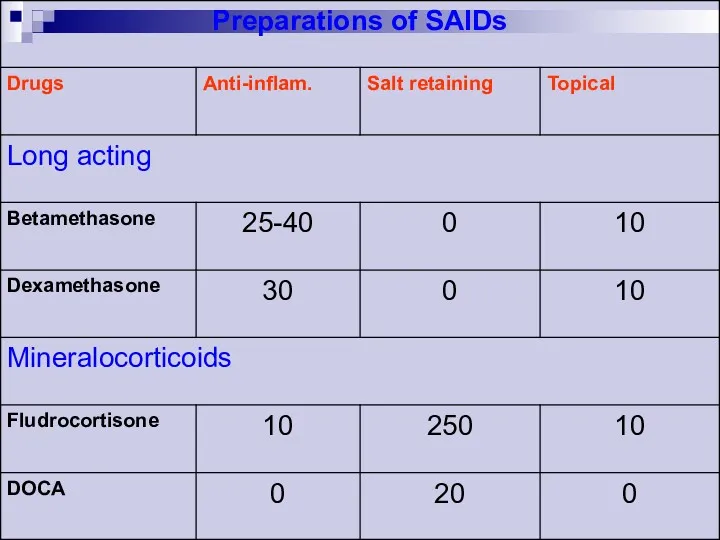
- 37. Steroidal anti-inflammatory drugs 1. Short-acting glucocorticoids (natural) Hydrocortisone Cortisone 2. Intermediate-acting glucocorticoids Prednisone Prednisolone Methylprednisolone Triamcinolone
- 40. Phospholipids Arachidonic acids Lipoxygenase Cycylooxygenase Leukotriene Prostaglandins, Thromboxane, Prostacyclins. Phospholipase A2 Corticosteroids MECHANISM OF ACTION OF
- 41. Clinical uses of SAIDs Adrenal insufficiency Arthrities Collagen diseases (systemic lupus erhymatosis, scleroderma) Bronchial asthma Severe
- 42. Main side effects of SAIDs Susceptibility to infections Delayed healing of wounds Osteoporosis Growth retardation in
- 43. ANTI-ALLERGIC DRUGS
- 44. Allergy An allergy is a hypersensitivity disorder of the immune system. Allergic reactions occur when a
- 45. mild/cutaneous mild to moderate severe/ anaphylactic erythema, urticaria, and/or itching skin reactions, tachycardia, dysrhythmias, moderate hypotension,
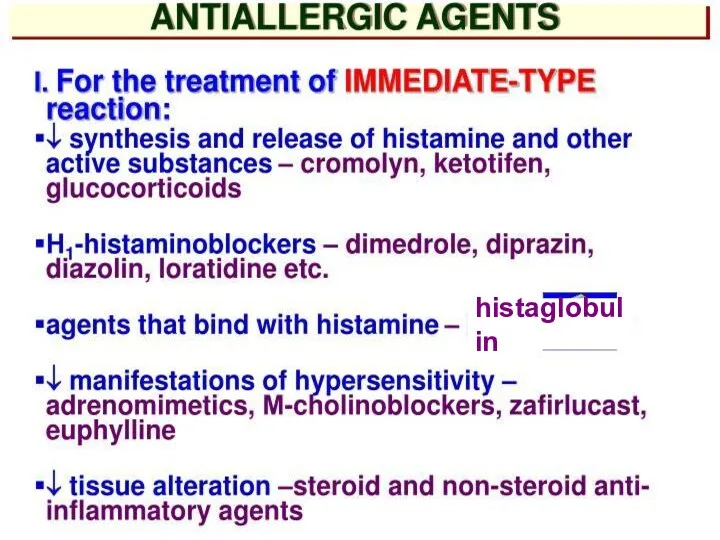
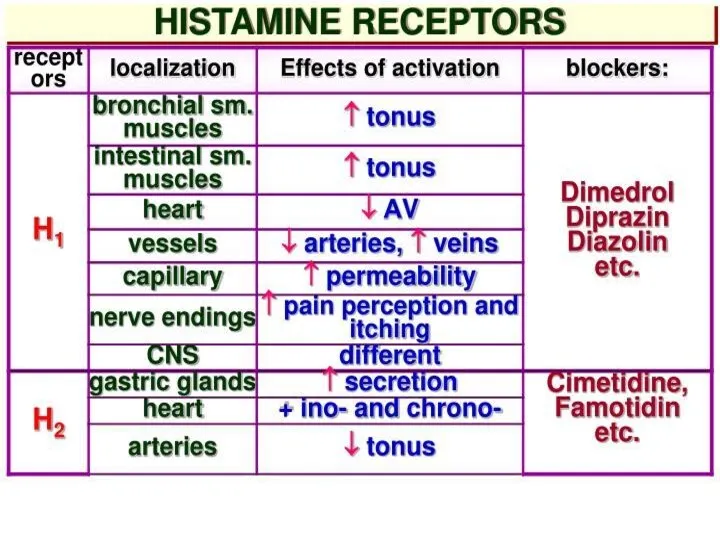
- 46. Histamine exerts its effects on many tissues and organs: It is not a drug but is
- 47. Pathophysiological Actions of Histamine Cellular mediator of immediate hypersensitivity reaction and acute inflammatory response Anaphylaxis Seasonal
- 48. Pharmacological Effects of Histamine Ranges from mild allergic symptoms to anaphylactic shock Involves both the H1
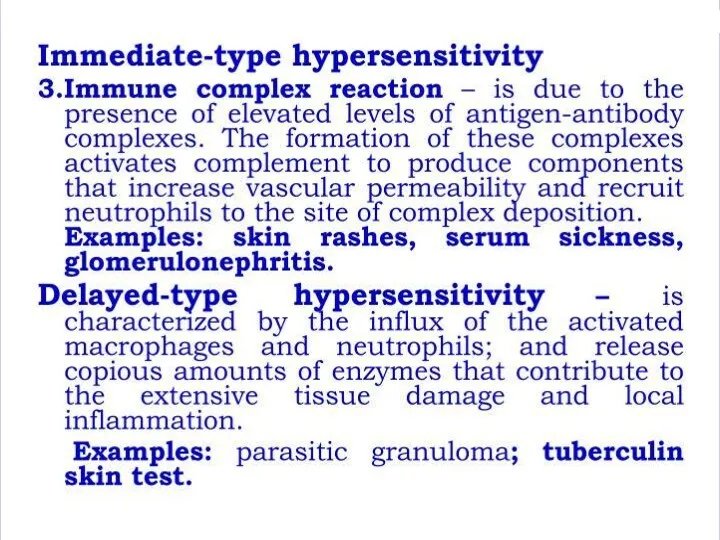
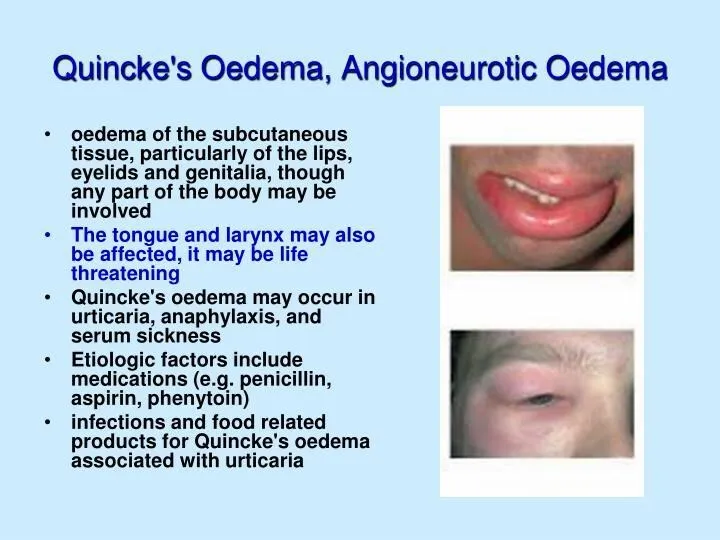
- 49. (Oedema of Quincke, Stevence-Johnson syndrome)
- 53. Antiallergic drugs 1. Antihistaminics 2. Corticosteroids 3. Mast cell stabilisers 4.Antileukotriene drugs
- 54. histaglobulin
- 58. Histamine-related Drugs Mast Cell Stabilizers (Cromolyn Na, Nedocromil –Tilade -, Albuterol) H1 Receptor Antagonists (1st and
- 59. First Generation ANTIHISTAMINE Agents Ethanolamines: DIPHENHYDRAMINE (Benadryl) CLEMASTINE (Tavist) Ethylenediamine:TRIPELENNAMINE Alkylamine:CHLORPHENIRAMINE (Chlortrimeton) Phenothiazine:PROMETHAZINE (Phenergan) Piperazines: HYDROXYZINE
- 60. Uses: Adjunctive in anaphylaxis and other cases where histamine release can occur (H2 antagonist, and epinephrine
- 61. First Generation Agents Adverse Effects: Sedation (Paradoxical Excitation in children) Dizziness Fatigue Tachydysrhythmias in overdose -
- 62. Drug interactions: Additive with classical antimuscarinics Potentiate CNS depressants opioids sedatives general and narcotic analgesics alcohol
- 63. Uses Antiallergy Examples CETIRIZINE (ZYRTEC) FEXOFENADINE (ALLEGRA) LORATADINE (CLARITIN) DESLORATADINE (CLARINEX- FDA APPROVED IN 2002) LORATADINE
- 65. Histamine H1- Antagonists First Generation: !!!Sedating!!! Second Generation: !!!Non sedating!!!
- 66. Advantages of 2nd generation antihistaminics Higher H1 selectivity, absence of anticholinergic side effects Absence of inhibitory
- 67. Mast cell stabilisers Cromolyn sodium (Sodium cromoglycate) Nedocromil sodium Ketotifen Corticosteroids (vide supra)
- 69. Antileukotriene drugs Montelukast Zafirlukast Mechanism: competitive block of LT1 receptors Clinical use: bronchial asthma
- 71. Immunomodulators
- 83. Скачать презентацию

Plan of lecture:
Anti-inflammatory agents
Anti-allergic drugs
Immunomodulators
Plan of lecture:
Anti-inflammatory agents
Anti-allergic drugs
Immunomodulators
Inflammation
Inflammation is a complex protective response of the organism to
Inflammation
Inflammation is a complex protective response of the organism to
Mediators of inflammation
Prostaglandins
Bradykinin
Serotonin
Histamine
Interleukins-2 – 6, 10, 12,13
Platelet activating factor
Gamma-Interferon
Tumor Necrosis Factor
Transforming
Mediators of inflammation
Prostaglandins
Bradykinin
Serotonin
Histamine
Interleukins-2 – 6, 10, 12,13
Platelet activating factor
Gamma-Interferon
Tumor Necrosis Factor
Transforming
The role of some prostaglandins in the body
PGE 2 – vasodilation,
The role of some prostaglandins in the body
PGE 2 – vasodilation,
Cyclo-oxygenase (COX)
Exists in the tissue as constitutive isoform (COX-1).
At site of
Cyclo-oxygenase (COX)
Exists in the tissue as constitutive isoform (COX-1).
At site of

NSAIDs – nonsteroidal
anti-inflammatory drugs
NSAIDs – nonsteroidal
anti-inflammatory drugs
1. Nonsteroidal anti-inflammatory drugs (NSAIDs)
Nonselective COX inhibitors
1. Salicylates
*Acetylsalicylic acid (Aspirin)
*
1. Nonsteroidal anti-inflammatory drugs (NSAIDs)
Nonselective COX inhibitors
1. Salicylates
*Acetylsalicylic acid (Aspirin)
*
Selective COX inhibitors
Preferential COX-2 inhibitors
Nimesulide
Meloxicam
Nabumeton
Selective COX-2 inhibitors
Celecoxib
Parecoxib
Rofecoxib
NB!!!These drugs cause little
Selective COX inhibitors
Preferential COX-2 inhibitors
Nimesulide
Meloxicam
Nabumeton
Selective COX-2 inhibitors
Celecoxib
Parecoxib
Rofecoxib
NB!!!These drugs cause little
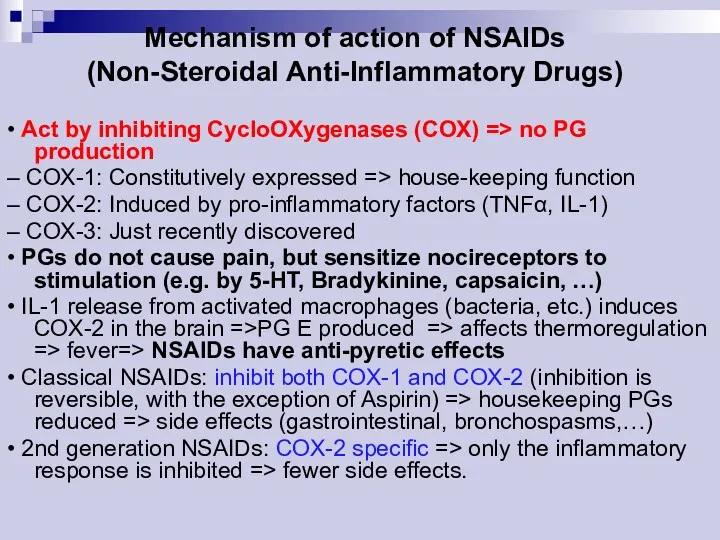
Mechanism of action of NSAIDs
(Non-Steroidal Anti-Inflammatory Drugs)
• Act by inhibiting CycloOXygenases
Mechanism of action of NSAIDs
(Non-Steroidal Anti-Inflammatory Drugs)
• Act by inhibiting CycloOXygenases
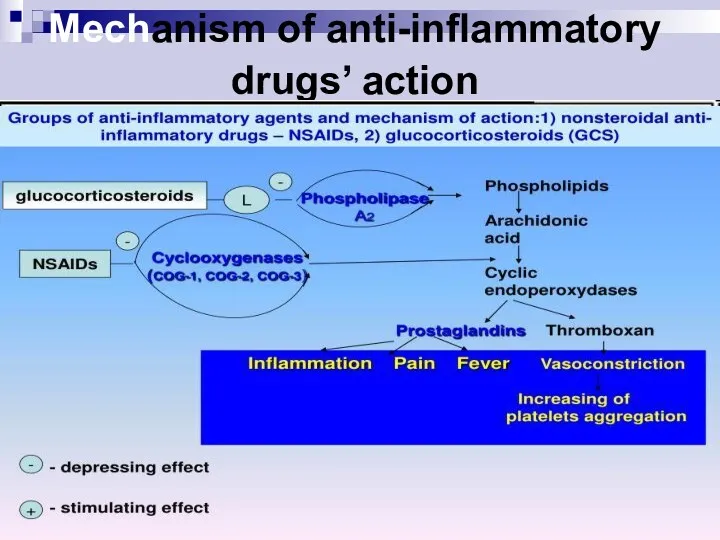
Mechanism of anti-inflammatory drugs’ action
Mechanism of anti-inflammatory drugs’ action
Pharmacological effects of NSAIDs
Anti-inflammatory
Analgesic
Antipyretic
Antiplatelet (Aspirin)
Closure of ductus arteriosus in newborn
Pharmacological effects of NSAIDs
Anti-inflammatory
Analgesic
Antipyretic
Antiplatelet (Aspirin)
Closure of ductus arteriosus in newborn
Clinical uses of NSAIDs
1. Pain: headache, toothache, myalgia, backpain;
2. Fever;
3. Arthritises:
Clinical uses of NSAIDs
1. Pain: headache, toothache, myalgia, backpain;
2. Fever;
3. Arthritises:
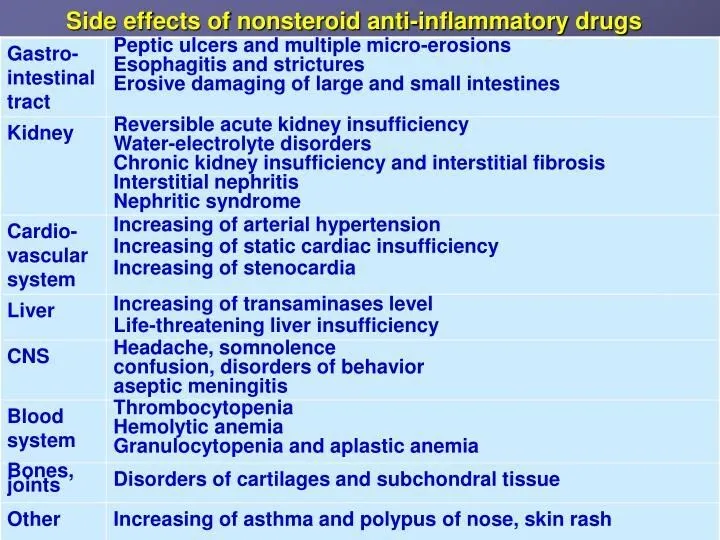
Side effects of NSAIDs
1. GIT disturbances: epigastric pain, nausea, gastric peptic
Side effects of NSAIDs
1. GIT disturbances: epigastric pain, nausea, gastric peptic
Contraindications
A) Pregnancy
B) Haemophilic patients
C) Hypersensitivity reactions
D) Viral infections mainly in
Contraindications
A) Pregnancy
B) Haemophilic patients
C) Hypersensitivity reactions
D) Viral infections mainly in
Drugs interaction
Potentiates the gastric irritant effect of alcohol
Potentiates the hypoglycaemic effects
Drugs interaction
Potentiates the gastric irritant effect of alcohol
Potentiates the hypoglycaemic effects
The Salicylates - ASPIRIN
Duration of action ~ 4 hr.
Orally taken.
Weak acid
The Salicylates - ASPIRIN
Duration of action ~ 4 hr.
Orally taken.
Weak acid

ASPIRIN - Therapeutic Uses
Antipyretic, analgesic.
Anti-inflammatory: rheumatic fever, rheumatoid arthritis (joint dis),
ASPIRIN - Therapeutic Uses
Antipyretic, analgesic.
Anti-inflammatory: rheumatic fever, rheumatoid arthritis (joint dis),
Propionic acid derivatives
IBUPROFEN:
Pharmacokinetics
Rapidly absorbed after oral ingestion.
Half-life 1-2 hours
Highly bound to
Propionic acid derivatives
IBUPROFEN:
Pharmacokinetics
Rapidly absorbed after oral ingestion.
Half-life 1-2 hours
Highly bound to
IBUPROFEN
The same mechanism & pharmacological actions of aspirin Except that it
IBUPROFEN
The same mechanism & pharmacological actions of aspirin Except that it
Clinical uses
A) Analgesic
B) Antipyretic
C) Anti-inflammatory
D)Acute gouty arthritis
E) Patent ductus arteriosus
Clinical uses
A) Analgesic
B) Antipyretic
C) Anti-inflammatory
D)Acute gouty arthritis
E) Patent ductus arteriosus
Preparations of Ibuprofen
Oral preparations.
Topical cream for osteoarthritis.
A liquid gel for rapid
Preparations of Ibuprofen
Oral preparations.
Topical cream for osteoarthritis.
A liquid gel for rapid
Adverse effects
1.Gastric upset (less frequent than aspirin).
2.Fluid retention
3.Hypersensetivity reactions
4.Ocular disturbances
5.Rare hematologic
Adverse effects
1.Gastric upset (less frequent than aspirin).
2.Fluid retention
3.Hypersensetivity reactions
4.Ocular disturbances
5.Rare hematologic
Contraindications
1. Peptic ulcer
2. Allergic patients to aspirin
3. Kidney impairment
4.Liver diseases
5.Pregnancy
6.Haemophilic patients
The
Contraindications
1. Peptic ulcer
2. Allergic patients to aspirin
3. Kidney impairment
4.Liver diseases
5.Pregnancy
6.Haemophilic patients
The
Piroxicam
Mechanism of actions:
A) Non-selective inhibitors to COX1 & COX2
B) Traps free
Piroxicam
Mechanism of actions:
A) Non-selective inhibitors to COX1 & COX2
B) Traps free

Pharmacokinetics
Well absorbed orally
Half- Life 45 hours
Given once daily
Pharmacokinetics
Well absorbed orally
Half- Life 45 hours
Given once daily
Adverse effects
Less frequent gastric upset (20%).
Dizziness.
Tinnitus.
Headache.
Allergy.
Adverse effects
Less frequent gastric upset (20%).
Dizziness.
Tinnitus.
Headache.
Allergy.

Acetic acid derivatives
DICLOFENAC
Mechanism of action
Non-selective inhibitor to COX1 & COX2.
More potent
Acetic acid derivatives
DICLOFENAC
Mechanism of action
Non-selective inhibitor to COX1 & COX2.
More potent
Clinical uses
DICLOFENAC
A) Any inflammatory conditions
B) Musculoskeletal pain
C) Dysmenorrhoea
D)Acute gouty arthritis
E) Fever
F)
Clinical uses
DICLOFENAC
A) Any inflammatory conditions
B) Musculoskeletal pain
C) Dysmenorrhoea
D)Acute gouty arthritis
E) Fever
F)
Adverse effects
DICLOFENAC
Gastric upset
Renal impairment
Elevation of serum aminotransferase
Salt & water retention
Adverse effects
DICLOFENAC
Gastric upset
Renal impairment
Elevation of serum aminotransferase
Salt & water retention
Preparations of DICLOFENAC
Diclofenac with misoprostol decreases upper gastrointestinal ulceration, but result
Preparations of DICLOFENAC
Diclofenac with misoprostol decreases upper gastrointestinal ulceration, but result
Selective COX 2 inhibitors
Advantages:
1. Highly selective inhibitors to COX2 enzyme.
2.
Selective COX 2 inhibitors
Advantages:
1. Highly selective inhibitors to COX2 enzyme.
2.
Selective Cox 2 inhibitors
5. Lower incidence of gastric upset.
6. No effect
Selective Cox 2 inhibitors
5. Lower incidence of gastric upset.
6. No effect
Selective Cox 2 inhibitors
9- They are recommended in postoperative patients undergoing
Selective Cox 2 inhibitors
9- They are recommended in postoperative patients undergoing
SAIDs – steroidal
anti-inflammatory drugs
SAIDs – steroidal
anti-inflammatory drugs
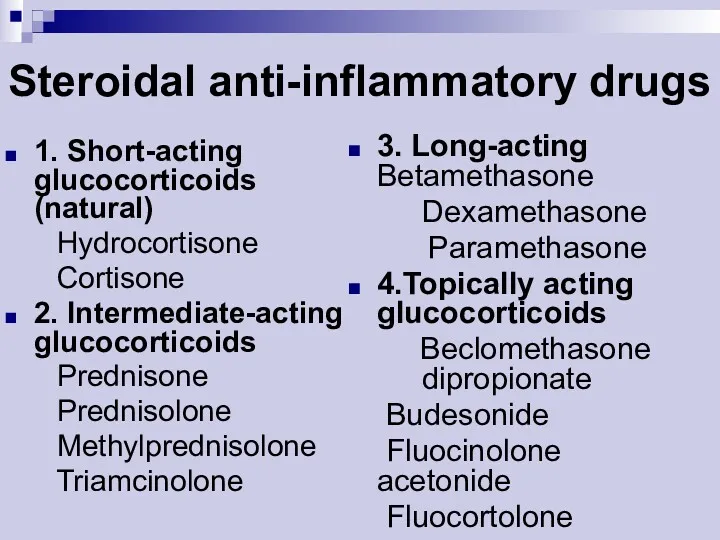
Steroidal anti-inflammatory drugs
1. Short-acting glucocorticoids (natural)
Hydrocortisone
Cortisone
2. Intermediate-acting glucocorticoids
Steroidal anti-inflammatory drugs
1. Short-acting glucocorticoids (natural)
Hydrocortisone
Cortisone
2. Intermediate-acting glucocorticoids
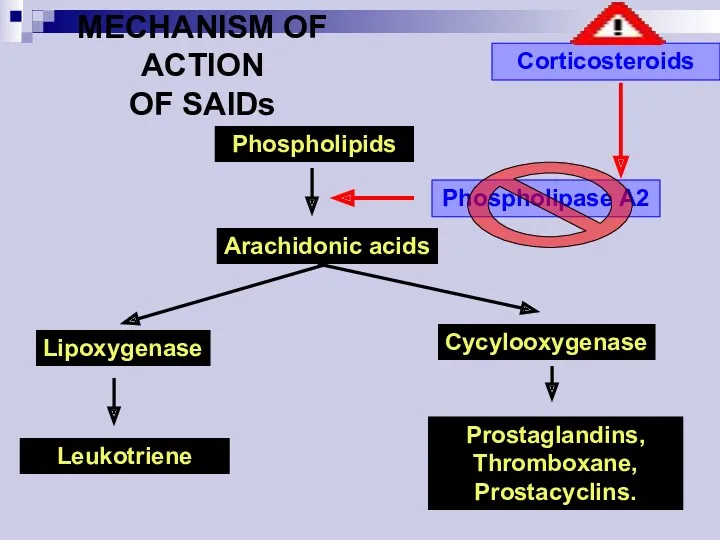
Phospholipids
Arachidonic acids
Lipoxygenase
Cycylooxygenase
Leukotriene
Prostaglandins,
Thromboxane,
Prostacyclins.
Phospholipase A2
Corticosteroids
MECHANISM OF ACTION
OF SAIDs
Phospholipids
Arachidonic acids
Lipoxygenase
Cycylooxygenase
Leukotriene
Prostaglandins,
Thromboxane,
Prostacyclins.
Phospholipase A2
Corticosteroids
MECHANISM OF ACTION
OF SAIDs
Clinical uses
of SAIDs
Adrenal insufficiency
Arthrities
Collagen diseases (systemic lupus erhymatosis, scleroderma)
Bronchial
Clinical uses
of SAIDs
Adrenal insufficiency
Arthrities
Collagen diseases (systemic lupus erhymatosis, scleroderma)
Bronchial
Main side effects of SAIDs
Susceptibility to infections
Delayed healing of wounds
Osteoporosis
Growth retardation
Main side effects of SAIDs
Susceptibility to infections
Delayed healing of wounds
Osteoporosis
Growth retardation

ANTI-ALLERGIC DRUGS
ANTI-ALLERGIC DRUGS
Allergy
An allergy is a hypersensitivity disorder of the immune system.
Allergic reactions
Allergy
An allergy is a hypersensitivity disorder of the immune system.
Allergic reactions
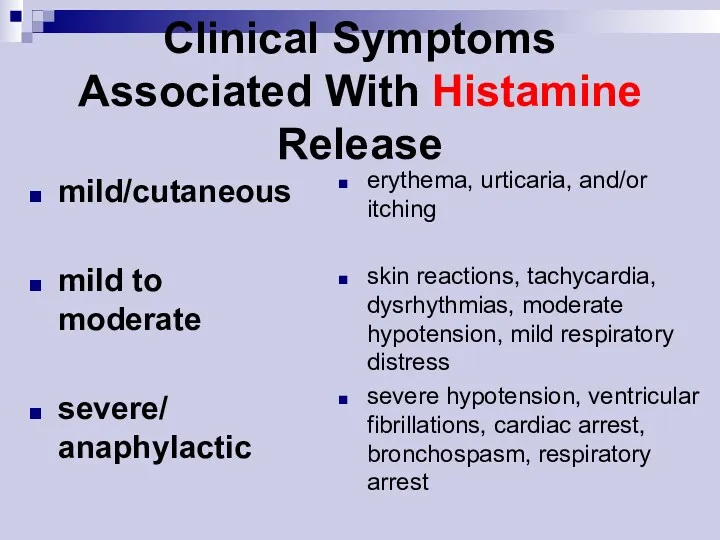
mild/cutaneous
mild to moderate
severe/
anaphylactic
erythema, urticaria, and/or itching
skin reactions, tachycardia, dysrhythmias, moderate
mild/cutaneous
mild to moderate
severe/
anaphylactic
erythema, urticaria, and/or itching
skin reactions, tachycardia, dysrhythmias, moderate
Histamine exerts its effects on many tissues and organs:
It is not
Histamine exerts its effects on many tissues and organs:
It is not
Pathophysiological Actions of Histamine
Cellular mediator of immediate hypersensitivity reaction and acute
Pathophysiological Actions of Histamine
Cellular mediator of immediate hypersensitivity reaction and acute
Pharmacological Effects of Histamine
Ranges from mild allergic symptoms to anaphylactic
Pharmacological Effects of Histamine
Ranges from mild allergic symptoms to anaphylactic
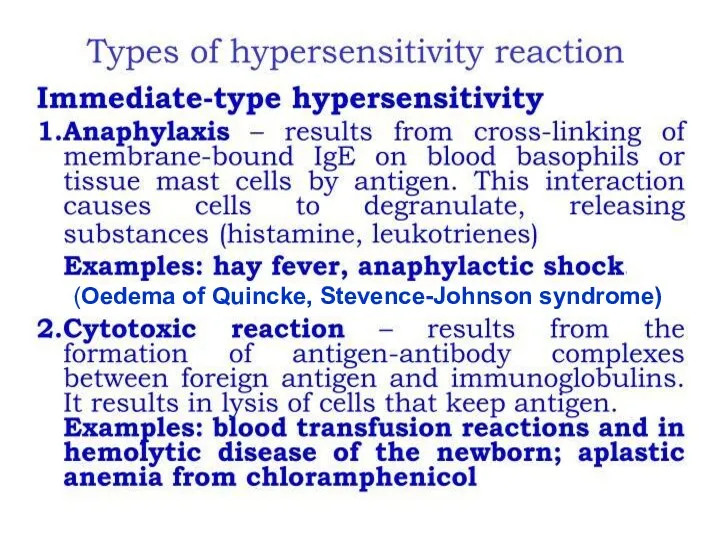
(Oedema of Quincke, Stevence-Johnson syndrome)
(Oedema of Quincke, Stevence-Johnson syndrome)

Antiallergic drugs
1. Antihistaminics
2. Corticosteroids
3. Mast cell stabilisers
4.Antileukotriene drugs
Antiallergic drugs
1. Antihistaminics
2. Corticosteroids
3. Mast cell stabilisers
4.Antileukotriene drugs
histaglobulin
histaglobulin
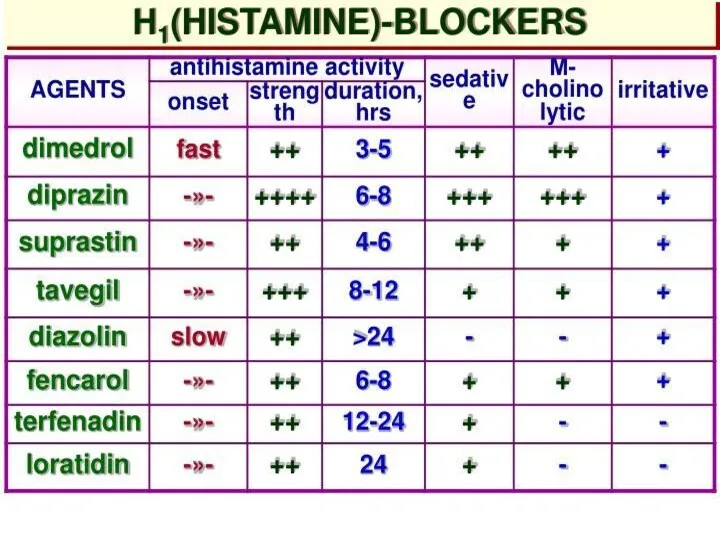
Histamine-related Drugs
Mast Cell Stabilizers (Cromolyn Na, Nedocromil –Tilade -, Albuterol)
H1 Receptor
Histamine-related Drugs
Mast Cell Stabilizers (Cromolyn Na, Nedocromil –Tilade -, Albuterol)
H1 Receptor
First Generation
ANTIHISTAMINE Agents
Ethanolamines: DIPHENHYDRAMINE (Benadryl) CLEMASTINE (Tavist)
Ethylenediamine:TRIPELENNAMINE
Alkylamine:CHLORPHENIRAMINE (Chlortrimeton)
Phenothiazine:PROMETHAZINE (Phenergan)
Piperazines:
First Generation
ANTIHISTAMINE Agents
Ethanolamines: DIPHENHYDRAMINE (Benadryl) CLEMASTINE (Tavist)
Ethylenediamine:TRIPELENNAMINE
Alkylamine:CHLORPHENIRAMINE (Chlortrimeton)
Phenothiazine:PROMETHAZINE (Phenergan)
Piperazines:
Uses:
Adjunctive in anaphylaxis and other cases where histamine release can occur
Uses:
Adjunctive in anaphylaxis and other cases where histamine release can occur
First Generation Agents
Adverse Effects:
Sedation (Paradoxical Excitation in children)
Dizziness
Fatigue
Tachydysrhythmias in overdose -
First Generation Agents
Adverse Effects:
Sedation (Paradoxical Excitation in children)
Dizziness
Fatigue
Tachydysrhythmias in overdose -
Drug interactions:
Additive with classical antimuscarinics
Potentiate CNS depressants
opioids
sedatives
general and narcotic analgesics
alcohol
First Generation
Drug interactions:
Additive with classical antimuscarinics
Potentiate CNS depressants
opioids
sedatives
general and narcotic analgesics
alcohol
First Generation
Uses
Antiallergy
Examples
CETIRIZINE (ZYRTEC)
FEXOFENADINE (ALLEGRA)
LORATADINE (CLARITIN)
DESLORATADINE (CLARINEX- FDA APPROVED IN 2002)
LORATADINE (CLARITIN
Uses
Antiallergy
Examples
CETIRIZINE (ZYRTEC)
FEXOFENADINE (ALLEGRA)
LORATADINE (CLARITIN)
DESLORATADINE (CLARINEX- FDA APPROVED IN 2002)
LORATADINE (CLARITIN
Histamine H1- Antagonists
First Generation:
!!!Sedating!!!
Second Generation:
!!!Non sedating!!!
Histamine H1- Antagonists
First Generation:
!!!Sedating!!!
Second Generation:
!!!Non sedating!!!
Advantages of 2nd generation antihistaminics
Higher H1 selectivity, absence of anticholinergic
Advantages of 2nd generation antihistaminics
Higher H1 selectivity, absence of anticholinergic
Mast cell stabilisers
Cromolyn sodium (Sodium cromoglycate)
Nedocromil sodium
Ketotifen
Corticosteroids (vide
Mast cell stabilisers
Cromolyn sodium (Sodium cromoglycate)
Nedocromil sodium
Ketotifen
Corticosteroids (vide
Antileukotriene drugs
Montelukast
Zafirlukast
Mechanism: competitive block of LT1 receptors
Clinical use: bronchial asthma
Antileukotriene drugs
Montelukast
Zafirlukast
Mechanism: competitive block of LT1 receptors
Clinical use: bronchial asthma

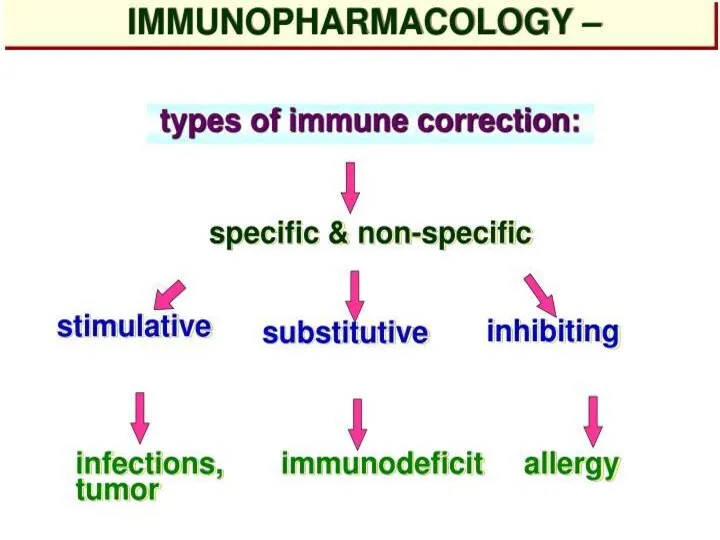
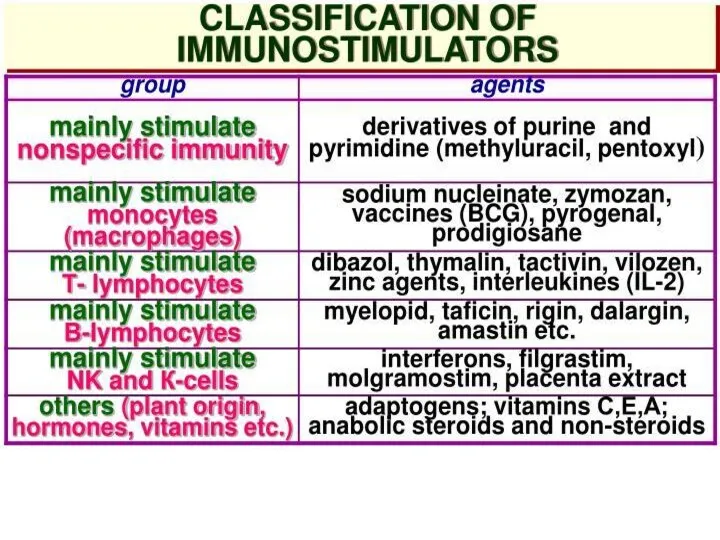
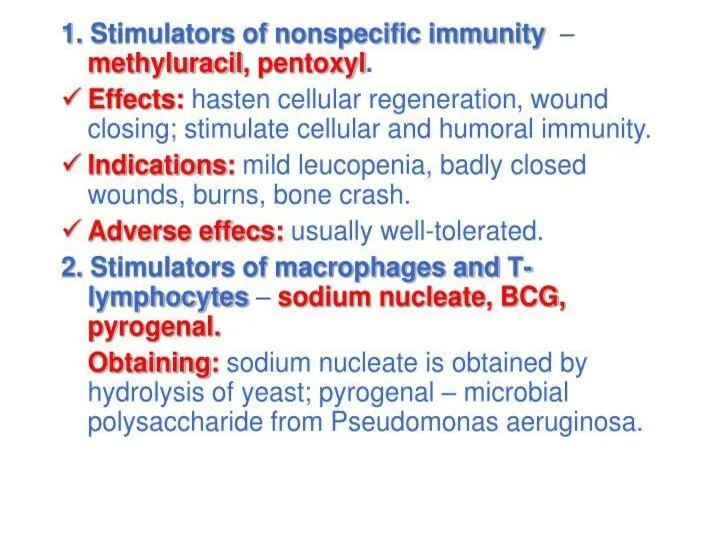
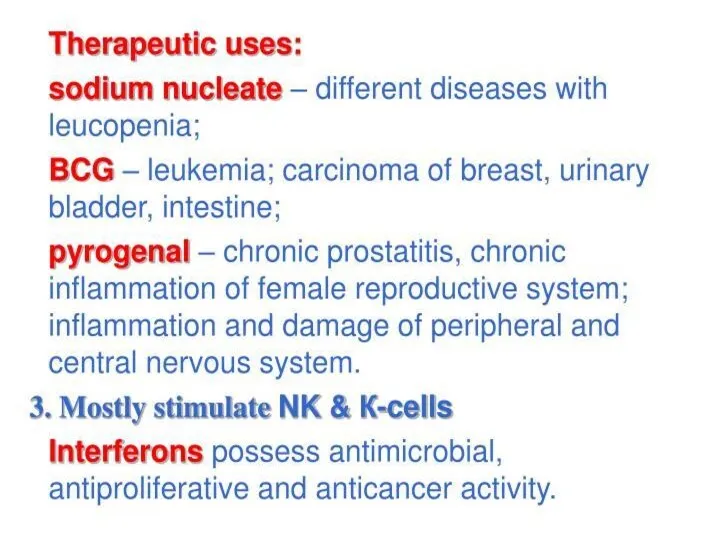
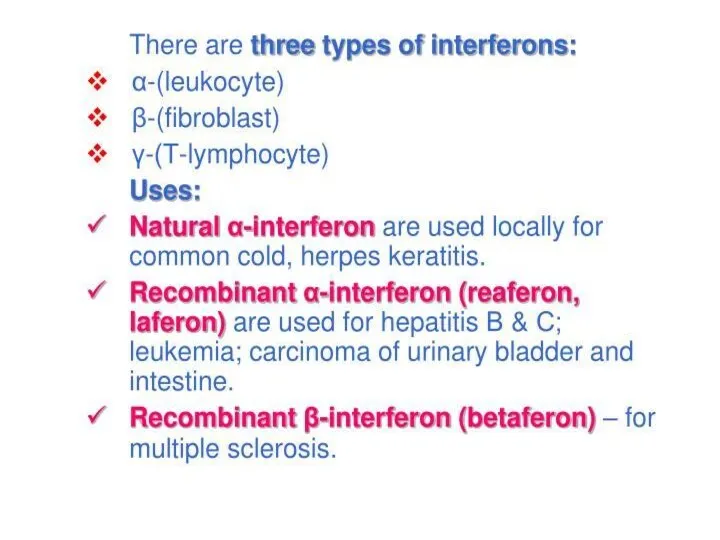
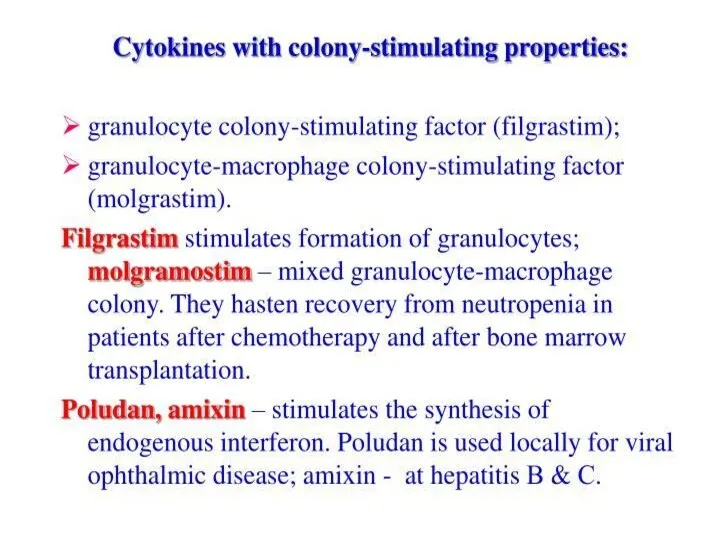
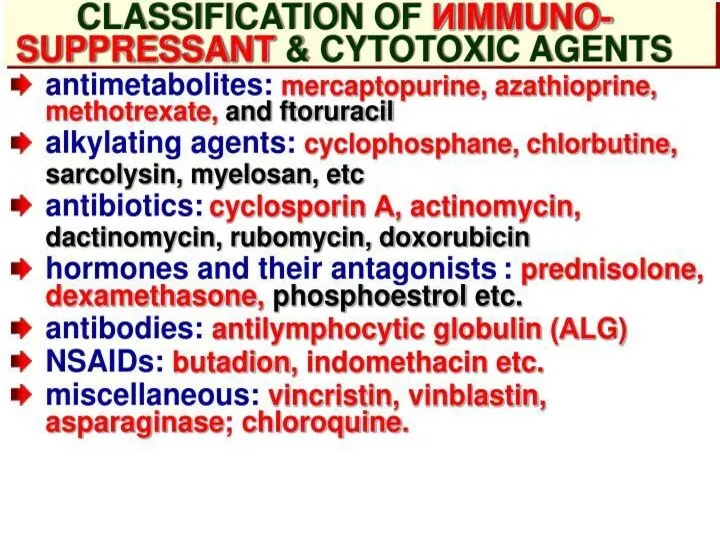
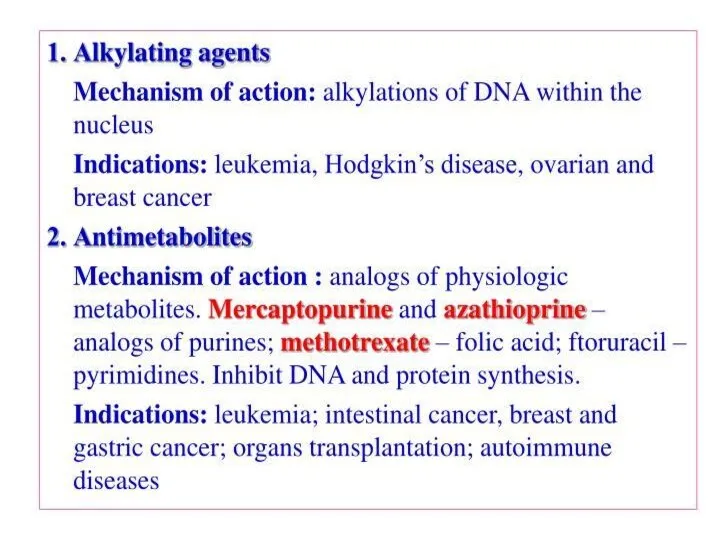
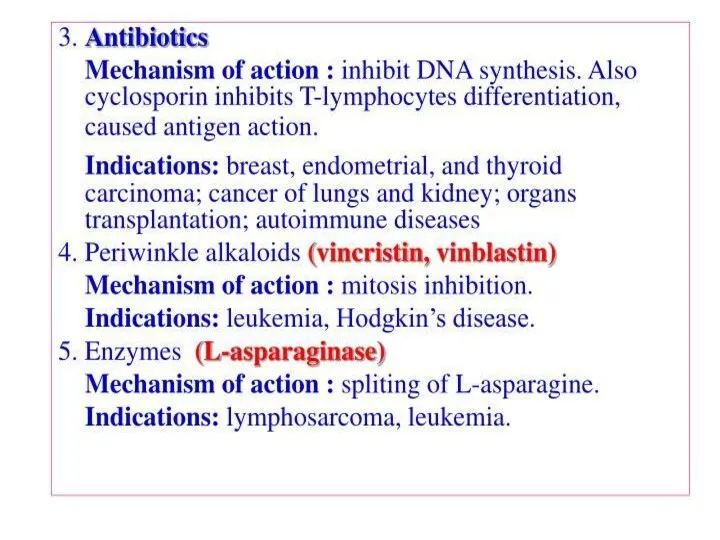
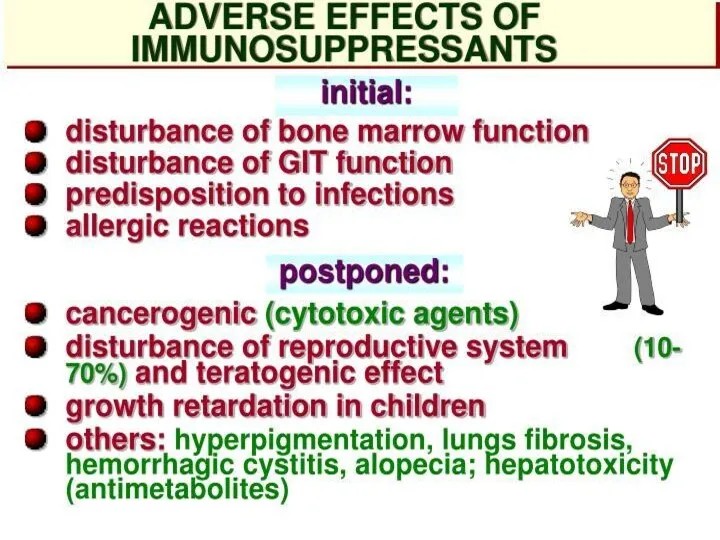
Immunomodulators
Immunomodulators
 Гигиенические требования к инфекционным стационарам
Гигиенические требования к инфекционным стационарам Гигиенические требования к качеству и безопасности пищевых продуктов
Гигиенические требования к качеству и безопасности пищевых продуктов История развития ветеринарно - санитарной экспертизы
История развития ветеринарно - санитарной экспертизы Препарат ритуксимаб
Препарат ритуксимаб Патологичес кая анатомия
Патологичес кая анатомия Энцефалиты. Классификация
Энцефалиты. Классификация Принципы межличностного общения и консультирования пациентов врачом общей практики
Принципы межличностного общения и консультирования пациентов врачом общей практики Вторичные иммунодефициты
Вторичные иммунодефициты Клиническая психология. Патопсихология. (Лекция 3)
Клиническая психология. Патопсихология. (Лекция 3) Ревматоидный артрит
Ревматоидный артрит Варикозная болезнь нижних конечностей. Хроническая венозная недостаточность
Варикозная болезнь нижних конечностей. Хроническая венозная недостаточность Повреждения и травмы
Повреждения и травмы Физикалық ластанудың қоршаған ортаға әсері және радиоактивні қалдықтармен ластануы
Физикалық ластанудың қоршаған ортаға әсері және радиоактивні қалдықтармен ластануы Ерте жастағы қауіп тобындағы балаларды ПМСП жағдайында бақылаудың дифференцирленген бақылау тактикасы
Ерте жастағы қауіп тобындағы балаларды ПМСП жағдайында бақылаудың дифференцирленген бақылау тактикасы Туберкулез и пневмокониоз
Туберкулез и пневмокониоз Патофизиология сердца. Сердечная недостаточность
Патофизиология сердца. Сердечная недостаточность Ўзбекистон Республикасида вирусли гепатитларнинг ташхисоти, давоси ва профилактикаси бўйича чора
Ўзбекистон Республикасида вирусли гепатитларнинг ташхисоти, давоси ва профилактикаси бўйича чора Здоровый образ жизни. (Тема 1.13)
Здоровый образ жизни. (Тема 1.13) Снотворные, противопаркинсонические, противоэпилептические средства
Снотворные, противопаркинсонические, противоэпилептические средства Эндокринная система
Эндокринная система Повреждение нижних конечностей
Повреждение нижних конечностей Геморрагическая лихорадка с почечным синдромом
Геморрагическая лихорадка с почечным синдромом Жүре пайда болған иммундық дефицитінің синдромы туралы. ЖИТС жұғу жолдары. ЖИТС негізгі белгілері. ЖИТС алдын алу шаралары
Жүре пайда болған иммундық дефицитінің синдромы туралы. ЖИТС жұғу жолдары. ЖИТС негізгі белгілері. ЖИТС алдын алу шаралары Периодонтит у детей
Периодонтит у детей Dysgraphia
Dysgraphia Вакцинопрофилактика в гинекологии
Вакцинопрофилактика в гинекологии Нейропластичность и нейродегенерация
Нейропластичность и нейродегенерация Профилактика воздушно-капельных инфекций
Профилактика воздушно-капельных инфекций