- Aortic Insufficiency

Содержание
- 2. Classification -1 Abnormalities of the Leaflets Rheumatic, Bicuspid, Degenerative Endocarditis Dilation of the Aortic Annulus Aortic
- 3. Classification -2
- 4. Chronic AI - Pathophysiology increased LV EDV addition of new sarcomeres in series/ elongation of myocytes
- 5. Pressure Volume Relationships in Chronic AI Braunwald 6th ed CO at rest may approach 25 L/min
- 6. History DOE, Orthopnea, PND usually after 4th / 5th decade and significant cardiomegaly and LV dysfx
- 7. Physical Findings Diastolic murmur high frequency, sitting up, leaning forward duration > intensity correlates with severity
- 8. Peripheral Signs of Severe Aortic Regurgitation Quincke’s sign: capillary pulsation Corrigan’s sign: water hammer pulse Bisferiens
- 9. CXR
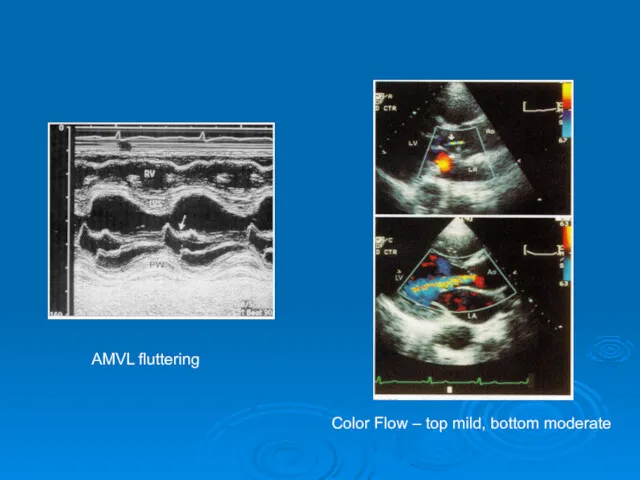
- 10. ECHO 2D/ M-Mode AV/ Ao Root anatomic abnormalities LV dimension / sphericity AMVL – fluttering, reverse
- 11. AMVL fluttering Color Flow – top mild, bottom moderate
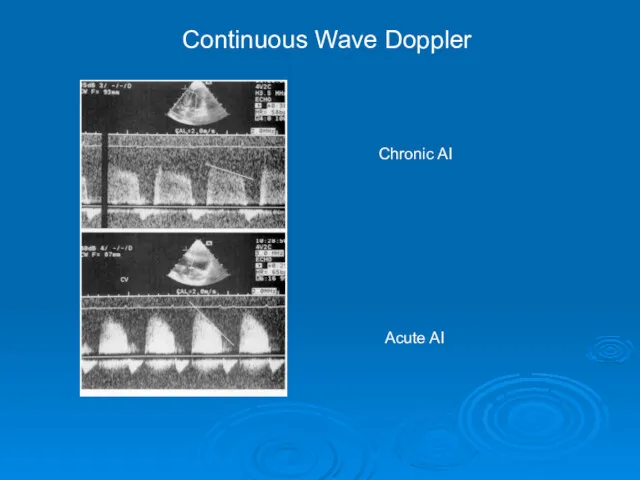
- 12. Chronic AI Acute AI Continuous Wave Doppler
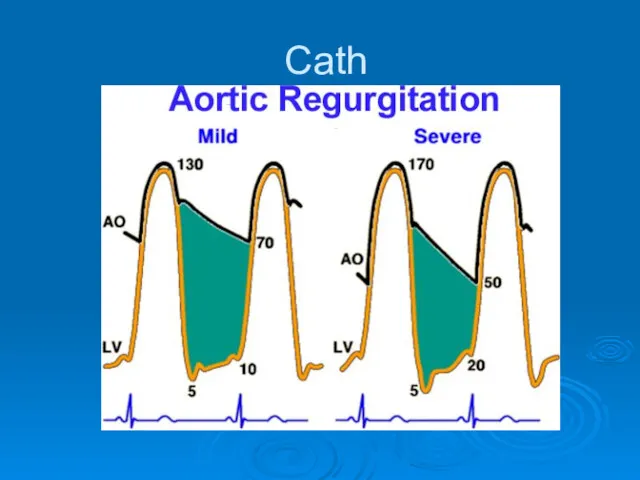
- 13. Cath
- 14. Medical Management Vasodilators goal is to reduce SBP, improve forward SV, reduce regurgitant volume Uses severe
- 15. Timing of Surgery Goal is to intervene before irreversible LV systolic dysfx ensues initially reversible, mainly
- 16. Surgical Therapy Indications for AVR (Severe AR)1 Symptoms (NYHA III-IV) regardless of LV fxn Symptoms (NYHA
- 20. Aortic Valve Replacement
- 21. Surgical Options Ao Root disease annuloplasty or other valve sparing surgery possible if pure Ao Root
- 22. Figure 46-42 Repair of the aortic valve in patient with severe AR. Conduit tailoring in the
- 23. Rx of Acute AI Treat cause of acute AI Dissection/Trauma Endocarditis Prosthesis malfunction ? Urgent AVR
- 25. Скачать презентацию
Classification -1
Abnormalities of the Leaflets
Rheumatic, Bicuspid, Degenerative
Endocarditis
Dilation of the Aortic Annulus
Aortic
Classification -1
Abnormalities of the Leaflets
Rheumatic, Bicuspid, Degenerative
Endocarditis
Dilation of the Aortic Annulus
Aortic
Classification -2
Classification -2

Chronic AI - Pathophysiology
increased LV EDV
addition of new sarcomeres
Chronic AI - Pathophysiology
increased LV EDV
addition of new sarcomeres
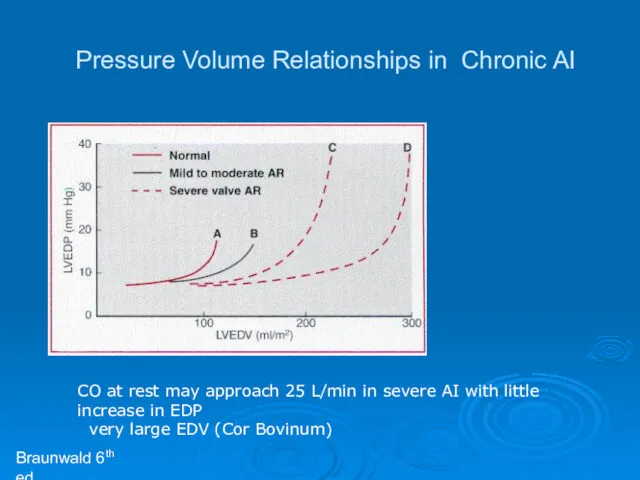
Pressure Volume Relationships in Chronic AI
Braunwald 6th ed
CO at rest may
Pressure Volume Relationships in Chronic AI
Braunwald 6th ed
CO at rest may
History
DOE, Orthopnea, PND
usually after 4th / 5th decade and significant cardiomegaly
History
DOE, Orthopnea, PND
usually after 4th / 5th decade and significant cardiomegaly
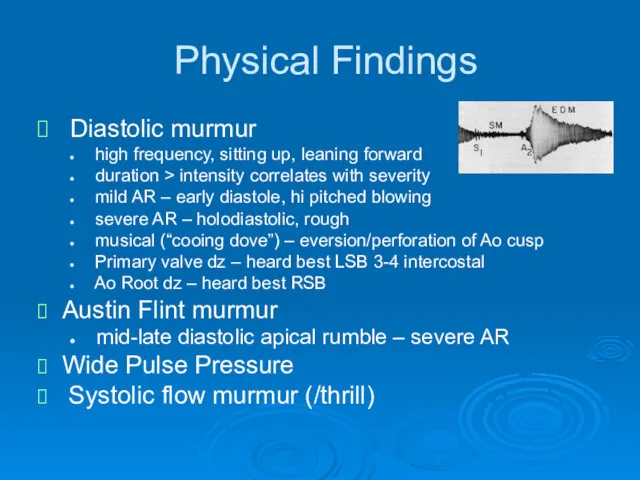
Physical Findings
Diastolic murmur
high frequency, sitting up, leaning forward
duration
Physical Findings
Diastolic murmur
high frequency, sitting up, leaning forward
duration
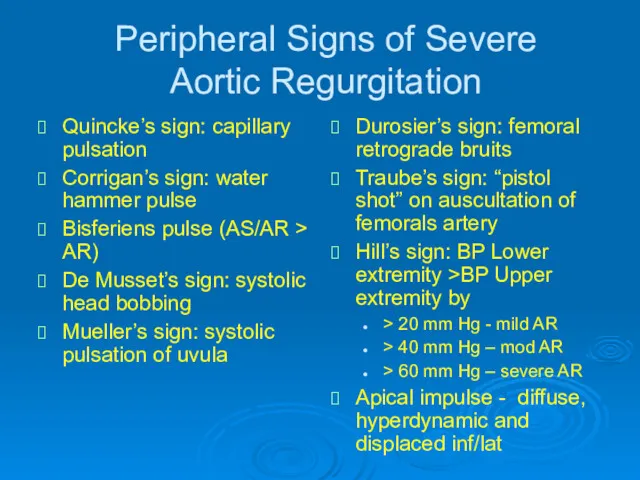
Peripheral Signs of Severe
Aortic Regurgitation
Quincke’s sign: capillary pulsation
Corrigan’s sign: water
Peripheral Signs of Severe
Aortic Regurgitation
Quincke’s sign: capillary pulsation
Corrigan’s sign: water
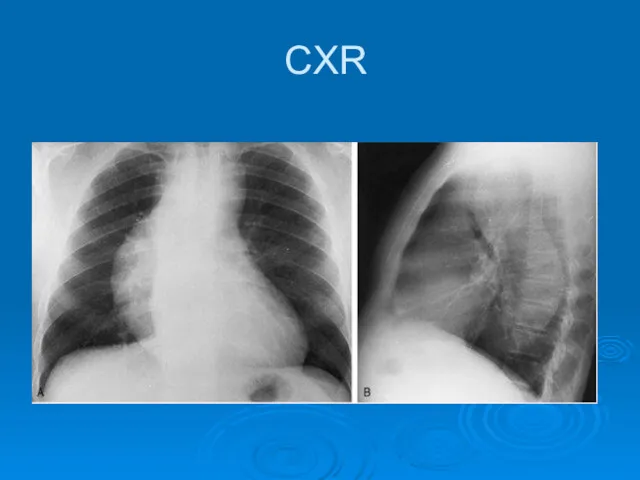
CXR
CXR
ECHO
2D/ M-Mode
AV/ Ao Root anatomic abnormalities
LV dimension /
ECHO
2D/ M-Mode
AV/ Ao Root anatomic abnormalities
LV dimension /
AMVL fluttering
Color Flow – top mild, bottom moderate
AMVL fluttering
Color Flow – top mild, bottom moderate
Chronic AI
Acute AI
Continuous Wave Doppler
Chronic AI
Acute AI
Continuous Wave Doppler
Cath
Cath
Medical Management
Vasodilators
goal is to reduce SBP, improve forward SV,
Medical Management
Vasodilators
goal is to reduce SBP, improve forward SV,
Timing of Surgery
Goal is to intervene before irreversible LV systolic
Timing of Surgery
Goal is to intervene before irreversible LV systolic
Surgical Therapy
Indications for AVR (Severe AR)1
Symptoms (NYHA III-IV) regardless
Surgical Therapy
Indications for AVR (Severe AR)1
Symptoms (NYHA III-IV) regardless

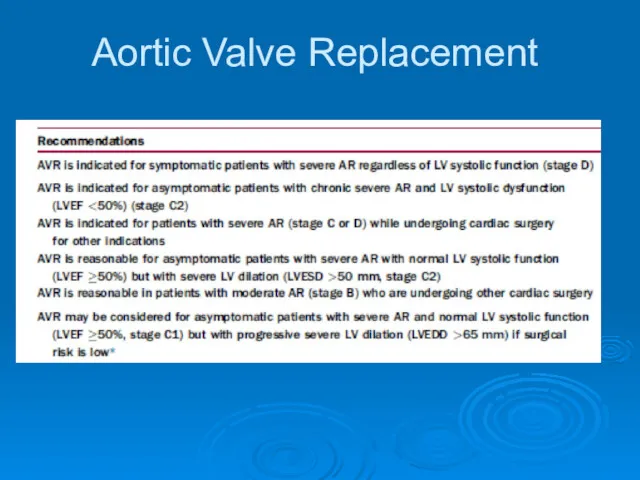
Aortic Valve Replacement
Aortic Valve Replacement
Surgical Options
Ao Root disease
annuloplasty or other valve sparing surgery
Surgical Options
Ao Root disease
annuloplasty or other valve sparing surgery
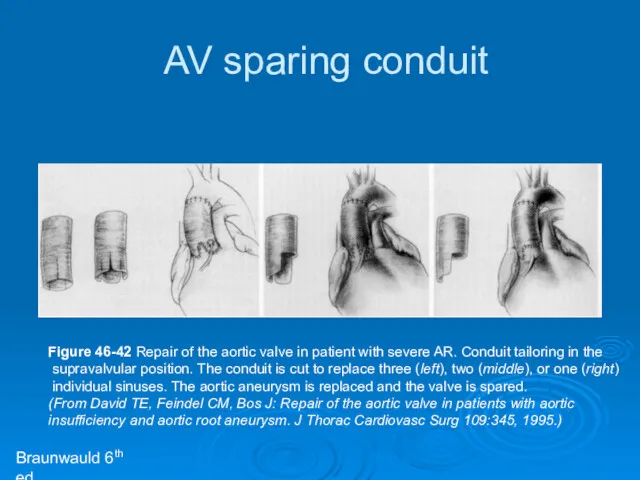
Figure 46-42 Repair of the aortic valve in patient with severe
Figure 46-42 Repair of the aortic valve in patient with severe
Rx of Acute AI
Treat cause of acute AI
Dissection/Trauma
Endocarditis
Prosthesis malfunction
? Urgent AVR
Rx of Acute AI
Treat cause of acute AI
Dissection/Trauma
Endocarditis
Prosthesis malfunction
? Urgent AVR
 Клинический случай. Диарейный синдром
Клинический случай. Диарейный синдром Диагностика вирусных инфекций
Диагностика вирусных инфекций Менінгококова інфекція
Менінгококова інфекція Туберкулез внутригрудных лимфатических узлов
Туберкулез внутригрудных лимфатических узлов Дифференциальная диагностика менингеального синдрома
Дифференциальная диагностика менингеального синдрома Тромбоемболія легеневої артерії (ТЕЛА)
Тромбоемболія легеневої артерії (ТЕЛА) Первая медицинская помощь при острых отравлениях
Первая медицинская помощь при острых отравлениях Балалардағы бет – жақ аймағындағы ауытқуларды емдеуде миогимнастикасы
Балалардағы бет – жақ аймағындағы ауытқуларды емдеуде миогимнастикасы Профилактика инсультов у пациентов с фибрилляцией предсердий
Профилактика инсультов у пациентов с фибрилляцией предсердий Регуляция иммунного ответа. Цитокины, факторы роста, гормоны. (Лекция 4)
Регуляция иммунного ответа. Цитокины, факторы роста, гормоны. (Лекция 4) Стоматологическое материаловедение
Стоматологическое материаловедение Синдромы функциональной несформированности, дефицитарности отделов головного мозга
Синдромы функциональной несформированности, дефицитарности отделов головного мозга Злокачественные опухоли и их профилактика
Злокачественные опухоли и их профилактика Инсулинотерапия при СД 2 типа
Инсулинотерапия при СД 2 типа Болезнь Дюринга (герпетифорный дерматит), многоформной экссудативной эритеме, синдроме Стивенса-Джонсона
Болезнь Дюринга (герпетифорный дерматит), многоформной экссудативной эритеме, синдроме Стивенса-Джонсона Организационные вопросы онкологической помощи в Российской Федерации
Организационные вопросы онкологической помощи в Российской Федерации Жоғарғы жүйке жүйесі бұзылыстарының балалардағы ерекшеліктері
Жоғарғы жүйке жүйесі бұзылыстарының балалардағы ерекшеліктері Методы лучевой диагностики
Методы лучевой диагностики Туберкулез. Микобактериозы
Туберкулез. Микобактериозы Активное ведение третьего периода родов
Активное ведение третьего периода родов Многоплодная беременность при экстракорпоральном оплодотворении
Многоплодная беременность при экстракорпоральном оплодотворении Болезнь Вакеза. Эритремия: критерии диагноза, этиология, патогенез, клиника, лечение
Болезнь Вакеза. Эритремия: критерии диагноза, этиология, патогенез, клиника, лечение Виписування, зберігання та застосування ліків
Виписування, зберігання та застосування ліків Этика и деонтология в педиатрии. Периоды детского возраста. Особенности ухода за детьми различного возраста
Этика и деонтология в педиатрии. Периоды детского возраста. Особенности ухода за детьми различного возраста Инфаркт миокарда. Роль медицинской сестры в лечении и профилактике
Инфаркт миокарда. Роль медицинской сестры в лечении и профилактике Адгезивті және алмалы көпіртәрізді протездермен, протездеу
Адгезивті және алмалы көпіртәрізді протездермен, протездеу БАБЖ бағдарламасы. Жөтел нмесе тыныс алудың қиындауы бар науқастарды жұргізу тәсілі
БАБЖ бағдарламасы. Жөтел нмесе тыныс алудың қиындауы бар науқастарды жұргізу тәсілі ЗОЖ (2). Развитие способностей. Задание на лето
ЗОЖ (2). Развитие способностей. Задание на лето