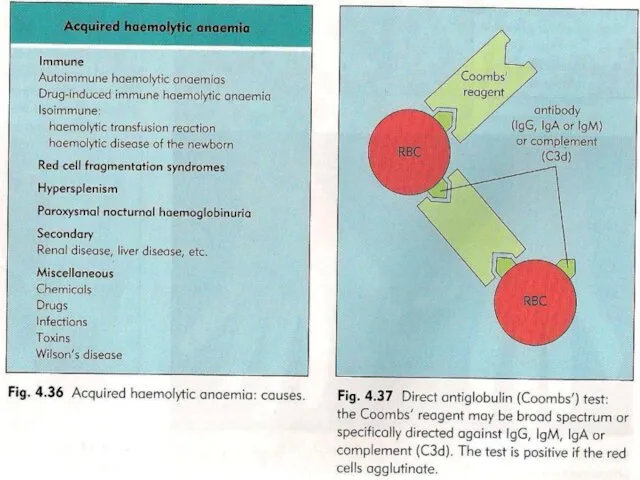
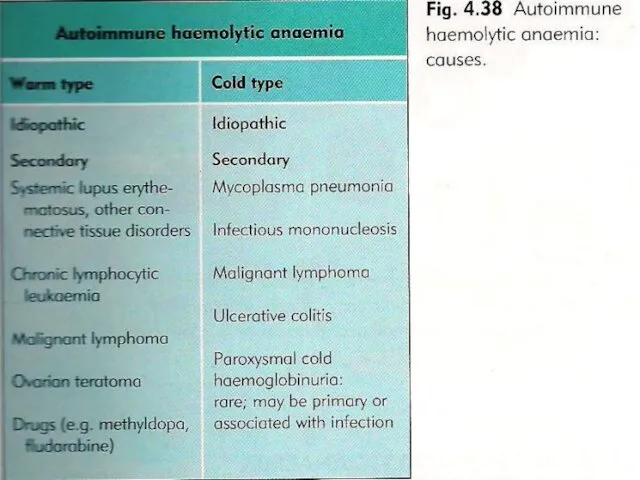
- Autoimmune hemolytic anemia

Содержание
- 4. EPIDEMIOLOGY Incidence: 10:1000000 population Women>men Usually midlife, can occur at any age 50% idiopathic Can be
- 5. CLINICAL FINDINGS Jaundice, usually mild Signs and symptoms of anemia – acute or chronic 30% splenomegaly
- 6. LABORATORY EVALUATION Anemia with enhanced erythropoesis Reticulocytosis Blood smear: spherocytes, occasional fragments, nucleated RBC Bone marrow
- 7. LABORATORY EVALUATION Unconjugated bilirubinemia, increased LDH, low haptoglobin Intravascular hemolysis – free Hb in plasma, hemosiderin
- 9. TREATMENT Transfusion, if severe symptomatic anemia, with steroids, close follow up and monitoring Corticosteroids – prednisone
- 10. COLD AGGLUTININ DISEASE Antibodies that bind RBC at cold temperature (5-18°C), usually IgM Chronic – idiopathic
- 11. THERAPY Warming, warmed blood transfusion Prednisone, splenectomy - mostly non beneficial Plasma exchange - temporal relief
- 13. Скачать презентацию
EPIDEMIOLOGY
Incidence: 10:1000000 population
Women>men
Usually midlife, can occur at any age
50% idiopathic
Can be
EPIDEMIOLOGY
Incidence: 10:1000000 population
Women>men
Usually midlife, can occur at any age
50% idiopathic
Can be
CLINICAL FINDINGS
Jaundice, usually mild
Signs and symptoms of anemia – acute or
CLINICAL FINDINGS
Jaundice, usually mild
Signs and symptoms of anemia – acute or
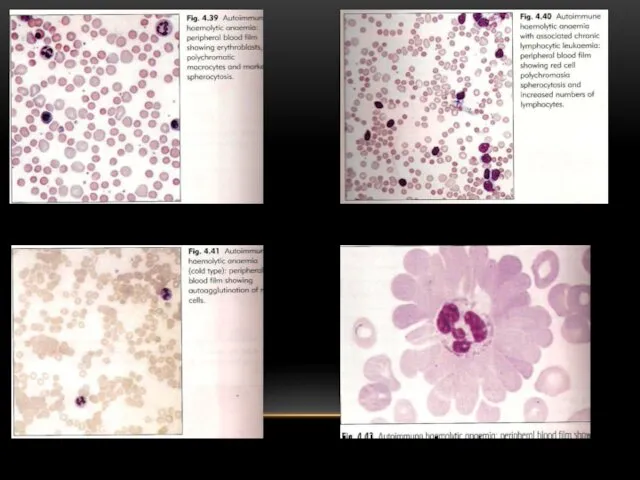
LABORATORY EVALUATION
Anemia with enhanced erythropoesis
Reticulocytosis
Blood smear: spherocytes, occasional fragments, nucleated RBC
Bone
LABORATORY EVALUATION
Anemia with enhanced erythropoesis
Reticulocytosis
Blood smear: spherocytes, occasional fragments, nucleated RBC
Bone
LABORATORY EVALUATION
Unconjugated bilirubinemia, increased LDH, low haptoglobin
Intravascular hemolysis – free Hb
LABORATORY EVALUATION
Unconjugated bilirubinemia, increased LDH, low haptoglobin
Intravascular hemolysis – free Hb
TREATMENT
Transfusion, if severe symptomatic anemia, with steroids, close follow up and
TREATMENT
Transfusion, if severe symptomatic anemia, with steroids, close follow up and
COLD AGGLUTININ DISEASE
Antibodies that bind RBC at cold temperature (5-18°C), usually
COLD AGGLUTININ DISEASE
Antibodies that bind RBC at cold temperature (5-18°C), usually
THERAPY
Warming, warmed blood transfusion
Prednisone, splenectomy - mostly non beneficial
Plasma exchange
THERAPY
Warming, warmed blood transfusion
Prednisone, splenectomy - mostly non beneficial
Plasma exchange
 Современная концепция естественного вскармливания
Современная концепция естественного вскармливания Deontology. Introduction
Deontology. Introduction Фармакология витамина Е
Фармакология витамина Е Разбор клинического случая. Демонстрация пациента
Разбор клинического случая. Демонстрация пациента Рак лёгкого
Рак лёгкого Тағамдық аллергия
Тағамдық аллергия Сестринская помощь пациентам с впервые выявленной бронхиальной астмой
Сестринская помощь пациентам с впервые выявленной бронхиальной астмой Онкогенні папіломавіруси
Онкогенні папіломавіруси Тістердің бұзылуы және олардың жоғалту кезіндегі морфологиялық және функционалды өзгерістер
Тістердің бұзылуы және олардың жоғалту кезіндегі морфологиялық және функционалды өзгерістер Нарушения ритма сердца. Синдром нарушения ритма
Нарушения ритма сердца. Синдром нарушения ритма Tratamentul Diabetului zaharat 2
Tratamentul Diabetului zaharat 2 Розацеа. Этиология и патогенез
Розацеа. Этиология и патогенез Энтеробактерии. Эшерихии
Энтеробактерии. Эшерихии Лечение опухолей толстого кишечника: лучевая и химиотерапия
Лечение опухолей толстого кишечника: лучевая и химиотерапия Лечебная физкультура при инфаркте миокарда
Лечебная физкультура при инфаркте миокарда Проводящие пути центральной нервной системы
Проводящие пути центральной нервной системы Факторы иммунитета. Новый мир COVID-19. Инфекции и прививки
Факторы иммунитета. Новый мир COVID-19. Инфекции и прививки Патофизиология эндокринной системы
Патофизиология эндокринной системы Целиакия у детей. Дифференциальный диагноз
Целиакия у детей. Дифференциальный диагноз Вирус бешенства
Вирус бешенства Лазеры в хирургии
Лазеры в хирургии Неотложная радиология в урологии. Почечная колика
Неотложная радиология в урологии. Почечная колика Протиста (только жгутиковые)
Протиста (только жгутиковые) Акне (Угри)
Акне (Угри) Фиброз и цирроз печени. Гемахроматоз. Болезнь Вильсона
Фиброз и цирроз печени. Гемахроматоз. Болезнь Вильсона Методы диагностики микобактерий туберкулеза
Методы диагностики микобактерий туберкулеза Чорна смерть. Чума
Чорна смерть. Чума Хронический панкреатит. Диагностика и лечение
Хронический панкреатит. Диагностика и лечение