- Biological Therapy in Psychiatry

Содержание
- 2. Biological Therapy in Psychiatry Anatoly Kreinin MD, PhD Director of Psychiatric Department, Tirat Carmel Mental Health
- 3. Mental Health Care Pre-1930’s
- 4. Before we begin… “It should be made clear that all psychotropic drugs can be safe or
- 5. What is a ‘drug’? A very vague term all ingested substances alter bodily function ‘drug’ is
- 6. HISTORY OF ANTIPSYCHOTICS Anti-psychotics were discovered accidentally by a French naval surgeon, Henri Laborit. Laborit was
- 7. Treatment Before Drugs Came into Play King Saul – vine, music-therapy Patients were kept isolated from
- 9. Efficacy and Potency Efficacy - Ability of a drug to produce a response as a result
- 10. Drug Toxicity Toxicity: Point at which concentrations of the drug in the blood stream become harmful
- 11. Absorption From site of administration into the plasma Oral - (tablet and liquid) (Table 8-3) Most
- 12. Pharmacokinetics: How the Body Acts on the Drug Absorption Distribution Metabolism Elimination
- 13. Bioavailability Amount of drug that reaches systemic circulation unchanged Often used to compare one drug to
- 14. Distribution Amount of drug found in various tissues, especially the intended ones. Psychiatric drugs must pass
- 15. Crossing the Blood Brain Barrier Passive diffusion Drug must dissolve in the structure of the cell
- 16. Metabolism Process by which the drug is altered and broken down into smaller substances (metabolites) that
- 17. Elimination Clearance: Total amount of blood, serum, or plasma from which a drug is completely removed
- 18. Dosing and Steady State Dosing: Administration of medication over time, so that therapeutic levels can be
- 19. Pharmacokinetics: Cultural Considerations 9% of whites - genetically defective P-4502D6 Asian descent Metabolize ethanol to produce
- 20. Phases of Drug Treatment Initiation Stabilization Maintenance Discontinuation
- 21. Tolerance & Dependence Tolerance – state of decreased sensitivity to the drug as a result of
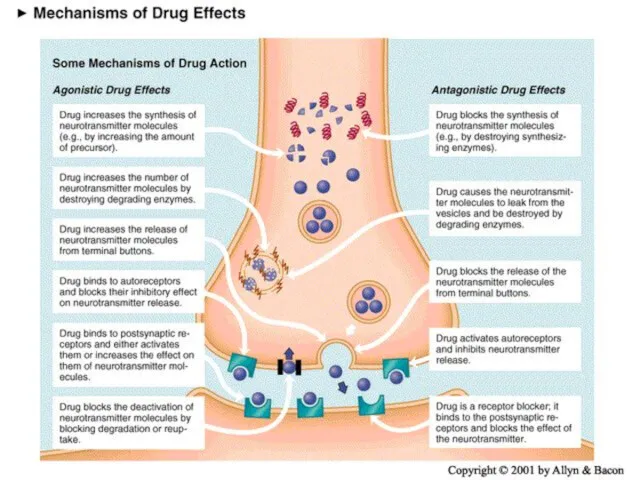
- 22. Receptors Types of Action Agonist: same biologic action Antagonist: opposite effect Interactions with a receptor Selectivity:
- 23. Ion Channels Drugs can block or open the ion channels Example: benzodiazepine drugs facilitate GABA in
- 24. Enzymes Enzymes catalyze specific biochemical reactions within cells and are targets for some drugs. Monoamine oxidase
- 25. Carrier Proteins Transport neurotransmitters across cell membranes Medications may block or inhibit this transport. Example: antidepressants
- 26. Being a neurotransmitter: What does it take? Exists presynaptically Synthesis enzymes exist presynaptically Released in response
- 27. Neurotransmitters 80 plus chemical substances that provide communication between cells. Some of these are actually NTs
- 28. All psychoactive drugs act centrally (i.e. on the brain) The vast majority of drug actions are
- 29. Neurotransmitters have 7 actions Synthesized Stored Enzymatically destroyed if not stored Exocytosis Termination of release via
- 30. A quick review of synaptic action receptor types (ionotropic and metabotropic) receptor subtypes
- 31. Metabotropic receptor Includes the metabotropic glutamate receptors, muscarinic acetylcholine receptors, GABAB receptors, and most serotonin receptors,
- 32. Since opening channels by metabotropic receptors involves activating a number of molecules in turn, channels associated
- 33. The classical neurotransmitters Amines Monoamines catecholamines (dopamine, noradrenaline, adrenaline) indoleamines (serotonin, melatonin) Quaternary amines acetylcholine Amino
- 34. Catecholamine synthesis -this is not for torture -understanding synthesis can be important for understanding drug action
- 35. Catecholamines Subtantia nigra and Parkinson’s disease Mesocorticolimbic system and schizophrenia Receptor specificity Dopamine
- 36. Catecholamines Noradrenergic pathways in the brain -locus coeruleus
- 37. Serotonin synthesis 5 HT – Serotonin – 5-hydroxytryptamine
- 38. Serotonin Serotonergic pathways in the brain -raphe, 16 subtypes
- 39. Acetylcholine synthesis
- 40. Acetylcholine Cholinergic pathways in the brain -basal forebrain, neuromuscular junction
- 41. Amino acids: The workhorses of the neurotransmitter family Glutamate - the primary excitatory neurotransmitter in brains
- 42. Amino Acid NTs Glutamate Uses both ionotropic and metabotropic receptors NT of the cerebral cortex Excitatory
- 43. The fabulous glutamate receptor Activation of NMDA receptor can cause changes in the numbers of AMPA
- 44. The fabulous GABA receptor Multiple binding sites
- 45. Drugs that Block Reuptake SSRIs (Serotonin Specific Reuptake Inhibitors) Cocaine - highly addictive, both physiologically and
- 46. Dose-Response Curves
- 47. Pharmacokinetics Blood Brain Barrier Blocks many chemicals in general circulation from entering the brain The capillaries
- 48. Pharmacokinetics
- 49. Pharmacokinetics Liver P450 Enzymes Everything absorbed from the GI tract passes through the liver before entering
- 50. Pharmacokinetics Liver P450 Enzymes (cont.) Levels of the ~50 P450 enzymes in humans can vary widely
- 51. Basic classification of drug actions Agonists stimulate or activate antagonists prevent
- 52. Ways that drugs can agonize Stimulate release receptor binding inhibition of reuptake inhibition of deactivation promote
- 53. Ways that drugs can antagonize Block release receptor blocker prevent synthesis
- 54. Schizophrenia Affects about 1/100 people Begins in 20’s Often triggered by stress, illness, etc. but there’s
- 55. Symptoms of schizophrenia Positive symptoms -hallucinations, delusions, paranoia Negative symptoms -lack of emotion, energy, directedness
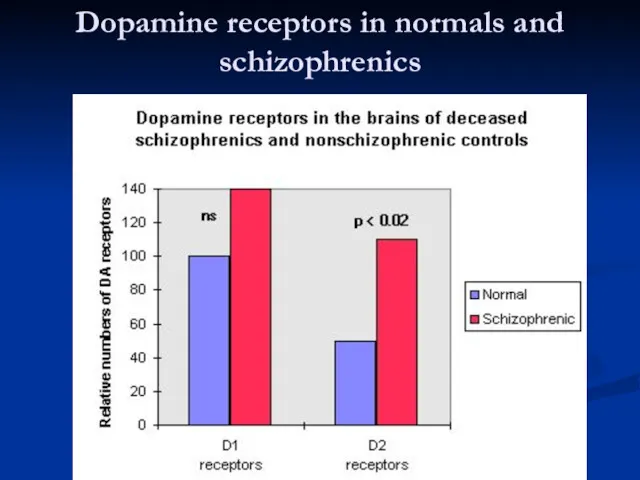
- 56. Schizophrenia Pathophysiology No consistent neuropathology or biomarkers for schizophrenia ? Increased dopamine in mesolimbic pathways causes
- 57. Schizophrenia Antipsychotics Typical / Conventional antipsychotics Atypical antipsychotics
- 58. The dopamine theory of schizophrenia
- 59. Dopamine receptors in normals and schizophrenics
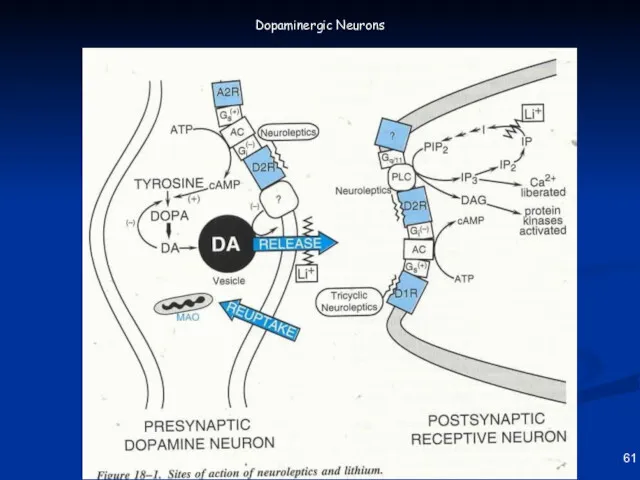
- 60. 61 Dopaminergic Neurons
- 61. Anti-psychotic Drugs Antipsychotic drugs (also known as major tranquilizers because they tranquilize and sedate mitigate or
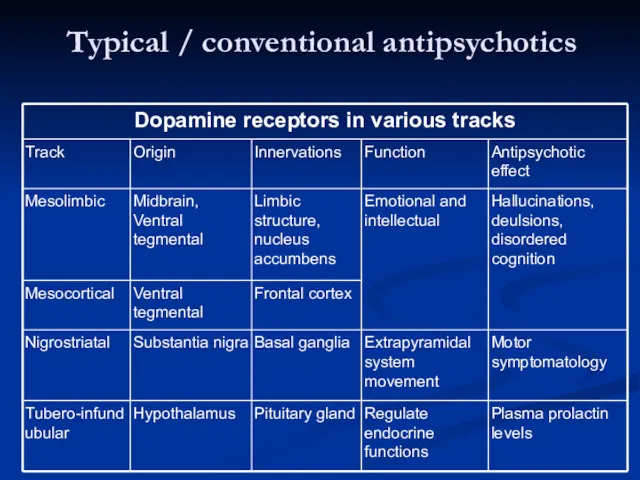
- 62. Typical / conventional antipsychotics
- 63. Typical / conventional antipsychotics Mechanism of action Blocks receptors for dopamine, acetylcholine, histamine and norepinephrine Current
- 64. Typical / conventional antipsychotics Properties Effective in reducing positive symptoms during acute episodes and in preventing
- 65. Typical / conventional antipsychotics Potency All have same ability to relieve symptoms of psychosis Differ from
- 66. Typical / conventional antipsychotics Low potency Chlorpromazine, thioridazine Medium potency Perphenazine High potency Trifluoperazine, thiothixene, fluphenazine,
- 67. BRAIN AREAS INVOLVED IN ANTIPSYCHOTIC TREATMENT The oversimplified version of what brain areas are involved in
- 68. BRAIN AREAS INVOLVED IN SCHIZOPHRENIA 4 DOPAMINE PATHWAYS There are four dopamine pathways in the brain:
- 69. Dopamine Pathways Nigrostriatal Chronic blockade can cause Potentially irreversible movement disorder “Tardive Dyskinesia”
- 70. Dopamine Pathways Mesocortical May be associated with both positive and negative symptoms Blockade may help reduce
- 71. Dopamine Pathways Tuberoinfundibular Blockade produces galactorrhea Dopamine = PIF (prolactin inhibiting factor)
- 72. Dopamine Pathways Summary Four dopamine pathways Appears that blocking dopamine receptors in only one of them
- 73. Dopaminergic D2 Blockade Possible Clinical Consequences Extrapyramidal movement disorders Endocrine changes Sexual dysfunction
- 74. Histamine H1 Blockade Possible Clinical Consequences Sedation, drowsiness Weight gain Hypotension
- 75. Alpha-1 receptor blockade Possible clinical consequences Postural hypotension Reflex tachycardia Dizziness
- 76. Muscarinic receptor blockade Possible clinical consequences Blurred vision Dry mouth Sinus tachycardia Constipation Urinary retention Memory
- 77. Extrapyramidal Symptoms Dopamine Vs Acetylcholine Dopamine and Acetylcholine have a reciprocal relationship in the Nigrostriatal pathway.
- 78. Extrapyramidal Symptoms Dopamine Vs Acetylcholine Dopamine blockade: A relative increase in cholinergic activity causing EPS Those
- 79. Extrapyramidal Symptoms Dopamine Vs Acetylcholine When high potency antipsychotics are chosen, we often prescribe anti-ACH medication
- 80. Neurological Side Effects: Dystonic Reactions: Uncoordinated spastic movements of muscle groups Trunk, tongue, face Akinesia: Decreased
- 81. Neurological Side Effects: Tremors: Fine movement (shaking) of the extremities Akathisia: Restlessness Pacing May result in
- 82. Typical / conventional antipsychotics Adverse effects Extrapyramidal symptoms (EPS) Early reactions – can be managed with
- 83. Typical / conventional antipsychotics Adverse effects Parkinsonism (neuroleptic induced) Occurs within first month of therapy Bradykinesia,
- 84. Typical / conventional antipsychotics Adverse effects Akathisia Develop within first 2 months of therapy Compulsive, restless
- 85. Tardive Dyskinesia Associated with long-term use of antipsychotics (chronic dopamine blockade) Potentially irreversible involuntary movements around
- 86. Tardive dyskinesia Can be precipitated by antipsychotic cessation Rate increased with comorbid substance use Aetiological hypotheses:
- 87. Tardive Dyskinesia Attempt of decrease dose will initially exacerbate the movements Increasing the dose will initially
- 88. Typical / conventional antipsychotics Adverse effects Tardive dyskinesia (TD) Develops months to years after therapy Involuntary
- 89. Typical / conventional antipsychotics Adverse effects Tardive dyskinesia (TD) Management Some manufacturers suggest drug withdrawal at
- 90. Neurological Effects
- 92. Скачать презентацию
Biological Therapy
in Psychiatry
Anatoly Kreinin MD, PhD
Director of Psychiatric Department, Tirat
Biological Therapy
in Psychiatry
Anatoly Kreinin MD, PhD
Director of Psychiatric Department, Tirat
Mental Health Care Pre-1930’s
Mental Health Care Pre-1930’s
Before we begin…
“It should be made clear that all psychotropic drugs
Before we begin…
“It should be made clear that all psychotropic drugs
What is a ‘drug’?
A very vague term
all ingested substances alter bodily
What is a ‘drug’?
A very vague term
all ingested substances alter bodily

HISTORY OF ANTIPSYCHOTICS
Anti-psychotics were discovered accidentally by a French naval surgeon,
HISTORY OF ANTIPSYCHOTICS
Anti-psychotics were discovered accidentally by a French naval surgeon,
Treatment Before Drugs Came into Play
King Saul – vine, music-therapy
Patients
Treatment Before Drugs Came into Play
King Saul – vine, music-therapy
Patients
Efficacy and Potency
Efficacy - Ability of a drug to produce a
Efficacy and Potency
Efficacy - Ability of a drug to produce a
Drug Toxicity
Toxicity: Point at which concentrations of the drug in the
Drug Toxicity
Toxicity: Point at which concentrations of the drug in the
Absorption
From site of administration into the plasma
Oral - (tablet and liquid)
Absorption
From site of administration into the plasma
Oral - (tablet and liquid)
Pharmacokinetics:
How the Body Acts on the Drug
Absorption
Distribution
Metabolism
Elimination
Pharmacokinetics:
How the Body Acts on the Drug
Absorption
Distribution
Metabolism
Elimination
Bioavailability
Amount of drug that reaches systemic circulation unchanged
Often used to
Bioavailability
Amount of drug that reaches systemic circulation unchanged
Often used to
Distribution
Amount of drug found in various tissues, especially the intended ones.
Distribution
Amount of drug found in various tissues, especially the intended ones.
Crossing the Blood Brain Barrier
Passive diffusion
Drug must dissolve in the structure
Crossing the Blood Brain Barrier
Passive diffusion
Drug must dissolve in the structure
Metabolism
Process by which the drug is altered and broken down into
Metabolism
Process by which the drug is altered and broken down into
Elimination
Clearance: Total amount of blood, serum, or plasma from which a
Elimination
Clearance: Total amount of blood, serum, or plasma from which a
Dosing and Steady State
Dosing: Administration of medication over time, so that
Dosing and Steady State
Dosing: Administration of medication over time, so that
Pharmacokinetics: Cultural Considerations
9% of whites - genetically defective P-4502D6
Asian descent
Metabolize ethanol
Pharmacokinetics: Cultural Considerations
9% of whites - genetically defective P-4502D6
Asian descent
Metabolize ethanol
Phases of Drug Treatment
Initiation
Stabilization
Maintenance
Discontinuation
Phases of Drug Treatment
Initiation
Stabilization
Maintenance
Discontinuation
Tolerance & Dependence
Tolerance – state of decreased sensitivity to the drug
Tolerance & Dependence
Tolerance – state of decreased sensitivity to the drug
Receptors
Types of Action
Agonist: same biologic action
Antagonist: opposite effect
Interactions with a receptor
Receptors
Types of Action
Agonist: same biologic action
Antagonist: opposite effect
Interactions with a receptor
Ion Channels
Drugs can block or open the ion channels
Example: benzodiazepine drugs
Ion Channels
Drugs can block or open the ion channels
Example: benzodiazepine drugs
Enzymes
Enzymes catalyze specific biochemical reactions within cells and are targets for
Enzymes
Enzymes catalyze specific biochemical reactions within cells and are targets for
Carrier Proteins
Transport neurotransmitters across cell membranes
Medications may block or inhibit this
Carrier Proteins
Transport neurotransmitters across cell membranes
Medications may block or inhibit this
Being a neurotransmitter: What does it take?
Exists presynaptically
Synthesis enzymes exist presynaptically
Released
Being a neurotransmitter: What does it take?
Exists presynaptically
Synthesis enzymes exist presynaptically
Released
Neurotransmitters
80 plus chemical substances that provide communication between cells. Some of
Neurotransmitters
80 plus chemical substances that provide communication between cells. Some of
All psychoactive drugs act centrally (i.e. on the brain)
The vast majority
All psychoactive drugs act centrally (i.e. on the brain)
The vast majority
Neurotransmitters have 7 actions
Synthesized
Stored
Enzymatically destroyed if not stored
Exocytosis
Termination
Neurotransmitters have 7 actions
Synthesized
Stored
Enzymatically destroyed if not stored
Exocytosis
Termination
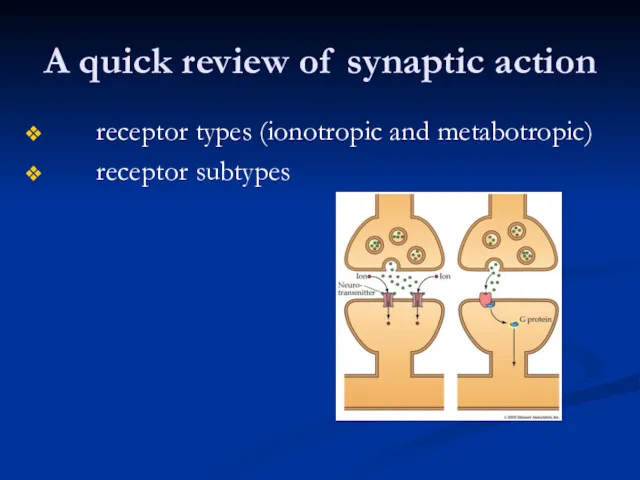
A quick review of synaptic action
receptor types (ionotropic and metabotropic)
receptor subtypes
A quick review of synaptic action
receptor types (ionotropic and metabotropic)
receptor subtypes
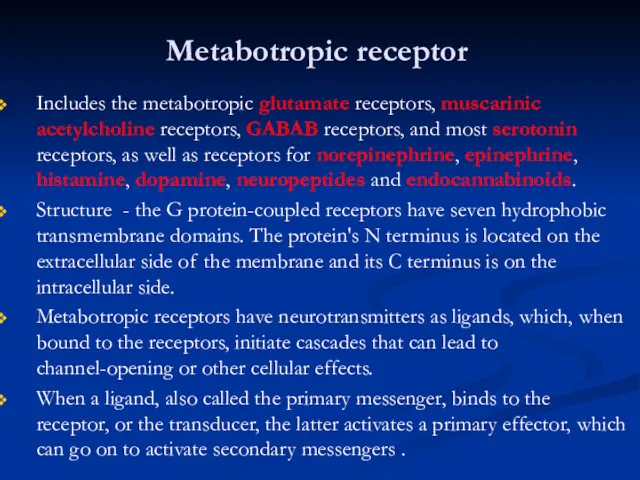
Metabotropic receptor
Includes the metabotropic glutamate receptors, muscarinic acetylcholine receptors, GABAB receptors,
Metabotropic receptor
Includes the metabotropic glutamate receptors, muscarinic acetylcholine receptors, GABAB receptors,
Since opening channels by metabotropic receptors involves activating a number of
Since opening channels by metabotropic receptors involves activating a number of
The classical neurotransmitters
Amines
Monoamines
catecholamines (dopamine, noradrenaline, adrenaline)
indoleamines (serotonin, melatonin)
Quaternary amines
acetylcholine
Amino acids (glutamate,
The classical neurotransmitters
Amines
Monoamines
catecholamines (dopamine, noradrenaline, adrenaline)
indoleamines (serotonin, melatonin)
Quaternary amines
acetylcholine
Amino acids (glutamate,
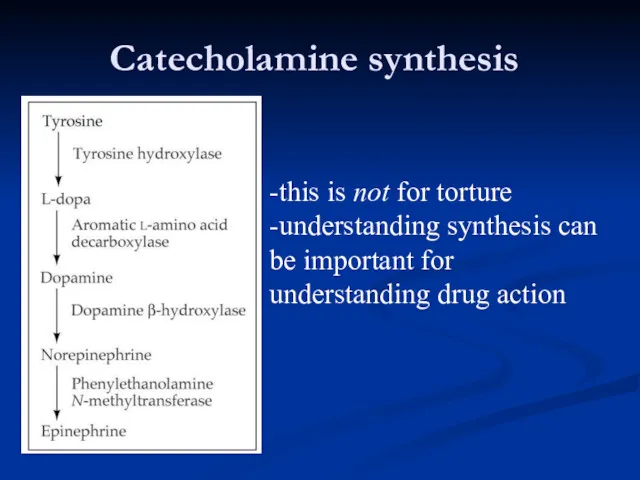
Catecholamine synthesis
-this is not for torture
-understanding synthesis can be important for
Catecholamine synthesis
-this is not for torture
-understanding synthesis can be important for
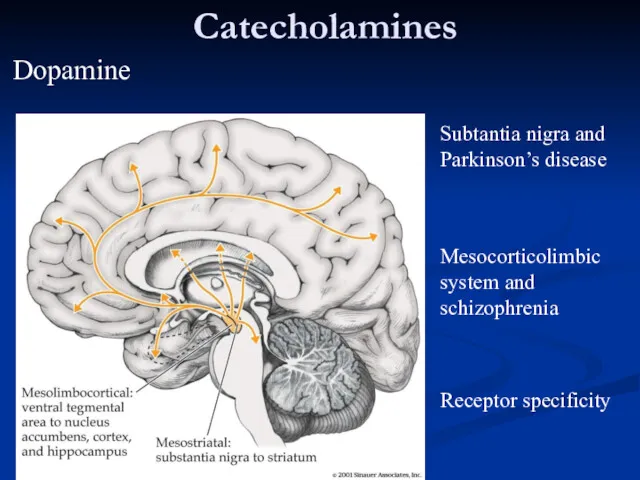
Catecholamines
Subtantia nigra and
Parkinson’s disease
Mesocorticolimbic system and schizophrenia
Receptor specificity
Dopamine
Catecholamines
Subtantia nigra and
Parkinson’s disease
Mesocorticolimbic system and schizophrenia
Receptor specificity
Dopamine
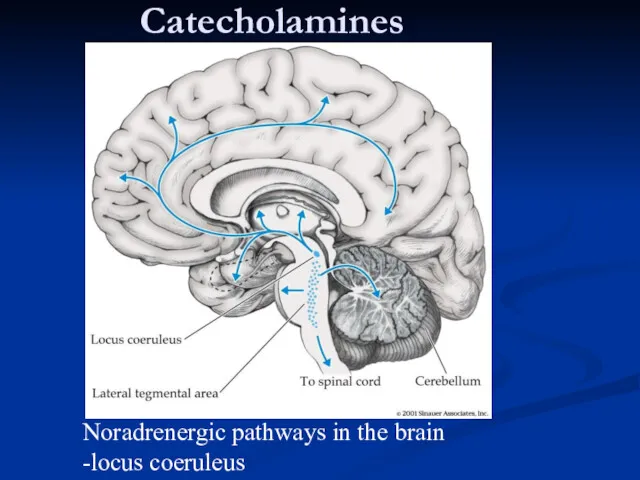
Catecholamines
Noradrenergic pathways in the brain
-locus coeruleus
Catecholamines
Noradrenergic pathways in the brain
-locus coeruleus
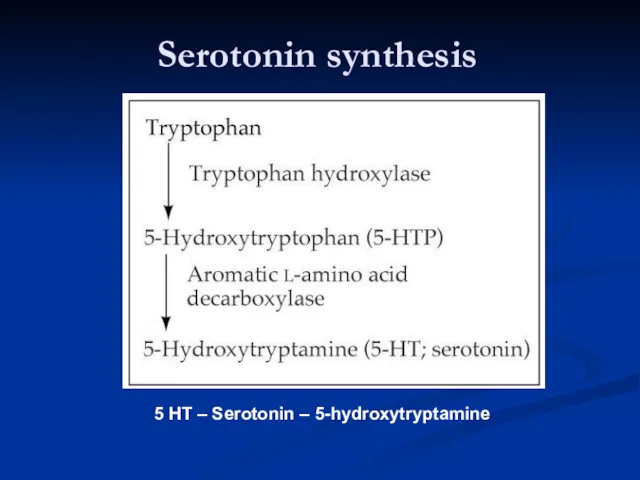
Serotonin synthesis
5 HT – Serotonin – 5-hydroxytryptamine
Serotonin synthesis
5 HT – Serotonin – 5-hydroxytryptamine
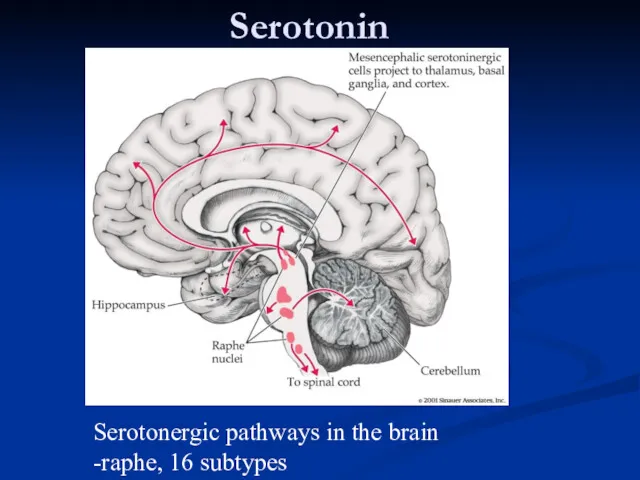
Serotonin
Serotonergic pathways in the brain
-raphe, 16 subtypes
Serotonin
Serotonergic pathways in the brain
-raphe, 16 subtypes
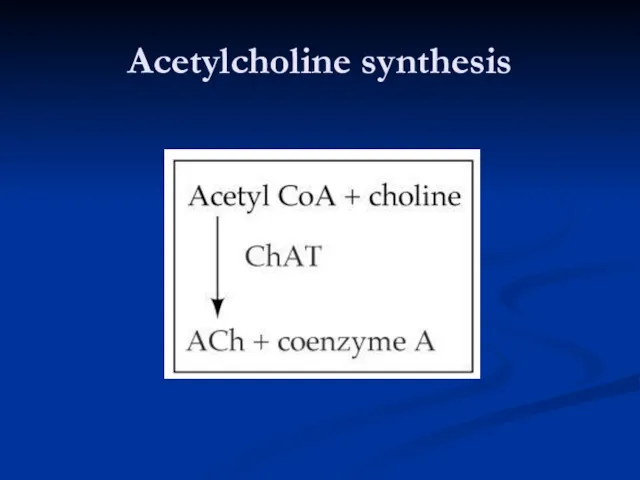
Acetylcholine synthesis
Acetylcholine synthesis
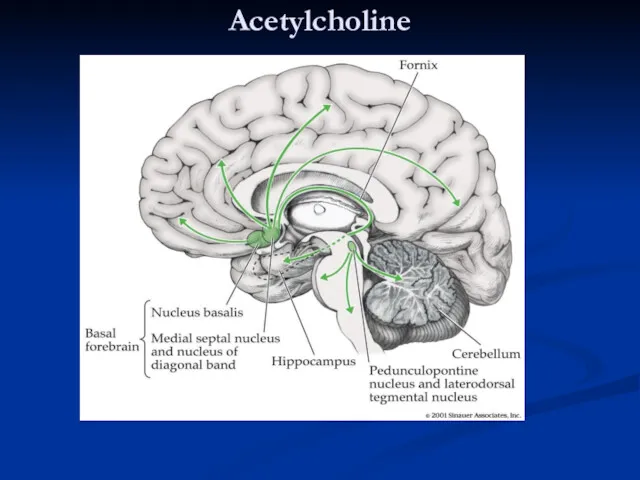
Acetylcholine
Cholinergic pathways in the brain
-basal forebrain, neuromuscular junction
Acetylcholine
Cholinergic pathways in the brain
-basal forebrain, neuromuscular junction
Amino acids: The workhorses of the neurotransmitter family
Glutamate - the primary
Amino acids: The workhorses of the neurotransmitter family
Glutamate - the primary
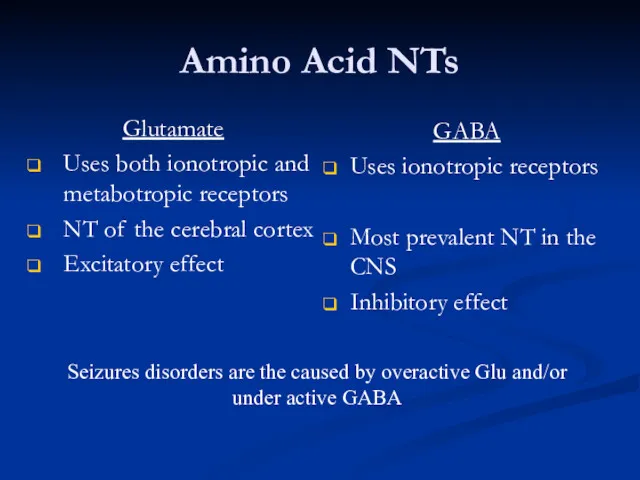
Amino Acid NTs
Glutamate
Uses both ionotropic and metabotropic receptors
NT of the cerebral
Amino Acid NTs
Glutamate
Uses both ionotropic and metabotropic receptors
NT of the cerebral
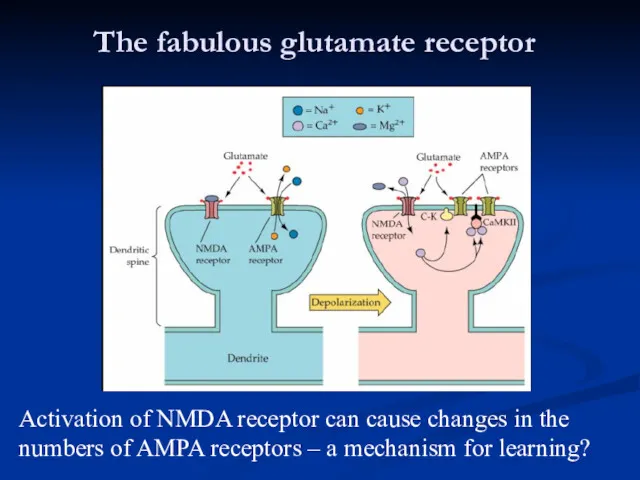
The fabulous glutamate receptor
Activation of NMDA receptor can cause changes in
The fabulous glutamate receptor
Activation of NMDA receptor can cause changes in
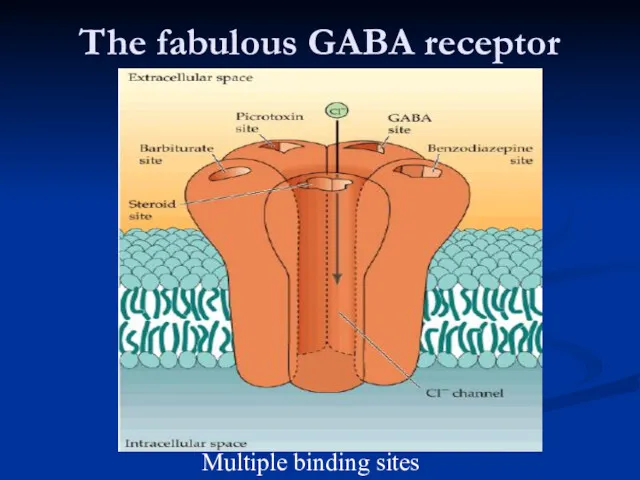
The fabulous GABA receptor
Multiple binding sites
The fabulous GABA receptor
Multiple binding sites
Drugs that Block Reuptake
SSRIs (Serotonin Specific Reuptake Inhibitors)
Cocaine
- highly addictive, both
Drugs that Block Reuptake
SSRIs (Serotonin Specific Reuptake Inhibitors)
Cocaine
- highly addictive, both
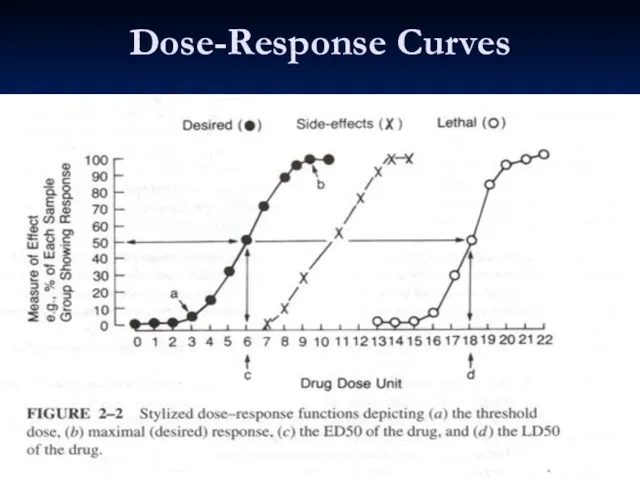
Dose-Response Curves
Dose-Response Curves
Pharmacokinetics
Blood Brain Barrier
Blocks many chemicals in general circulation from entering the
Pharmacokinetics
Blood Brain Barrier
Blocks many chemicals in general circulation from entering the
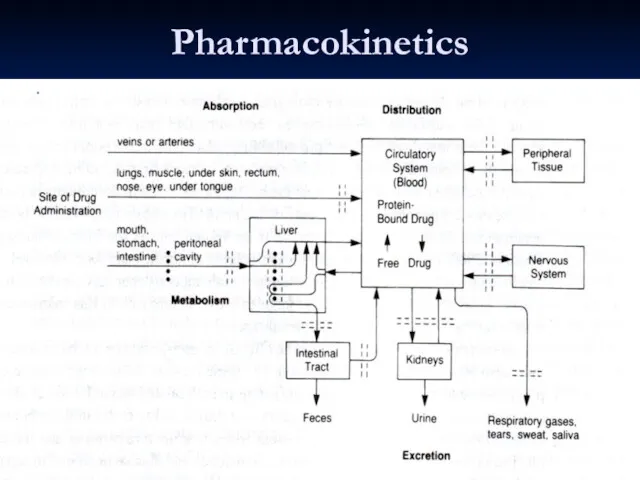
Pharmacokinetics
Pharmacokinetics
Pharmacokinetics
Liver P450 Enzymes
Everything absorbed from the GI tract passes through the
Pharmacokinetics
Liver P450 Enzymes
Everything absorbed from the GI tract passes through the
Pharmacokinetics
Liver P450 Enzymes (cont.)
Levels of the ~50 P450 enzymes in humans
Pharmacokinetics
Liver P450 Enzymes (cont.)
Levels of the ~50 P450 enzymes in humans
Basic classification of drug actions
Agonists stimulate or activate
antagonists prevent
Basic classification of drug actions
Agonists stimulate or activate
antagonists prevent
Ways that drugs can agonize
Stimulate release
receptor binding
inhibition of reuptake
inhibition
Ways that drugs can agonize
Stimulate release
receptor binding
inhibition of reuptake
inhibition
Ways that drugs can antagonize
Block release
receptor blocker
prevent synthesis
Ways that drugs can antagonize
Block release
receptor blocker
prevent synthesis
Schizophrenia
Affects about 1/100 people
Begins in 20’s
Often triggered by stress, illness, etc.
Schizophrenia
Affects about 1/100 people
Begins in 20’s
Often triggered by stress, illness, etc.
Symptoms of schizophrenia
Positive symptoms
-hallucinations, delusions, paranoia
Negative symptoms
-lack of emotion, energy, directedness
Symptoms of schizophrenia
Positive symptoms
-hallucinations, delusions, paranoia
Negative symptoms
-lack of emotion, energy, directedness
Schizophrenia
Pathophysiology
No consistent neuropathology or biomarkers for schizophrenia
? Increased dopamine in
Schizophrenia
Pathophysiology
No consistent neuropathology or biomarkers for schizophrenia
? Increased dopamine in
Schizophrenia
Antipsychotics
Typical / Conventional antipsychotics
Atypical antipsychotics
Schizophrenia
Antipsychotics
Typical / Conventional antipsychotics
Atypical antipsychotics
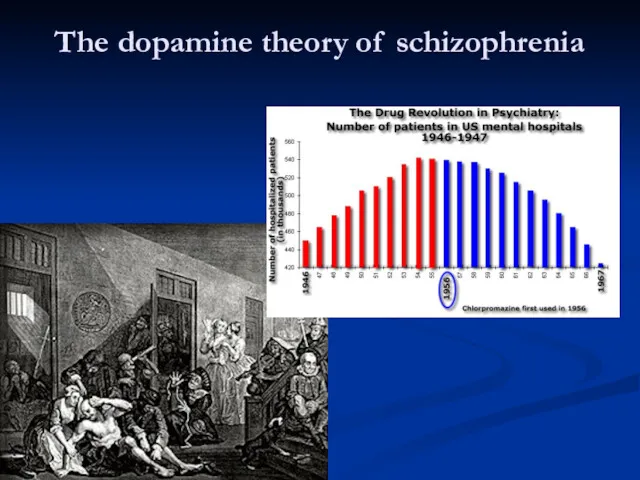
The dopamine theory of schizophrenia
The dopamine theory of schizophrenia
Dopamine receptors in normals and schizophrenics
Dopamine receptors in normals and schizophrenics
61
Dopaminergic Neurons
61
Dopaminergic Neurons
Anti-psychotic Drugs
Antipsychotic drugs (also known as major tranquilizers because they tranquilize
Anti-psychotic Drugs
Antipsychotic drugs (also known as major tranquilizers because they tranquilize
Typical / conventional antipsychotics
Typical / conventional antipsychotics
Typical / conventional antipsychotics
Mechanism of action
Blocks receptors for dopamine, acetylcholine, histamine
Typical / conventional antipsychotics
Mechanism of action
Blocks receptors for dopamine, acetylcholine, histamine
Typical / conventional antipsychotics
Properties
Effective in reducing positive symptoms during acute episodes
Typical / conventional antipsychotics
Properties
Effective in reducing positive symptoms during acute episodes
Typical / conventional antipsychotics
Potency
All have same ability to relieve symptoms of
Typical / conventional antipsychotics
Potency
All have same ability to relieve symptoms of
Typical / conventional antipsychotics
Low potency
Chlorpromazine, thioridazine
Medium potency
Perphenazine
High potency
Trifluoperazine, thiothixene, fluphenazine, haloperidol,
Typical / conventional antipsychotics
Low potency
Chlorpromazine, thioridazine
Medium potency
Perphenazine
High potency
Trifluoperazine, thiothixene, fluphenazine, haloperidol,
BRAIN AREAS INVOLVED IN ANTIPSYCHOTIC TREATMENT
The oversimplified version of what brain
BRAIN AREAS INVOLVED IN ANTIPSYCHOTIC TREATMENT
The oversimplified version of what brain
BRAIN AREAS INVOLVED IN SCHIZOPHRENIA
4 DOPAMINE PATHWAYS
There are four dopamine
BRAIN AREAS INVOLVED IN SCHIZOPHRENIA
4 DOPAMINE PATHWAYS
There are four dopamine
Dopamine Pathways
Nigrostriatal
Chronic blockade can cause
Potentially irreversible movement disorder
“Tardive Dyskinesia”
Dopamine Pathways
Nigrostriatal
Chronic blockade can cause
Potentially irreversible movement disorder
“Tardive Dyskinesia”
Dopamine Pathways
Mesocortical
May be associated with both positive and negative symptoms
Blockade may
Dopamine Pathways
Mesocortical
May be associated with both positive and negative symptoms
Blockade may
Dopamine Pathways
Tuberoinfundibular
Blockade produces galactorrhea
Dopamine = PIF (prolactin inhibiting factor)
Dopamine Pathways
Tuberoinfundibular
Blockade produces galactorrhea
Dopamine = PIF (prolactin inhibiting factor)
Dopamine Pathways
Summary
Four dopamine pathways
Appears that blocking dopamine receptors in only one
Dopamine Pathways
Summary
Four dopamine pathways
Appears that blocking dopamine receptors in only one
Dopaminergic D2 Blockade
Possible Clinical Consequences
Extrapyramidal movement disorders
Endocrine changes
Sexual dysfunction
Dopaminergic D2 Blockade
Possible Clinical Consequences
Extrapyramidal movement disorders
Endocrine changes
Sexual dysfunction
Histamine H1 Blockade
Possible Clinical Consequences
Sedation, drowsiness
Weight gain
Hypotension
Histamine H1 Blockade
Possible Clinical Consequences
Sedation, drowsiness
Weight gain
Hypotension
Alpha-1 receptor blockade
Possible clinical consequences
Postural hypotension
Reflex tachycardia
Dizziness
Alpha-1 receptor blockade
Possible clinical consequences
Postural hypotension
Reflex tachycardia
Dizziness
Muscarinic receptor blockade
Possible clinical consequences
Blurred vision
Dry mouth
Sinus tachycardia
Constipation
Urinary retention
Memory dysfunction
Muscarinic receptor blockade
Possible clinical consequences
Blurred vision
Dry mouth
Sinus tachycardia
Constipation
Urinary retention
Memory dysfunction
Extrapyramidal Symptoms
Dopamine Vs Acetylcholine
Dopamine and Acetylcholine have a reciprocal relationship in
Extrapyramidal Symptoms
Dopamine Vs Acetylcholine
Dopamine and Acetylcholine have a reciprocal relationship in
Extrapyramidal Symptoms
Dopamine Vs Acetylcholine
Dopamine blockade:
A relative increase in cholinergic activity
causing EPS
Those
Extrapyramidal Symptoms
Dopamine Vs Acetylcholine
Dopamine blockade:
A relative increase in cholinergic activity
causing EPS
Those
Extrapyramidal Symptoms
Dopamine Vs Acetylcholine
When high potency antipsychotics are chosen, we often
Extrapyramidal Symptoms
Dopamine Vs Acetylcholine
When high potency antipsychotics are chosen, we often
Neurological Side Effects:
Dystonic Reactions:
Uncoordinated spastic movements of muscle groups
Trunk, tongue, face
Akinesia:
Decreased
Neurological Side Effects:
Dystonic Reactions:
Uncoordinated spastic movements of muscle groups
Trunk, tongue, face
Akinesia:
Decreased
Neurological Side Effects:
Tremors:
Fine movement (shaking) of the extremities
Akathisia:
Restlessness
Pacing
May result in
Neurological Side Effects:
Tremors:
Fine movement (shaking) of the extremities
Akathisia:
Restlessness
Pacing
May result in
Typical / conventional antipsychotics
Adverse effects
Extrapyramidal symptoms (EPS)
Early reactions – can be
Typical / conventional antipsychotics
Adverse effects
Extrapyramidal symptoms (EPS)
Early reactions – can be
Typical / conventional antipsychotics
Adverse effects
Parkinsonism (neuroleptic induced)
Occurs within first month of
Typical / conventional antipsychotics
Adverse effects
Parkinsonism (neuroleptic induced)
Occurs within first month of
Typical / conventional antipsychotics
Adverse effects
Akathisia
Develop within first 2 months of therapy
Compulsive,
Typical / conventional antipsychotics
Adverse effects
Akathisia
Develop within first 2 months of therapy
Compulsive,
Tardive Dyskinesia
Associated with long-term use of antipsychotics
(chronic dopamine blockade)
Potentially irreversible involuntary
Tardive Dyskinesia
Associated with long-term use of antipsychotics
(chronic dopamine blockade)
Potentially irreversible involuntary
Tardive dyskinesia
Can be precipitated by antipsychotic cessation
Rate increased with comorbid substance
Tardive dyskinesia
Can be precipitated by antipsychotic cessation
Rate increased with comorbid substance
Tardive Dyskinesia
Attempt of decrease dose
will initially exacerbate the movements
Increasing the dose
Tardive Dyskinesia
Attempt of decrease dose
will initially exacerbate the movements
Increasing the dose
Typical / conventional antipsychotics
Adverse effects
Tardive dyskinesia (TD)
Develops months to years after
Typical / conventional antipsychotics
Adverse effects
Tardive dyskinesia (TD)
Develops months to years after
Typical / conventional antipsychotics
Adverse effects
Tardive dyskinesia (TD)
Management
Some manufacturers suggest drug withdrawal
Typical / conventional antipsychotics
Adverse effects
Tardive dyskinesia (TD)
Management
Some manufacturers suggest drug withdrawal
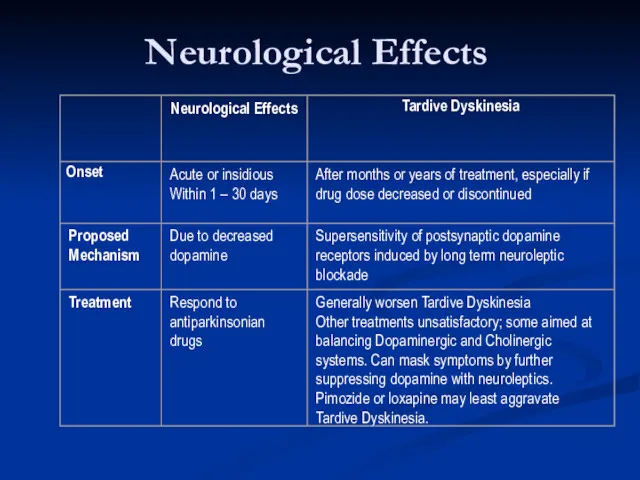
Neurological Effects
Neurological Effects
 Лучевая диагностика остеоартрозов и артрозоартритов
Лучевая диагностика остеоартрозов и артрозоартритов Гипертермический синдром
Гипертермический синдром Клинический случай
Клинический случай Показания и противопоказания переливания крови. Способы, виды, методы переливания. Осложнения и профилактика
Показания и противопоказания переливания крови. Способы, виды, методы переливания. Осложнения и профилактика Развитие органов кроветворения и иммунной защиты
Развитие органов кроветворения и иммунной защиты Физика и метафизика смерти
Физика и метафизика смерти Доказательная медицина в сестринском деле. Концепция доказательной медицины. Основные понятия
Доказательная медицина в сестринском деле. Концепция доказательной медицины. Основные понятия Закрытые и открытые повреждения грудной клетки и ее органов
Закрытые и открытые повреждения грудной клетки и ее органов Особенности конструирования зубных протезов при опоре на имплантаты. Принципы выбора рациональных структур имплантатов
Особенности конструирования зубных протезов при опоре на имплантаты. Принципы выбора рациональных структур имплантатов Ветеринарная вирусология. Вирус европейской чумы свиней
Ветеринарная вирусология. Вирус европейской чумы свиней ботулизм
ботулизм Листериялар. Морфологиясы, физиологиясы, листериялардың антигендері. Экологиясы. Әйелдер патологиясындағы ролі
Листериялар. Морфологиясы, физиологиясы, листериялардың антигендері. Экологиясы. Әйелдер патологиясындағы ролі Энцефалопатия Балалардың церебралдық салдары
Энцефалопатия Балалардың церебралдық салдары Ортопедическое лечение при заболеваниях пародонта
Ортопедическое лечение при заболеваниях пародонта Коморбидные формы ВИЧ-инфекции
Коморбидные формы ВИЧ-инфекции Эпилепсия. Диагностика и лечение
Эпилепсия. Диагностика и лечение Биохимия почек и мочи. (Лекция 10)
Биохимия почек и мочи. (Лекция 10) Неспецифический язвенный колит
Неспецифический язвенный колит Симтоматология гастритов, язвенной болезни желудка и двенадцатиперстной кишки. Заболевания тонкого и толстого кишечника
Симтоматология гастритов, язвенной болезни желудка и двенадцатиперстной кишки. Заболевания тонкого и толстого кишечника Функциональная анатомия органов мужской половой системы
Функциональная анатомия органов мужской половой системы Faberlic - Expert. Домашняя альтернатива салонным процедурам
Faberlic - Expert. Домашняя альтернатива салонным процедурам Дорсопатия - дегенеративно-дистрофические заболевания позвоночника и околопозвоночных тканей
Дорсопатия - дегенеративно-дистрофические заболевания позвоночника и околопозвоночных тканей Желтуха новорожденных
Желтуха новорожденных Әйелдер консультациясы және отбасын жоспарлау орталықтарында жас ата-аналар мектебінің жұмысына қатысып есеп жазу
Әйелдер консультациясы және отбасын жоспарлау орталықтарында жас ата-аналар мектебінің жұмысына қатысып есеп жазу Сердечно-сосудистая недостаточность у новорожденных детей
Сердечно-сосудистая недостаточность у новорожденных детей Расстройства ощущений и восприятия
Расстройства ощущений и восприятия Приобретённые пороки сердца
Приобретённые пороки сердца Жүкті әйелді антенаталды бақылау, физиологиялық жүктілікті бақылау, босануға психологиялық дайындық
Жүкті әйелді антенаталды бақылау, физиологиялық жүктілікті бақылау, босануға психологиялық дайындық