- Burns

Содержание
- 2. Frequency 67% occur in males Young adults (20-29 yr) Children > 50 years of age fewest
- 3. INCIDENCE Approx. one million burn patients/annually in the United States 3-5% cases are life-threatening 60,000 hospitalized
- 4. Functions Skin is the largest organ of the body 1,5—2 м2 Essential for: - Thermoregulation -
- 5. Skin Anatomy and Function Largest organ 3 major tissue layers Epidermis Outermost layer Dermis Below epidermis
- 6. Types of burn injuries Thermal: direct contact with heat (flame, scald, contact) Electrical A.C. – alternating
- 7. Classification Burns are classified by depth, type and extent of injury Every aspect of burn treatment
- 8. First degree burn Involves only the epidermis Tissue will blanch with pressure Tissue is erythematous and
- 9. Second degree burn Referred to as partial-thickness burns Involve the epidermis and portions of the dermis
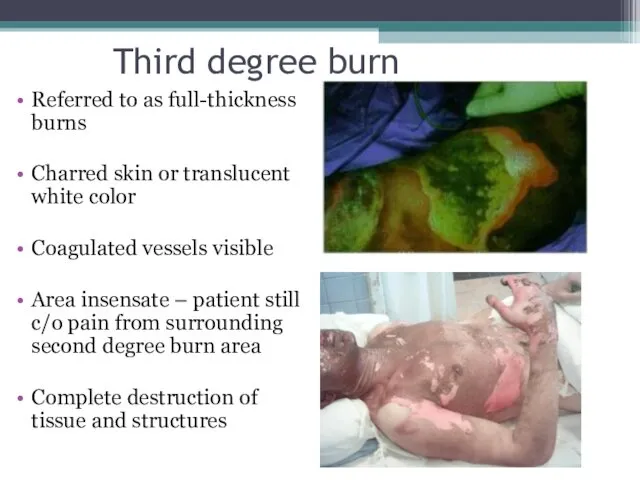
- 10. Third degree burn Referred to as full-thickness burns Charred skin or translucent white color Coagulated vessels
- 11. Fourth degree burn Involves subcutaneous tissue, tendons and bone
- 12. Zones of Burn Wounds Zone of Coagulation devitalized, necrotic, white, no circulation Zone of Stasis ‘circulation
- 13. Burn extent % BSA involved morbidity Burn extent is calculated only on individuals with second and
- 14. Measurement charts Rule of Nines: Quick estimate of percent of burn Rule of Palms: Good for
- 15. Rule of 9s ABA
- 16. Rule of Palms
- 17. Lab studies Severe burns: CBC Chemistry profile Coagulation profile creatine phosphokinase and urine myoglobin (with electrical
- 18. otolaryngologist Neurologist ophthalmologist Fibrobronchoscopy Examination by doctors
- 19. Imaging studies X-Ray Plain Films / CT scan: Dependent upon history and physical findings
- 20. Criteria for burn center admission Full-thickness > 5% BSA Partial-thickness > 10% BSA Any full-thickness or
- 21. Initial patient treatment Stop the burning process Consider burn patient as a multiple trauma patient until
- 22. Details of the incident Cause of the burn Time of injury Place of the occurrence (closed
- 23. Care of small burns What can YOU do?
- 24. Care of small burns Clean entire limb with soap and water (also under nails). Apply antibiotic
- 25. Blisters In the pre-hospital setting, there is no hurry to remove blisters. Leaving the blister intact
- 26. Blisters break on their own Upper arm burn day 1 day 2 Burn “looks worse” the
- 27. Upper arm burn Blisters show probable partial thickness burn. Area without blister might be deeper partial
- 28. Debride blister using simple instruments
- 29. After debridement
- 30. Before and after debridement Removing the blister leaves a weeping, very tender wound, that requires much
- 31. Silver sulfadiazene
- 32. Arm burn 7 days – note the exudate
- 33. Burns of special areas of the body Face Mouth Neck Hands and feet Genitalia
- 34. Face Be VERY concerned for the airway!! Eyelids, lips and ears often swell. In fact, they
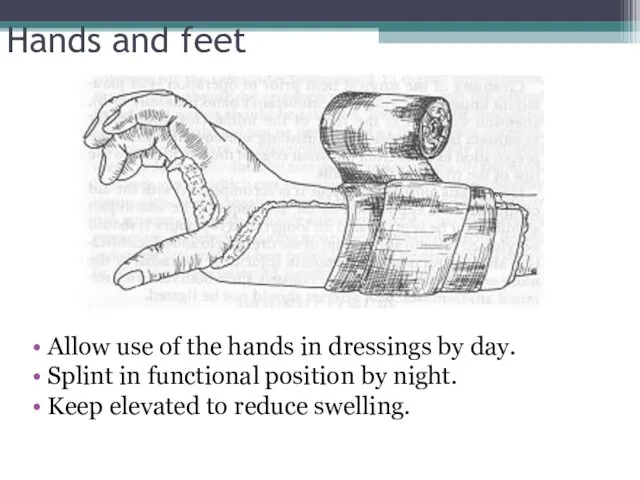
- 35. Hands and feet This is rather deep and might require grafting. But initial management is basic.
- 36. Hands and feet Allow use of the hands in dressings by day. Splint in functional position
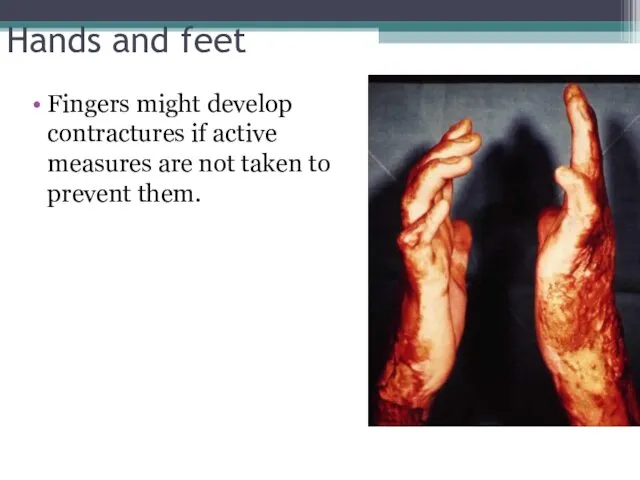
- 37. Hands and feet Fingers might develop contractures if active measures are not taken to prevent them.
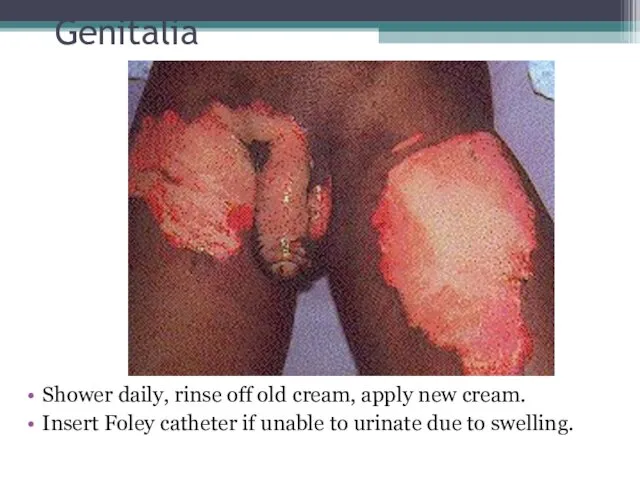
- 38. Genitalia Shower daily, rinse off old cream, apply new cream. Insert Foley catheter if unable to
- 39. Large Burns
- 40. Causes of death in burn patients Airway Facial edema, and/or airway edema Breathing Toxic inhalation (CO,
- 41. Edema Formation Amount of edema can be immense (even without facial burns) Depression of mental status
- 42. Causes of death in burn patients Circulation: “failure of resuscitation” Cardiovascular collapse, or acute MI Acute
- 43. Patients with larger burns First assess CBA’s “Disability” (brief neuro exam) Later Examine rest of patient
- 44. Airway considerations Upper airway injury (above the glottis): Area buffers the heat of smoke – thermal
- 45. Criteria for intubation Changes in voice Wheezing / labored respirations Excessive, continuous coughing Altered mental status
- 46. Ventilatory therapies Rapid Sequence Intubation Pain Management, Sedation and Paralysis PEEP (positive end expiratory pressure) High
- 47. Ventilatory therapies Burn patients with Acute respiratory distress syndrome (ARDS) requiring PEEP (positive end expiratory pressure)
- 48. Circumferential burns of the chest Eschar - burned, inflexible, necrotic tissue Compromises ventilatory motion Escharotomy may
- 49. Carbon Monoxide Intoxication Carbon monoxide has a binding affinity for hemoglobin which is 210-240 times greater
- 50. Signs and Symptoms of Carbon Monoxide Intoxication Usually symptoms not present until 15% of the hemoglobin
- 51. Signs and Symptoms of Carbon Monoxide Intoxication Confused, irritable, restless Headache Tachycardia, arrhythmias or infarction Vomiting
- 52. Carboxyhemoglobin Levels/Symptoms 0 – 5 15 – 20 20 – 40 40 - 60 > 60
- 53. Management of Carbon Monoxide Intoxication Remove patient from source of exposure. Administer 100% high flow oxygen
- 54. Circulation considerations Formation of edema is the greatest initial volume loss Burns 30% or Edema is
- 55. Circulation considerations Capillary permeability increased Protein molecules are now able to cross the membrane Reduced intravascular
- 56. Circulation considerations Loss of plasma volume is greatest during the first 4 – 6 hours, decreasing
- 57. Fluid resuscitation Goal: Maintain perfusion to vital organs Based on the TBSA, body weight and whether
- 58. Fluid resuscitation Lactated Ringers - preferred solution Contains Na+ - restoration of Na+ loss is essential
- 59. Fluid resuscitation Burned patients have large insensible fluid losses Fluid volumes may increase in patients with
- 60. Fluid resuscitation Fluid requirement calculations for infusion rates are based on the time from injury, not
- 61. Assessing adequacy of resuscitation Peripheral blood pressure: may be difficult to obtain Urine Output: Best indicator
- 62. Parkland Formula 4 x % burn x body wt. In kg. ½ of calculated fluid is
- 63. Effects of hypothermia Hypothermia may lead to acidosis/coagulopathy Hypothermia causes peripheral vasoconstriction and impairs oxygen delivery
- 64. Prevention of hypothermia Cover patients with a dry sheet – keep head covered Pre-warm trauma room
- 65. Pain management Adequate analgesia imperative! DOC: Morphine Sulfate Dose: Adults: 0.1 – 0.2 mg/kg IVP Children:
- 66. Antibiotics Prophylactic antibiotics are not indicated in the early postburn period.
- 67. Other considerations Check tetanus status – administer Td as appropriate Debride and treat open blisters or
- 68. Electrical burns: are thermal injuries resulting from high intensity heat. The skin injury area may appear
- 69. Chemical burns- Most often caused by strong acids or alkalis. Unlike thermal burns, they can cause
- 70. Burn Injury: Summary Many risk factors age dependent Pediatricians primary role: prevention High risk of multiple
- 72. Скачать презентацию
Frequency
67% occur in males
Young adults (20-29 yr)
Children < 9 years of
Frequency
67% occur in males
Young adults (20-29 yr)
Children < 9 years of
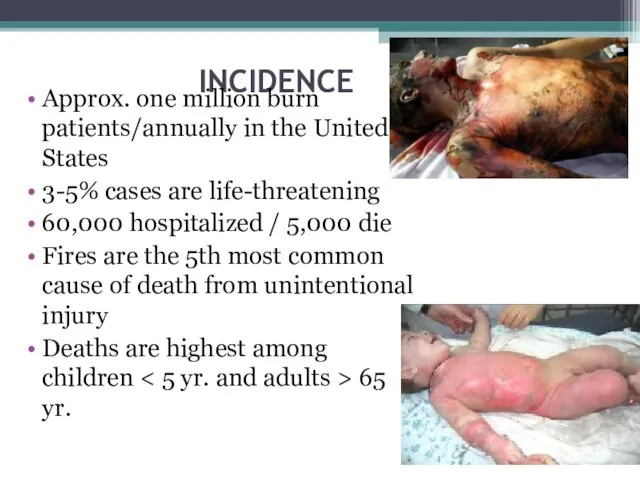
INCIDENCE
Approx. one million burn patients/annually in the United States
3-5% cases are
INCIDENCE
Approx. one million burn patients/annually in the United States
3-5% cases are
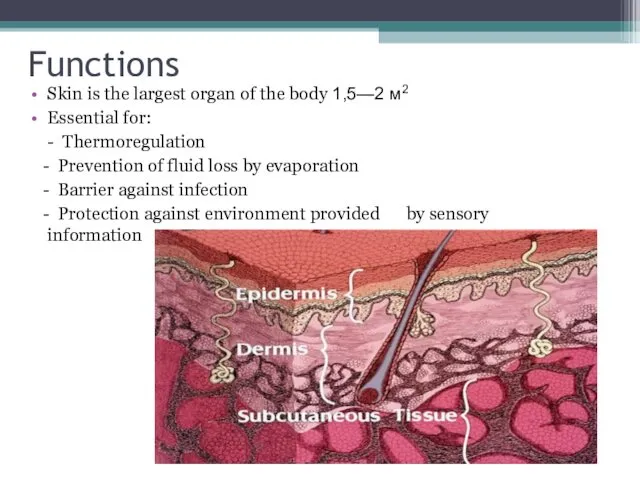
Functions
Skin is the largest organ of the body 1,5—2 м2
Essential for:
-
Functions
Skin is the largest organ of the body 1,5—2 м2
Essential for:
-
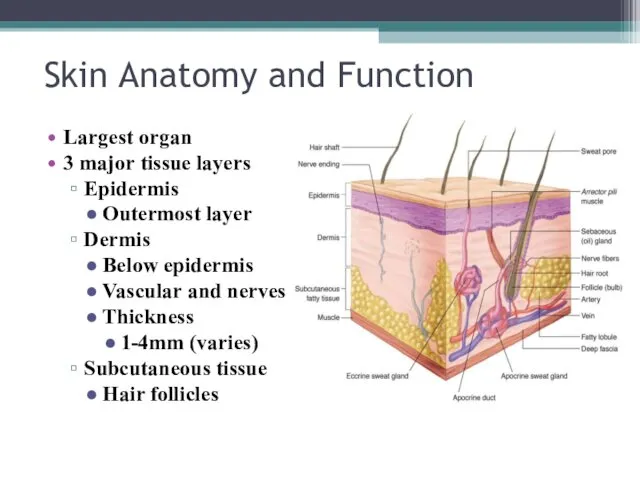
Skin Anatomy and Function
Largest organ
3 major tissue layers
Epidermis
Outermost layer
Dermis
Below epidermis
Vascular and
Skin Anatomy and Function
Largest organ
3 major tissue layers
Epidermis
Outermost layer
Dermis
Below epidermis
Vascular and
Types of burn injuries
Thermal: direct contact with heat
(flame, scald, contact)
Electrical
Types of burn injuries
Thermal: direct contact with heat
(flame, scald, contact)
Electrical
Classification
Burns are classified by depth, type and extent of injury
Every aspect
Classification
Burns are classified by depth, type and extent of injury
Every aspect
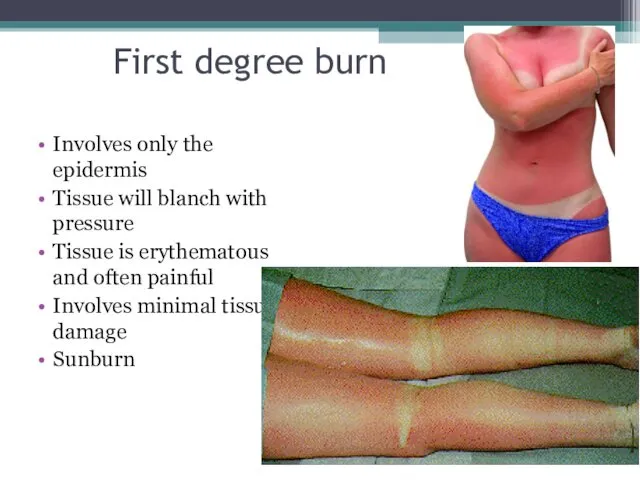
First degree burn
Involves only the epidermis
Tissue will blanch with pressure
Tissue
First degree burn
Involves only the epidermis
Tissue will blanch with pressure
Tissue
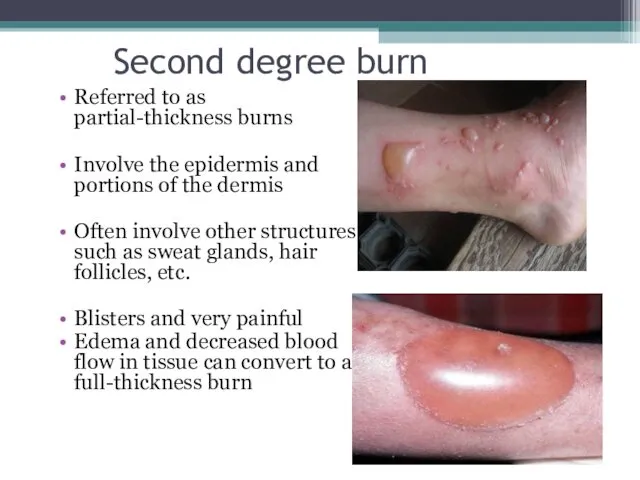
Second degree burn
Referred to as partial-thickness burns
Involve the epidermis and portions
Second degree burn
Referred to as partial-thickness burns
Involve the epidermis and portions
Third degree burn
Referred to as full-thickness burns
Charred skin or translucent white
Third degree burn
Referred to as full-thickness burns
Charred skin or translucent white
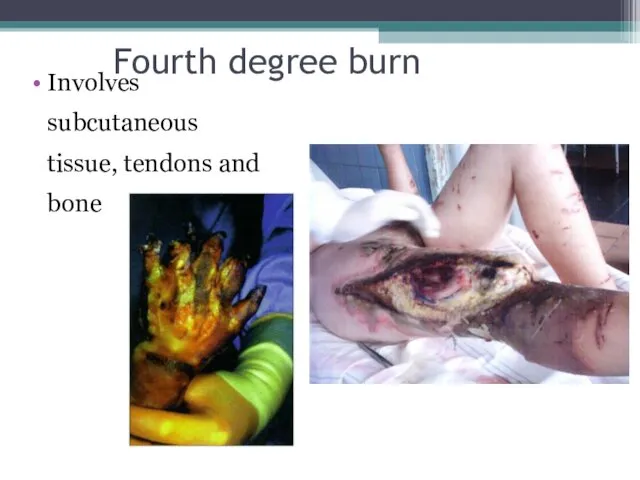
Fourth degree burn
Involves subcutaneous tissue, tendons and bone
Fourth degree burn
Involves subcutaneous tissue, tendons and bone
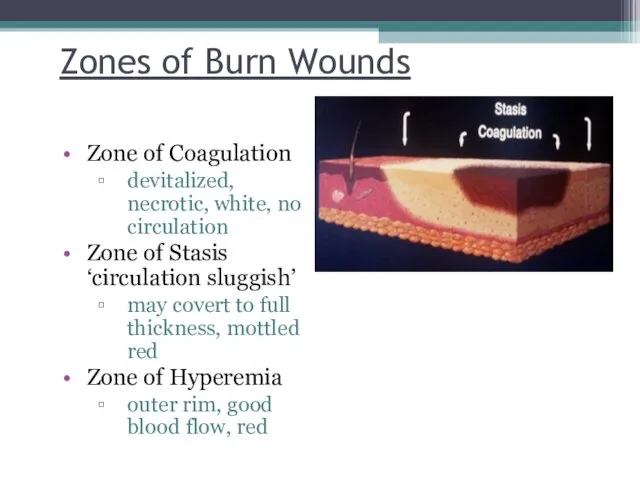
Zones of Burn Wounds
Zone of Coagulation
devitalized, necrotic, white, no circulation
Zone
Zones of Burn Wounds
Zone of Coagulation
devitalized, necrotic, white, no circulation
Zone
Burn extent
% BSA involved morbidity
Burn extent is calculated only on
Burn extent
% BSA involved morbidity
Burn extent is calculated only on
Measurement charts
Rule of Nines:
Quick estimate of percent of burn
Rule of Palms:
Good
Measurement charts
Rule of Nines:
Quick estimate of percent of burn
Rule of Palms:
Good
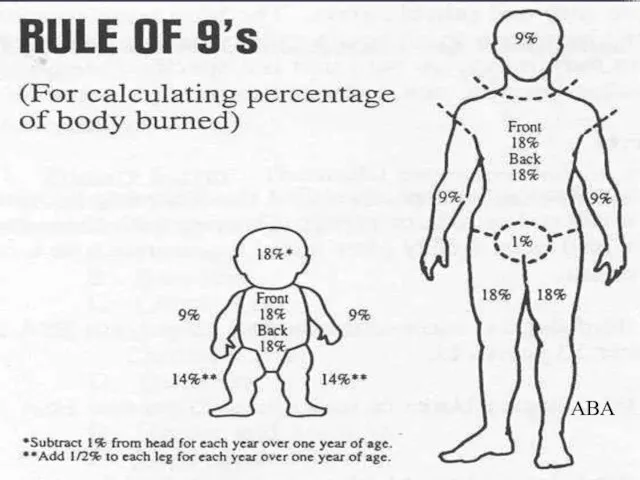
Rule of 9s
ABA
Rule of 9s
ABA
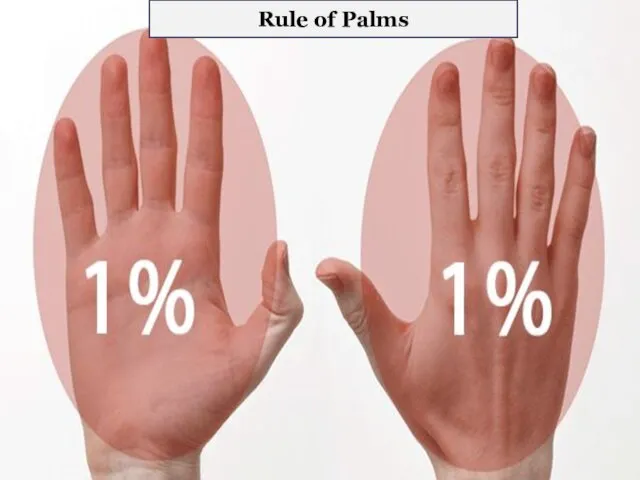
Rule of Palms
Rule of Palms
Lab studies
Severe burns:
CBC
Chemistry profile
Coagulation profile
creatine phosphokinase and urine myoglobin (with electrical injuries)
12
Lab studies
Severe burns:
CBC
Chemistry profile
Coagulation profile
creatine phosphokinase and urine myoglobin (with electrical injuries)
12
otolaryngologist
Neurologist
ophthalmologist
Fibrobronchoscopy
Examination by doctors
otolaryngologist
Neurologist
ophthalmologist
Fibrobronchoscopy
Examination by doctors
Imaging studies
X-Ray
Plain Films / CT scan: Dependent upon
history and physical
Imaging studies
X-Ray
Plain Films / CT scan: Dependent upon
history and physical
Criteria for burn center admission
Full-thickness > 5% BSA
Partial-thickness > 10% BSA
Any
Criteria for burn center admission
Full-thickness > 5% BSA
Partial-thickness > 10% BSA
Any
Initial patient treatment
Stop the burning process
Consider burn patient as a multiple
Initial patient treatment
Stop the burning process
Consider burn patient as a multiple
Details of the incident
Cause of the burn
Time of injury
Place of the
Details of the incident
Cause of the burn
Time of injury
Place of the
Care of small burns
What can YOU do?
Care of small burns
What can YOU do?
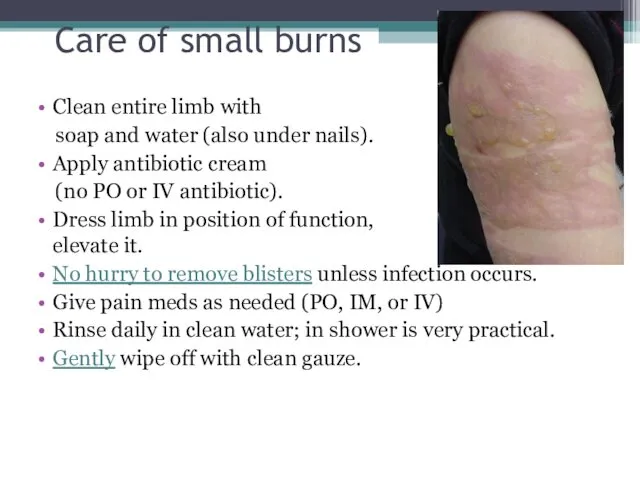
Care of small burns
Clean entire limb with
soap and water
Care of small burns
Clean entire limb with
soap and water
Blisters
In the pre-hospital setting, there is no hurry to remove blisters.
Blisters
In the pre-hospital setting, there is no hurry to remove blisters.
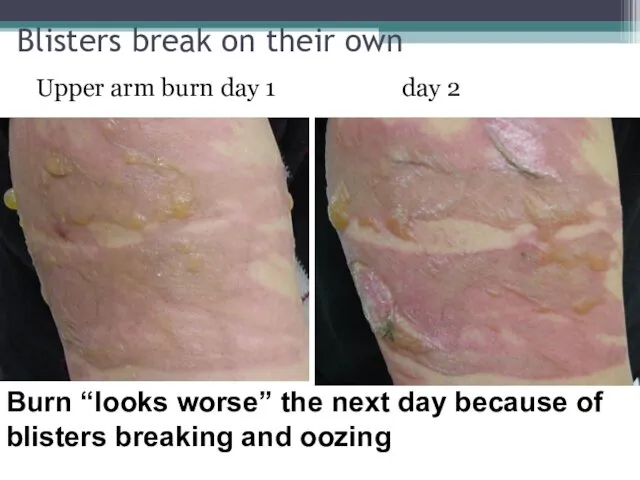
Blisters break on their own
Upper arm burn day 1 day 2
Burn
Blisters break on their own
Upper arm burn day 1 day 2
Burn
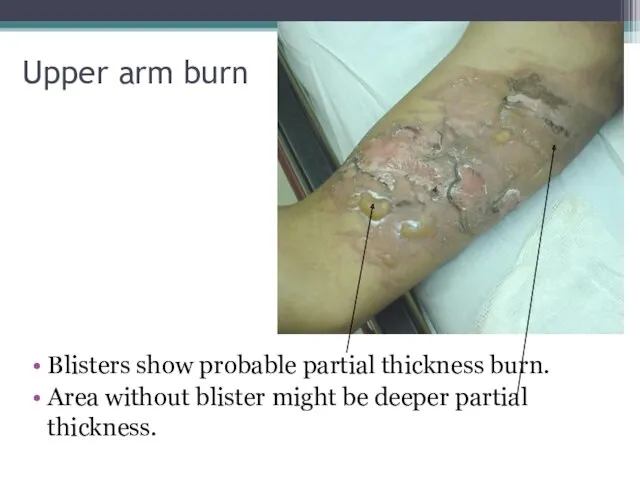
Upper arm burn
Blisters show probable partial thickness burn.
Area without blister might
Upper arm burn
Blisters show probable partial thickness burn.
Area without blister might

Debride blister using simple instruments
Debride blister using simple instruments

After debridement
After debridement
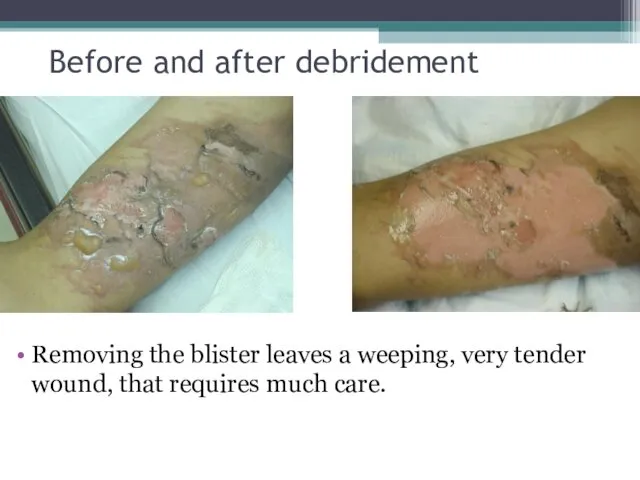
Before and after debridement
Removing the blister leaves a weeping, very tender
Before and after debridement
Removing the blister leaves a weeping, very tender
Silver sulfadiazene
Silver sulfadiazene
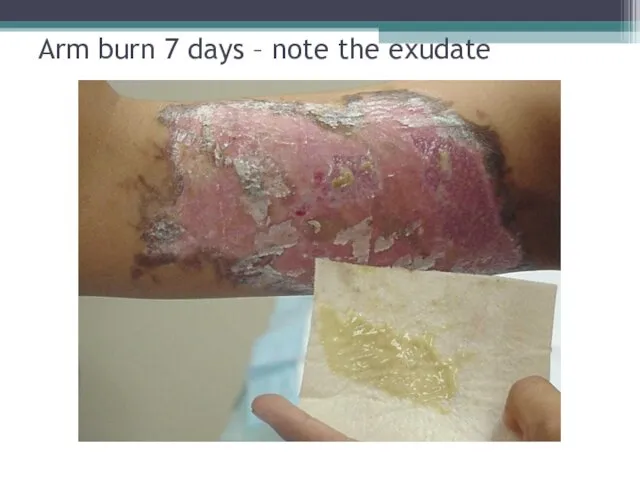
Arm burn 7 days – note the exudate
Arm burn 7 days – note the exudate
Burns of special areas
of the body
Face
Mouth
Neck
Hands
Burns of special areas
of the body
Face
Mouth
Neck
Hands
Face
Be VERY concerned for the airway!!
Eyelids, lips and ears often swell.
In
Face
Be VERY concerned for the airway!!
Eyelids, lips and ears often swell.
In
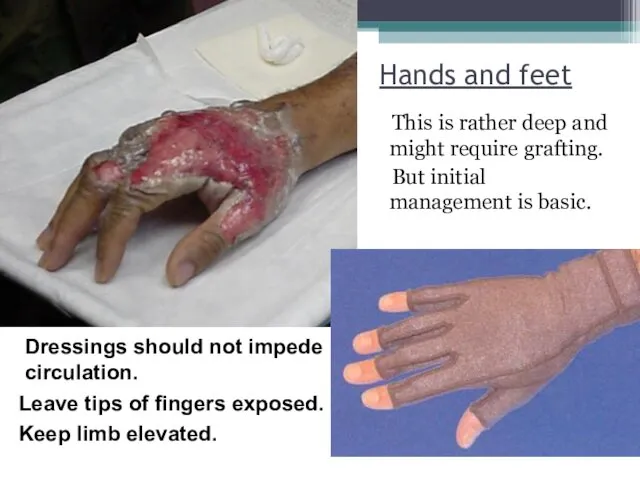
Hands and feet
This is rather deep and might require grafting.
Hands and feet
This is rather deep and might require grafting.
Hands and feet
Allow use of the hands in dressings by day.
Splint
Hands and feet
Allow use of the hands in dressings by day.
Splint
Hands and feet
Fingers might develop contractures if active measures are not
Hands and feet
Fingers might develop contractures if active measures are not
Genitalia
Shower daily, rinse off old cream, apply new cream.
Insert Foley catheter
Genitalia
Shower daily, rinse off old cream, apply new cream.
Insert Foley catheter

Large Burns
Large Burns
Causes of death in burn patients
Airway
Facial edema, and/or airway edema
Breathing
Toxic
Causes of death in burn patients
Airway
Facial edema, and/or airway edema
Breathing
Toxic
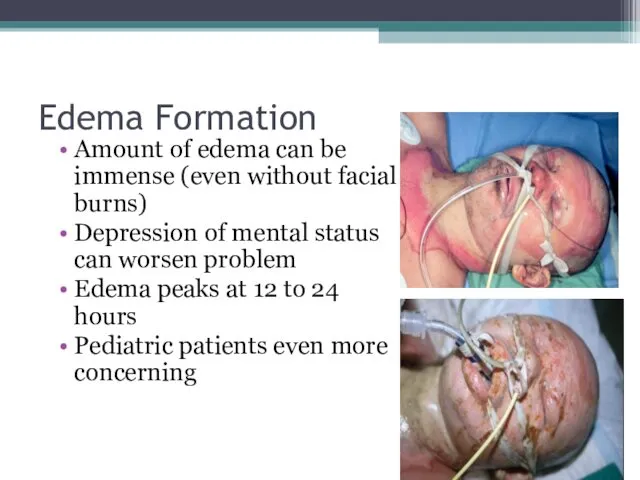
Edema Formation
Amount of edema can be immense (even without facial burns)
Depression
Edema Formation
Amount of edema can be immense (even without facial burns)
Depression
Causes of death in burn patients
Circulation: “failure of resuscitation”
Cardiovascular collapse, or
Causes of death in burn patients
Circulation: “failure of resuscitation”
Cardiovascular collapse, or
Patients with larger burns
First assess
CBA’s
“Disability” (brief neuro exam)
Later
Examine rest of patient
Calculate
Patients with larger burns
First assess
CBA’s
“Disability” (brief neuro exam)
Later
Examine rest of patient
Calculate
Airway considerations
Upper airway injury (above the glottis): Area buffers the heat
Airway considerations
Upper airway injury (above the glottis): Area buffers the heat
Criteria for intubation
Changes in voice
Wheezing / labored respirations
Excessive, continuous coughing
Altered
Criteria for intubation
Changes in voice
Wheezing / labored respirations
Excessive, continuous coughing
Altered
Ventilatory therapies
Rapid Sequence Intubation
Pain Management, Sedation and Paralysis
PEEP (positive end expiratory pressure)
High concentration oxygen
Avoid
Ventilatory therapies
Rapid Sequence Intubation
Pain Management, Sedation and Paralysis
PEEP (positive end expiratory pressure)
High concentration oxygen
Avoid
Ventilatory therapies
Burn patients with Acute respiratory distress syndrome (ARDS) requiring
PEEP (positive end expiratory pressure) >
Ventilatory therapies
Burn patients with Acute respiratory distress syndrome (ARDS) requiring
PEEP (positive end expiratory pressure) >
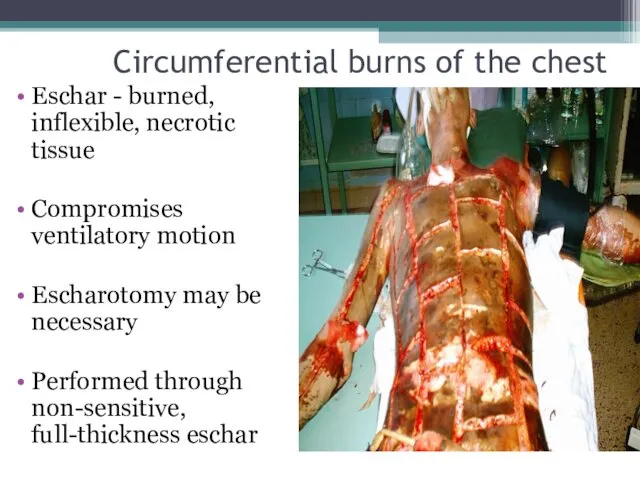
Circumferential burns of the chest
Eschar - burned, inflexible, necrotic tissue
Compromises
Circumferential burns of the chest
Eschar - burned, inflexible, necrotic tissue
Compromises
Carbon Monoxide Intoxication
Carbon monoxide has a binding affinity for hemoglobin which
Carbon Monoxide Intoxication
Carbon monoxide has a binding affinity for hemoglobin which
Signs and Symptoms of Carbon Monoxide Intoxication
Usually symptoms not present until
Signs and Symptoms of Carbon Monoxide Intoxication
Usually symptoms not present until
Signs and Symptoms of Carbon Monoxide Intoxication
Confused, irritable, restless
Headache
Tachycardia, arrhythmias or
Signs and Symptoms of Carbon Monoxide Intoxication
Confused, irritable, restless
Headache
Tachycardia, arrhythmias or
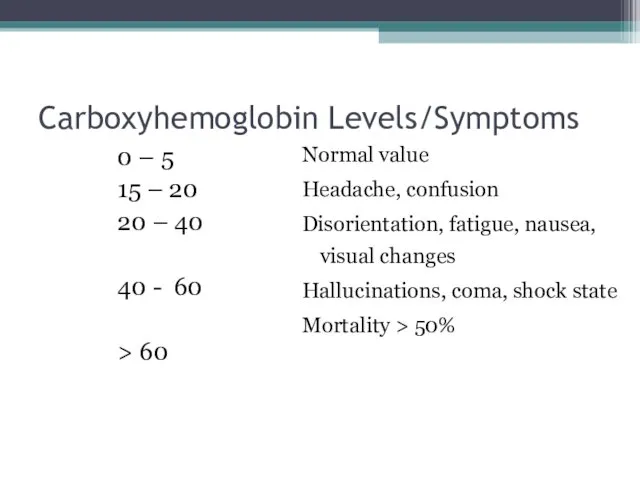
Carboxyhemoglobin Levels/Symptoms
0 – 5
15 – 20
20 – 40
40 - 60
> 60
Normal
Carboxyhemoglobin Levels/Symptoms
0 – 5
15 – 20
20 – 40
40 - 60
> 60
Normal
Management of Carbon Monoxide Intoxication
Remove patient from source of exposure.
Administer 100%
Management of Carbon Monoxide Intoxication
Remove patient from source of exposure.
Administer 100%
Circulation considerations
Formation of edema is the greatest initial volume loss
Burns 30%
Circulation considerations
Formation of edema is the greatest initial volume loss
Burns 30%
Circulation considerations
Capillary permeability increased
Protein molecules are now able to cross the
Circulation considerations
Capillary permeability increased
Protein molecules are now able to cross the
Circulation considerations
Loss of plasma volume is greatest during the first 4
Circulation considerations
Loss of plasma volume is greatest during the first 4
Fluid resuscitation
Goal: Maintain perfusion to vital organs
Based on the TBSA, body
Fluid resuscitation
Goal: Maintain perfusion to vital organs
Based on the TBSA, body
Fluid resuscitation
Lactated Ringers - preferred solution
Contains Na+ - restoration of Na+
Fluid resuscitation
Lactated Ringers - preferred solution
Contains Na+ - restoration of Na+
Fluid resuscitation
Burned patients have large insensible fluid losses
Fluid volumes may increase
Fluid resuscitation
Burned patients have large insensible fluid losses
Fluid volumes may increase
Fluid resuscitation
Fluid requirement calculations for infusion rates are based on the
Fluid resuscitation
Fluid requirement calculations for infusion rates are based on the
Assessing adequacy of resuscitation
Peripheral blood pressure: may be difficult to obtain
Urine
Assessing adequacy of resuscitation
Peripheral blood pressure: may be difficult to obtain
Urine
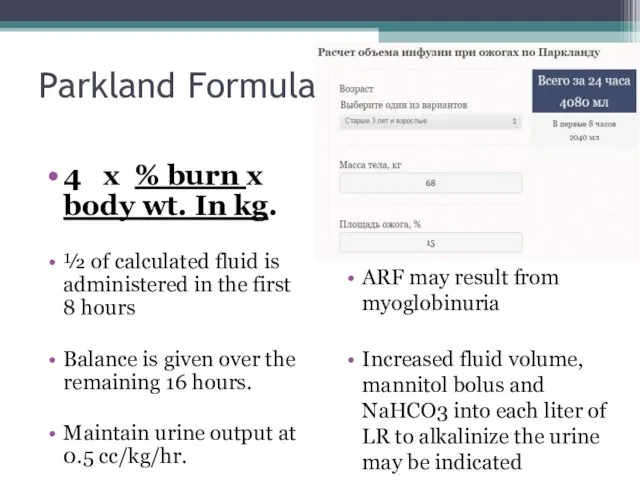
Parkland Formula
4 x % burn x body wt. In kg.
½ of
Parkland Formula
4 x % burn x body wt. In kg.
½ of
Effects of hypothermia
Hypothermia may lead to acidosis/coagulopathy
Hypothermia causes peripheral vasoconstriction and
Effects of hypothermia
Hypothermia may lead to acidosis/coagulopathy
Hypothermia causes peripheral vasoconstriction and
Prevention of hypothermia
Cover patients with a dry sheet – keep head
Prevention of hypothermia
Cover patients with a dry sheet – keep head
Pain management
Adequate analgesia imperative!
DOC: Morphine Sulfate
Dose: Adults: 0.1 – 0.2 mg/kg
Pain management
Adequate analgesia imperative!
DOC: Morphine Sulfate
Dose: Adults: 0.1 – 0.2 mg/kg
Antibiotics
Prophylactic antibiotics are not indicated
in the early postburn period.
Antibiotics
Prophylactic antibiotics are not indicated
in the early postburn period.
Other considerations
Check tetanus status – administer Td as appropriate
Debride and treat
Other considerations
Check tetanus status – administer Td as appropriate
Debride and treat
Electrical burns: are thermal injuries resulting from high intensity heat.
Electrical burns: are thermal injuries resulting from high intensity heat.
Chemical burns- Most often caused by strong acids or alkalis.
Chemical burns- Most often caused by strong acids or alkalis.
Burn Injury: Summary
Many risk factors age dependent
Pediatricians primary role: prevention
High risk
Burn Injury: Summary
Many risk factors age dependent
Pediatricians primary role: prevention
High risk
 Медициналық технологияны бағалау бойынша жұмыс:практикалық сұрақтар
Медициналық технологияны бағалау бойынша жұмыс:практикалық сұрақтар Микрохирургическое отделение. Объемно-планировочные решения зданий
Микрохирургическое отделение. Объемно-планировочные решения зданий Нерв жүйесі ауруларын диагностикалаудың нейровизуализациялық әдістері
Нерв жүйесі ауруларын диагностикалаудың нейровизуализациялық әдістері Гемостаз. Механизмы и патология
Гемостаз. Механизмы и патология Электрокардиография. Электрофизиологические основы ЭКГ
Электрокардиография. Электрофизиологические основы ЭКГ Вирусные гепатиты А, В, С, Д и Е
Вирусные гепатиты А, В, С, Д и Е Диареи у детей
Диареи у детей Национальные клинические руководства в Казахстане: история развития, структура и внедрения
Национальные клинические руководства в Казахстане: история развития, структура и внедрения Психотропные средства
Психотропные средства Ботулизм (ихтиизм)
Ботулизм (ихтиизм) Патология красной крови. Диагностика анемий. Терминология. Классификация
Патология красной крови. Диагностика анемий. Терминология. Классификация Выбор препарата 1-ой линии терапии для лечения больных распространённым почечно-клеточным раком
Выбор препарата 1-ой линии терапии для лечения больных распространённым почечно-клеточным раком Лечебная физическая культура
Лечебная физическая культура Патология терморегуляции. Лекция № 8
Патология терморегуляции. Лекция № 8 Понятие боли
Понятие боли Ревматоидный артрит
Ревматоидный артрит Биохимия костной ткани. Лекция № 4
Биохимия костной ткани. Лекция № 4 Паренхиматозные дистрофии
Паренхиматозные дистрофии ВИЧ-инфекция. Классификация, клиника, лечение
ВИЧ-инфекция. Классификация, клиника, лечение Периферическая венозная катетеризация
Периферическая венозная катетеризация Жүйке жүйесі мен тері жабындыларының туа біткен ақаулары
Жүйке жүйесі мен тері жабындыларының туа біткен ақаулары Современные подходы к лечению хронической сердечной недостаточности
Современные подходы к лечению хронической сердечной недостаточности Клиническая анатомия слабых мест передней брюшной стенки и диафрагмы
Клиническая анатомия слабых мест передней брюшной стенки и диафрагмы Ветеринарно-санітарна оцінка риби при філометроїдозі
Ветеринарно-санітарна оцінка риби при філометроїдозі Личная гигиена младшего школьника
Личная гигиена младшего школьника Действие массажа на кожу
Действие массажа на кожу Группа компаний Росгосстрах. Программа страхования Международная медицинская помощь
Группа компаний Росгосстрах. Программа страхования Международная медицинская помощь Защитные функции антител
Защитные функции антител