- Choose the Correct answer

Содержание
- 2. 2- As regard nephrotic syndrome a-Remission is defined as urine trace or negative for protein for
- 3. 3-As regard pyuria a-Defined as the presence of more than 5 leucocytes/hpf b- Always indicate the
- 4. 4-In acute poststreptococcal glomerulonephritis a-Follows infection of throat or skin by nephritogenic strains of group C
- 5. 5- As regard nephrotic syndrome a- Remission is defined as urine trace or negative for protein
- 6. 6- Charateristics of normal urine include a-PH is 9 b-RBCs are 5 – 7 / HPF
- 7. 7- As regard nephrotic syndrome a-Rapid response to steroids & absence of relapse in 1st six
- 8. 8- The most reliable diagnostic laboratory test diagnosing acute renal failure is a-Blood urea nitrogen b-Serum
- 9. 9- Diagnostic laboratory investigation associated with acute renal failure include a-hypophosphatemia b-hypernatremia c-metabolic alkalosis d-metaboloic acidosis
- 10. 10-As regard protein excretion in urine a- Normal protein excretion up to 40mg/m2/hr urine b-Nephrotic range
- 11. 11-As regard nephrotic syndrome a-Secondary nephrotic syndrome conistitute 90% of cases in children b-Minimal change disease
- 12. 12-As regard spot urine protein / creatinine ratio a- Its normal level in children less than
- 13. 13-AS regard urinary tract infction A-significant bacteruria is defined as bacterial count of the clean catch
- 14. 14-As regard diagnosis of urinary tract inection a-Urine culture shows 10,000 colonies of a single pathogen
- 15. 15-As regard hematuria: a-Microscopic hematuria is defined as the presence of 15 or more RBCs /
- 16. 16-In acute poststreptococcal glomerulonephritis a- Serum C3 level is decreased & returns normal 2 weeks after
- 17. 17-As regard treatment of urinary tract infection a-A 7 days course of a broad spectrum antibiotics
- 18. 18-As regard treatment of minimal change nephrotic syndrome a-Diet should be protein resricted b-Judicious use of
- 19. 19-As regad management of acute renal failure a-Protein in diet is normal b-Potassium intake is not
- 20. 20- Diagnostic laboratory investigations associated with acute renal failure include: a-Hypokalemia b-Hypercalcemia c-Anemia,thrombocytopenia,leucopenia d-Respiratory acidosis
- 21. 21- causes of acute post- renal failure a-Burns b-Glomerulonephritis c-Cyanotic congenital heart diseases d-Bilateral pelviureteric junction
- 22. 22-As regard nephrotic syndrome a-85% of idiopathic nephrotic syndrome is membranoproliferative b-Worest prognosis is associated with
- 23. a-Edema is due to increased plasma protein level b-Renin-angiotensin system activation has no role in etiology
- 24. 24- As regard diagnosis of minimal change nephrotic syndrome a-Renal biobsy is required for diagnosis in
- 25. 25-As regard complications of nephrotic syndrome a- Spontaneous peritonitis the most common type of infection and
- 26. False & True Systemic hypertension is a common complication of idiopathic nephrotic syndrome Generalized non pitting
- 27. Case Senario A 5 years old boy presenting with a one week history of generalized edema
- 28. Case senario 2 A 13 years old girl presenting with a 15 days history of generalized
- 29. Case senario 3 A 5 years old boy presenting with a 5 days history of cola-like
- 39. Скачать презентацию
2- As regard nephrotic syndrome
a-Remission is defined as urine trace or negative for
2- As regard nephrotic syndrome
a-Remission is defined as urine trace or negative for
3-As regard pyuria
a-Defined as the presence of more than 5
leucocytes/hpf
b-
3-As regard pyuria
a-Defined as the presence of more than 5
leucocytes/hpf
b-
4-In acute poststreptococcal glomerulonephritis
a-Follows infection of throat or skin by nephritogenic
strains
4-In acute poststreptococcal glomerulonephritis
a-Follows infection of throat or skin by nephritogenic
strains
5- As regard nephrotic syndrome
a- Remission is defined as urine trace or negative
5- As regard nephrotic syndrome
a- Remission is defined as urine trace or negative
6- Charateristics of normal urine include
a-PH is 9
b-RBCs are 5 – 7 /
6- Charateristics of normal urine include
a-PH is 9
b-RBCs are 5 – 7 /
7- As regard nephrotic syndrome
a-Rapid response to steroids & absence of relapse
7- As regard nephrotic syndrome
a-Rapid response to steroids & absence of relapse
8- The most reliable diagnostic laboratory test diagnosing acute renal failure is
a-Blood urea
8- The most reliable diagnostic laboratory test diagnosing acute renal failure is
a-Blood urea
9- Diagnostic laboratory investigation associated with acute renal failure include
a-hypophosphatemia
b-hypernatremia
c-metabolic alkalosis
d-metaboloic acidosis
9- Diagnostic laboratory investigation associated with acute renal failure include
a-hypophosphatemia
b-hypernatremia
c-metabolic alkalosis
d-metaboloic acidosis
10-As regard protein excretion in urine
a- Normal protein excretion up to 40mg/m2/hr urine
b-Nephrotic
10-As regard protein excretion in urine
a- Normal protein excretion up to 40mg/m2/hr urine
b-Nephrotic
11-As regard nephrotic syndrome
a-Secondary nephrotic syndrome conistitute 90% of
cases in children
b-Minimal change
11-As regard nephrotic syndrome
a-Secondary nephrotic syndrome conistitute 90% of
cases in children
b-Minimal change
12-As regard spot urine protein / creatinine ratio
a- Its normal level in
12-As regard spot urine protein / creatinine ratio
a- Its normal level in
13-AS regard urinary tract infction
A-significant bacteruria is defined as bacterial count
of the
13-AS regard urinary tract infction
A-significant bacteruria is defined as bacterial count
of the
14-As regard diagnosis of urinary tract inection
a-Urine culture shows 10,000 colonies of a
14-As regard diagnosis of urinary tract inection
a-Urine culture shows 10,000 colonies of a
15-As regard hematuria:
a-Microscopic hematuria is defined as the presence of 15 or more
15-As regard hematuria:
a-Microscopic hematuria is defined as the presence of 15 or more
16-In acute poststreptococcal glomerulonephritis
a- Serum C3 level is decreased & returns normal
16-In acute poststreptococcal glomerulonephritis
a- Serum C3 level is decreased & returns normal
17-As regard treatment of urinary tract
infection
a-A 7 days course of a broad
17-As regard treatment of urinary tract
infection
a-A 7 days course of a broad
18-As regard treatment of minimal change nephrotic
syndrome
a-Diet should be protein resricted
b-Judicious
18-As regard treatment of minimal change nephrotic
syndrome
a-Diet should be protein resricted
b-Judicious
19-As regad management of acute renal failure
a-Protein in diet is normal
b-Potassium intake is
19-As regad management of acute renal failure
a-Protein in diet is normal
b-Potassium intake is
20- Diagnostic laboratory investigations associated with acute renal failure include:
a-Hypokalemia
b-Hypercalcemia
c-Anemia,thrombocytopenia,leucopenia
d-Respiratory acidosis
20- Diagnostic laboratory investigations associated with acute renal failure include:
a-Hypokalemia
b-Hypercalcemia
c-Anemia,thrombocytopenia,leucopenia
d-Respiratory acidosis
21- causes of acute post- renal failure
a-Burns
b-Glomerulonephritis
c-Cyanotic congenital heart diseases
d-Bilateral pelviureteric junction
obstruction
21- causes of acute post- renal failure
a-Burns
b-Glomerulonephritis
c-Cyanotic congenital heart diseases
d-Bilateral pelviureteric junction
obstruction
22-As regard nephrotic syndrome
a-85% of idiopathic nephrotic syndrome is
membranoproliferative
b-Worest prognosis is associated
22-As regard nephrotic syndrome
a-85% of idiopathic nephrotic syndrome is
membranoproliferative
b-Worest prognosis is associated
a-Edema is due to increased plasma protein level
b-Renin-angiotensin system activation has no role
a-Edema is due to increased plasma protein level
b-Renin-angiotensin system activation has no role
24- As regard diagnosis of minimal change nephrotic
syndrome
a-Renal biobsy is required for
24- As regard diagnosis of minimal change nephrotic
syndrome
a-Renal biobsy is required for
25-As regard complications of nephrotic syndrome
a- Spontaneous peritonitis the most common type of
25-As regard complications of nephrotic syndrome
a- Spontaneous peritonitis the most common type of
False & True
Systemic hypertension is a common complication of idiopathic nephrotic syndrome
Generalized non
False & True
Systemic hypertension is a common complication of idiopathic nephrotic syndrome
Generalized non
Case Senario
A 5 years old boy presenting with a one week history of
Case Senario
A 5 years old boy presenting with a one week history of
Case senario 2
A 13 years old girl presenting with a 15 days history
Case senario 2
A 13 years old girl presenting with a 15 days history
Case senario 3
A 5 years old boy presenting with a 5 days history
Case senario 3
A 5 years old boy presenting with a 5 days history





 СПИД
СПИД Кавернозный туберкулёз
Кавернозный туберкулёз Дослідження хворих тварин з ураженням очей. Методи дослідження очей
Дослідження хворих тварин з ураженням очей. Методи дослідження очей Особенности аппаратной чистки лица
Особенности аппаратной чистки лица Введение в курс нормальной анатомии
Введение в курс нормальной анатомии Раны и раневой процесс, лечение ран
Раны и раневой процесс, лечение ран Гепатит B
Гепатит B Нарушения менструального цикла
Нарушения менструального цикла Альбинизм. Причины альбинизма
Альбинизм. Причины альбинизма Нервно-психическое развитие детей в связи с анатомо-физиологическими особенностями ЦНС
Нервно-психическое развитие детей в связи с анатомо-физиологическими особенностями ЦНС Demodex Mites
Demodex Mites Санкт-Петербургское государственное бюджетное учреждение здравоохранения Николаевская больница
Санкт-Петербургское государственное бюджетное учреждение здравоохранения Николаевская больница Норма и отклонение в физическом, психическом, интеллектуальном, речевом и сенсорном развитии ребенка
Норма и отклонение в физическом, психическом, интеллектуальном, речевом и сенсорном развитии ребенка Классификация раннего детского аутизма по Никольской О.С
Классификация раннего детского аутизма по Никольской О.С Гинекологиялық ауруларды тексеру әдістері
Гинекологиялық ауруларды тексеру әдістері Гидрокинезотерапия-гидротерапия
Гидрокинезотерапия-гидротерапия Гипогалактия дәрежелері, диагностикасы, емі, алдын алуы. Лактациялық криздерді шешу шаралары
Гипогалактия дәрежелері, диагностикасы, емі, алдын алуы. Лактациялық криздерді шешу шаралары Правила формулировки диагноза
Правила формулировки диагноза Влияние никотина и алкоголя на организм беременной женщины
Влияние никотина и алкоголя на организм беременной женщины Особенности кодирования медицинской помощи в 2020 году
Особенности кодирования медицинской помощи в 2020 году Сердечные гликозиды. Общая характеристика, методы выделения, анализ. (Тема 7)
Сердечные гликозиды. Общая характеристика, методы выделения, анализ. (Тема 7) Судебно-медицинская токсикология. Повреждения от действия отравляющих веществ
Судебно-медицинская токсикология. Повреждения от действия отравляющих веществ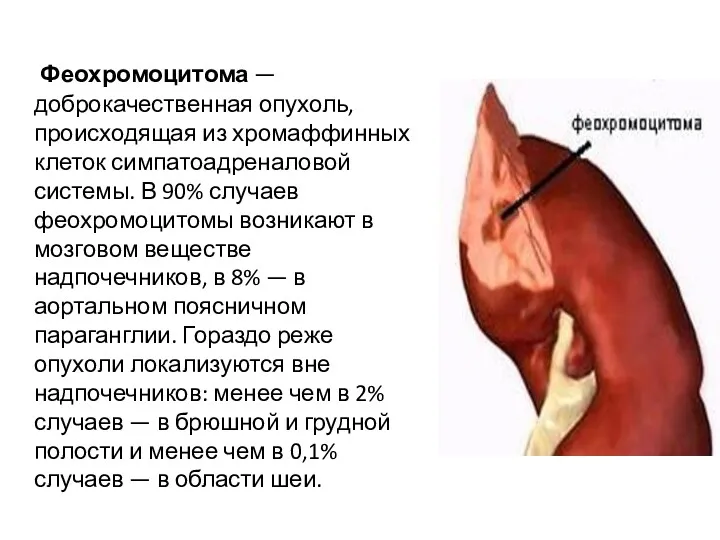 Доброкачественная опухоль феохромоцитома
Доброкачественная опухоль феохромоцитома Принципы профилактики аномалий и деформаций челюстно-лицевой области в детском возрасте
Принципы профилактики аномалий и деформаций челюстно-лицевой области в детском возрасте Чума. Симптомы. Клиника. Лечение
Чума. Симптомы. Клиника. Лечение Туберкулёз. Профилактика. Лечение
Туберкулёз. Профилактика. Лечение Клиническая фармация антибактериальных лекарственных препаратов. Принципы антибактериальной терапии
Клиническая фармация антибактериальных лекарственных препаратов. Принципы антибактериальной терапии Олимпиада по хирургии
Олимпиада по хирургии