- Chronic kidney disease

Содержание
- 2. Chronic kidney disease – it is a damage of the kidneys, or a decrease their function
- 3. Risk factors and progression of CKD
- 4. Diabetes of stroke
- 5. International classification of stages of CKD
- 6. The value of GFR In clinical practice GFR is calculated by special formulas based on the
- 7. The main pathogenetic mechanism of CKD is a progressive decrease in the number of active nephrons,
- 8. patient complains about Weakness, loss of appetite; a constant thirst; aversion to meat food; Dyspeptic disorders
- 9. Physical examination There are no visible signs in the stage of CKD I-III. In the IV-V
- 10. changes in respiratory and cardiovascular systems hematologic disorders disorders of the gastrointestinal tract endocrine disorders skin
- 11. CKD is an independent risk factor of cardiovascular complications
- 12. PLAN OF THE PATIENT'S SURVEY
- 13. Markers of kidney damage Changes in general urine analysis- Proteinuria, increased albuminuria Changes in urinary sediment
- 14. Proteinuria tests The most sensitive and accurate are the colorimetric methods for determining the total urine
- 15. The most complete information on the composition of urine proteins is provided by the uroproteinogram, a
- 16. NB! Diagnostic criteria a) clinico-laboratory (primarily, increased albuminuria / proteinuria), confirmed by repeated studies and saved
- 17. Basic principles of treatment Preparations of iron Calcium carbonate, vitamin D3
- 18. Diet: In the initial stage of CRF - table number 7 In patients who are on
- 19. Correction of arterial hypertension Arterial hypertension (AH) is one of the most important independent risk factors
- 20. TEN "GOLD RULES", allowing to keep the kidneys healthy 1. Do not abuse salt and meat.
- 22. Скачать презентацию
Chronic kidney disease – it is a damage of the kidneys,
Chronic kidney disease – it is a damage of the kidneys,
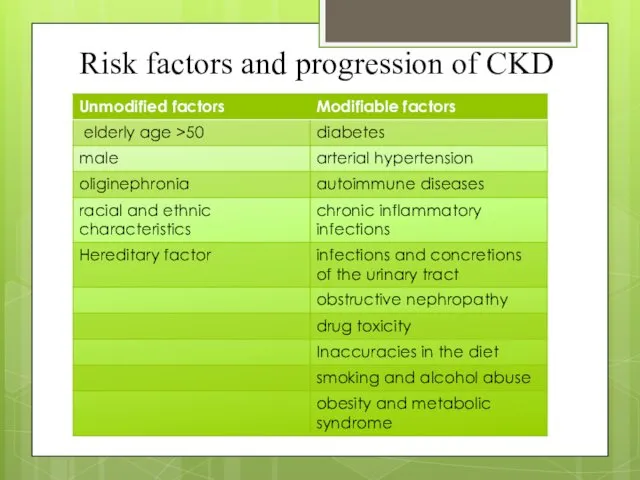
Risk factors and progression of CKD
Risk factors and progression of CKD
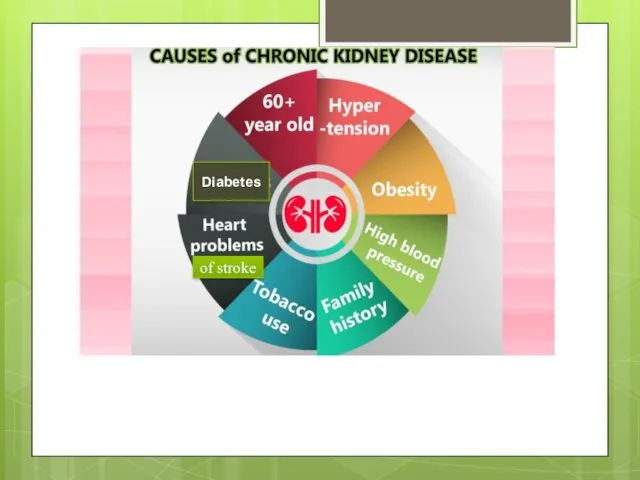
Diabetes
of stroke
Diabetes
of stroke
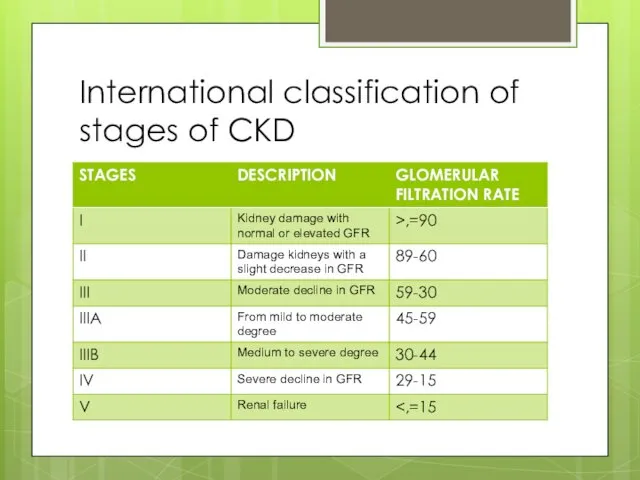
International classification of stages of CKD
International classification of stages of CKD
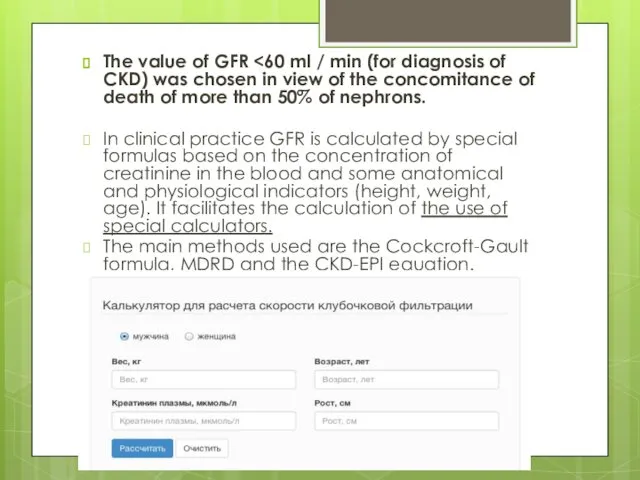
The value of GFR <60 ml / min (for diagnosis of
The value of GFR <60 ml / min (for diagnosis of
The main pathogenetic mechanism of CKD is a progressive decrease in
The main pathogenetic mechanism of CKD is a progressive decrease in
patient complains about
Weakness, loss of appetite;
a constant thirst;
aversion to meat
patient complains about
Weakness, loss of appetite;
a constant thirst;
aversion to meat
Physical examination
There are no visible signs in the stage of CKD
Physical examination
There are no visible signs in the stage of CKD
changes in respiratory and cardiovascular systems
hematologic disorders
disorders of the gastrointestinal tract
endocrine
changes in respiratory and cardiovascular systems
hematologic disorders
disorders of the gastrointestinal tract
endocrine
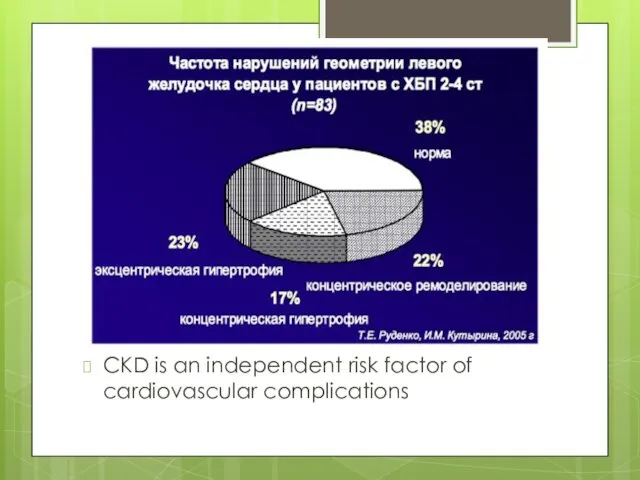
CKD is an independent risk factor of cardiovascular complications
CKD is an independent risk factor of cardiovascular complications
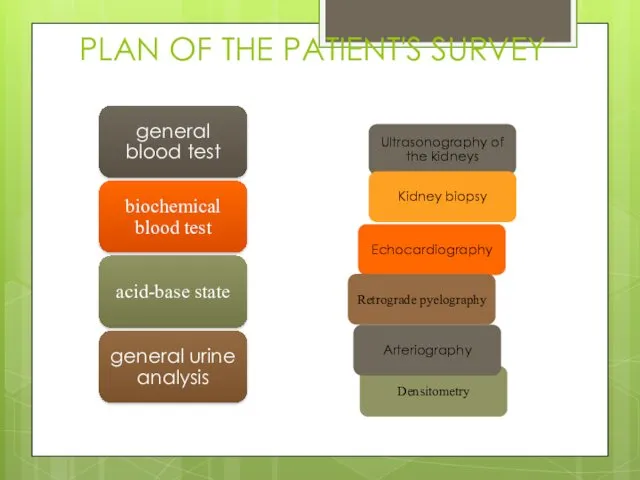
PLAN OF THE PATIENT'S SURVEY
PLAN OF THE PATIENT'S SURVEY
Markers of kidney damage
Changes in general urine analysis- Proteinuria, increased albuminuria
Changes
Markers of kidney damage
Changes in general urine analysis- Proteinuria, increased albuminuria
Changes
Proteinuria tests
The most sensitive and accurate are the colorimetric methods for
Proteinuria tests
The most sensitive and accurate are the colorimetric methods for
The most complete information on the composition of urine proteins is
The most complete information on the composition of urine proteins is
NB!
Diagnostic criteria
a) clinico-laboratory (primarily, increased albuminuria / proteinuria), confirmed by repeated
NB!
Diagnostic criteria
a) clinico-laboratory (primarily, increased albuminuria / proteinuria), confirmed by repeated
Basic principles of treatment
Preparations of iron
Calcium carbonate, vitamin D3
Basic principles of treatment
Preparations of iron
Calcium carbonate, vitamin D3
Diet:
In the initial stage of CRF - table number 7
In patients
Diet:
In the initial stage of CRF - table number 7
In patients
Correction of arterial hypertension
Arterial hypertension (AH) is one of the most
Correction of arterial hypertension
Arterial hypertension (AH) is one of the most
TEN "GOLD RULES", allowing to keep the kidneys healthy
1. Do not
TEN "GOLD RULES", allowing to keep the kidneys healthy
1. Do not
 Неотложная помощь при тяжелых приступах бронхиальной астмы
Неотложная помощь при тяжелых приступах бронхиальной астмы Генные заболевания
Генные заболевания Ісікке қарсы препараттардың клиникалық фармакологиясы
Ісікке қарсы препараттардың клиникалық фармакологиясы Неинвазивные методы диагностики кожи
Неинвазивные методы диагностики кожи Анализ работы фельдшерско - акушерских пунктов Кировской области, 2016
Анализ работы фельдшерско - акушерских пунктов Кировской области, 2016 Антипротозойные ЛС. Противоглистные ЛС
Антипротозойные ЛС. Противоглистные ЛС Местное и общее обезболивание
Местное и общее обезболивание Антиадренергиялық заттар
Антиадренергиялық заттар Современные методы диагностики и лечения гастрошизиса и эмбриональных грыж у детей
Современные методы диагностики и лечения гастрошизиса и эмбриональных грыж у детей The heart sounds
The heart sounds Здравоохранение как социальный институт
Здравоохранение как социальный институт Приобретенные пороки сердца
Приобретенные пороки сердца Значение двигательной активности и закаливание организма
Значение двигательной активности и закаливание организма Пневмонии и рак легких
Пневмонии и рак легких Антитромбоцитарные препараты
Антитромбоцитарные препараты Роды при поперечных и косых положениях плода
Роды при поперечных и косых положениях плода Сестринское обследование пациентов с заболеваниями желудочно-кишечного тракта
Сестринское обследование пациентов с заболеваниями желудочно-кишечного тракта Современные технологии обработки информации. Концепция информатизации здравоохранения. (Тема 7)
Современные технологии обработки информации. Концепция информатизации здравоохранения. (Тема 7) Иммунитет. Система гемостаза
Иммунитет. Система гемостаза Массаж при нарушениях обмена веществ. (Тема 5.8)
Массаж при нарушениях обмена веществ. (Тема 5.8) Инфекционный эндокардит у детей
Инфекционный эндокардит у детей Электрокардиограмма при гипертрофии различных отделов сердца
Электрокардиограмма при гипертрофии различных отделов сердца Энцефалопатия Балалардың церебралдық салдары
Энцефалопатия Балалардың церебралдық салдары Психологические особенности женщин на этапе подготовки ЭКО (психоаналитический подход)
Психологические особенности женщин на этапе подготовки ЭКО (психоаналитический подход) Клостридиозы овец
Клостридиозы овец Лабораторная диагностика коронавирусной инфекции COVID-19
Лабораторная диагностика коронавирусной инфекции COVID-19 Генные болезни
Генные болезни Отравления веществами наркотического действия. Клиника, диагностика, лечение
Отравления веществами наркотического действия. Клиника, диагностика, лечение