- Colorectal Cancer

Содержание
- 2. Top 10 Cancer Types and Colorectal Statistics in the US The third most common cancer in
- 3. Anatomy of the Colon and Rectum The colon has four sections: ascending, transverse, descending, and sigmoid
- 4. Colorectal Cancer Development Colorectal cancer refers to cancer originating in the colon or rectum and can
- 5. TNM system Primary tumor (T) Regional lymph nodes (N) Distant metastasis (M) Staging of CRC
- 6. T Staging-American Joint Committee on Cancer system (AJCC/TNM) T Categories: Describes the extent of spread of
- 7. N and M Staging-American Joint Committee on Cancer system (AJCC/TNM) N categories: describes the absence or
- 8. Staging-American Joint Committee on Cancer system (AJCC/TNM) Staging is an indicator of survival Stage grouping: From
- 9. Staging of colorectal cancer
- 10. Staging of colorectal cancer
- 11. 90 % cancers arise from polyps polyp – cancer 8 – 10 yrs
- 12. Symptoms of Colorectal Cancer Early colon cancer usually presents with no symptoms. Symptoms appear with more
- 13. Typical sites of incidence and sympoms of colon cancer
- 14. Sites of metastasis Liver Lung Brain Bones Via blood Lymph nodes Abdominal wall Nerves Vessels Via
- 15. Risk Factors
- 16. Risk Factors (cont’d)
- 17. Risk factors – Hereditary Family Syndromes The development of colorectal cancer is a multi-step process involving
- 18. Familial Adenomatous Polyposis (FAP) FAP: Multiple colonic polyps Patients with an APC mutation have a 100%
- 19. Juvenile Polyposis Syndrome (JP) Juvenile Polyposis: -occurs in children with sporadic juvenile polyps (benign and isolated,
- 20. Lynch Syndrome (also known as HNPCC) Lynch syndrome: Also known as hereditary nonpolyposis colorectal cancer (HNPCC)
- 21. Factors that may reduce risk
- 22. Screening Medical History and Physical Exam: A history (symptoms and risk factors) and DRE (digital rectal
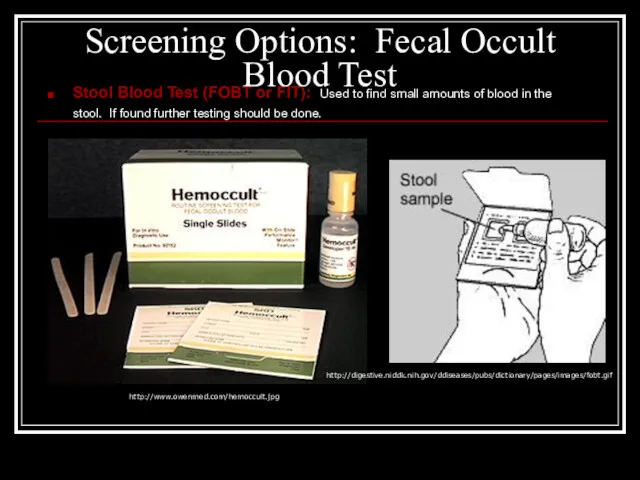
- 23. Screening Options: Fecal Occult Blood Test Stool Blood Test (FOBT or FIT): Used to find small
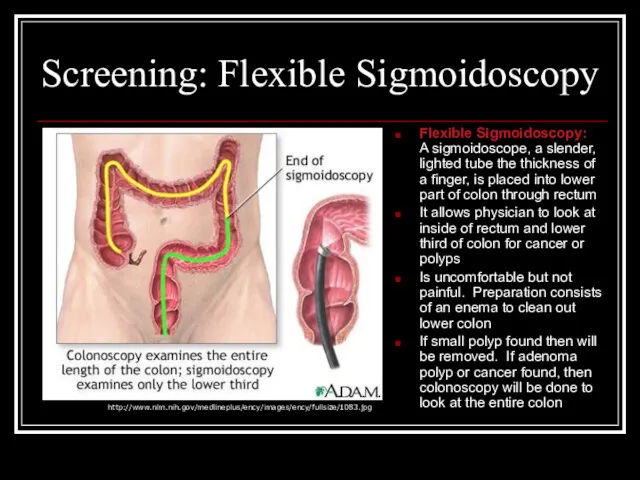
- 24. Screening: Flexible Sigmoidoscopy Flexible Sigmoidoscopy: A sigmoidoscope, a slender, lighted tube the thickness of a finger,
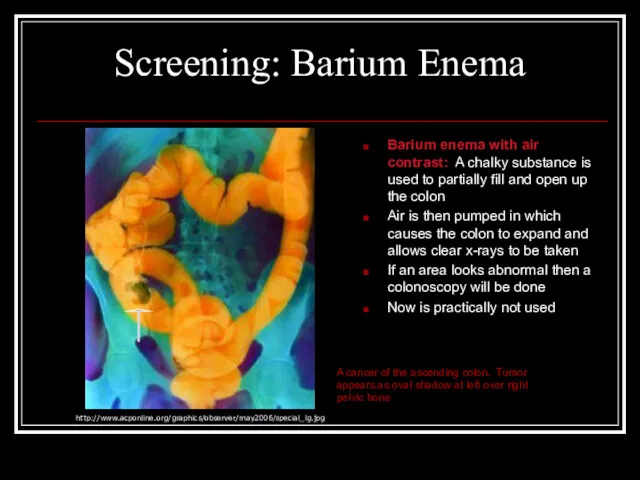
- 25. Screening: Barium Enema Barium enema with air contrast: A chalky substance is used to partially fill
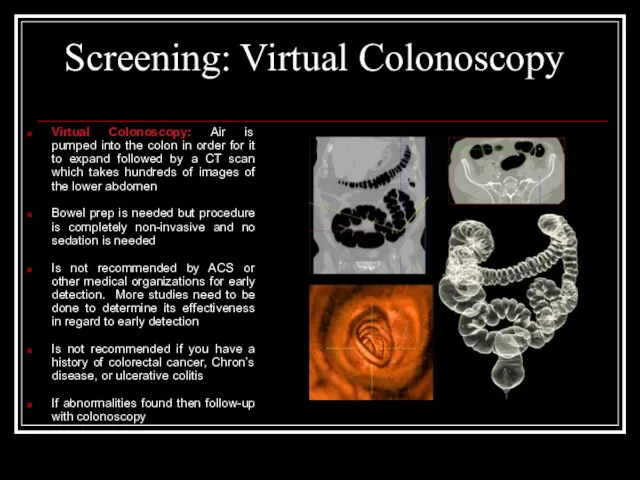
- 26. Screening: Virtual Colonoscopy Virtual Colonoscopy: Air is pumped into the colon in order for it to
- 27. Screening: Colonoscopy Colonoscopy: A colonoscope, a long, flexible, lighted tube about the thickness of a finger,
- 28. Screening Guidelines, Advantages, and Disadvantages *American Cancer Society Recommendation
- 30. Скачать презентацию
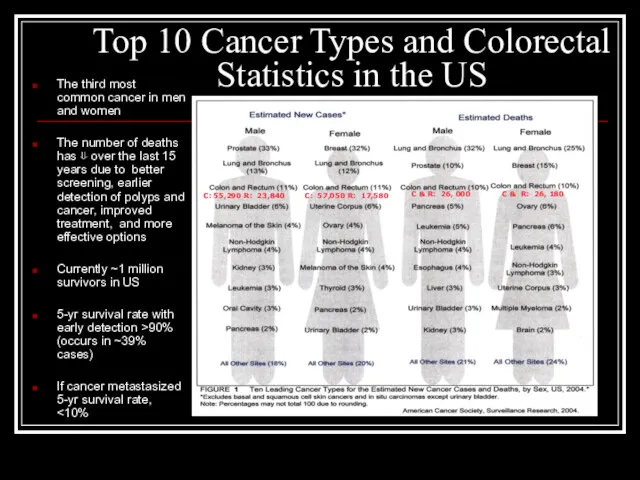
Top 10 Cancer Types and Colorectal Statistics in the US
The third
Top 10 Cancer Types and Colorectal Statistics in the US
The third
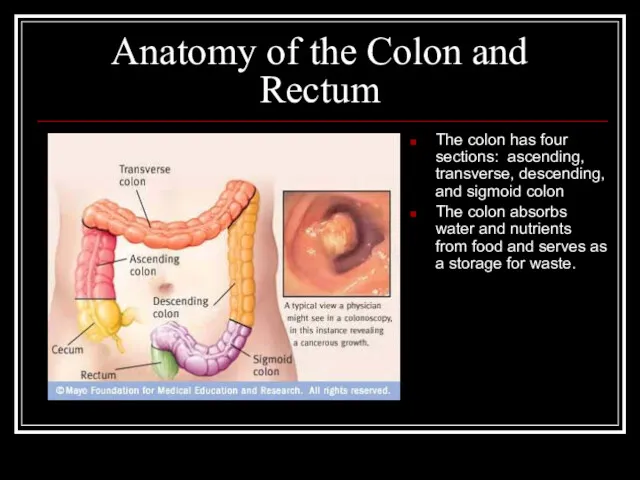
Anatomy of the Colon and Rectum
The colon has four sections: ascending,
Anatomy of the Colon and Rectum
The colon has four sections: ascending,
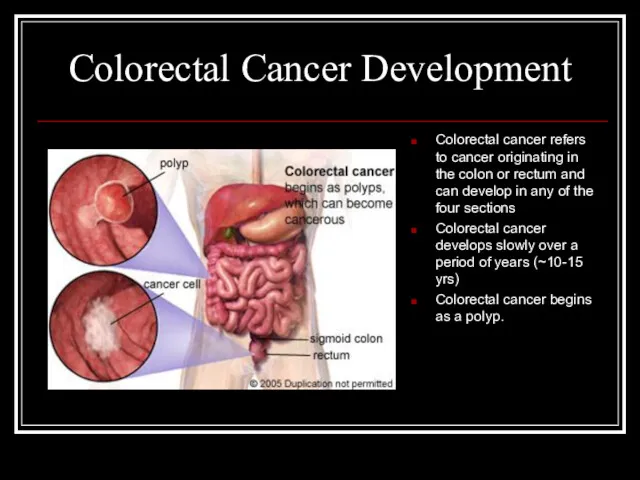
Colorectal Cancer Development
Colorectal cancer refers to cancer originating in the colon
Colorectal Cancer Development
Colorectal cancer refers to cancer originating in the colon
TNM system
Primary tumor (T)
Regional lymph nodes (N)
Distant metastasis (M)
Staging of
TNM system
Primary tumor (T)
Regional lymph nodes (N)
Distant metastasis (M)
Staging of
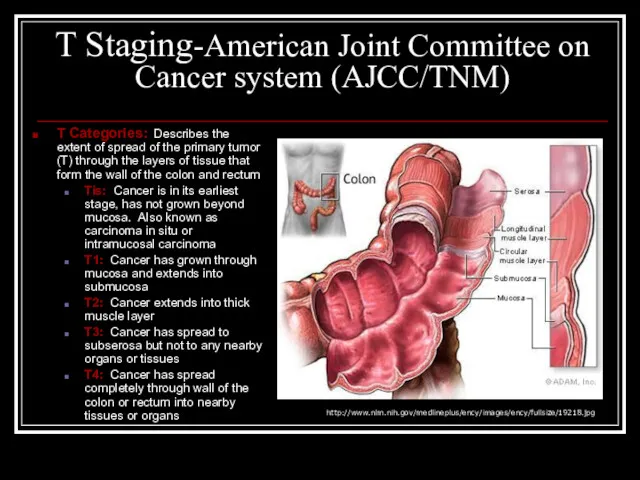
T Staging-American Joint Committee on Cancer system (AJCC/TNM)
T Categories: Describes the
T Staging-American Joint Committee on Cancer system (AJCC/TNM)
T Categories: Describes the
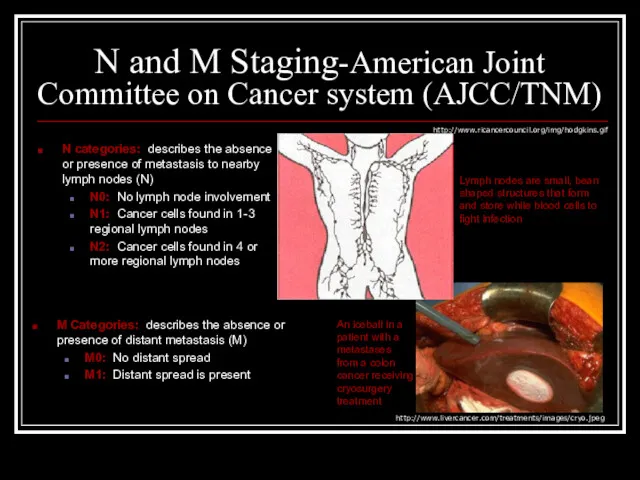
N and M Staging-American Joint Committee on Cancer system (AJCC/TNM)
N categories:
N and M Staging-American Joint Committee on Cancer system (AJCC/TNM)
N categories:
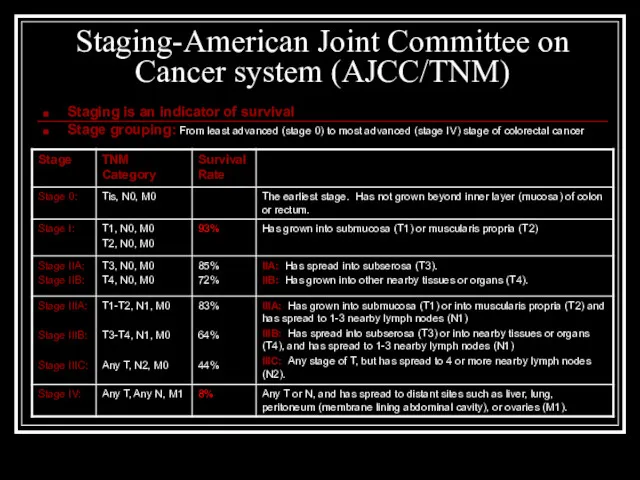
Staging-American Joint Committee on Cancer system (AJCC/TNM)
Staging is an indicator of
Staging-American Joint Committee on Cancer system (AJCC/TNM)
Staging is an indicator of
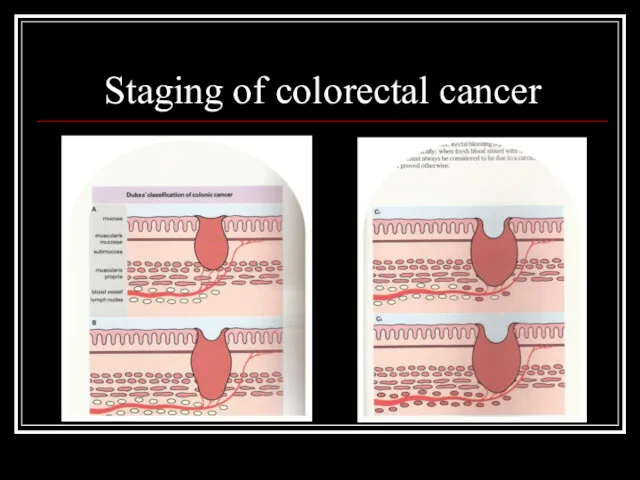
Staging of colorectal cancer
Staging of colorectal cancer
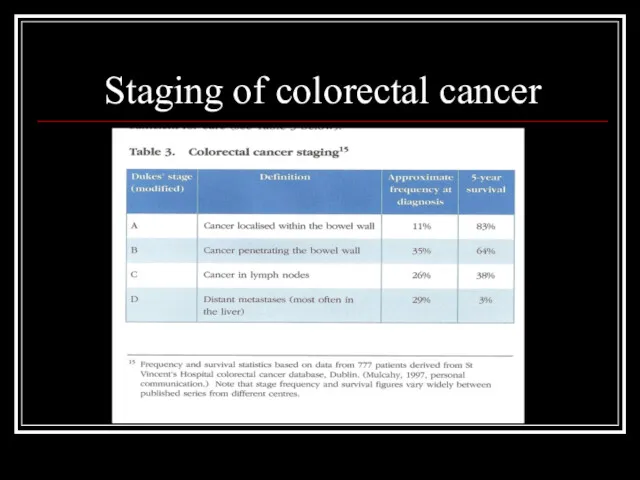
Staging of colorectal cancer
Staging of colorectal cancer
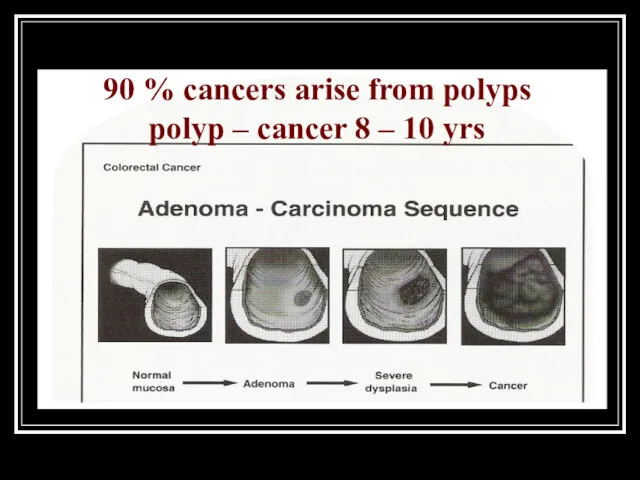
90 % cancers arise from polyps
polyp – cancer 8 – 10
90 % cancers arise from polyps polyp – cancer 8 – 10
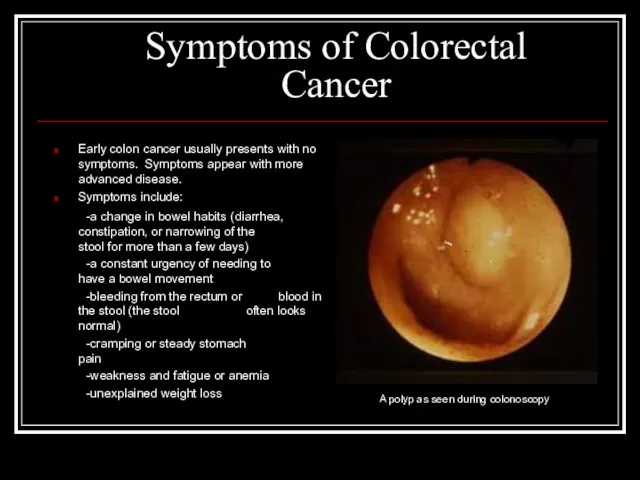
Symptoms of Colorectal Cancer
Early colon cancer usually presents with no symptoms.
Symptoms of Colorectal Cancer
Early colon cancer usually presents with no symptoms.
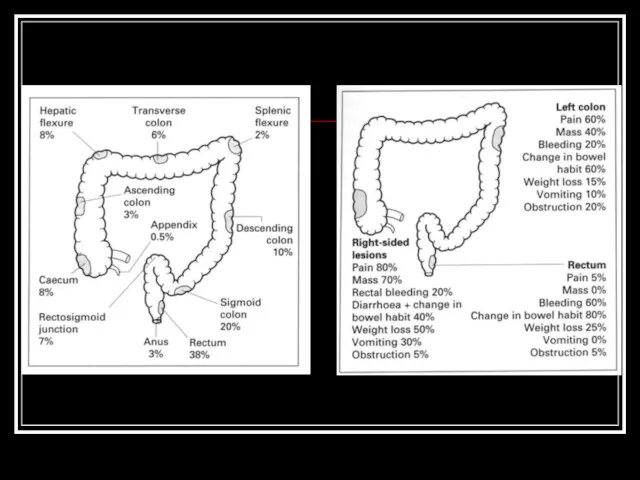
Typical sites of incidence and sympoms of colon cancer
Typical sites of incidence and sympoms of colon cancer
Sites of metastasis
Liver
Lung
Brain
Bones
Via blood
Lymph nodes
Abdominal wall
Nerves
Vessels
Via lymphatics
Per continuitatem
Sites of metastasis
Liver
Lung
Brain
Bones
Via blood
Lymph nodes
Abdominal wall
Nerves
Vessels
Via lymphatics
Per continuitatem
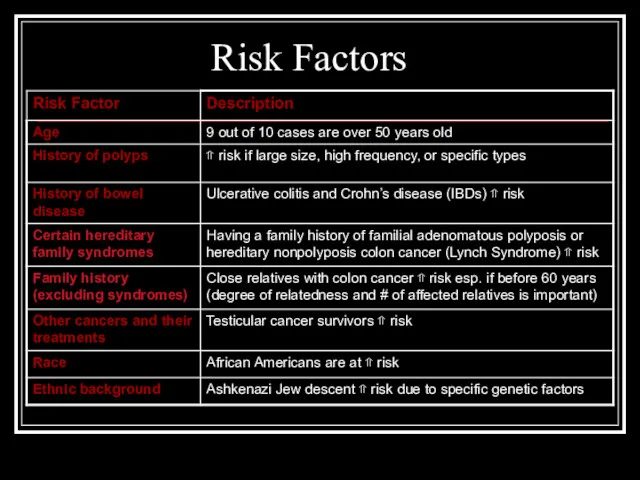
Risk Factors
Risk Factors

Risk Factors (cont’d)
Risk Factors (cont’d)
Risk factors – Hereditary Family Syndromes
The development of colorectal cancer is
Risk factors – Hereditary Family Syndromes
The development of colorectal cancer is
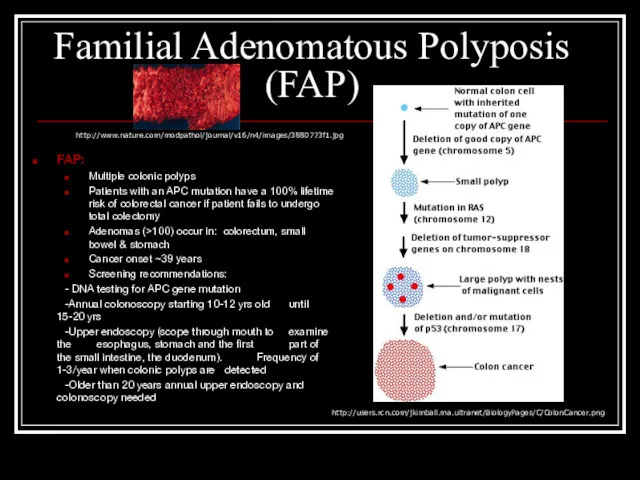
Familial Adenomatous Polyposis (FAP)
FAP:
Multiple colonic polyps
Patients with an APC mutation
Familial Adenomatous Polyposis (FAP)
FAP:
Multiple colonic polyps
Patients with an APC mutation
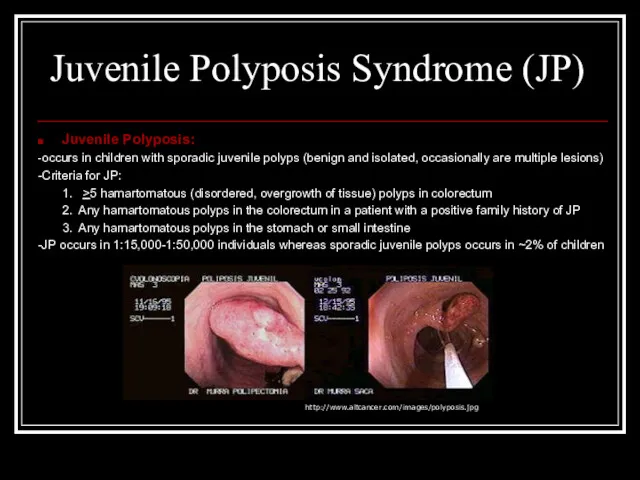
Juvenile Polyposis Syndrome (JP)
Juvenile Polyposis:
-occurs in children with sporadic juvenile polyps
Juvenile Polyposis Syndrome (JP)
Juvenile Polyposis:
-occurs in children with sporadic juvenile polyps
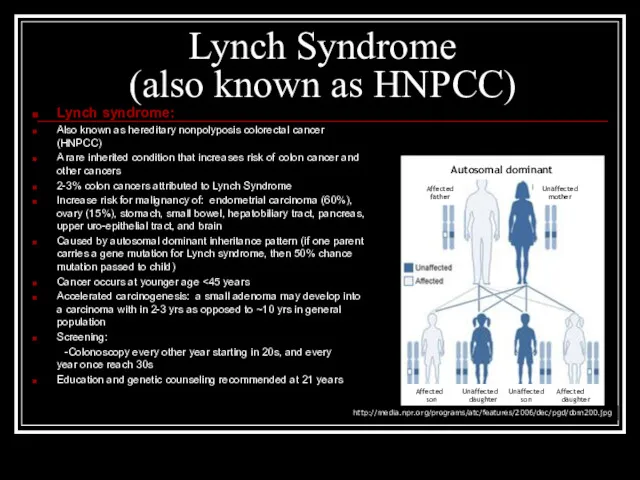
Lynch Syndrome
(also known as HNPCC)
Lynch syndrome:
Also known as hereditary
Lynch Syndrome
(also known as HNPCC)
Lynch syndrome:
Also known as hereditary
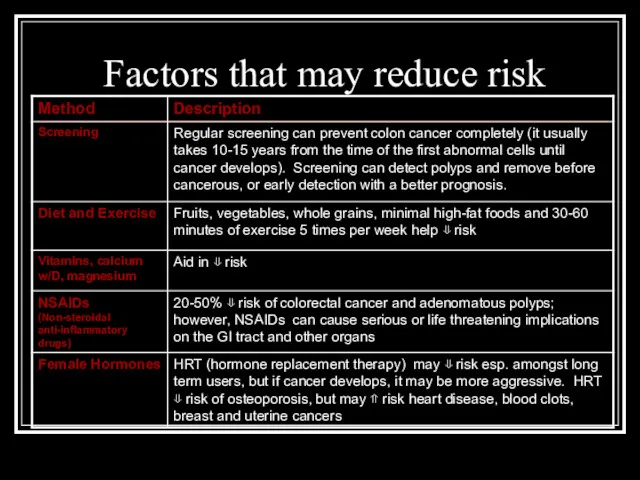
Factors that may reduce risk
Factors that may reduce risk
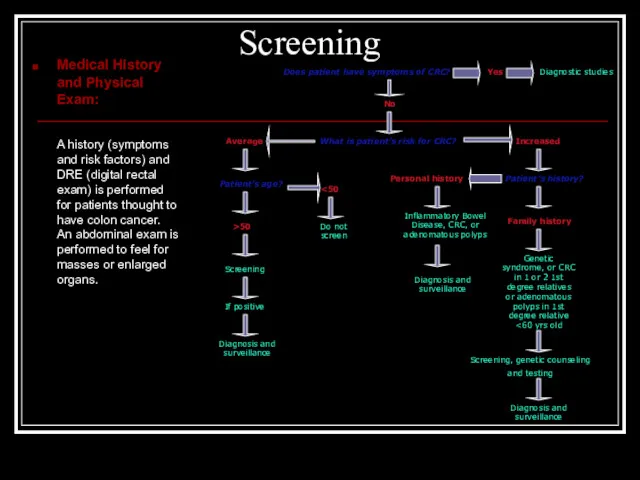
Screening
Medical History and Physical Exam:
A history (symptoms and risk factors) and
Screening
Medical History and Physical Exam:
A history (symptoms and risk factors) and
Screening Options: Fecal Occult Blood Test
Stool Blood Test (FOBT or FIT):
Screening Options: Fecal Occult Blood Test
Stool Blood Test (FOBT or FIT):
Screening: Flexible Sigmoidoscopy
Flexible Sigmoidoscopy: A sigmoidoscope, a slender, lighted tube the
Screening: Flexible Sigmoidoscopy
Flexible Sigmoidoscopy: A sigmoidoscope, a slender, lighted tube the
Screening: Barium Enema
Barium enema with air contrast: A chalky substance is
Screening: Barium Enema
Barium enema with air contrast: A chalky substance is
Screening: Virtual Colonoscopy
Virtual Colonoscopy: Air is pumped into the colon in
Screening: Virtual Colonoscopy
Virtual Colonoscopy: Air is pumped into the colon in

Screening: Colonoscopy
Colonoscopy: A colonoscope, a long, flexible, lighted tube about the
Screening: Colonoscopy
Colonoscopy: A colonoscope, a long, flexible, lighted tube about the
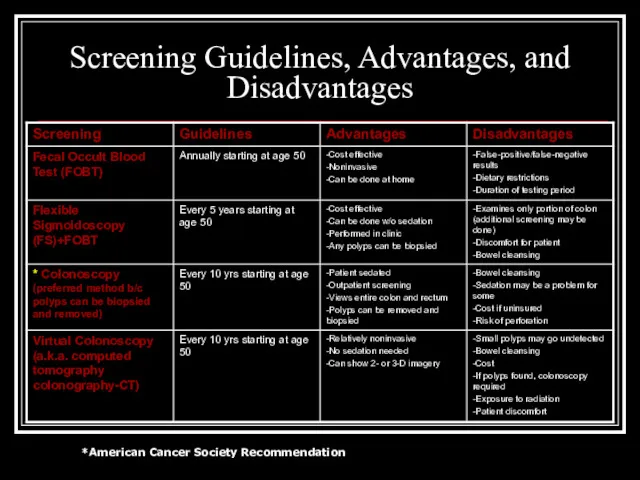
Screening Guidelines, Advantages, and Disadvantages
*American Cancer Society Recommendation
Screening Guidelines, Advantages, and Disadvantages
*American Cancer Society Recommendation
 Психическое здоровье и общество. Новые вызовы и угрозы
Психическое здоровье и общество. Новые вызовы и угрозы Балалардың жүйке ауруларындағы негізгі тексеру тәсілдері
Балалардың жүйке ауруларындағы негізгі тексеру тәсілдері Профилактика заболеваний. СПИД
Профилактика заболеваний. СПИД Отличительные черты креативных видов адаптивной физической культуры
Отличительные черты креативных видов адаптивной физической культуры Единство двух систем иммунитета – врожденного и приобретенного
Единство двух систем иммунитета – врожденного и приобретенного Здоровый образ жизни — образ жизни отдельного человека с целью профилактики болезней и укрепления здоровья
Здоровый образ жизни — образ жизни отдельного человека с целью профилактики болезней и укрепления здоровья Тема урока Лекарства (10 класс)
Тема урока Лекарства (10 класс) Фармацевтическая микробиология
Фармацевтическая микробиология Влияние распространения ВИЧинфекции на показатели функционирования здравоохранения Челябинской области
Влияние распространения ВИЧинфекции на показатели функционирования здравоохранения Челябинской области Гипертензивные расстройства во время беременности, в родах и послеродовом периоде. Часть 3
Гипертензивные расстройства во время беременности, в родах и послеродовом периоде. Часть 3 Варикоцеле. Расширение вен семенного канатика
Варикоцеле. Расширение вен семенного канатика Сечовидільна система
Сечовидільна система Зоонозды инфекция қоздырғыштары
Зоонозды инфекция қоздырғыштары Варикозная болезнь вен нижних конечностей
Варикозная болезнь вен нижних конечностей Рентгенологическая картина поражений суставов и позвоночника при анкилозирующем спондилоартрите
Рентгенологическая картина поражений суставов и позвоночника при анкилозирующем спондилоартрите Өкпеқап топографиясы,құрылысы мен қызметі,өкпеқап қуысы. Өкпеқап туындылары.Тынысалу ағзалары анатомиясының жастық ерекшеліктері
Өкпеқап топографиясы,құрылысы мен қызметі,өкпеқап қуысы. Өкпеқап туындылары.Тынысалу ағзалары анатомиясының жастық ерекшеліктері Эндометриоз и его лечение
Эндометриоз и его лечение Возбудители оппортунистических инфекций. Кандиды и кандидозы
Возбудители оппортунистических инфекций. Кандиды и кандидозы Хронический аутоиммунный тиреоидит и гипотиреоз: диагностика и лечение
Хронический аутоиммунный тиреоидит и гипотиреоз: диагностика и лечение Личная и общественная гигиена. Гигиенические основы физических упражнений
Личная и общественная гигиена. Гигиенические основы физических упражнений Хроническое, рецидивирующее заболевание - ожирение
Хроническое, рецидивирующее заболевание - ожирение Медицинская династия Пашковых- Бахтиных
Медицинская династия Пашковых- Бахтиных Лечение псориаза топическими ГКС с салициловой кислотой
Лечение псориаза топическими ГКС с салициловой кислотой Донорство. Як підготуватися до кровоздачі
Донорство. Як підготуватися до кровоздачі Группа заболеваний (инфекций) ЗППП/ИПП
Группа заболеваний (инфекций) ЗППП/ИПП Острый гематогенный остеомиелит у детей
Острый гематогенный остеомиелит у детей Аритмиялар (өміріне қауіп төндірген аритмия кезінде ауруханаға жатқызғанға дейін шұғыл және жедел көмек көрсету)
Аритмиялар (өміріне қауіп төндірген аритмия кезінде ауруханаға жатқызғанға дейін шұғыл және жедел көмек көрсету) Антибиотики и химиотерапевтические средства разных групп
Антибиотики и химиотерапевтические средства разных групп