- Iron Metabolism, Iron Deficiency and Overload

Содержание
- 2. IRON METABOLISM Iron has the capacity to accept and donate electrons: Fe2+⮀Fe3+, this capability makes it
- 3. Proteins of Iron Transport, Uptake and Storage Transferrin – a transport protein, carries iron in the
- 4. Proteins of iron regulation Iron Regulatory Proteins (IRP-1, IRP-2) are mRNA-binding proteins that coordinate expression of
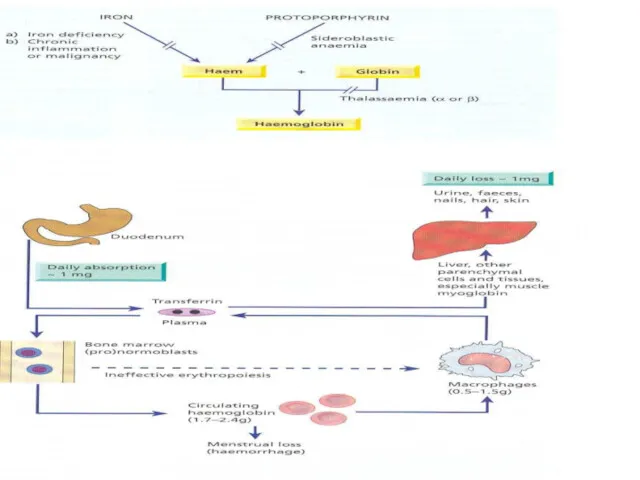
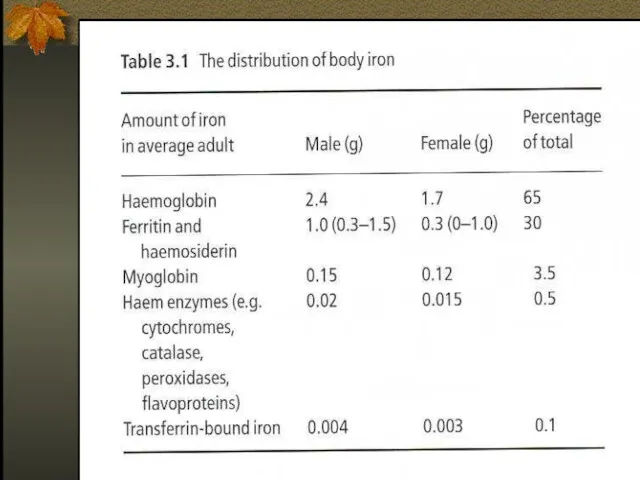
- 5. Iron Metabolism Adult man normally have 35-45mg/kg iron, women have less. 2/3 of body iron is
- 8. IRON METABOLISM Dietary Iron: Iron is essential element and must be precisely regulated. On the lumen
- 9. Regulation of Iron Absorption Humans have no physiologic way for iron excretion and regulation of absorption
- 10. TRANSPORT PROTEINS DMT1 (Divalent Metal Transporter 1) (Tranports from lumen into the enterocytes) FERROPORTIN1 (Transports from
- 11. Hepicidin, Primary regulator Increased expression of hepicidin leads to Decrease iron absorption and release. Mutation :Hemochromatosis
- 12. Hepcidin A 25 amino acid polypeptide produced by liver cells An acute phase protein The major
- 13. HEPICIDN 25 Amino acid disulfide peptide.
- 14. O Hepcidin lowers iron absorption in the intestine , lowers iron releasing from hepatocytes and macrophages
- 15. Ferroportin The only cellular iron exporter in vertebrates. Present in macrophages, placenta and the hepatocytes.
- 16. Mechanism of action of hepicidin The major mechanism of hepicidin is THE REGULATION OF TRANSMEMBRANE IRON
- 17. Hepicidin Regulation So when hepicidin levels are low ,iron exporting cells have abundant ferroportin and thus
- 18. IRON DEFICIENCY In 1997 Looker et al reported that 3% of American toddlers, 2-5% of American
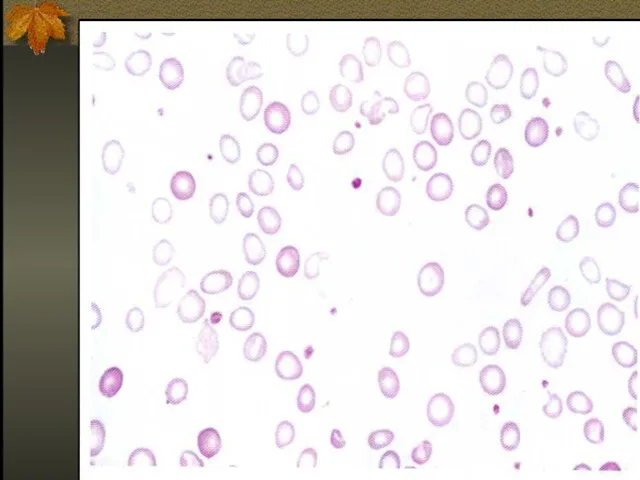
- 19. Iron deficiency is the commonest cause of anemia world wild. The anemia of iron deficiency is
- 21. Causes of Iron Deficiency Inadequate absorption Antiacid or high gastric Ph Excess bran,phytates Loss of enterocytes
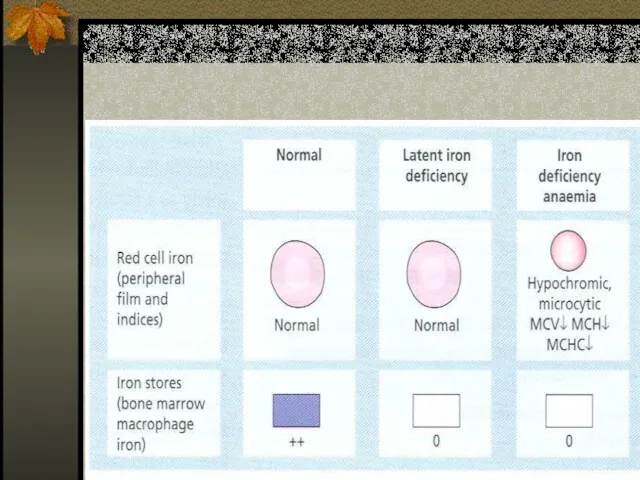
- 23. Stages of Iron Deficiency Iron depletion - decrement of iron stores, no decline in functional iron
- 25. Clinical Presentation Asymptomatic Signs and symptoms of underlying disorders Manifestations common to anemia from all causes:
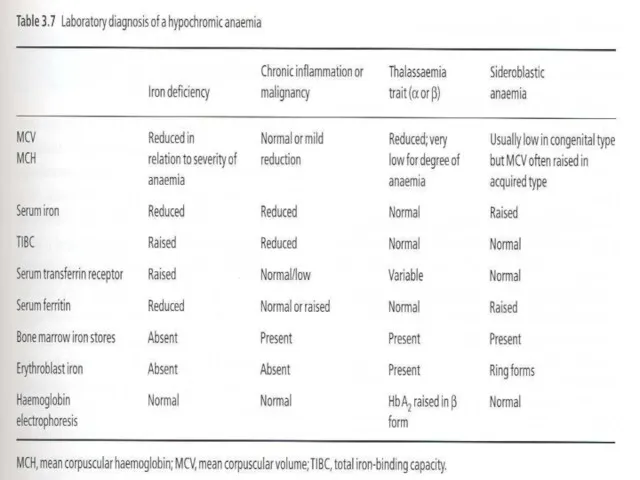
- 27. Laboratory Evaluation
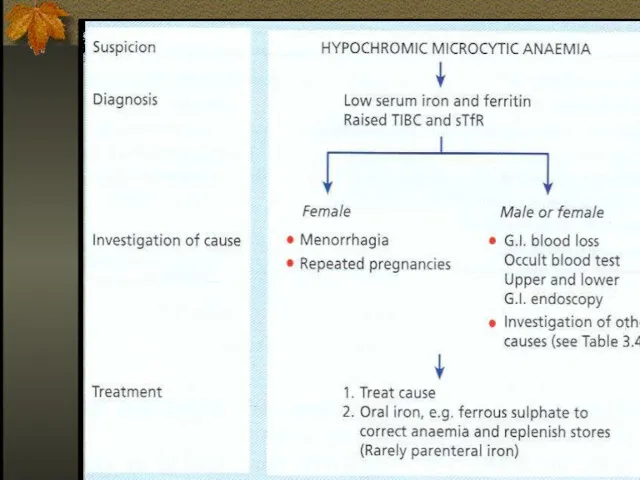
- 29. Differential Diagnosis of Microcytic Anemias With decreased iron stores Iron Deficiency Anemia With normal or increased
- 30. THERAPY Therapeutic trail of iron – confirms diagnosis of IDA if: Reticulocytosis starts 3-5 days from
- 31. ORAL IRON THERAPY Ferrous (Fe3+) iron salt supplying 150-200 mg elemental iron daily divided in 3-4
- 32. Parenteral Iron Therapy Malabsorption Intolerance to oral treatment Chronic uncontrolled bleeding RISKS – anaphylaxis (0.5-1%), severe
- 34. Iron Overload Accumulation of iron can occur in disorders associated with excessive absorption or chronic blood
- 35. Disease States Hepcidin deficiency, physiological = Haemochromatosis Hepcidin excess – anaemia of chronic disease
- 37. The role of Hepcidin in hereditary hemochromatosis Hereditary hemochromatosis: -excessive intestinal iron absorption -Saturation of transferrin
- 38. Hereditary Hemochromatosis Autosomal recessive disease Excessive absorption of Fe from GIT HFE – the gene involved,
- 39. Iron Overload The clinical features of iron overload from any cause are similar: - skin hyper
- 40. Therapy Hemochromatosis without anemia – regular venesection, each unit of blood removes 200-250 mg of iron,
- 41. Iron chelators Deferoxamine – parenteral use, excretion in urine, side effects – deafness, visual, growth, and
- 43. Скачать презентацию
IRON METABOLISM
Iron has the capacity to accept and donate electrons: Fe2+⮀Fe3+,
IRON METABOLISM
Iron has the capacity to accept and donate electrons: Fe2+⮀Fe3+,
Proteins of Iron Transport, Uptake and Storage
Transferrin – a transport protein,
Proteins of Iron Transport, Uptake and Storage
Transferrin – a transport protein,
Proteins of iron regulation
Iron Regulatory Proteins (IRP-1, IRP-2) are mRNA-binding proteins
Proteins of iron regulation
Iron Regulatory Proteins (IRP-1, IRP-2) are mRNA-binding proteins
Iron Metabolism
Adult man normally have 35-45mg/kg iron, women have less.
2/3 of
Iron Metabolism
Adult man normally have 35-45mg/kg iron, women have less.
2/3 of
IRON METABOLISM
Dietary Iron:
Iron is essential element and must be
IRON METABOLISM
Dietary Iron:
Iron is essential element and must be
Regulation of Iron Absorption
Humans have no physiologic way for iron excretion
Regulation of Iron Absorption
Humans have no physiologic way for iron excretion
TRANSPORT PROTEINS
DMT1 (Divalent Metal Transporter 1)
(Tranports from lumen into
TRANSPORT PROTEINS
DMT1 (Divalent Metal Transporter 1)
(Tranports from lumen into
Hepicidin, Primary regulator
Increased expression of hepicidin leads to
Decrease iron
Hepicidin, Primary regulator
Increased expression of hepicidin leads to
Decrease iron
Hepcidin
A 25 amino acid polypeptide produced by liver cells
An
Hepcidin
A 25 amino acid polypeptide produced by liver cells
An
HEPICIDN
25 Amino acid disulfide peptide.
HEPICIDN
25 Amino acid disulfide peptide.
O
Hepcidin lowers iron absorption in the intestine , lowers iron releasing
O
Hepcidin lowers iron absorption in the intestine , lowers iron releasing
Ferroportin
The only cellular iron exporter in vertebrates.
Present in macrophages,
Ferroportin
The only cellular iron exporter in vertebrates.
Present in macrophages,
Mechanism of action of hepicidin
The major mechanism of hepicidin is
Mechanism of action of hepicidin
The major mechanism of hepicidin is
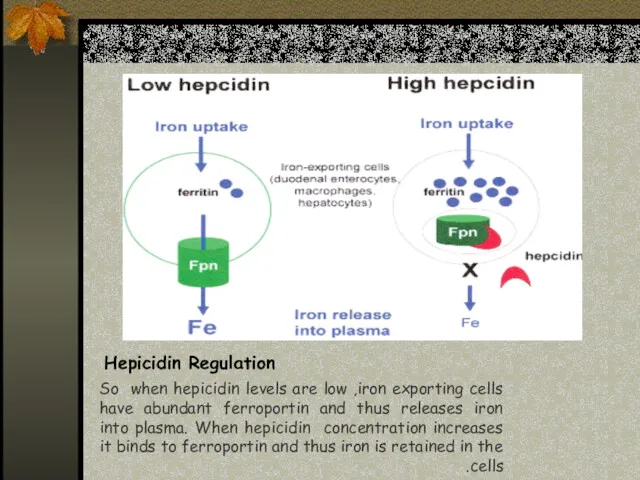
Hepicidin Regulation
So when hepicidin levels are low ,iron exporting cells have
Hepicidin Regulation
So when hepicidin levels are low ,iron exporting cells have
IRON DEFICIENCY
In 1997 Looker et al reported that 3% of American
IRON DEFICIENCY
In 1997 Looker et al reported that 3% of American
Iron deficiency is the commonest cause of anemia world wild.
The anemia
Iron deficiency is the commonest cause of anemia world wild.
The anemia
Causes of Iron Deficiency
Inadequate absorption
Antiacid or high gastric Ph
Excess bran,phytates
Loss
Causes of Iron Deficiency
Inadequate absorption
Antiacid or high gastric Ph
Excess bran,phytates
Loss

Stages of Iron Deficiency
Iron depletion - decrement of iron stores, no
Stages of Iron Deficiency
Iron depletion - decrement of iron stores, no
Clinical Presentation
Asymptomatic
Signs and symptoms of underlying disorders
Manifestations common to anemia from
Clinical Presentation
Asymptomatic
Signs and symptoms of underlying disorders
Manifestations common to anemia from

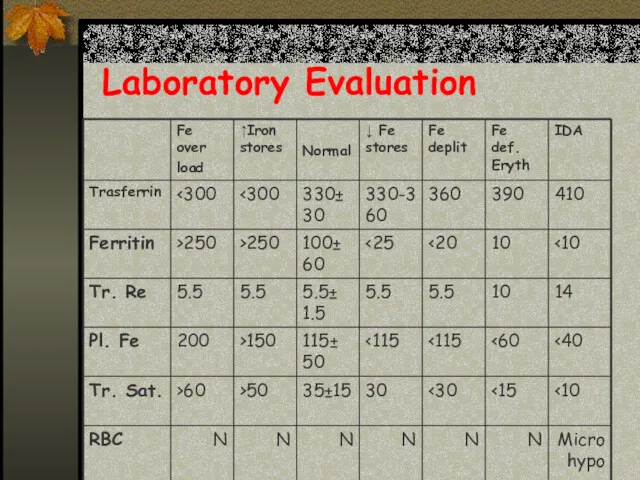
Laboratory Evaluation
Laboratory Evaluation
Differential Diagnosis of Microcytic Anemias
With decreased iron stores
Iron Deficiency Anemia
Differential Diagnosis of Microcytic Anemias
With decreased iron stores
Iron Deficiency Anemia
THERAPY
Therapeutic trail of iron – confirms diagnosis of IDA if:
Reticulocytosis starts
THERAPY
Therapeutic trail of iron – confirms diagnosis of IDA if:
Reticulocytosis starts
ORAL IRON THERAPY
Ferrous (Fe3+) iron salt supplying 150-200 mg elemental iron
ORAL IRON THERAPY
Ferrous (Fe3+) iron salt supplying 150-200 mg elemental iron
Parenteral Iron Therapy
Malabsorption
Intolerance to oral treatment
Chronic uncontrolled bleeding
RISKS – anaphylaxis (0.5-1%),
Parenteral Iron Therapy
Malabsorption
Intolerance to oral treatment
Chronic uncontrolled bleeding
RISKS – anaphylaxis (0.5-1%),
Iron Overload
Accumulation of iron can occur in disorders associated with
Iron Overload
Accumulation of iron can occur in disorders associated with
Disease States
Hepcidin deficiency, physiological = Haemochromatosis
Hepcidin excess – anaemia
Disease States
Hepcidin deficiency, physiological = Haemochromatosis
Hepcidin excess – anaemia

The role of Hepcidin in hereditary hemochromatosis
Hereditary hemochromatosis:
-excessive intestinal iron absorption
-Saturation
The role of Hepcidin in hereditary hemochromatosis
Hereditary hemochromatosis:
-excessive intestinal iron absorption
-Saturation
Hereditary Hemochromatosis
Autosomal recessive disease
Excessive absorption of Fe from GIT
HFE –
Hereditary Hemochromatosis
Autosomal recessive disease
Excessive absorption of Fe from GIT
HFE –
Iron Overload
The clinical features of iron overload from any cause are
Iron Overload
The clinical features of iron overload from any cause are
Therapy
Hemochromatosis without anemia – regular venesection, each unit of blood
Therapy
Hemochromatosis without anemia – regular venesection, each unit of blood
Iron chelators
Deferoxamine – parenteral use, excretion in urine, side effects –
Iron chelators
Deferoxamine – parenteral use, excretion in urine, side effects –
 Трансплантация және оның түрлері. Тері, бұлшықет, сіңір, жүйке, сүйек, тамырлардың пластикасы. Донорды таңдау
Трансплантация және оның түрлері. Тері, бұлшықет, сіңір, жүйке, сүйек, тамырлардың пластикасы. Донорды таңдау Oral diagnosis
Oral diagnosis Қанайналым бұзылуының жалпы және жергілік түрлері жайлы ұғым, олардың өзара байланыстылығы, классификациясы
Қанайналым бұзылуының жалпы және жергілік түрлері жайлы ұғым, олардың өзара байланыстылығы, классификациясы Ревматоидный артрит
Ревматоидный артрит Сестринский процесс при гломерулонефритах
Сестринский процесс при гломерулонефритах Диагностика абсцесса легких, бронхоэктатической болезни
Диагностика абсцесса легких, бронхоэктатической болезни Дерматиты. Токсидермии. Экзема
Дерматиты. Токсидермии. Экзема Дифференциальная диагностика снижения зрения
Дифференциальная диагностика снижения зрения Планирование семьи
Планирование семьи Влияние гормонов паращитовидных желез на состояние зубочелюстной системы
Влияние гормонов паращитовидных желез на состояние зубочелюстной системы Сахарный диабет
Сахарный диабет Тяжелая сочетанная травма
Тяжелая сочетанная травма Современные методы фармацевтического анализа
Современные методы фармацевтического анализа Неспецифические воспалительные заболевания кишечника
Неспецифические воспалительные заболевания кишечника Оказания неотложной помощи больным с сочетанными черепно-мозговыми травмами
Оказания неотложной помощи больным с сочетанными черепно-мозговыми травмами Туберкулез в полости рта
Туберкулез в полости рта Сепсис. Перитонит
Сепсис. Перитонит Параллелометрия. Определение
Параллелометрия. Определение Боль и обезболивание
Боль и обезболивание Босанғаннан кейінгі ерте кезеңдегі қан кетудің себептері: тонус, тін
Босанғаннан кейінгі ерте кезеңдегі қан кетудің себептері: тонус, тін Внебольничные пневмонии и грипп
Внебольничные пневмонии и грипп Стаз. Причины развития стаза
Стаз. Причины развития стаза Клиническая фармакология антибактериальных лекарственных препаратов
Клиническая фармакология антибактериальных лекарственных препаратов Гемолитико-уремический синдром. Клиническая картина, диагностика и лечение
Гемолитико-уремический синдром. Клиническая картина, диагностика и лечение Рак молочной железы
Рак молочной железы Неотложные урологические состояния у детей. Принципы интенсивной терапии
Неотложные урологические состояния у детей. Принципы интенсивной терапии Поддержание женского здоровья. Капсулы СуперСерен Тяньши
Поддержание женского здоровья. Капсулы СуперСерен Тяньши Синтетические противомикробные средства
Синтетические противомикробные средства