- Oral diagnosis

Содержание
- 2. Oral Diagnosis It is the art of using scientific knowledge to identify oral disease processes and
- 3. Types of oral diagnosis : 1) - Comprehensive oral diagnosis :- The diagnostic assessment for all
- 4. 2) Emergency diagnosis :- It is the immediate diagnosis of the patient's complaint that requires immediate
- 5. 3) Spot (snap) diagnosis :- In simple cases where rapid diagnosis can be achieved perfectly, based
- 6. 4) Differential diagnosis :- It is the collection and categorization of data to develop a list
- 7. 5) Tentative (working or provisional diagnosis :- It is primary, uncertain diagnosis before all diagnostic data
- 8. Symptoms and signs: All findings can be grouped as either:- - symptoms (subjective) - or signs
- 9. Signs (objective findings): Objective findings are the changes or deviations from normal that can be detected
- 10. Treatment plan: Treatment plan may take one of two forms: A. Emergency or immediate treatment plan:-
- 11. The diagnostic method It is the application of a scientific method to reach a final diagnosis.
- 12. 1-Collection of information for reaching a diagnosis include: 1 – Patient history. 2 – Clinical examination.
- 13. 2 - Evaluation of the information It is the organization of the collected information to determine
- 14. Methods for obtaining a patient's history The primary methods for obtaining a patient's history are:- 1.
- 15. II – Chief complaint (cc) The chief complaint (cc) is a statement of why the patient
- 16. Common chief complaints Usually the patient comes to the dental clinic complaining of one or more
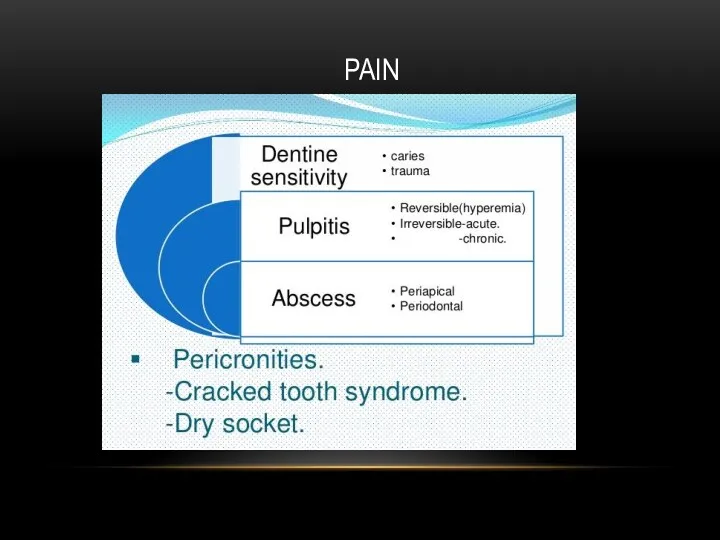
- 17. PAIN
- 18. 3 – Paraesthesia and numbness Caused by vitamin deficiency, pressure on the mandibular nerve such as
- 19. 4 - Sensitivity Sensitivity to hot, cold and sweats may result from decayed teeth, pulpitis or
- 20. 6 – Swelling - Soft tissue swelling such as:- - facial cellulitis - and glandular swelling
- 21. 7 – Oral ulceration Ulceration of the oral mucous membrane are multiple and caused by different
- 22. 8 – T.M.J. disorders Patients with T.M.J. disorders may complaint of:- - clicking in jaw joint
- 23. 9 – Functional disorders The patient complaint may result from functional disorders such as:- - dysphagia
- 24. 10 – Bad breath (halitosis) It results from either extra-oral or more commonly oral causes especially
- 25. 11- Esthetic problem Orthodontic treatment or malposed teeth may be the only complaint of certain age
- 26. Chief complaint chart Chief complaint C/c …………………………………………….……………………………………………………………………… History of chief complaint ………………………………. 1 – Onset: ………………
- 27. [1] Onset a - Character b - Date Sudden (abrupt) a) Character of onset: gradual (1)
- 28. Gradual onset = (1) Chronic inflammatory conditions (2) Neoplastic lesions . (b) Date of onset: Should
- 29. [2] Duration: Recorded is hours, days, weeks, months, years, including periods of remissions and exacerbations. *
- 30. [3] Character and severity : Severity : (Mainly of pain) : - This will be affected
- 31. Character : of pain may be (1) Throbbing pain means fluid accumulation e.g.:. - pus accumulation
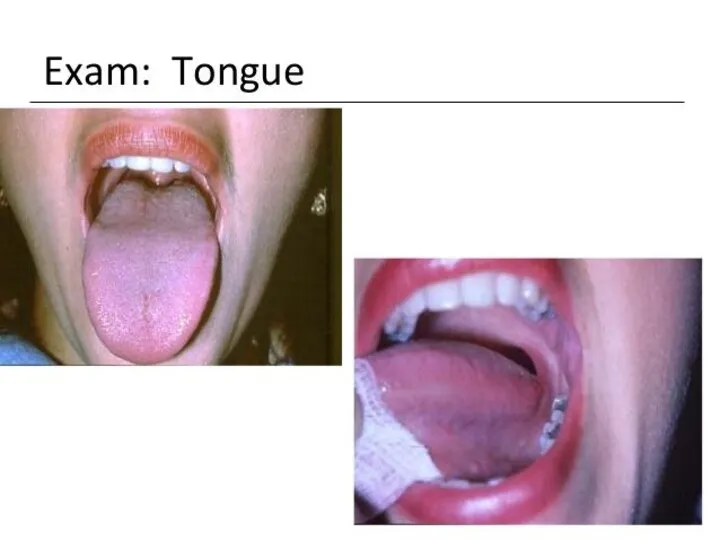
- 32. [4] Location and site: * Location : - The anatomical area : tongue, cheek, gingiva, etc..
- 33. [5] Course: Could be recorded as: Progressive: (increasing in severity) e.g. - tumours, - acute inflammatory
- 34. Remission/Exacerbation Lesion is present all the time, signs are present and the change is in the
- 35. [6] History of recurrence: The history of previous occurrence of the lesion may be of importance
- 36. [8] Precipitating factors and relation to other activities:- *Pain may increase by eating, swallowing, sleeping, cold
- 37. [9] Relieving factors: Factors which relieve chief complaint e.g.:- - Rest, - Medications as simple analgesics,
- 38. [10] Associated phenomena: These are manifestations associated with the complaint: ● Fever ( acute abscess). ●
- 39. [11] Previous medication: Mouth washes, analgesics, antibiotics, previously used by the patient, and their effect on
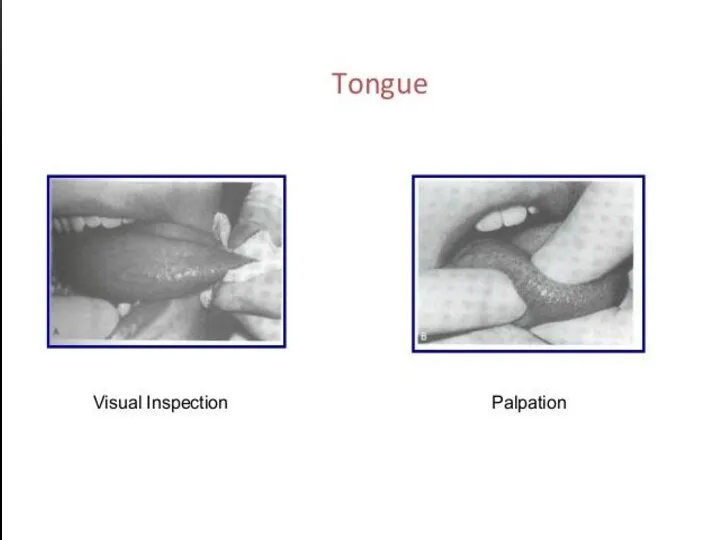
- 40. EXTRA ORAL EXAMINATION INTRA ORAL EXAMINATION CLINICAL EXAMINATION Inspection – palpation – percussion – probing -
- 50. ANGULAR CHEILITIS
- 53. Dr.Anas Almisurati
- 54. NORMAL ORAL MUCOSA Normal oral mucosa with variation in structure and appearance :- 1- Fordyces granules
- 56. LINEA ALBA
- 58. FORDYCE'S GRANULES Dr.Anas Almisurati
- 60. KERATOTIC LESION Keratotic lesion (can’t rubbed off) :- 1- oral keratosis 2- leukoplakia 3- candidal leukoplakia
- 61. ORAL KERATOSIS (CAN’T RUBBED OFF ) Dr.Anas Almisurati Def. :IS a group of the white keratotic
- 62. FRICTIONAL KERATOTIC Dr.Anas Almisurati (reversible)
- 63. SMOKER,S PATCHES (reversible) White keratinized patch on the vermilion border of the lips. b. it may
- 64. NICOTINIC STOMATITIS Dr.Anas Almisurati Etiology → the epithelial lining of the ducts of the minor salivary
- 65. ACTINIC KERATOSIS (irreversible) It is a premalignant lesion due to exposure to ultraviolet rays. Damaging effect
- 66. HOMOGENOUS LEUKOPLAKIA Flat Corrugated smooth & elevated wrinkled
- 67. SPECKLED LEUKOPLAKIA corner of the mouth. white patches (keratotic) on erythematous base (atrophic mucosa).
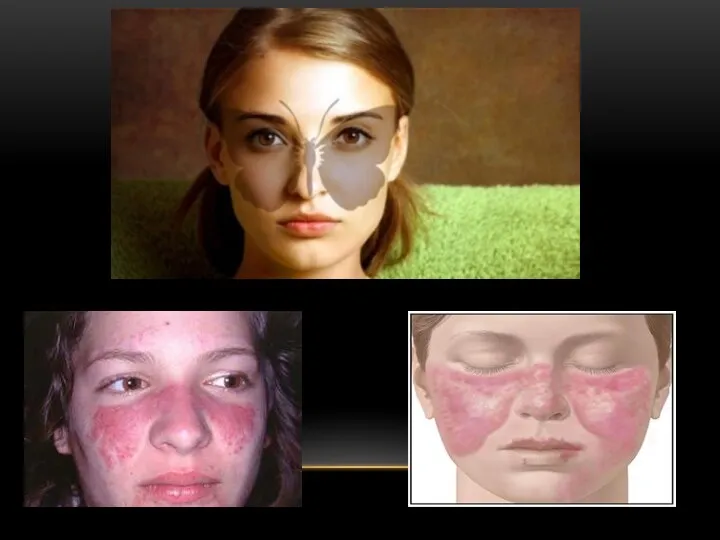
- 70. DURATION 2 YEARS MAXIMUM → LEAVING SOME PIGMENTATIONS ON THE SKIN. Wickham's striae Kobner phenomenon
- 81. RAYNAUD’S PHENOMAN Is cyanosis and pain of finger and toes on exposure to cold Common in
- 82. STRETCHING OF WHITE LESION MAY SHOW:-
- 93. Gingiva: The following features of the gingiva should be considered e.g.: colour, size, contour, consistency, surface
- 94. MARGINAL GINGIVAL INFLAMMATION
- 95. Periodontal pockets: In order to evaluate the amount of periodontal tissues lost in periodontal disease and
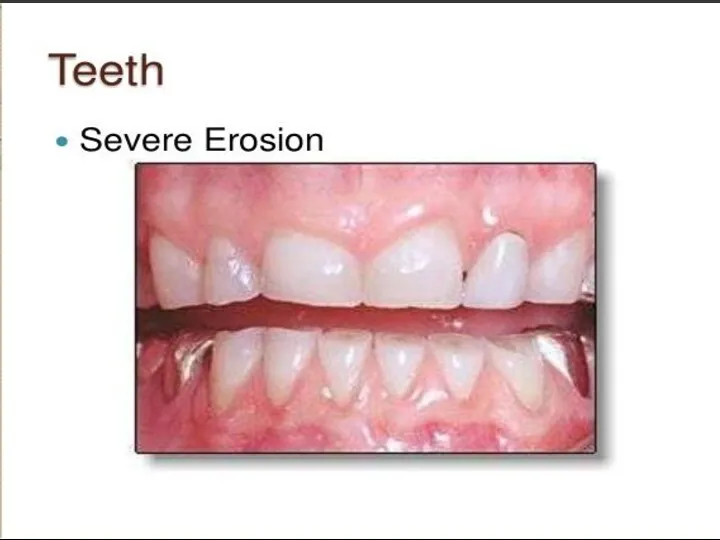
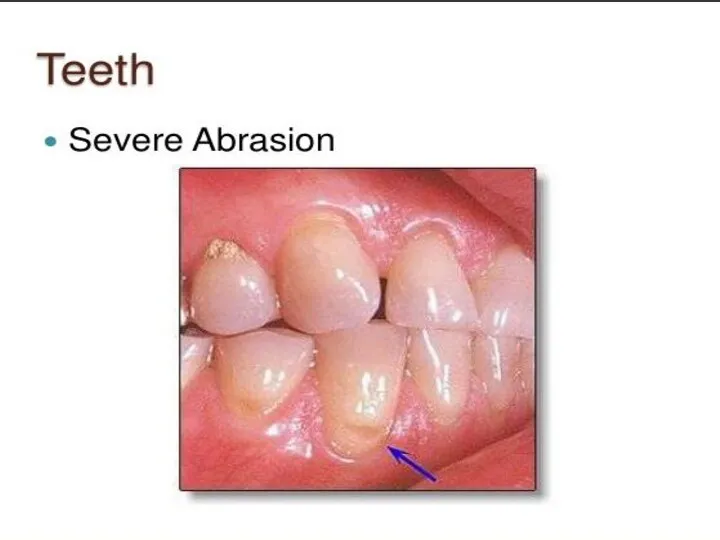
- 102. Examination of the teeth: Teeth are examined for caries, overhanging fillings, hypersensitivity, proximal contact relationships, tooth
- 105. - History of habits: Clenching or grinding the teeth. Tongue thrusting. Smoking.
- 106. GENERAL APPRAISAL SKULL ( CRANIUM) FACE EYE NOSE HAIR SKIN JAWS & TMJ SALIVARY GLANDS LYMPH
- 107. GENERAL APPRAISAL Starts while patient entering the clinic. Performed without patient interruption. Report, record, or observe
- 108. 1. Physical structure ( body type ) - asthenic : slender or slim - normosthenic :
- 109. 3. Body weight over, under or normal 4. Behavior lazy, nervous, irritable or normal. 5. Speech
- 111. 7. Recording vital signs temperature 37 normal pulse rate 72 B/M normal blood pressure 80/120 normal
- 112. SKULL AND CRANIUM Size : from supra orbital ridge to occipital protuberance. - Small head (micro
- 113. CONGENITAL SYPHILIS
- 114. PAGET,S DISEASE
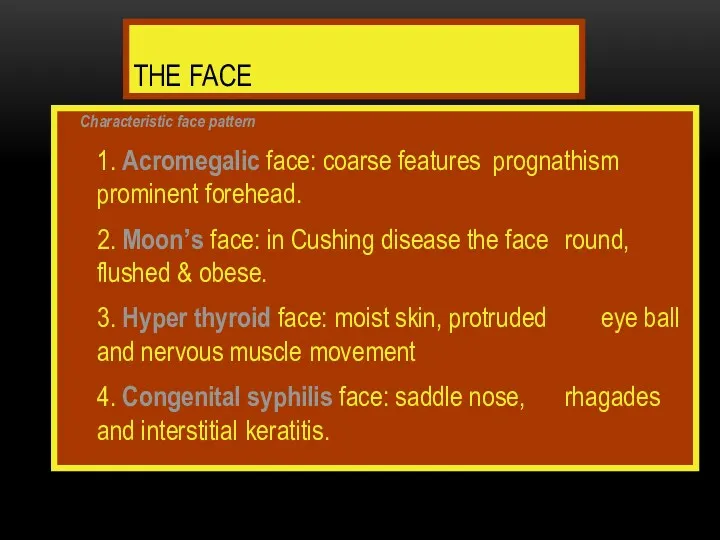
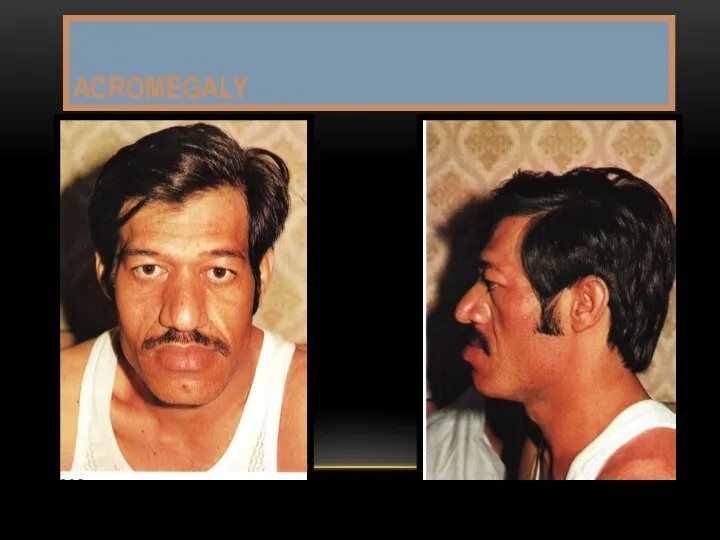
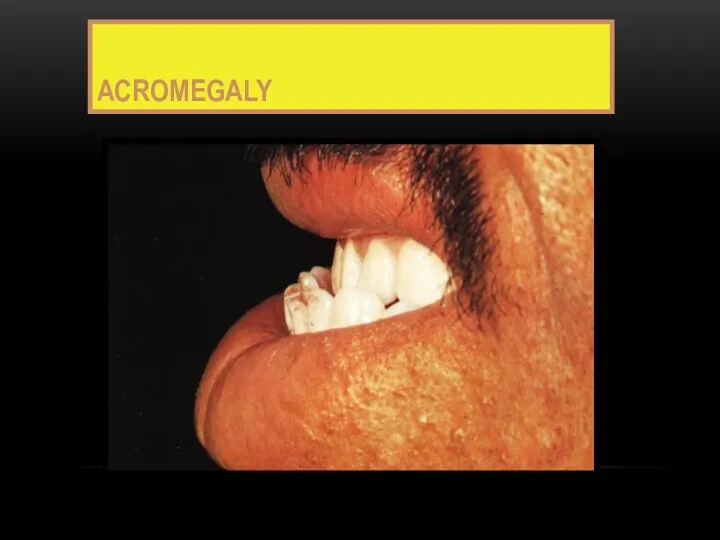
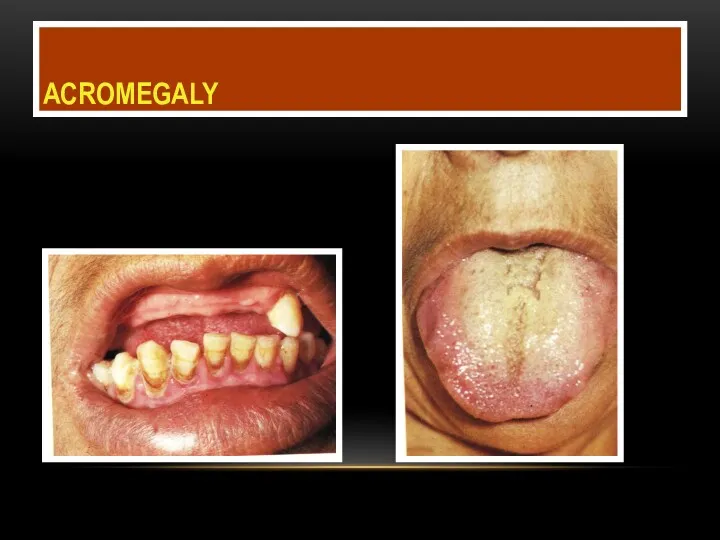
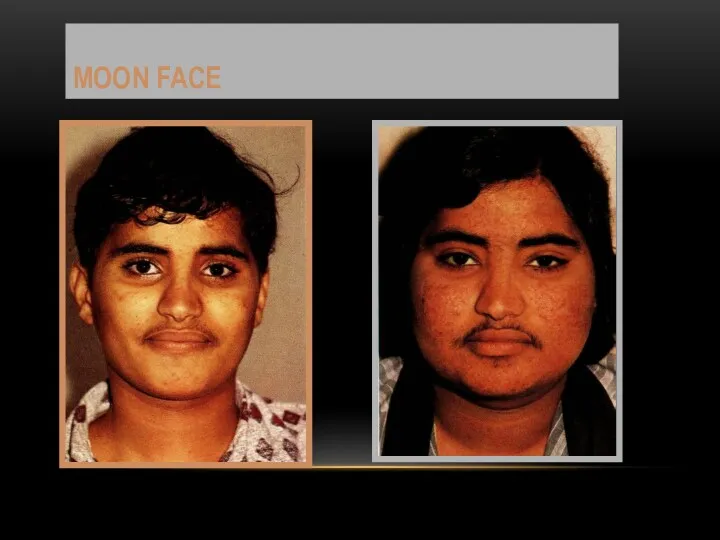
- 115. THE FACE Characteristic face pattern 1. Acromegalic face: coarse features prognathism prominent forehead. 2. Moon’s face:
- 116. ACROMEGALY
- 117. ACROMEGALY
- 118. ACROMEGALY
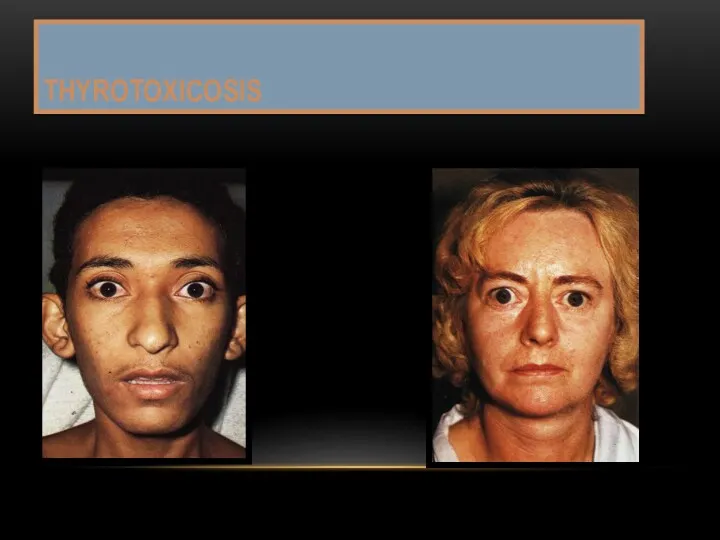
- 119. THYROTOXICOSIS
- 120. MOON FACE
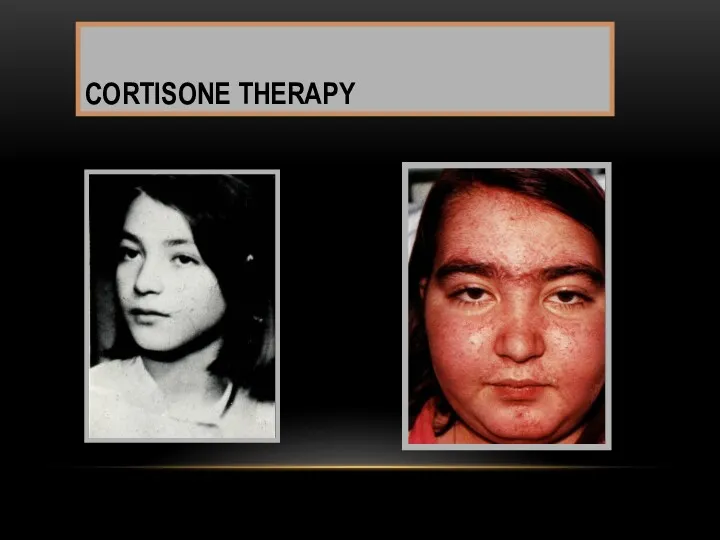
- 121. CORTISONE THERAPY
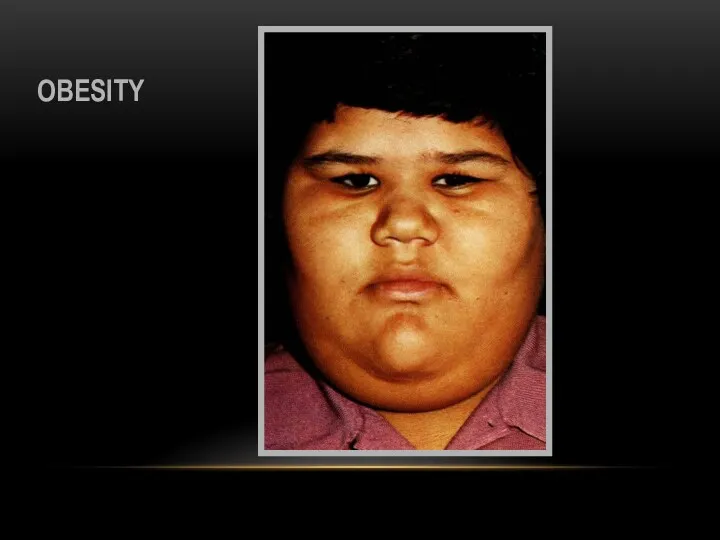
- 122. OBESITY
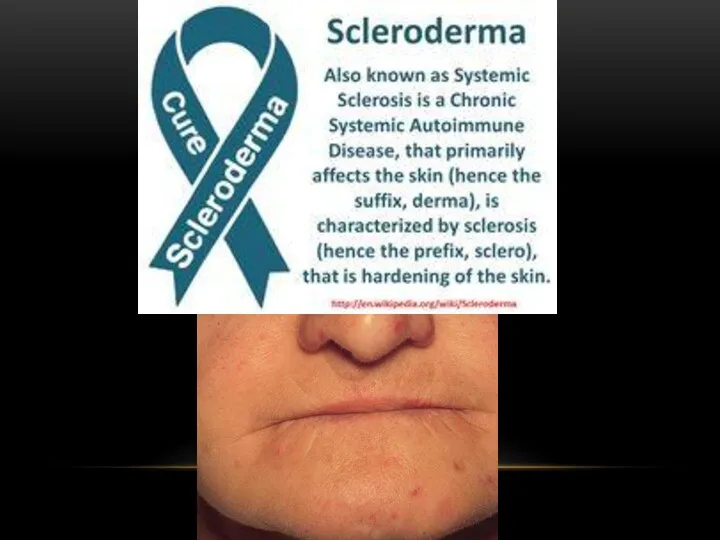
- 123. 5. Nephrotic face : puffy, pale with baggy eyelids 6. Sclerodermic face: “mask face” smiling, whistling
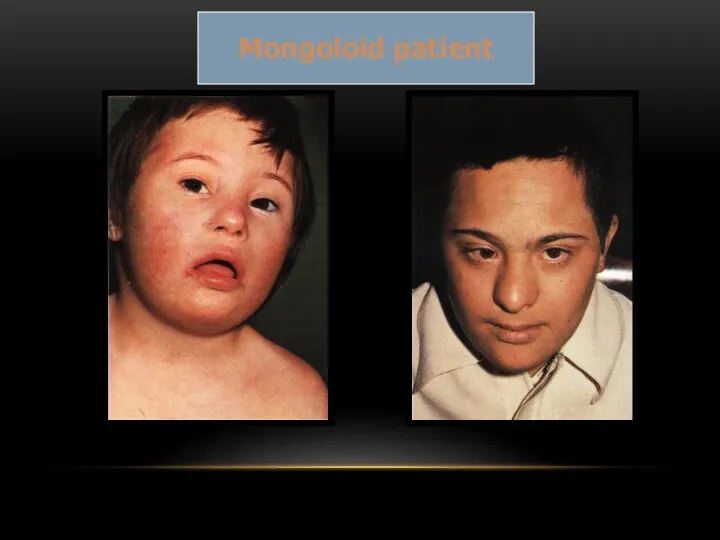
- 124. Mongoloid patient
- 125. DOWN,S SYNDROME
- 126. Mouth breather Cracked lips Macroglossia Fissured tongue Cleft lip or palate Poor oral hygiene Short roots
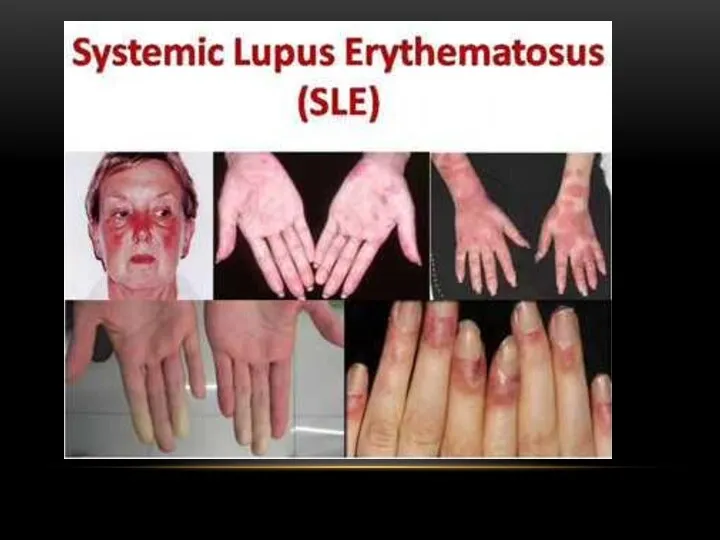
- 127. Clinical findings
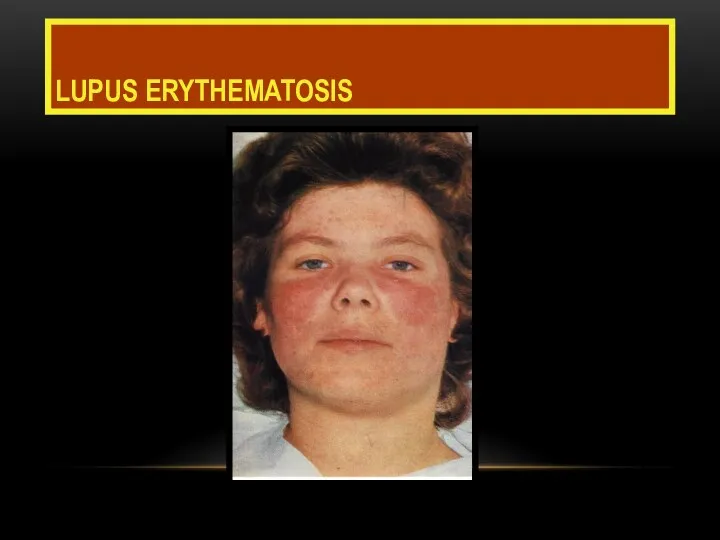
- 128. LUPUS ERYTHEMATOSIS
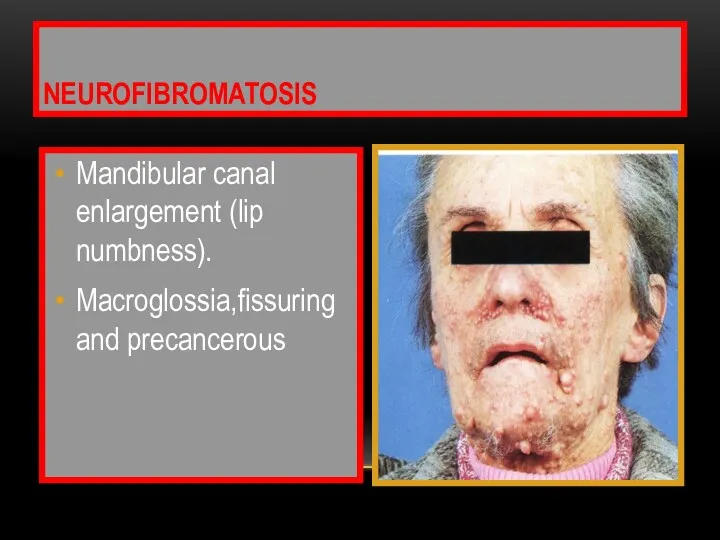
- 129. Mandibular canal enlargement (lip numbness). Macroglossia,fissuring and precancerous NEUROFIBROMATOSIS
- 130. ANGIO EDEMA sever facial swelling
- 131. Third molars ext SURGICAL TRAUMA Post operative Two weeks later
- 132. MASSETER HYPERTROPHY
- 133. AIR EMPHYSEMA is a compressible swelling that produce crackling sound upon palpation . It is caused
- 135. An aggressive and rapidly growing malignant tumor that has extended via mandibular cortical plate . EWING,S
- 136. BELL, S PALSY Left side paralysis
- 137. HERPES ZOSTER Chicken pox is the primary infection by Varicella – Zoster herpetic virus. Papules, vesicles
- 138. Shingles affects skin by vesicles and pustules that ruptures to form painful crusts persists for weeks
- 139. INFECTED CYST UPPER INCISORS
- 140. ACUTE DENTO ALVEOLAR ABSCESS LOWER INCISORS
- 141. ADAA UPPER PRE MOLARS LOWER MOLAR
- 142. MICROGNATHIA
- 143. FACIAL PALSY
- 144. PAROTID GLAND ENLARGEMENT
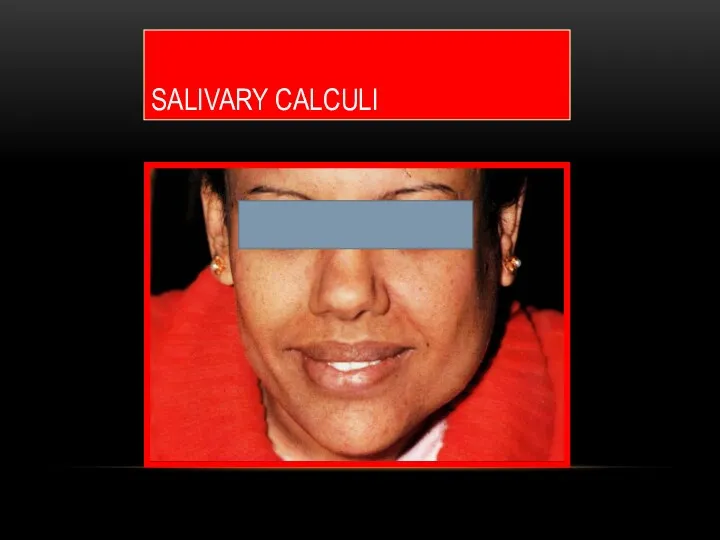
- 145. SALIVARY CALCULI
- 147. THE NOSE Nasal abnormalities may be interrelated to oral lesions. The following might be affected: -
- 148. SADDLE NOSE
- 149. ACROMEGALY Enlarged nose
- 150. THE EYE sclera pupil Iris conjunctiva
- 151. 1) Ptosis - Dropping of upper eye lid - Inability to open the eye completely It
- 152. CONGENITAL PTOSIS bilateral unilateral
- 153. DENTINOGENESIS IMPERFECTA Blue sclera Opalescent cracked teeth
- 154. Autoimmune vesiculobullous lesion affects skin and oral mucosa or other mucosal tissue. Clinically flaccid intraepithelial bullae
- 155. Exophthalmia - Protruded eye ball is common finding in THyrotoxicosis.
- 156. CONJUNCTIVITIS Behcet,s REITER,S
- 157. SYNDROMES AND OTHER DISEASES Muco Cutaneous Ocular Syndromes 1- STEVEN JHONSON S 2- BEHCET S 3-
- 158. THE SKIN The skin should be inspected for : color changes, pigmented lesions, and scars
- 159. Palpation is used to examine surface texture changes and to check skin temperature. - Skin lesions
- 160. Skin color - Depends mainly on the amount deposited pigmented material as:- Melanin ? Brownish black
- 161. Increased melanin physiologically in pregnancy or pathologically as in Addison’s disease. - Pallor skin in anemia
- 162. - Bluish or cyanotic color occurs due to stagnation of reduced blood as in heart failure.
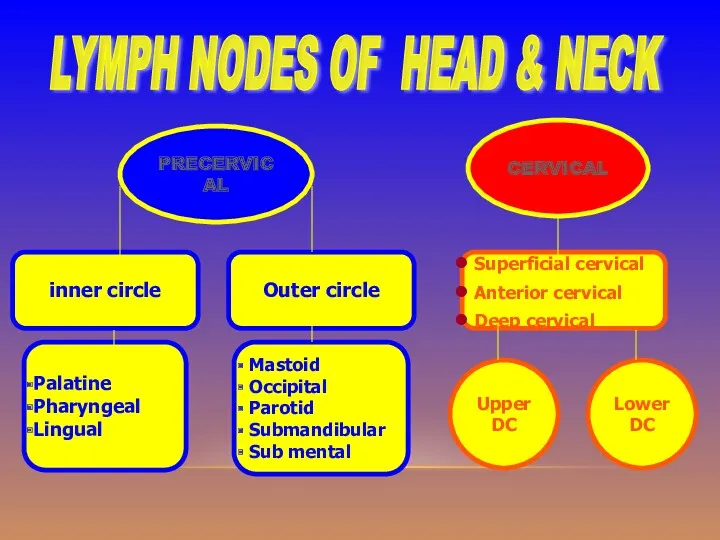
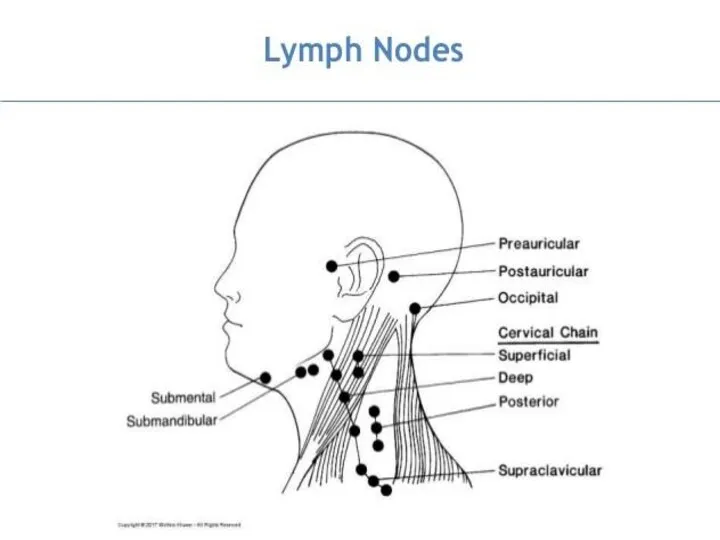
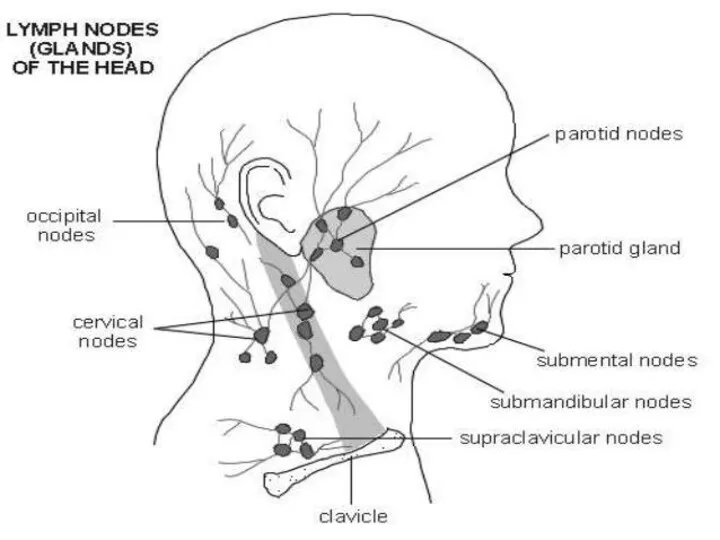
- 164. PRECERVICAL CERVICAL Superficial cervical Anterior cervical Deep cervical Outer circle inner circle Palatine Pharyngeal Lingual Mastoid
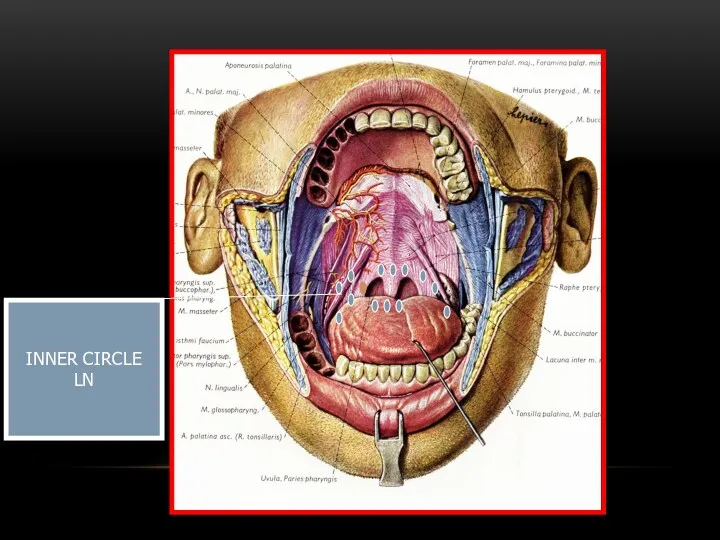
- 165. PRE-CERVICAL GROUP Inner Circle lymphoid tissue around pharynx 1) Palatine at the mucous membrane of the
- 166. 3) Lingual lymphoid aggregations mostly at dorsal & lateral aspects of post 1/3 of the tongue.
- 167. Drainage all lymphoid tissue of inner circle drains into deep cervical.
- 168. Outer Circle 1) Occipital drain posterior part of scalp. 2) Mastoid drain parietal region of scalp.
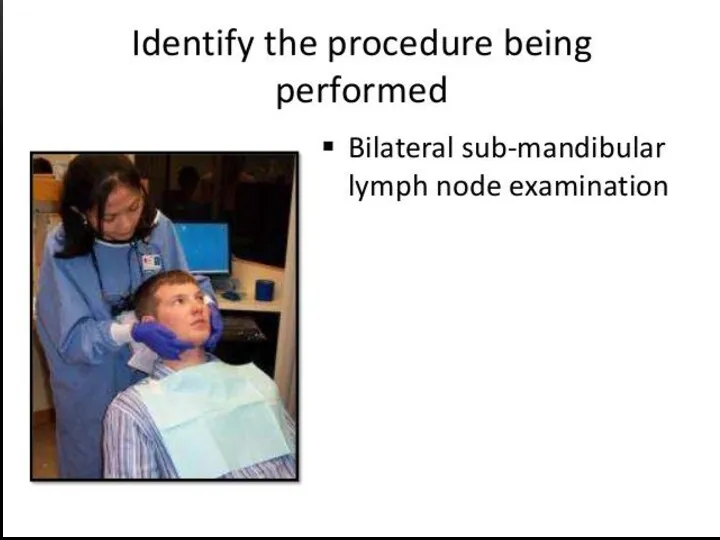
- 169. 5) Submandibular (submax.) - Medial part of eye lid. - Nasal, cheek & upper lip skin
- 170. CERVICAL GROUP 1) Superficial Cervical group - Below parotid gland, associated with the external & anterior
- 171. 2) Anterior C.G (Pre-tracheal) - It drains larynx, trachea & thyroid gland. 3) Deep C.G (upper
- 172. N.B. Deep cervical drains - Maxillary teeth, gum, hard palate and post 1/3 of tongue. -
- 173. Upper deep Cervical LN LOWER deep Cervical LN SUB MANDIBULAR LN
- 174. Thyroid G SUB MENTAL LN ITHMUS OF THYROID ANT CERVICAL (PRETRACHEAL) LN
- 176. INNER CIRCLE LN
- 180. Lymph node enlargement Localized factors 1. Infection a) Acute: NUG, ADAA, AHGS, Chancre b) Chronic: Scrofula
- 181. Generalized factors 1) Infection a) Acute : infectious mononucleosis b) Chronic : secondary stage of syphilis
- 182. Other Causes :- * Sarcoidosis * S.L.E * rheumatoid arthritis * histoplasmosis * phenytoin & drug
- 183. Lymph node should be examined for - Being solitary or multiple. - Unilateral or bilateral. -
- 184. The lymph node may be - Tender, soft and discrete in acute infections. - Firm without
- 185. Lab tests in LN enlargement diagnosis 1- Pulp test for tooth vitality. 2- Chest X ray
- 186. 5- Biopsy. 6- Smear & Culture in TB or Syphilis. 7- Blood Ca++ level ( increase
- 187. SALIVARY GLANDS Enlargement of major salivary glands may be due to : 1) Infection (viral or
- 188. Enlargement of salivary glands may be accompanied by Pain & tenderness Facial asymmetry Facial palsy Xerostomia
- 191. THYROID GLANDS Normally the gland is usually palpable as two lobes connected by isthmus at the
- 192. Palpation The examiner should be behind the patient palpating the gland by fingers of the two
- 194. TMJ Occlusion Ms of mastication Jiont
- 202. Скачать презентацию
Oral Diagnosis
It is the art of using scientific knowledge to
Oral Diagnosis
It is the art of using scientific knowledge to
Types of oral diagnosis :
1) - Comprehensive oral diagnosis :-
The
Types of oral diagnosis :
1) - Comprehensive oral diagnosis :-
The
2) Emergency diagnosis :-
It is the immediate diagnosis of the
2) Emergency diagnosis :-
It is the immediate diagnosis of the
3) Spot (snap) diagnosis :-
In simple cases where rapid diagnosis
3) Spot (snap) diagnosis :-
In simple cases where rapid diagnosis
4) Differential diagnosis :-
It is the collection and categorization of
4) Differential diagnosis :-
It is the collection and categorization of
5) Tentative (working or provisional
diagnosis :-
It is
5) Tentative (working or provisional
diagnosis :-
It is
Symptoms and signs:
All findings can be grouped as either:-
-
Symptoms and signs:
All findings can be grouped as either:-
-
Signs (objective findings):
Objective findings are the changes or deviations from normal
Signs (objective findings):
Objective findings are the changes or deviations from normal
Treatment plan:
Treatment plan may take one of two forms:
A. Emergency
Treatment plan:
Treatment plan may take one of two forms:
A. Emergency
The diagnostic method
It is the application of a scientific method to
The diagnostic method
It is the application of a scientific method to
1-Collection of information for reaching a diagnosis include:
1 –
1-Collection of information for reaching a diagnosis include:
1 –
2 - Evaluation of the information
It is the organization
2 - Evaluation of the information
It is the organization
Methods for obtaining a patient's history
The primary methods for obtaining a
Methods for obtaining a patient's history
The primary methods for obtaining a
II – Chief complaint (cc)
The chief complaint (cc) is a statement
II – Chief complaint (cc)
The chief complaint (cc) is a statement
Common chief complaints
Usually the patient comes to the dental clinic complaining
Common chief complaints
Usually the patient comes to the dental clinic complaining
PAIN
PAIN
3 – Paraesthesia and numbness
Caused by vitamin deficiency, pressure on the
3 – Paraesthesia and numbness
Caused by vitamin deficiency, pressure on the
4 - Sensitivity
Sensitivity to hot, cold and sweats may result
4 - Sensitivity
Sensitivity to hot, cold and sweats may result
6 – Swelling
- Soft tissue swelling such as:-
- facial
6 – Swelling
- Soft tissue swelling such as:-
- facial
7 – Oral ulceration
Ulceration of the oral mucous membrane are multiple
7 – Oral ulceration
Ulceration of the oral mucous membrane are multiple
8 – T.M.J. disorders
Patients with T.M.J. disorders may complaint of:-
8 – T.M.J. disorders
Patients with T.M.J. disorders may complaint of:-
9 – Functional disorders
The patient complaint may result from functional
9 – Functional disorders
The patient complaint may result from functional
10 – Bad breath (halitosis)
It results from either extra-oral or
10 – Bad breath (halitosis)
It results from either extra-oral or
11- Esthetic problem
Orthodontic treatment or malposed teeth may be the only
11- Esthetic problem
Orthodontic treatment or malposed teeth may be the only
Chief complaint chart
Chief complaint C/c …………………………………………….………………………………………………………………………
History of chief
Chief complaint chart
Chief complaint C/c …………………………………………….………………………………………………………………………
History of chief
![[1] Onset a - Character b - Date Sudden (abrupt)](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/283565/slide-26.jpg)
[1] Onset a - Character
b - Date
Sudden (abrupt)
a) Character
[1] Onset a - Character
b - Date
Sudden (abrupt)
a) Character
Gradual onset = (1) Chronic inflammatory
conditions
(2) Neoplastic lesions
.
Gradual onset = (1) Chronic inflammatory
conditions
(2) Neoplastic lesions
.
![[2] Duration: Recorded is hours, days, weeks, months, years, including](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/283565/slide-28.jpg)
[2] Duration:
Recorded is hours, days, weeks, months, years, including periods
[2] Duration:
Recorded is hours, days, weeks, months, years, including periods
![[3] Character and severity : Severity : (Mainly of pain)](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/283565/slide-29.jpg)
[3] Character and severity :
Severity :
(Mainly of pain) :
[3] Character and severity :
Severity :
(Mainly of pain) :
Character : of pain may be
(1) Throbbing pain
means fluid
Character : of pain may be
(1) Throbbing pain
means fluid
![[4] Location and site: * Location : - The anatomical](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/283565/slide-31.jpg)
[4] Location and site:
* Location :
- The
[4] Location and site:
* Location :
- The
![[5] Course: Could be recorded as: Progressive: (increasing in severity)](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/283565/slide-32.jpg)
[5] Course:
Could be recorded as:
Progressive:
(increasing in severity)
[5] Course:
Could be recorded as:
Progressive:
(increasing in severity)
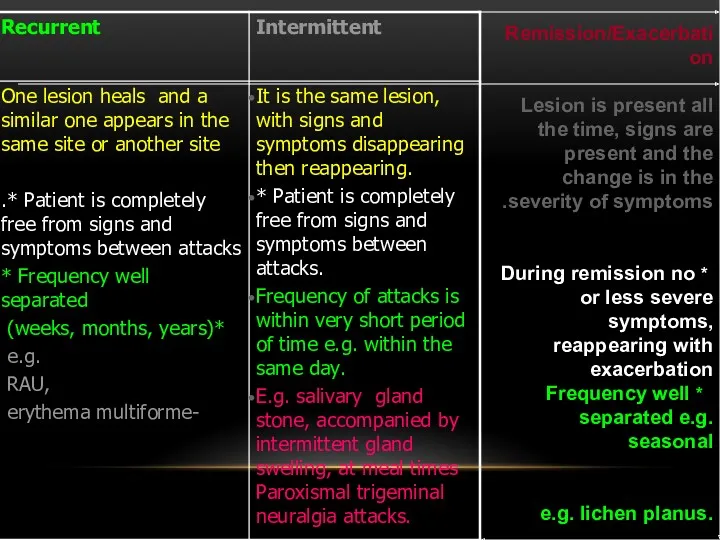
Remission/Exacerbation
Lesion is present all the time, signs are present and the
Remission/Exacerbation
Lesion is present all the time, signs are present and the
![[6] History of recurrence: The history of previous occurrence of](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/283565/slide-34.jpg)
[6] History of recurrence:
The history of previous occurrence of the
[6] History of recurrence:
The history of previous occurrence of the
![[8] Precipitating factors and relation to other activities:- *Pain may](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/283565/slide-35.jpg)
[8] Precipitating factors and relation to other activities:-
*Pain may increase by eating,
[8] Precipitating factors and relation to other activities:-
*Pain may increase by eating,
![[9] Relieving factors: Factors which relieve chief complaint e.g.:- -](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/283565/slide-36.jpg)
[9] Relieving factors:
Factors which relieve chief complaint e.g.:-
- Rest,
[9] Relieving factors:
Factors which relieve chief complaint e.g.:-
- Rest,
![[10] Associated phenomena: These are manifestations associated with the complaint:](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/283565/slide-37.jpg)
[10] Associated phenomena:
These are manifestations associated with the complaint:
●
[10] Associated phenomena:
These are manifestations associated with the complaint:
●
![[11] Previous medication: Mouth washes, analgesics, antibiotics, previously used by](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/283565/slide-38.jpg)
[11] Previous medication:
Mouth washes, analgesics, antibiotics, previously used by the patient,
[11] Previous medication:
Mouth washes, analgesics, antibiotics, previously used by the patient,
EXTRA ORAL EXAMINATION
INTRA ORAL EXAMINATION
CLINICAL EXAMINATION
Inspection – palpation –
EXTRA ORAL EXAMINATION
INTRA ORAL EXAMINATION
CLINICAL EXAMINATION
Inspection – palpation –
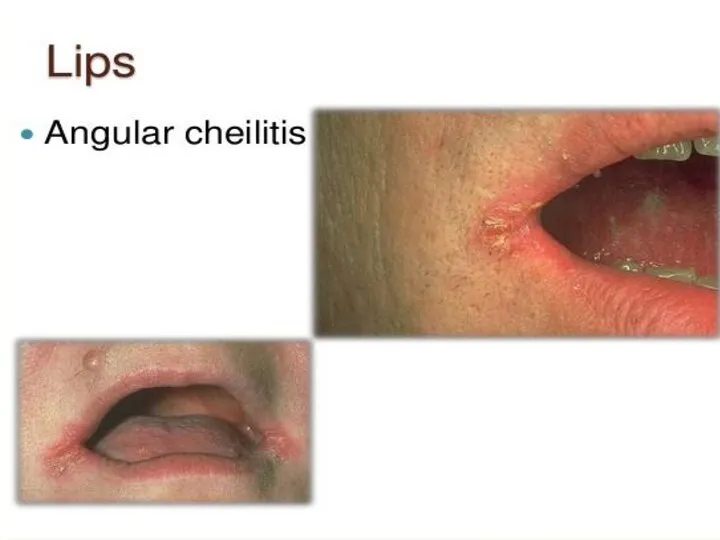

ANGULAR CHEILITIS
ANGULAR CHEILITIS
Dr.Anas Almisurati
Dr.Anas Almisurati
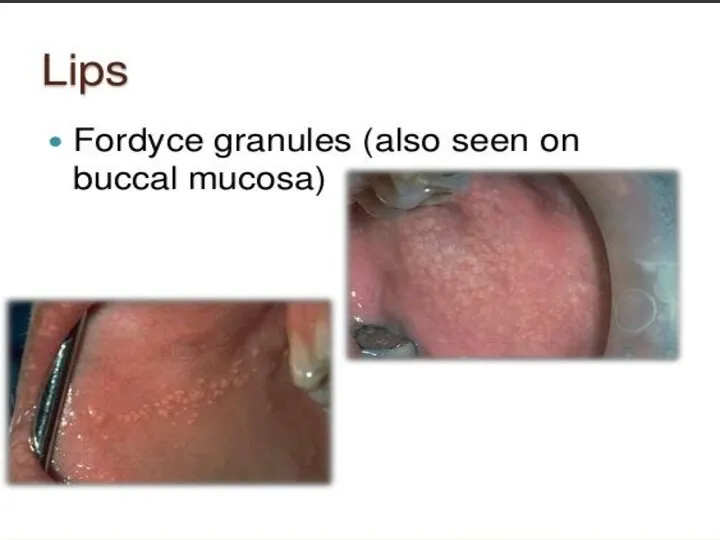
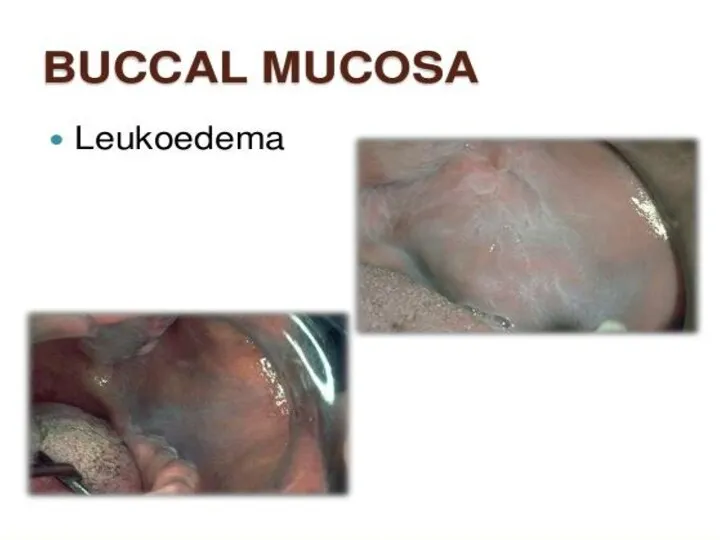
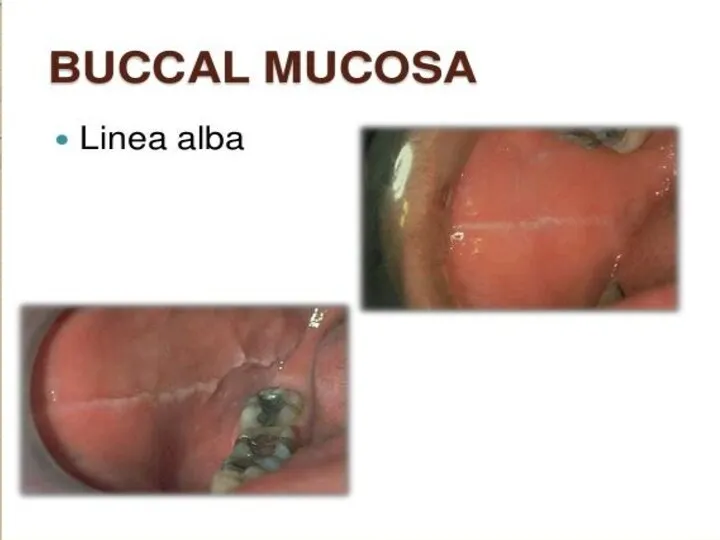
NORMAL ORAL MUCOSA
Normal oral mucosa with variation in structure and appearance
NORMAL ORAL MUCOSA
Normal oral mucosa with variation in structure and appearance
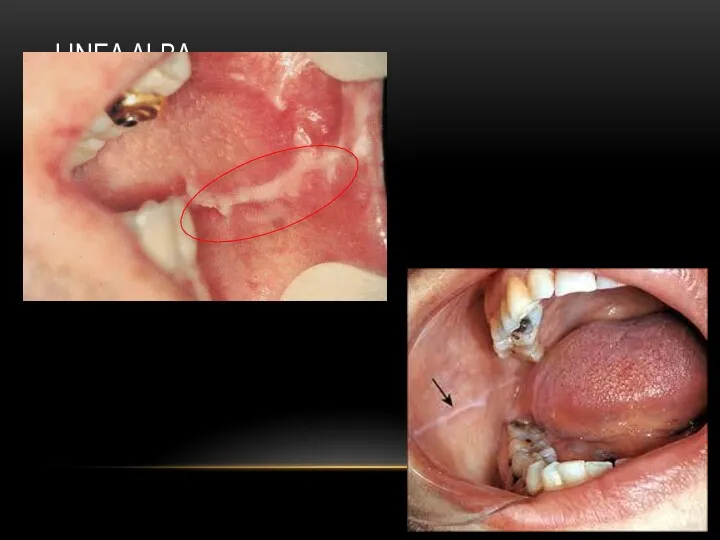
LINEA ALBA
LINEA ALBA
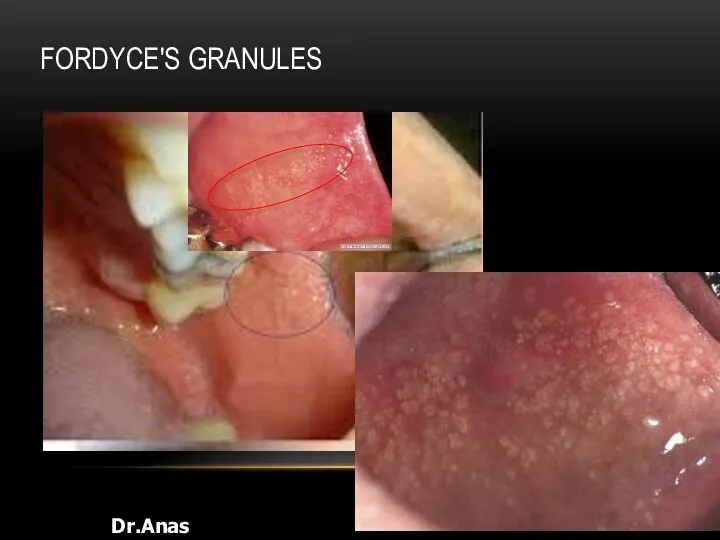
FORDYCE'S GRANULES
Dr.Anas Almisurati
FORDYCE'S GRANULES
Dr.Anas Almisurati

KERATOTIC LESION
Keratotic lesion (can’t rubbed off) :-
1- oral keratosis
2- leukoplakia
3-
KERATOTIC LESION
Keratotic lesion (can’t rubbed off) :-
1- oral keratosis
2- leukoplakia
3-
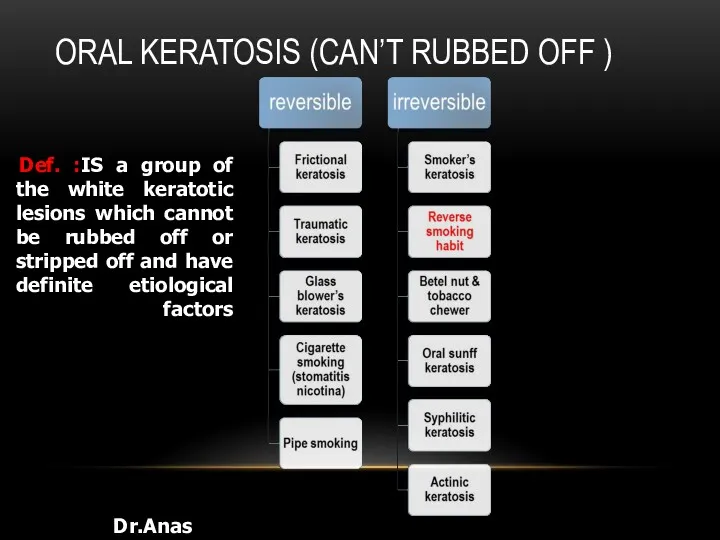
ORAL KERATOSIS (CAN’T RUBBED OFF )
Dr.Anas Almisurati
Def. :IS a group of
ORAL KERATOSIS (CAN’T RUBBED OFF )
Dr.Anas Almisurati
Def. :IS a group of
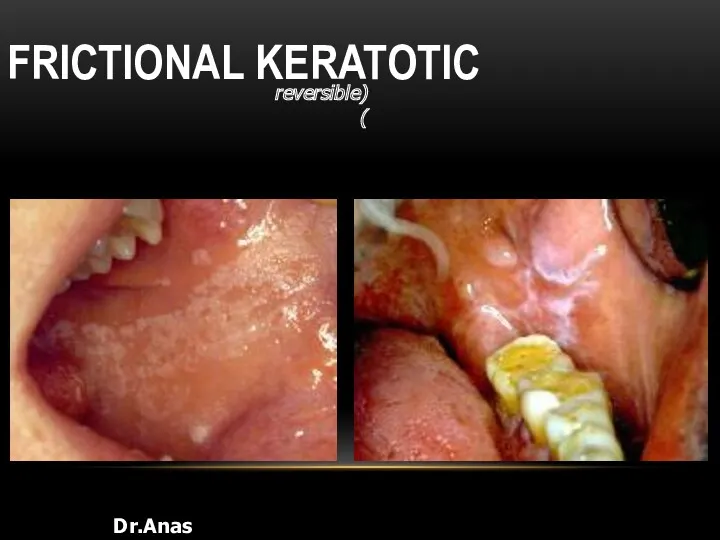
FRICTIONAL KERATOTIC
Dr.Anas Almisurati
(reversible)
FRICTIONAL KERATOTIC
Dr.Anas Almisurati
(reversible)
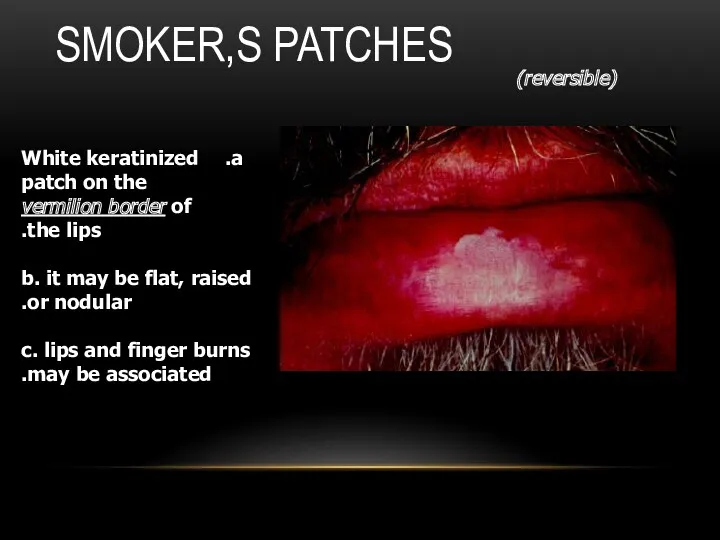
SMOKER,S PATCHES
(reversible)
White keratinized patch on the vermilion border of the lips.
b.
SMOKER,S PATCHES
(reversible)
White keratinized patch on the vermilion border of the lips.
b.
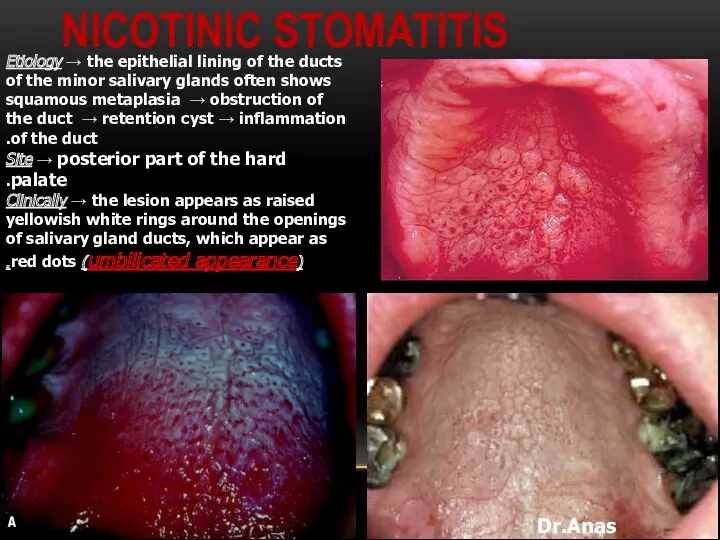
NICOTINIC STOMATITIS
Dr.Anas Almisurati
Etiology → the epithelial lining of the ducts
NICOTINIC STOMATITIS
Dr.Anas Almisurati
Etiology → the epithelial lining of the ducts
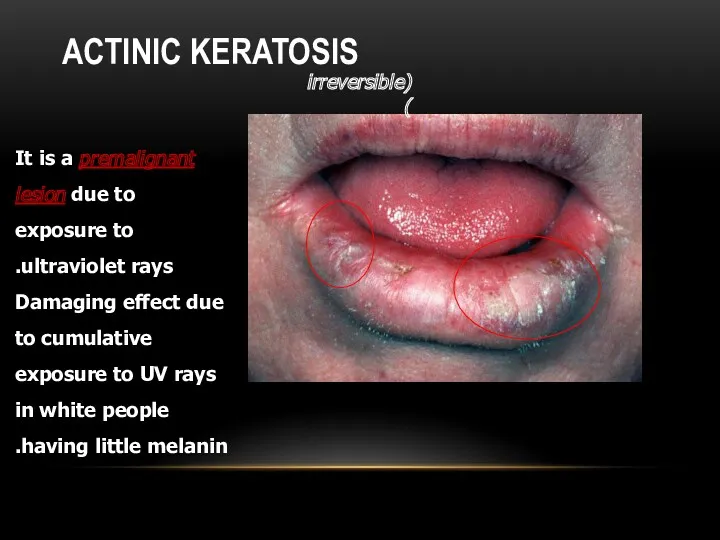
ACTINIC KERATOSIS
(irreversible)
It is a premalignant lesion due to exposure to
ACTINIC KERATOSIS
(irreversible)
It is a premalignant lesion due to exposure to
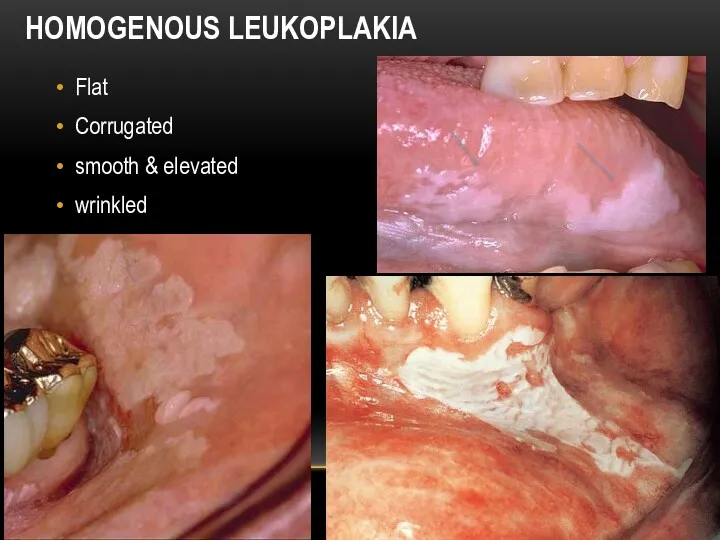
HOMOGENOUS LEUKOPLAKIA
Flat
Corrugated
smooth & elevated
wrinkled
HOMOGENOUS LEUKOPLAKIA
Flat
Corrugated
smooth & elevated
wrinkled

SPECKLED LEUKOPLAKIA
corner of the mouth.
white patches (keratotic) on erythematous base (atrophic
SPECKLED LEUKOPLAKIA
corner of the mouth.
white patches (keratotic) on erythematous base (atrophic
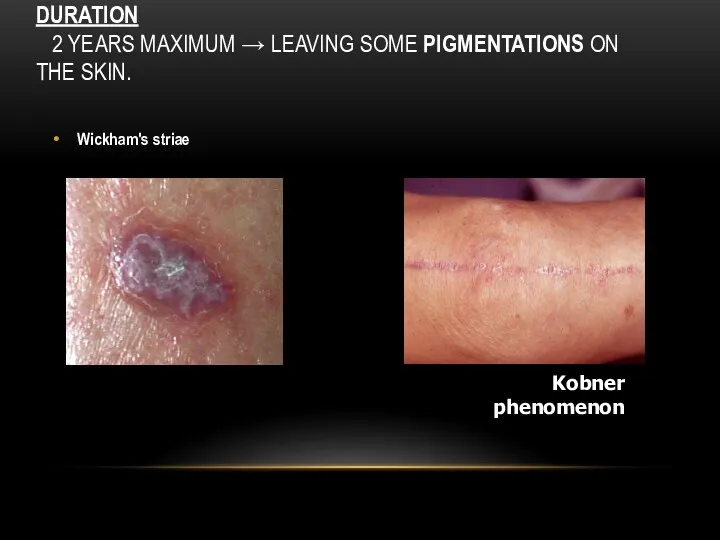
DURATION
2 YEARS MAXIMUM → LEAVING SOME PIGMENTATIONS ON THE SKIN.
Wickham's
DURATION
2 YEARS MAXIMUM → LEAVING SOME PIGMENTATIONS ON THE SKIN.
Wickham's

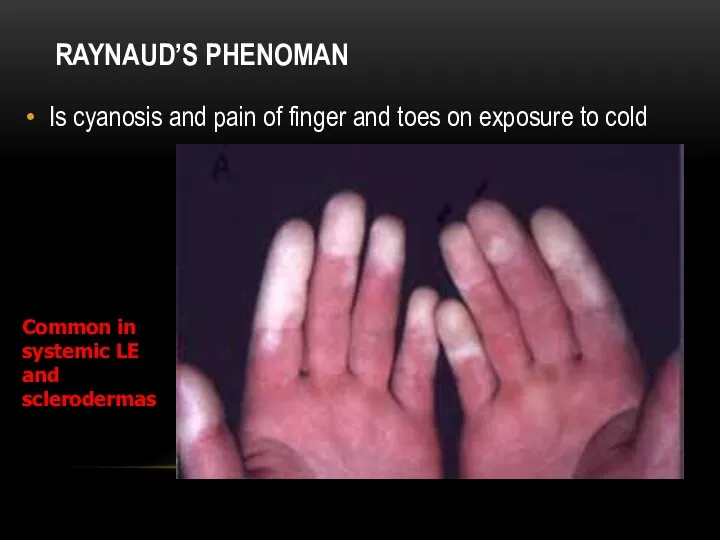
RAYNAUD’S PHENOMAN
Is cyanosis and pain of finger and toes on exposure
RAYNAUD’S PHENOMAN
Is cyanosis and pain of finger and toes on exposure
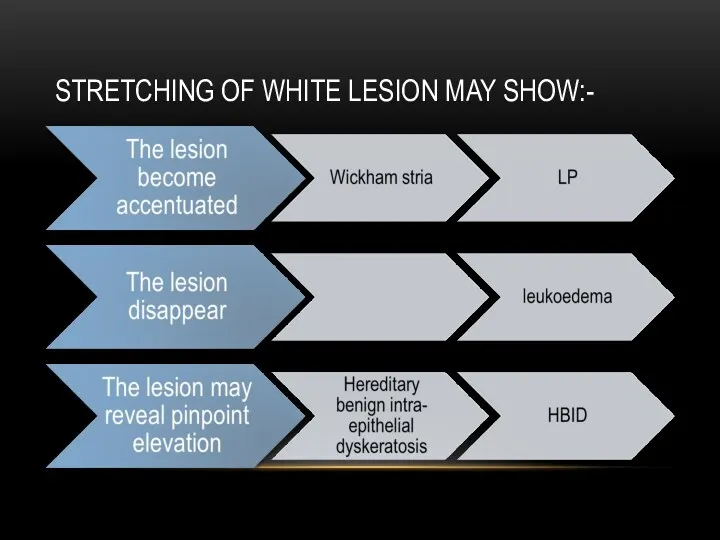
STRETCHING OF WHITE LESION MAY SHOW:-
STRETCHING OF WHITE LESION MAY SHOW:-

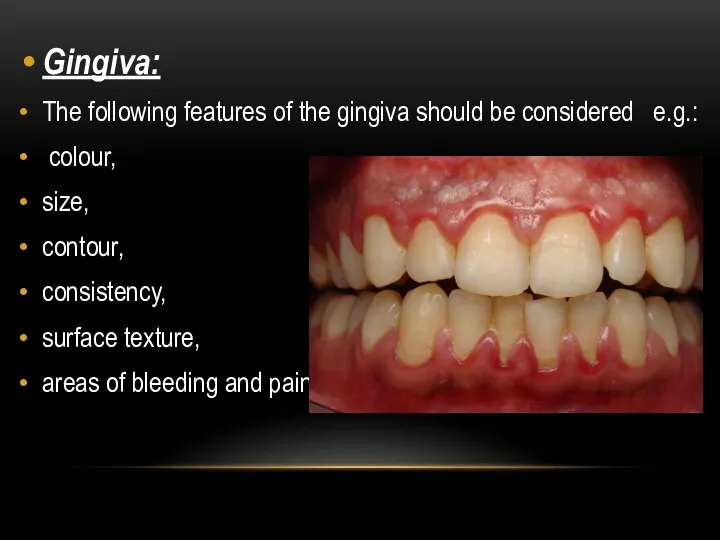
Gingiva:
The following features of the gingiva should be considered e.g.:
colour,
Gingiva:
The following features of the gingiva should be considered e.g.:
colour,

MARGINAL GINGIVAL INFLAMMATION
MARGINAL GINGIVAL INFLAMMATION
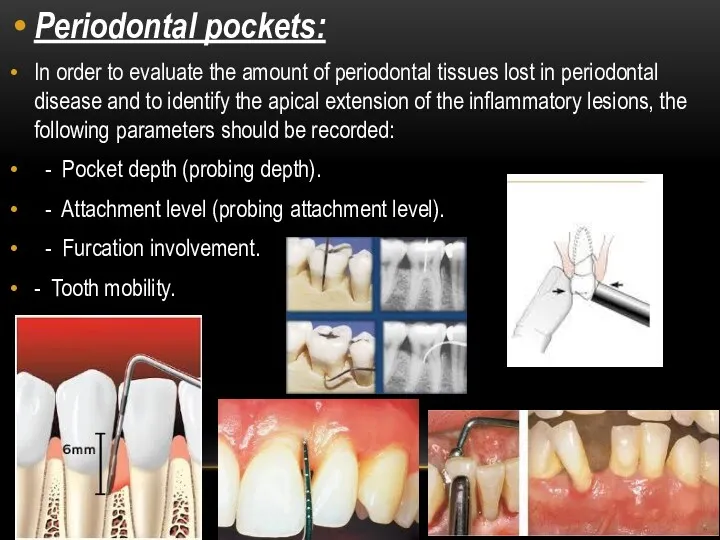
Periodontal pockets:
In order to evaluate the amount of periodontal tissues lost
Periodontal pockets:
In order to evaluate the amount of periodontal tissues lost




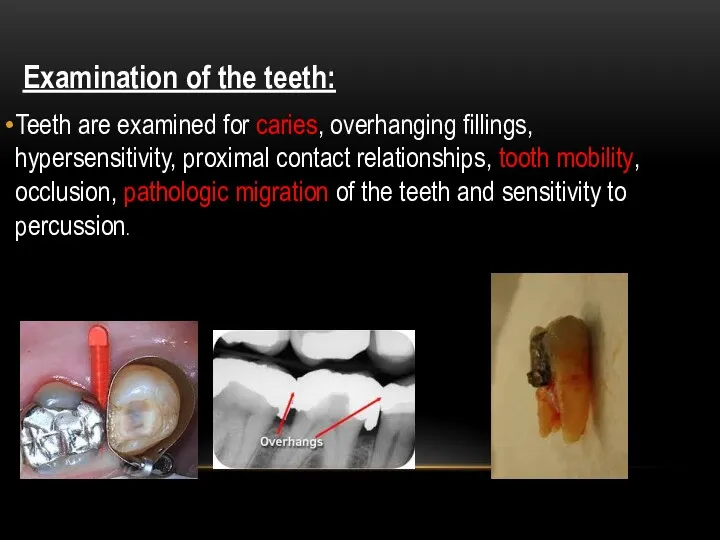
Examination of the teeth:
Teeth are examined for caries, overhanging fillings,
Examination of the teeth:
Teeth are examined for caries, overhanging fillings,

- History of habits:
Clenching or grinding the teeth.
Tongue thrusting.
Smoking.
- History of habits:
Clenching or grinding the teeth.
Tongue thrusting.
Smoking.
GENERAL APPRAISAL
SKULL ( CRANIUM)
FACE
EYE
NOSE
HAIR
SKIN
JAWS & TMJ
SALIVARY GLANDS
LYMPH NODES
THYROID GLAND
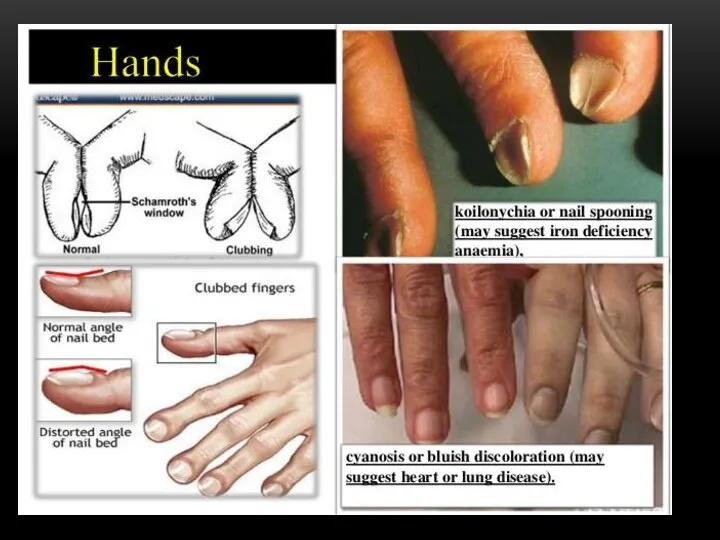
HANDS
GENERAL APPRAISAL
SKULL ( CRANIUM)
FACE
EYE
NOSE
HAIR
SKIN
JAWS & TMJ
SALIVARY GLANDS
LYMPH NODES
THYROID GLAND
HANDS
GENERAL APPRAISAL
Starts while patient entering the clinic.
Performed without patient interruption.
Report, record,
GENERAL APPRAISAL
Starts while patient entering the clinic.
Performed without patient interruption.
Report, record,
1. Physical structure ( body type )
- asthenic : slender
1. Physical structure ( body type )
- asthenic : slender
3. Body weight
over, under or normal
4. Behavior
lazy, nervous, irritable or
over, under or normal
4. Behavior
lazy, nervous, irritable or
7. Recording vital signs
temperature 37 normal
pulse rate 72 B/M normal
blood pressure 80/120 normal
7. Recording vital signs
temperature 37 normal
pulse rate 72 B/M normal
blood pressure 80/120 normal
SKULL AND CRANIUM
Size : from supra orbital ridge to occipital protuberance.
-
SKULL AND CRANIUM
Size : from supra orbital ridge to occipital protuberance.
-
CONGENITAL SYPHILIS
CONGENITAL SYPHILIS
PAGET,S DISEASE
PAGET,S DISEASE
THE FACE
Characteristic face pattern
1. Acromegalic face: coarse features prognathism prominent
THE FACE
Characteristic face pattern
1. Acromegalic face: coarse features prognathism prominent
ACROMEGALY
ACROMEGALY
ACROMEGALY
ACROMEGALY
ACROMEGALY
ACROMEGALY
THYROTOXICOSIS
THYROTOXICOSIS
MOON FACE
MOON FACE
CORTISONE THERAPY
CORTISONE THERAPY
OBESITY
OBESITY
5. Nephrotic face : puffy, pale with baggy eyelids
6. Sclerodermic face:
5. Nephrotic face : puffy, pale with baggy eyelids
6. Sclerodermic face:
Mongoloid patient
Mongoloid patient

DOWN,S SYNDROME
DOWN,S SYNDROME

Mouth breather
Cracked lips
Macroglossia
Fissured tongue
Cleft lip or palate
Poor oral hygiene
Short roots
Mouth breather
Cracked lips
Macroglossia
Fissured tongue
Cleft lip or palate
Poor oral hygiene
Short roots

Clinical findings
Clinical findings
LUPUS ERYTHEMATOSIS
LUPUS ERYTHEMATOSIS
Mandibular canal enlargement (lip numbness).
Macroglossia,fissuring and precancerous
NEUROFIBROMATOSIS
Mandibular canal enlargement (lip numbness).
Macroglossia,fissuring and precancerous
NEUROFIBROMATOSIS
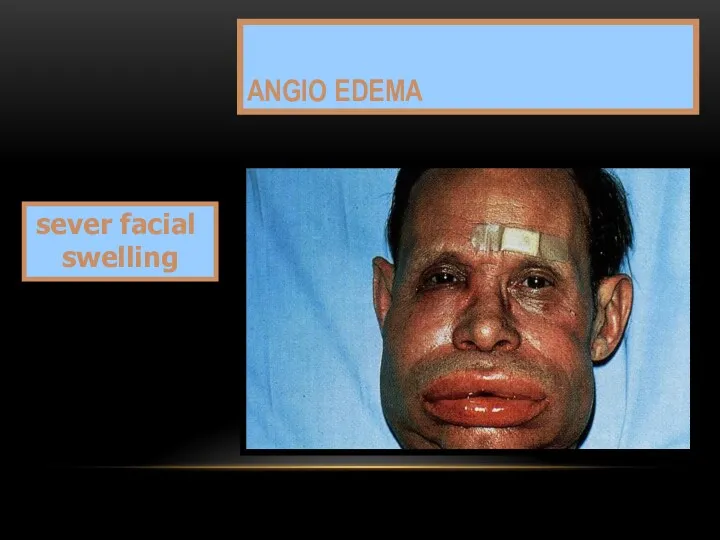
ANGIO EDEMA
sever facial swelling
ANGIO EDEMA
sever facial swelling

Third molars
ext
SURGICAL TRAUMA
Post operative
Two weeks later
Third molars
ext
SURGICAL TRAUMA
Post operative
Two weeks later
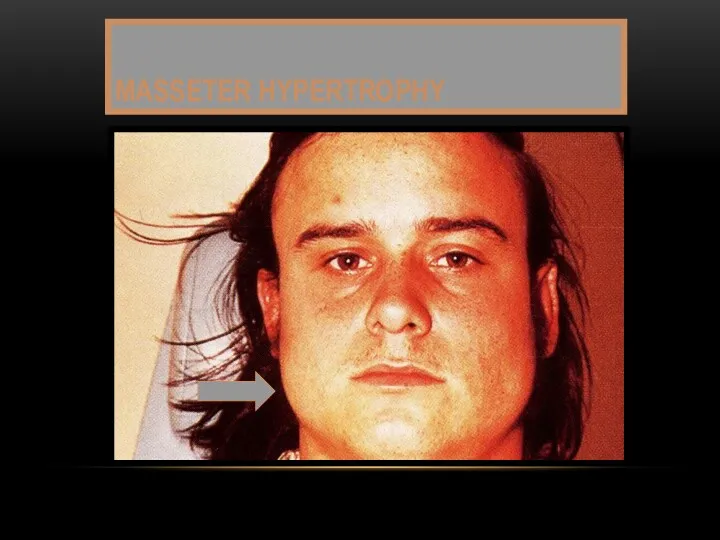
MASSETER HYPERTROPHY
MASSETER HYPERTROPHY
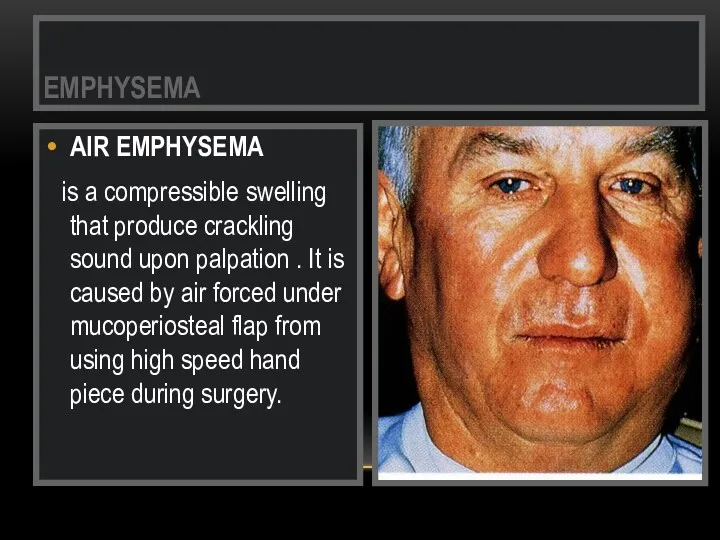
AIR EMPHYSEMA
is a compressible swelling that produce crackling sound
AIR EMPHYSEMA
is a compressible swelling that produce crackling sound
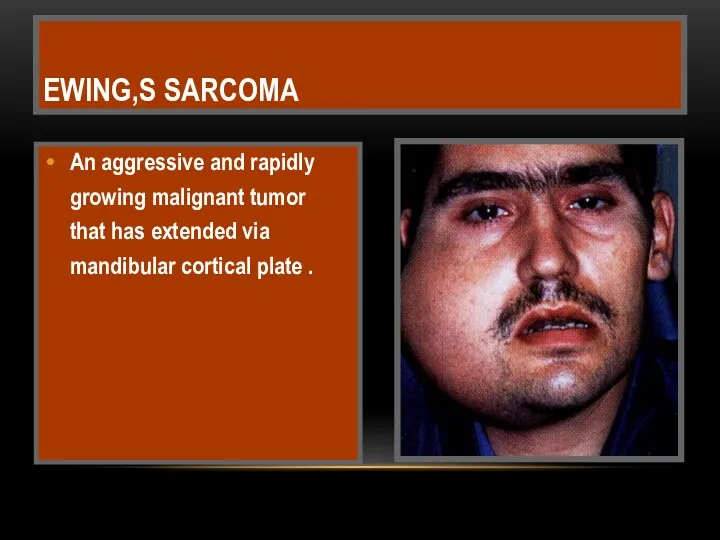
An aggressive and rapidly growing malignant tumor that has extended via
An aggressive and rapidly growing malignant tumor that has extended via
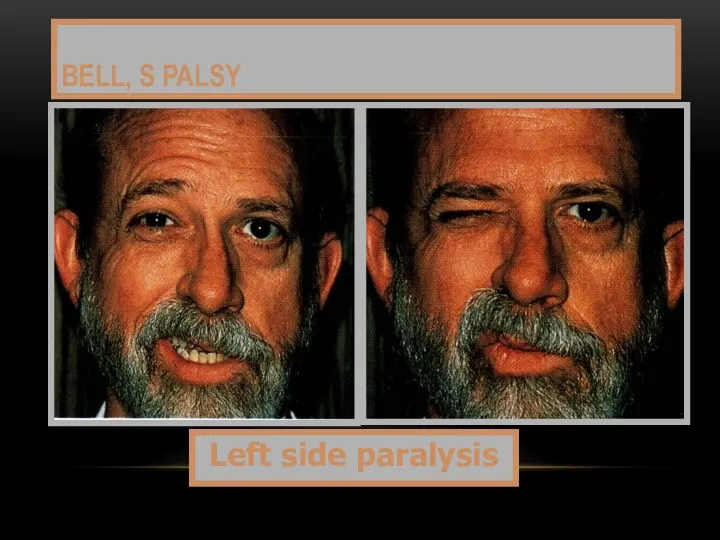
BELL, S PALSY
Left side paralysis
BELL, S PALSY
Left side paralysis

HERPES ZOSTER
Chicken pox is the primary infection by Varicella – Zoster
HERPES ZOSTER
Chicken pox is the primary infection by Varicella – Zoster

Shingles affects skin by vesicles and pustules that ruptures to form
Shingles affects skin by vesicles and pustules that ruptures to form
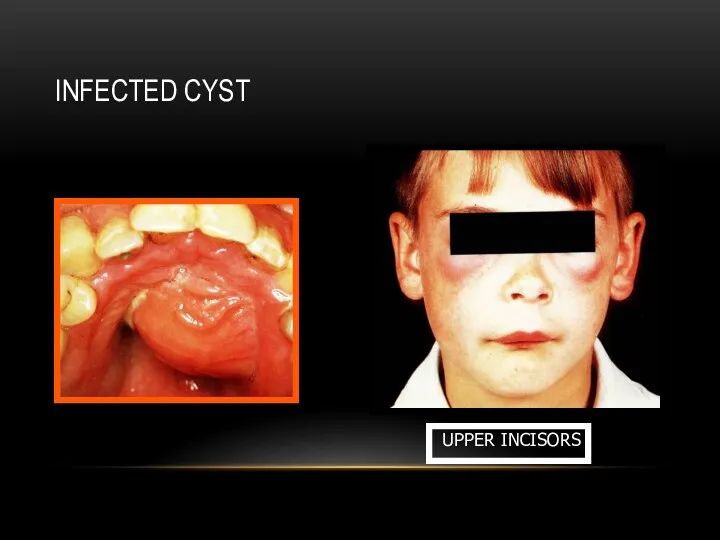
INFECTED CYST
UPPER INCISORS
INFECTED CYST
UPPER INCISORS
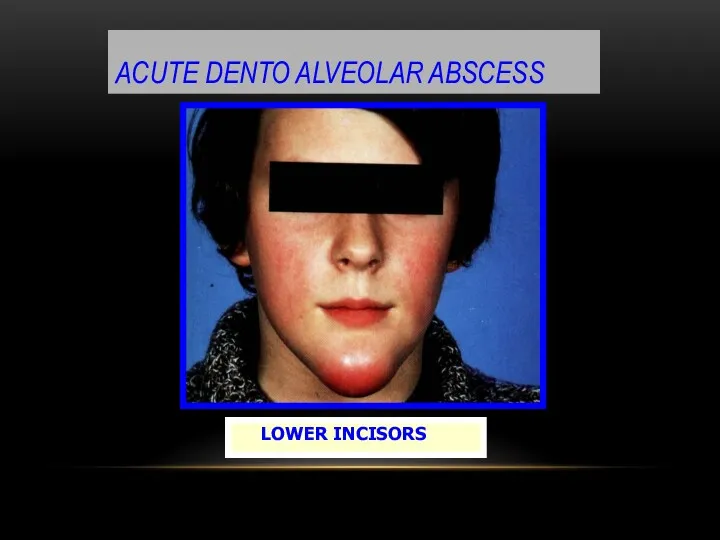
ACUTE DENTO ALVEOLAR ABSCESS
LOWER INCISORS
ACUTE DENTO ALVEOLAR ABSCESS
LOWER INCISORS
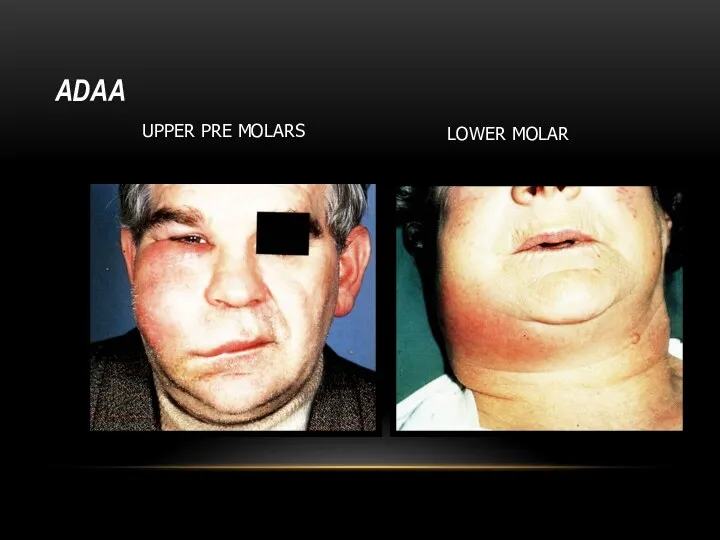
ADAA
UPPER PRE MOLARS
LOWER MOLAR
ADAA
UPPER PRE MOLARS
LOWER MOLAR
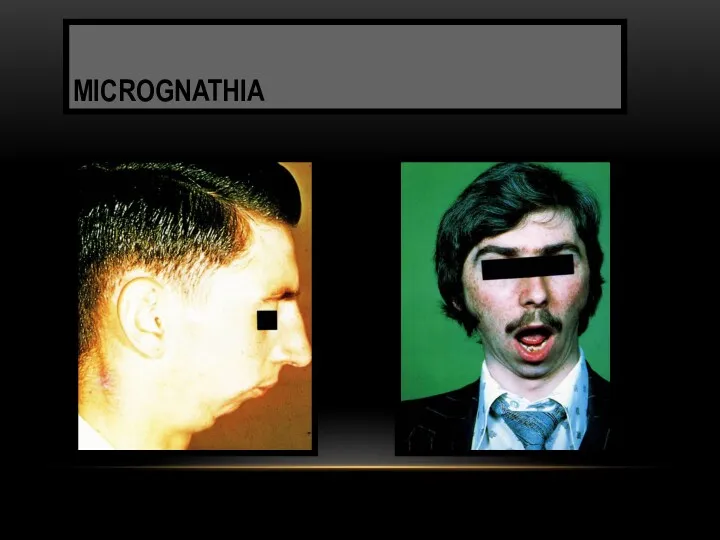
MICROGNATHIA
MICROGNATHIA
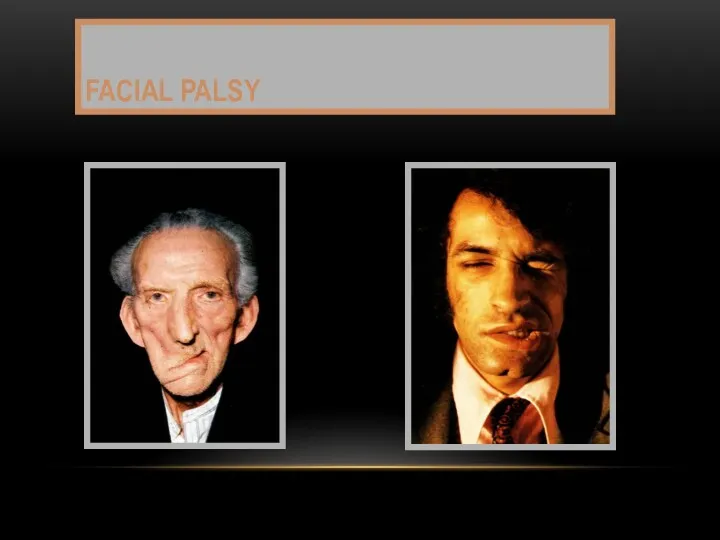
FACIAL PALSY
FACIAL PALSY
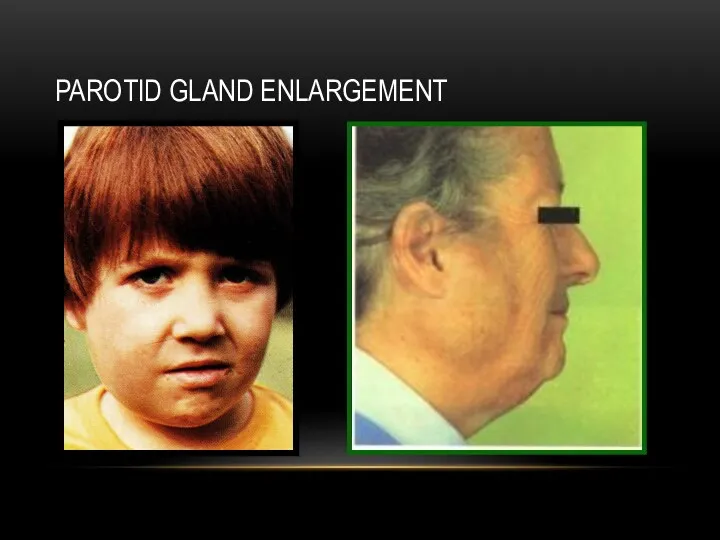
PAROTID GLAND ENLARGEMENT
PAROTID GLAND ENLARGEMENT
SALIVARY CALCULI
SALIVARY CALCULI
THE NOSE
Nasal abnormalities may be interrelated to oral lesions.
The following
THE NOSE
Nasal abnormalities may be interrelated to oral lesions.
The following
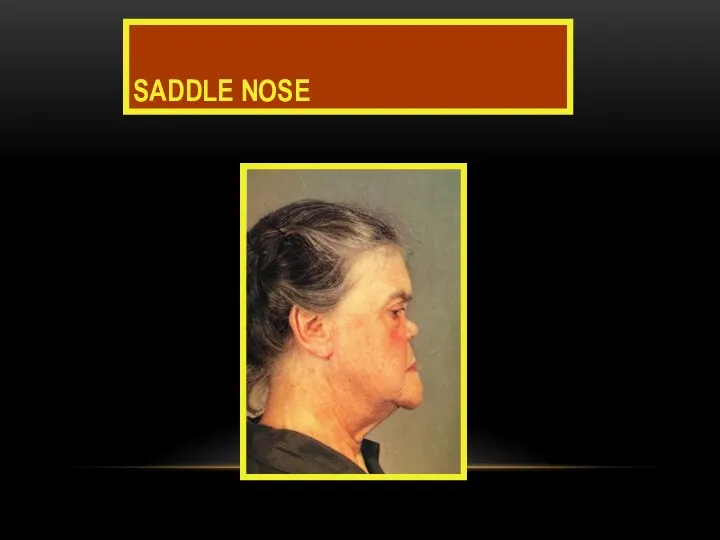
SADDLE NOSE
SADDLE NOSE
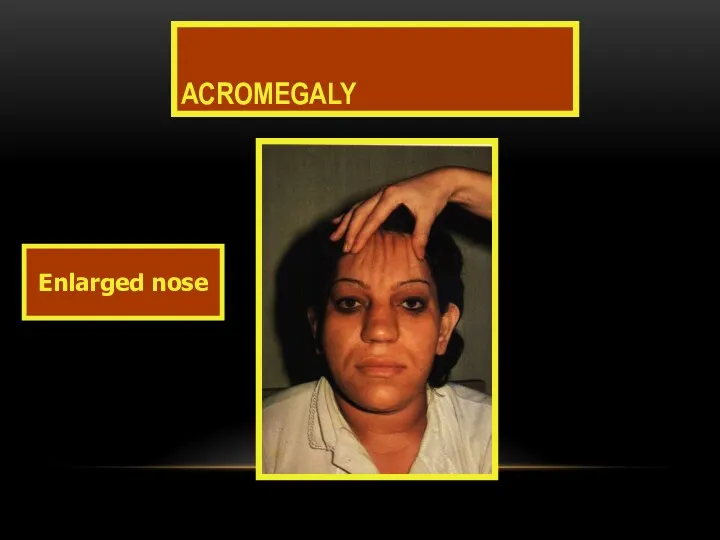
ACROMEGALY
Enlarged nose
ACROMEGALY
Enlarged nose
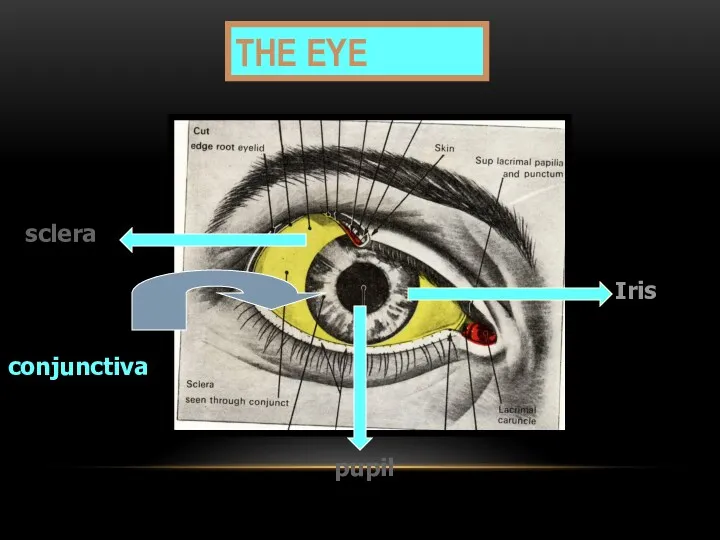
THE EYE
sclera
pupil
Iris
conjunctiva
THE EYE
sclera
pupil
Iris
conjunctiva
1) Ptosis
- Dropping of upper eye lid
- Inability to open the
1) Ptosis
- Dropping of upper eye lid
- Inability to open the
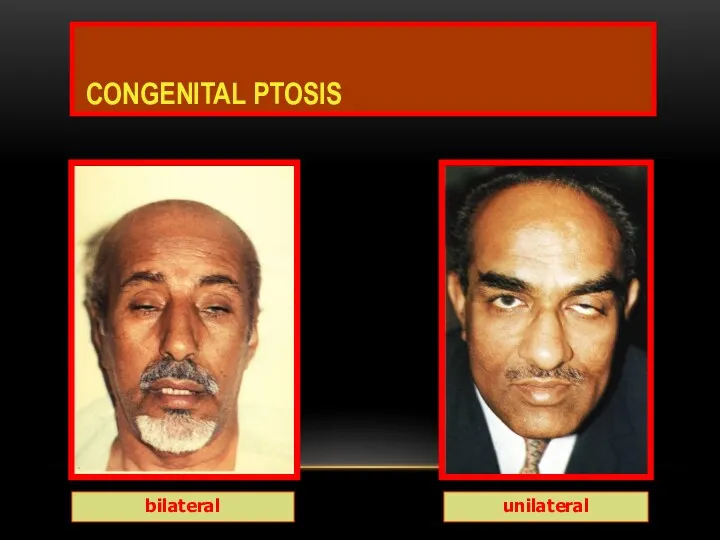
CONGENITAL PTOSIS
bilateral
unilateral
CONGENITAL PTOSIS
bilateral
unilateral
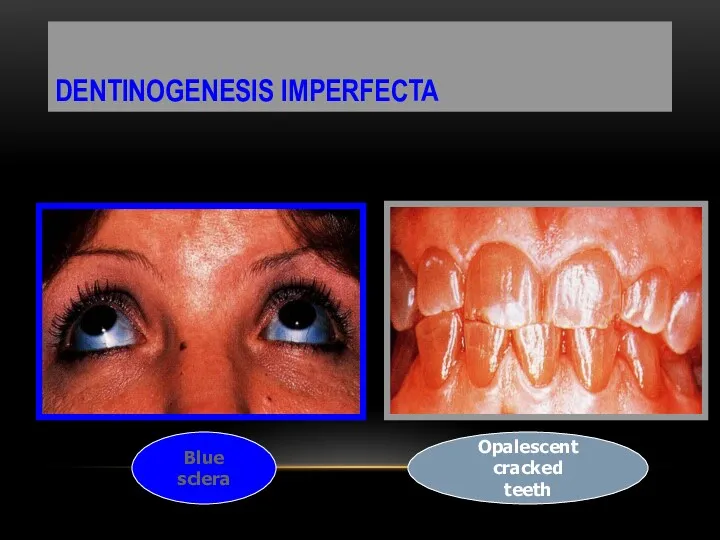
DENTINOGENESIS IMPERFECTA
Blue sclera
Opalescent cracked
teeth
DENTINOGENESIS IMPERFECTA
Blue sclera
Opalescent cracked
teeth
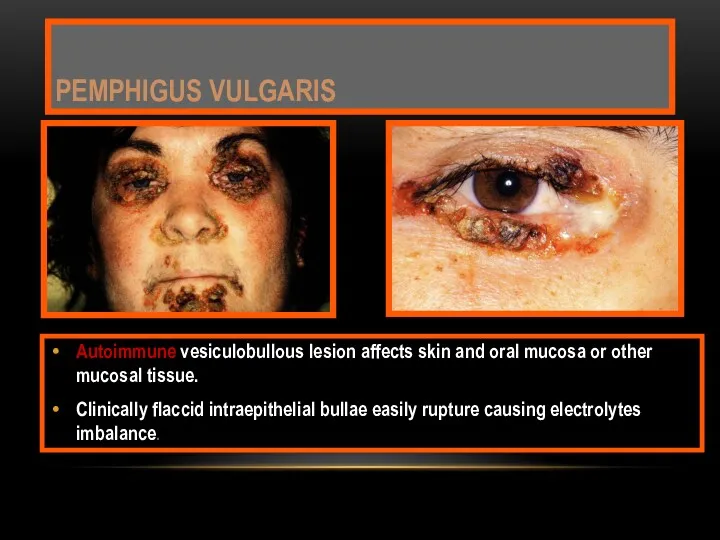
Autoimmune vesiculobullous lesion affects skin and oral mucosa or other mucosal
Autoimmune vesiculobullous lesion affects skin and oral mucosa or other mucosal
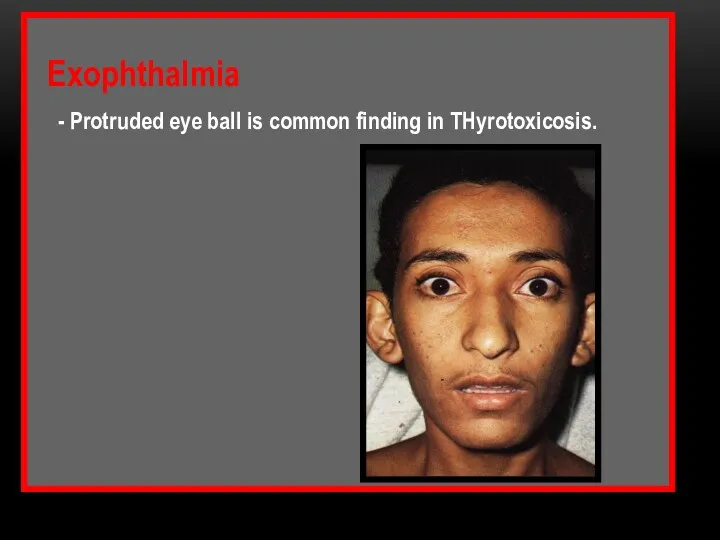
Exophthalmia
- Protruded eye ball is common finding in
Exophthalmia
- Protruded eye ball is common finding in

CONJUNCTIVITIS
Behcet,s
REITER,S
CONJUNCTIVITIS
Behcet,s
REITER,S
SYNDROMES AND OTHER DISEASES
Muco Cutaneous Ocular Syndromes
1- STEVEN JHONSON
SYNDROMES AND OTHER DISEASES
Muco Cutaneous Ocular Syndromes
1- STEVEN JHONSON
THE SKIN
The skin should be inspected for :
color changes,
pigmented
THE SKIN
The skin should be inspected for :
color changes,
pigmented
Palpation is used to examine surface texture changes and to check
Palpation is used to examine surface texture changes and to check
Skin color
- Depends mainly on the amount deposited pigmented
Skin color
- Depends mainly on the amount deposited pigmented
Increased melanin physiologically in pregnancy or pathologically as in Addison’s disease.
-
Increased melanin physiologically in pregnancy or pathologically as in Addison’s disease.
-
- Bluish or cyanotic color occurs due to stagnation of reduced
- Bluish or cyanotic color occurs due to stagnation of reduced

PRECERVICAL
CERVICAL
Superficial cervical
Anterior cervical
Deep cervical
Outer circle
inner circle
Palatine
Pharyngeal
Lingual
Mastoid
Occipital
PRECERVICAL
CERVICAL
Superficial cervical
Anterior cervical
Deep cervical
Outer circle
inner circle
Palatine
Pharyngeal
Lingual
Mastoid
Occipital
PRE-CERVICAL GROUP
Inner Circle lymphoid tissue around pharynx
1) Palatine at the mucous
PRE-CERVICAL GROUP
Inner Circle lymphoid tissue around pharynx
1) Palatine at the mucous
3) Lingual lymphoid aggregations mostly at dorsal & lateral aspects of
3) Lingual lymphoid aggregations mostly at dorsal & lateral aspects of
Drainage all lymphoid tissue of inner circle drains into deep cervical.
Drainage all lymphoid tissue of inner circle drains into deep cervical.
Outer Circle
1) Occipital drain posterior part of scalp.
2) Mastoid drain parietal
Outer Circle
1) Occipital drain posterior part of scalp.
2) Mastoid drain parietal
5) Submandibular (submax.)
- Medial part of eye lid.
- Nasal, cheek &
5) Submandibular (submax.)
- Medial part of eye lid.
- Nasal, cheek &
CERVICAL GROUP
1) Superficial Cervical group
- Below parotid gland, associated with
CERVICAL GROUP
1) Superficial Cervical group
- Below parotid gland, associated with
2) Anterior C.G (Pre-tracheal)
- It drains larynx, trachea & thyroid
2) Anterior C.G (Pre-tracheal)
- It drains larynx, trachea & thyroid
N.B.
Deep cervical drains
- Maxillary teeth, gum, hard palate and
N.B.
Deep cervical drains
- Maxillary teeth, gum, hard palate and
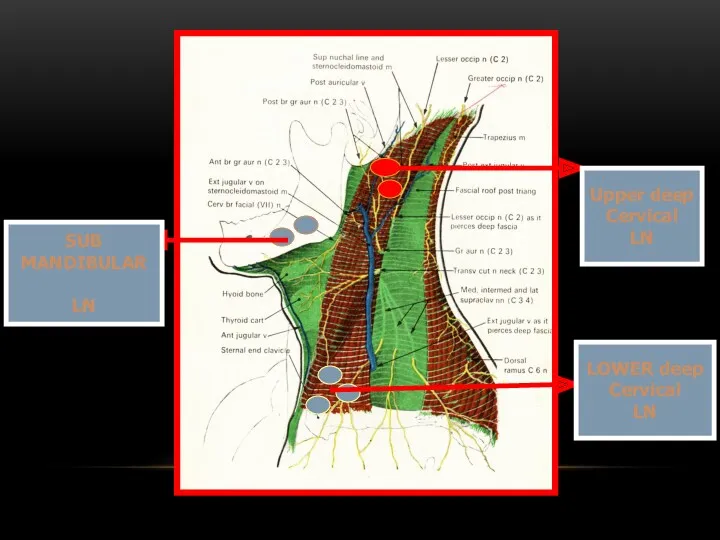
Upper deep
Cervical
LN
LOWER deep
Cervical
LN
SUB
MANDIBULAR
LN
Upper deep
Cervical
LN
LOWER deep
Cervical
LN
SUB
MANDIBULAR
LN
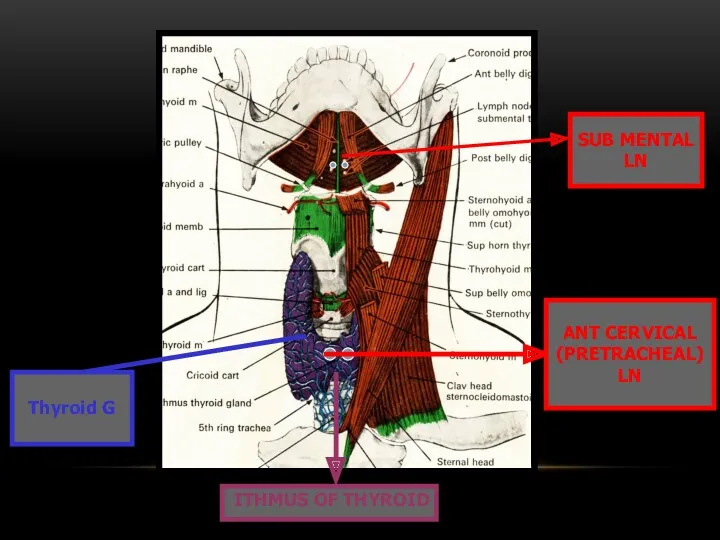
Thyroid G
SUB MENTAL
LN
ITHMUS OF THYROID
ANT CERVICAL
(PRETRACHEAL)
LN
Thyroid G
SUB MENTAL
LN
ITHMUS OF THYROID
ANT CERVICAL
(PRETRACHEAL)
LN
INNER CIRCLE
LN
INNER CIRCLE
LN

Lymph node enlargement
Localized factors
1. Infection
a) Acute: NUG, ADAA, AHGS, Chancre
b) Chronic:
Lymph node enlargement
Localized factors
1. Infection
a) Acute: NUG, ADAA, AHGS, Chancre
b) Chronic:
Generalized factors
1) Infection
a) Acute : infectious mononucleosis
b) Chronic : secondary stage
Generalized factors
1) Infection
a) Acute : infectious mononucleosis
b) Chronic : secondary stage
Other Causes :-
* Sarcoidosis
* S.L.E
* rheumatoid arthritis
* histoplasmosis
* phenytoin
Other Causes :-
* Sarcoidosis
* S.L.E
* rheumatoid arthritis
* histoplasmosis
* phenytoin
Lymph node should be examined for
- Being solitary or multiple.
- Unilateral
- Being solitary or multiple.
- Unilateral
The lymph node may be
- Tender, soft and discrete in acute
The lymph node may be
- Tender, soft and discrete in acute
Lab tests in LN enlargement diagnosis
1- Pulp test for tooth vitality.
2-
Lab tests in LN enlargement diagnosis
1- Pulp test for tooth vitality.
2-
5- Biopsy.
6- Smear & Culture in TB or Syphilis.
7-
5- Biopsy.
6- Smear & Culture in TB or Syphilis.
7-
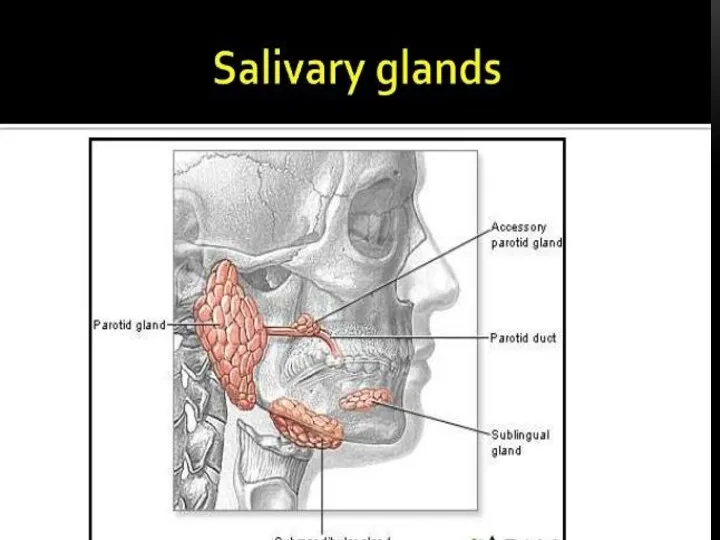
SALIVARY GLANDS
Enlargement of major salivary glands may be due to
SALIVARY GLANDS
Enlargement of major salivary glands may be due to
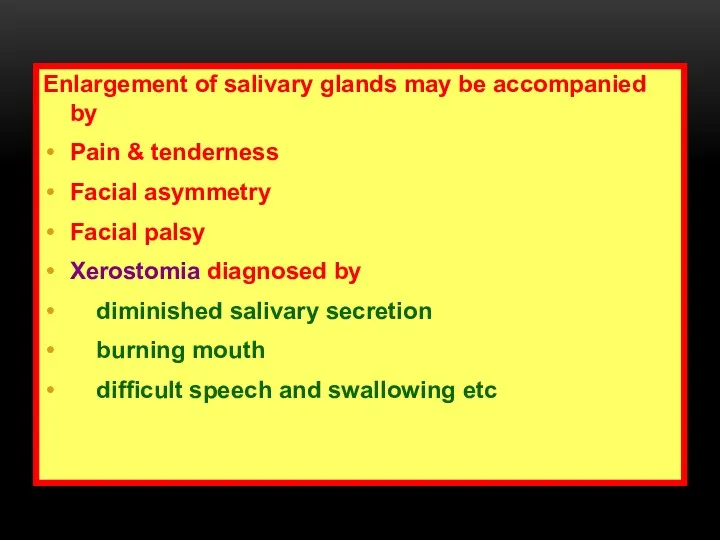
Enlargement of salivary glands may be accompanied by
Pain & tenderness
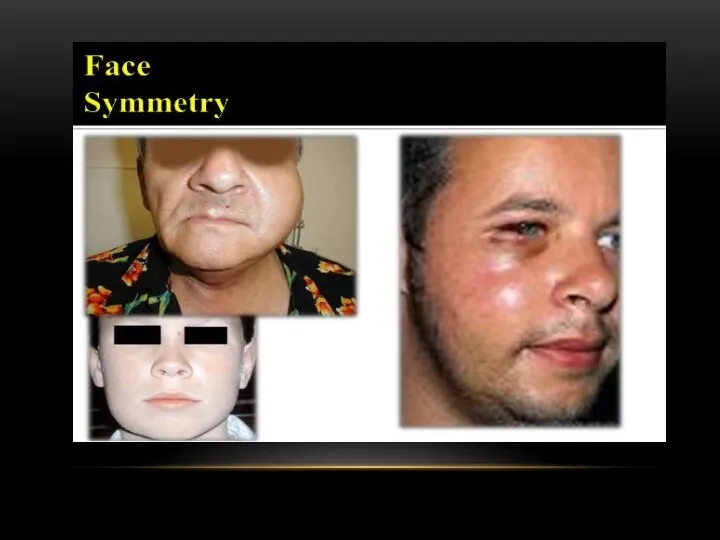
Facial asymmetry
Facial
Enlargement of salivary glands may be accompanied by
Pain & tenderness
Facial asymmetry
Facial
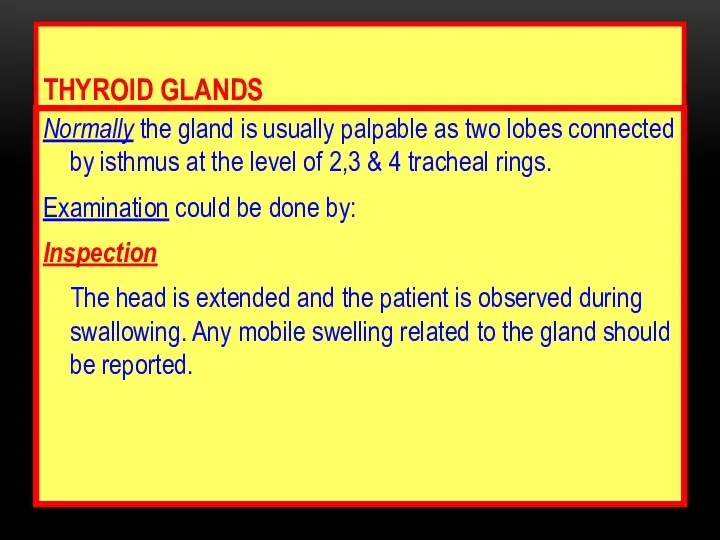
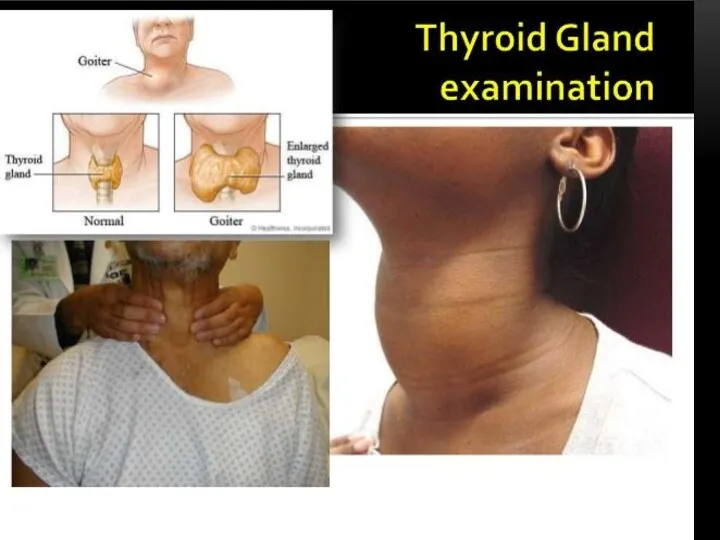
THYROID GLANDS
Normally the gland is usually palpable as two lobes connected
THYROID GLANDS
Normally the gland is usually palpable as two lobes connected

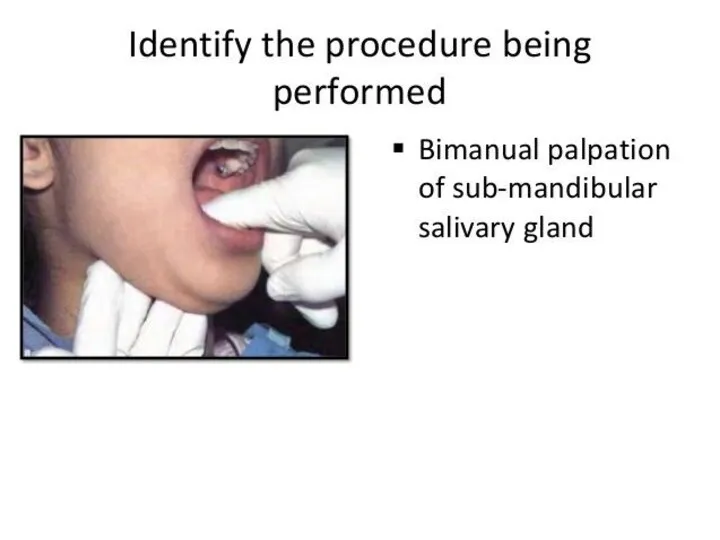
Palpation
The examiner should be behind the patient palpating the gland by
Palpation
The examiner should be behind the patient palpating the gland by
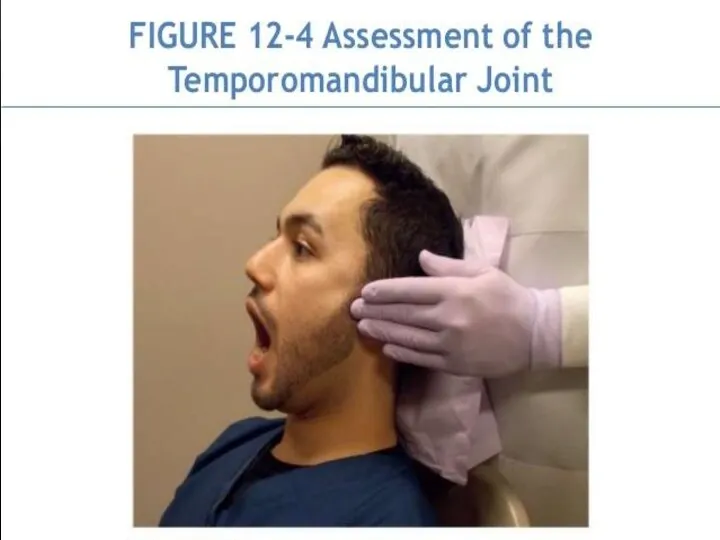
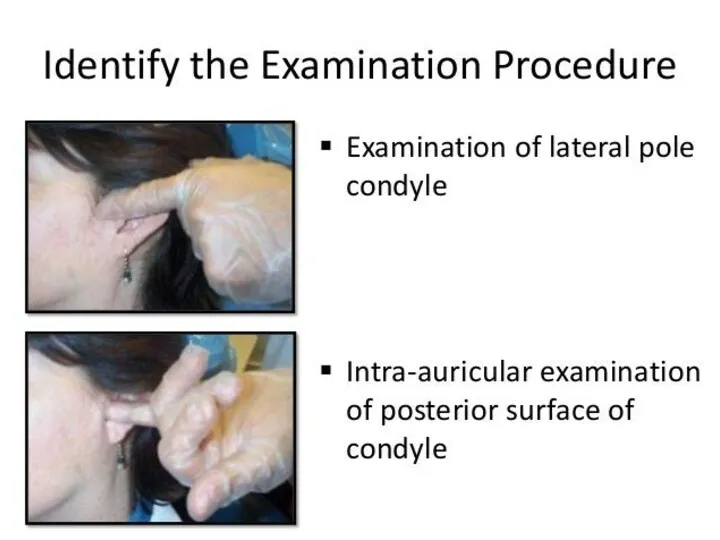
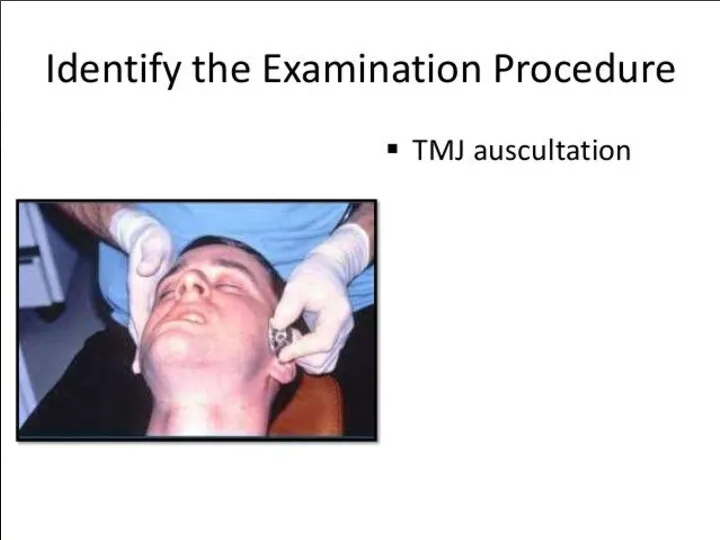
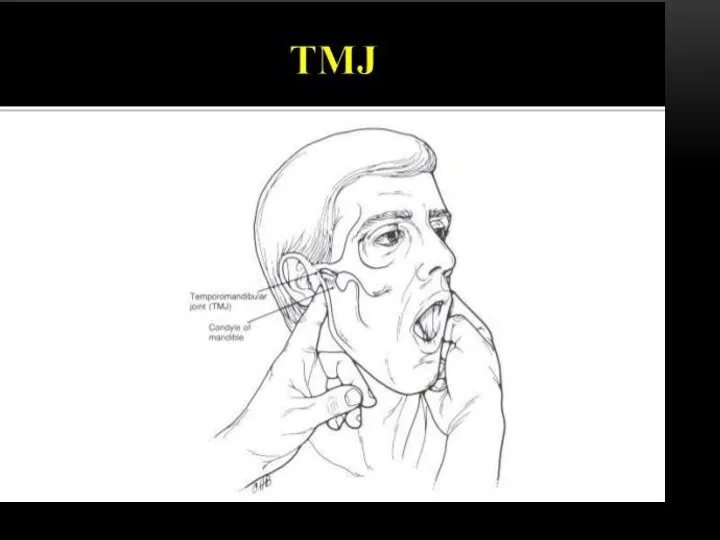
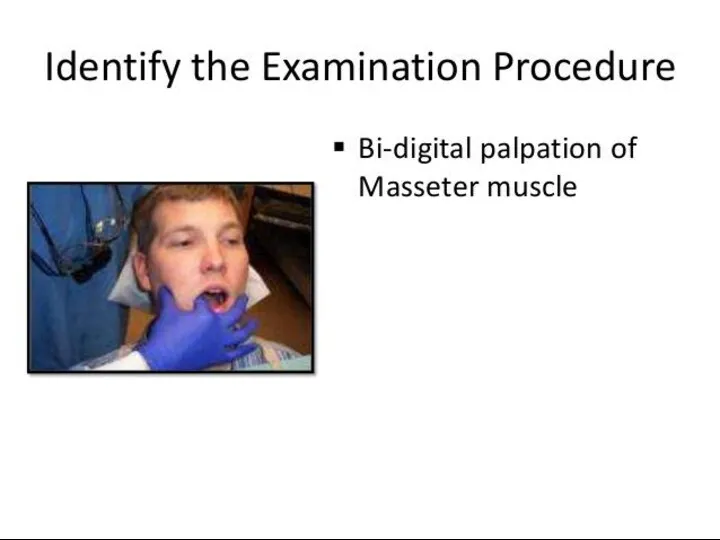
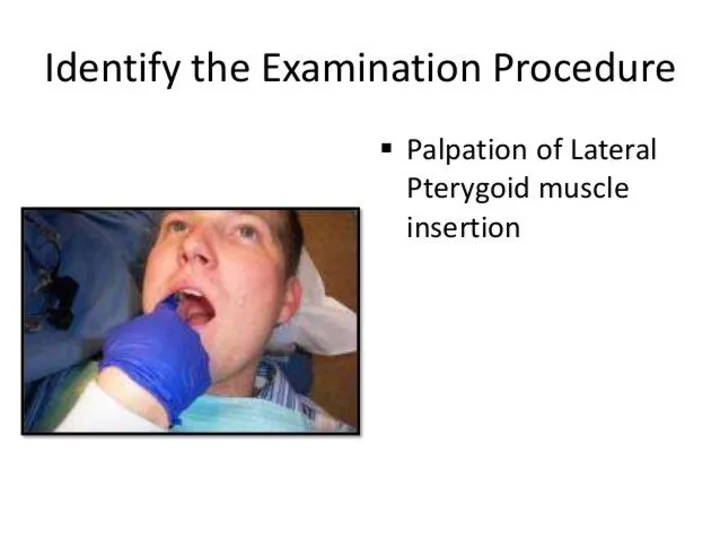
TMJ
Occlusion
Ms of mastication
Jiont
TMJ
Occlusion
Ms of mastication
Jiont
 Разбор клинического случая
Разбор клинического случая Хронический гастрит
Хронический гастрит Травматические повреждения костей и суставов
Травматические повреждения костей и суставов Принципы нормирования опасных и вредных факторов
Принципы нормирования опасных и вредных факторов Хирургиялык жане тану кабинеті
Хирургиялык жане тану кабинеті Основные проблемы гигиены детей и подростков
Основные проблемы гигиены детей и подростков Экспертиза временной нетрудоспособности терапевтических больных в поликлинике
Экспертиза временной нетрудоспособности терапевтических больных в поликлинике Иммобилизденген ферменттер
Иммобилизденген ферменттер Cестринский уход за новорождёнными при многоплодной беременности
Cестринский уход за новорождёнными при многоплодной беременности Dentists in Canada
Dentists in Canada Частная патологическая анатомия. Болезни ССС
Частная патологическая анатомия. Болезни ССС Adult Nursing Care I
Adult Nursing Care I Ветряная оспа
Ветряная оспа Острые лейкозы. Основные методы исследования при ОЛ
Острые лейкозы. Основные методы исследования при ОЛ Совершенствование системы оплаты труда в здравоохранении - как по-новому запланировать расходы
Совершенствование системы оплаты труда в здравоохранении - как по-новому запланировать расходы Есту және тепе-теңдік мүшесі
Есту және тепе-теңдік мүшесі Инфекциялық емес патологиядағы менингеальды синдром. Туберкулезді менингитпен екшеу диагностикасы
Инфекциялық емес патологиядағы менингеальды синдром. Туберкулезді менингитпен екшеу диагностикасы Балалардың асқазан - ішек аурулары туралы түсінік беру. Балаларда ішек жұқпасының көріністері
Балалардың асқазан - ішек аурулары туралы түсінік беру. Балаларда ішек жұқпасының көріністері Серонегативные спондилоартриты
Серонегативные спондилоартриты Актуальные вопросы профилактики, диагностики коронавирусной инфекции
Актуальные вопросы профилактики, диагностики коронавирусной инфекции Перитонеальный диализ
Перитонеальный диализ Сульфаниламидные препараты
Сульфаниламидные препараты OMS - Organizaţia Mondială a Sănătăţii
OMS - Organizaţia Mondială a Sănătăţii Гепатит С
Гепатит С Бактерия Helicobacter pylori
Бактерия Helicobacter pylori Острая печеночная недостаточность
Острая печеночная недостаточность Термические повреждения
Термические повреждения Жай және күрделі ұнтақтардың дайындалуы. Улы және күшті әсер ететін дәрілік заттары бар ұнтақтардың технологиясы. Тритурация
Жай және күрделі ұнтақтардың дайындалуы. Улы және күшті әсер ететін дәрілік заттары бар ұнтақтардың технологиясы. Тритурация