- Congestive Heart Failure

Содержание
- 2. Heart Failure: Epidemiology Burden of CHF is staggering 5 million in US (1.5% of all adults)
- 3. Definition HF is a clinical syndrome characterized by typical symptoms (e.g. breathlessness, ankle swelling and fatigue)
- 5. Etiologies of Chronic Heart Failure Men Women
- 6. Stages of Heart Failure NYHA Class Class I : Symptoms with more than ordinary activity Class
- 7. Types of HF
- 8. Systolic vs. Diastolic HF (HFrEF vs. HFpEF) Diastolic dysfunction EF normal or increased Hypertension Due to
- 9. Subtypes of Systolic Heart Failure Low cardiac output High output Severe anemia AV malformations Hyperthyroidism Left
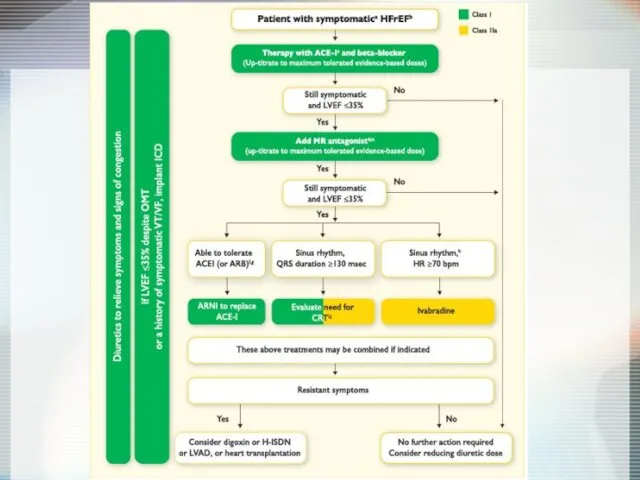
- 10. Principles of Treatment Systolic HF ↓ Preload ↓ Afterload ↑ Inotropism ↓ Neurohumoral activity ACE-I, β-blockers,
- 11. Management of Heart Failure Therapies ACE-Inhibitors Beta Blockers Aldactone Diuretics Digoxin Recent non-Pharmacological Advances Sudden death
- 12. Diagnosis of HF Anamnesis Chest X-Ray ECG Echocardiography Cardiac catheterization: coronary angiography and Rt heart catheterization
- 14. Aims of therapy Reduce symptoms & improve QOL Reduce hospitalization Reduce mortality Pump failure Sudden cardiac
- 15. Targets for treatment: Neurohormonal responses to impaired cardiac performance
- 16. Renin-Angiotensin Cascade & β-blockers Angiotensinogen Angiotensin II AT1 AT2 Aldosterone - + + Spironolactone - -
- 17. Purpose To determine whether long-term therapy with the ACE inhibitor captopril reduces morbidity and mortality in
- 18. Design Multicenter, randomized, double-blind, placebo-controlled Patients 2231 patients, aged 21–80 years, with left ventricular dysfunction (ejection
- 19. In patients with left ventricular dysfunction after MI, long-term captopril over a mean 3.5-year period: Significantly
- 20. 0 0 1 2 4 3 0.3 0.2 0.1 Mortality and recurrent MI Years after randomization
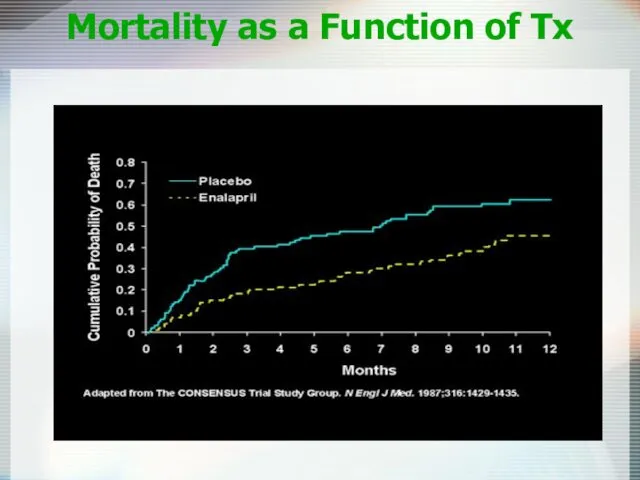
- 21. ACE-I: Use at Any Stage of CHF! SOLVD trial - Enalapril 20mg/day (41 mo) 2569 Patients
- 22. Mortality as a Function of Tx
- 23. Angiotensin-Receptor Blockers Comparable to ACE inhibitors Reduce all-cause mortality Suitable alternative for patient with adverse events
- 24. ACE + ARB CHARM trial 2548 NYHA II-IV; LVEF Decrease in CV death, hospital admission NNT=25
- 25. ACE Inhibitors Dosage - ATLAS Trial Results No difference in primary endpoint All-cause mortality (42.5% vs.
- 26. ACE-Inhibitors in CHF In patients with CHF total mortality and mortality combined with hospitalization from CHF
- 27. Entresto® - Sacubitril/Valsartan Drug Facts Pharmacology: Sacubitril – prodrug metabolized to active metabolite (LBQ657), which inhibits
- 28. Neprilysin Inhibition Potentiates Actions of Endogenous Vasoactive Peptides That Counter Maladaptive Mechanisms in Heart Failure Endogenous
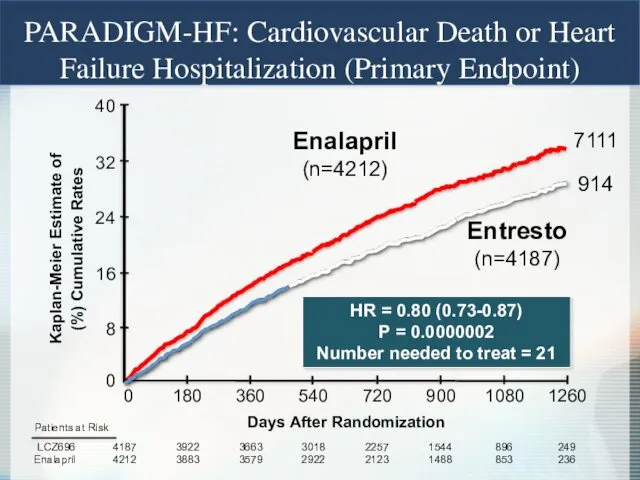
- 29. Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart
- 30. 0 16 32 40 24 8 Enalapril (n=4212) 360 720 1080 0 180 540 900 1260
- 31. Enalapril (n=4212) LCZ696 (n=4187) HR = 0.80 (0.71-0.89) P = 0.00004 Number need to treat =
- 32. PARADIGM-HF: Effect of LCZ696 vs Enalapril on Primary Endpoint and Its Components
- 33. Hydralazine (Apresoline) Plus Isosorbide Dinitrate (Sorbitrate) African-American Heart Failure Trial (A-HeFT) Hydralazine Reduces systemic vascular resistance
- 34. Beta-Blockers Decrease cardiac sympathetic activity 34% reduction in all mortality with use of β-blockers Use in
- 35. β-blocker - which to pick? Three beta-blockers : Bisoprolol (Zebeta) -Trial CIBIS-II trial Metoprolol (Toprol XL)
- 36. Initial and Target Doses of β-blockers for CHF
- 37. β-blockers in symptomatic Heat Failure: Meta-analysis Results 123 articles, 18 trials, 2986 patients 7 (n=562) of
- 38. β-blockers therapy for congestive heart failure: a systematic overwiew and critical appraisal of the published trails.
- 39. Digoxin May relieve symptoms, does not reduce mortality Pts taking digoxin are less likely to be
- 40. The Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart
- 41. Digoxin in symptomatic systolic dysfunction: RCT Design Patients 6800 patients with heart failure, LVEF Most patients
- 42. DIG : Reduces Hospitalization but not Mortality Benefit The Digitalis Investigation Group. The effect of digoxin
- 43. Digoxin in symptomatic systolic dysfunction: RCT Results No differences in deaths 1181 vs 1194 More patients
- 44. Ivabradin Specifically binds the Funny channel Reduces the slope for diastolic depolarization Prolongs diastolic duration Does
- 45. BEAUTIFUL Trial: Inclusion criteria Male or female Nondiabetic ≥55 years, diabetic ≥18 years Documented coronary artery
- 46. Effect of ivabradine on primary endpoint (Overall population) % with primary composite end point of CV
- 47. Ivabradine reduces fatal and nonfatal myocardial infarction (HR ≥70 bpm) Hospitalization for fatal or nonfatal MI
- 48. Ivabradine In patients with coronary artery disease and left ventricular dysfunction, those with a heart rate
- 49. Spironolactone in Severe Heart Failure: RCT Design Pitt B, Zannad F, Remme WJ, et al, for
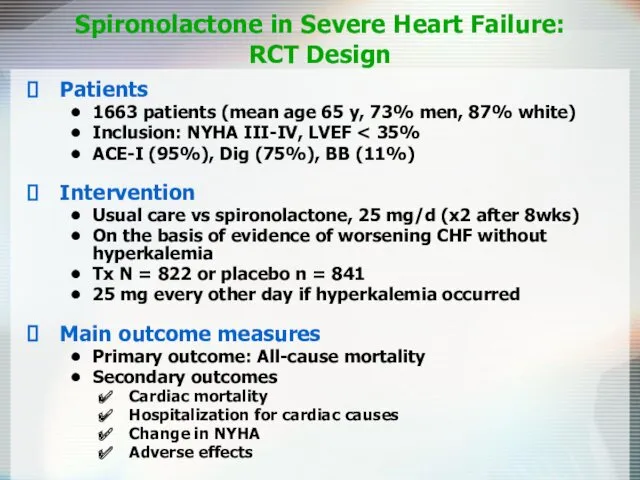
- 50. Spironolactone in Severe Heart Failure: RCT Design Patients 1663 patients (mean age 65 y, 73% men,
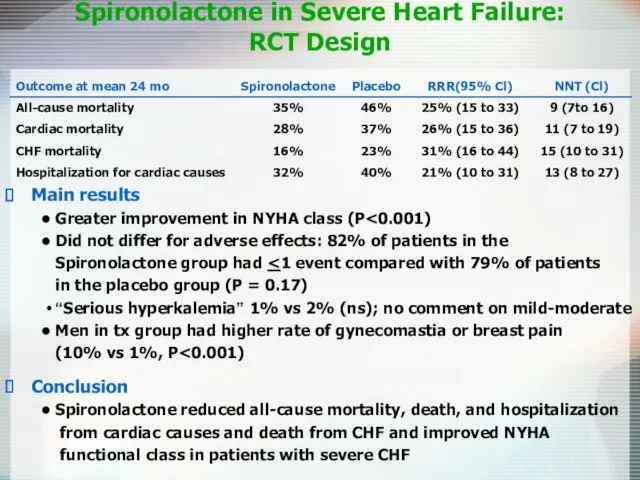
- 51. Spironolactone in Severe Heart Failure: RCT Design Main results Greater improvement in NYHA class (P Did
- 52. Eplerenone Post-AMI Heart Failure Efficacy and Survival Study EPHESUS Trial
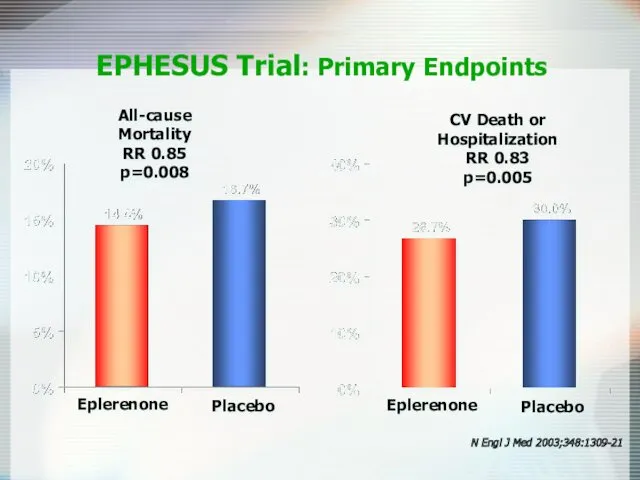
- 53. Eplerenone (n = 3,313) Placebo (n = 3,319) Endpoints (at mean of 16 month follow-up): Primary
- 54. All-cause Mortality RR 0.85 p=0.008 EPHESUS Trial: Primary Endpoints CV Death or Hospitalization RR 0.83 p=0.005
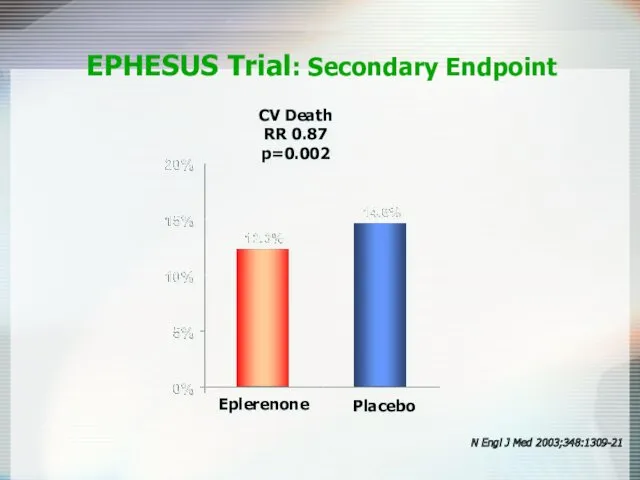
- 55. CV Death RR 0.87 p=0.002 EPHESUS Trial: Secondary Endpoint N Engl J Med 2003;348:1309-21 Eplerenone Placebo
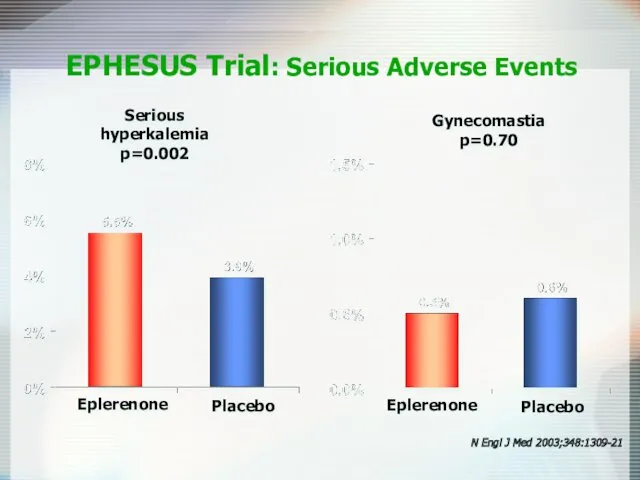
- 56. Serious hyperkalemia p=0.002 EPHESUS Trial: Serious Adverse Events Gynecomastia p=0.70 Eplerenone Placebo N Engl J Med
- 57. Loop Diuretics Mainstay of symptomatic treatment Improve fluid retention Increase exercise tolerance No effects on morbidity
- 58. Diuretics in Heart Failure Benefits Improve symptoms of congestion Can improve cardiac output Improved neurohormonal milieu
- 59. Antiplatelet Therapy and Anticoagulation Increased risk of thromboembolic events, 1.6-3.2% per year Antiplatelet therapy (aspirin) in
- 60. Nesiritide (Natrecor) Recombinant form of human BNP Causes venous and arterial vasodilation Has been shown to
- 61. Anti-Diabetic Drugs and Cardiovascular Outcomes UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998. The University Group
- 62. Cardiovascular Outcomes EMPA-REG Trial
- 63. Not recommended
- 64. Pharmacological Therapies for Heart Failure: Conclusions Symptomatic systolic dysfunction ACE-I: reduce mortality & hospitalization for heart
- 65. Device Therapy Implantable Cardioverter-Defibrillators (ICD) Cardiac Resynchronization Therapy (CRT) Left Ventricular Assist Devices (LVAD)
- 66. Rates of Sudden Cardiac Rate NYHA II NYHA III NYHA IV
- 67. ICD SCD-HeFT (sudden cardiac death) 2521 patients with depressed LV systolic function and Class II-III HF
- 68. MADIT-II: Eligibility Chronic CAD with prior MI EF No requirement for NSVT or EPS No upper
- 69. MADIT-II: Results
- 70. ICD Recommended in pts with EF Survival with good functional capacity is anticipated for > 1
- 71. Cardiac Resynchronization Therapy Patient Indications CRT device: Moderate to severe HF (NYHA Class III/IV) patients Symptomatic
- 72. CRT COMPANION trial 1520 patients, most with class III-IV HF, QRS duration >120 ms Randomized in
- 73. Conclusions ACE inhibitors improve symptoms in CCF (CONSENSUS) and reduce mortality even in asymptomatic patients with
- 74. Left Ventricular Assist Devices (LVAD) REMATCH trial- 1 yr survival 52% (LVAD) vs 24% (medical Rx)
- 75. Diastolic Dysfunction 20-40% of presenting CHF syndrome Risk of death lower than systolic dysfunction Dx: Doppler
- 76. Diastolic Dysfunction Acute Management is the SAME Chronic Management is CONTROVERSIAL Diuretics-dec fluid volume CCB-promote left
- 77. Heart Failure: More than just drugs Dietary counseling Patient education Physical activity Medication compliance Aggressive follow-up
- 80. Скачать презентацию
Heart Failure: Epidemiology
Burden of CHF is staggering
5 million in US (1.5%
Heart Failure: Epidemiology
Burden of CHF is staggering
5 million in US (1.5%
Definition
HF is a clinical syndrome characterized by typical symptoms (e.g. breathlessness,
Definition
HF is a clinical syndrome characterized by typical symptoms (e.g. breathlessness,
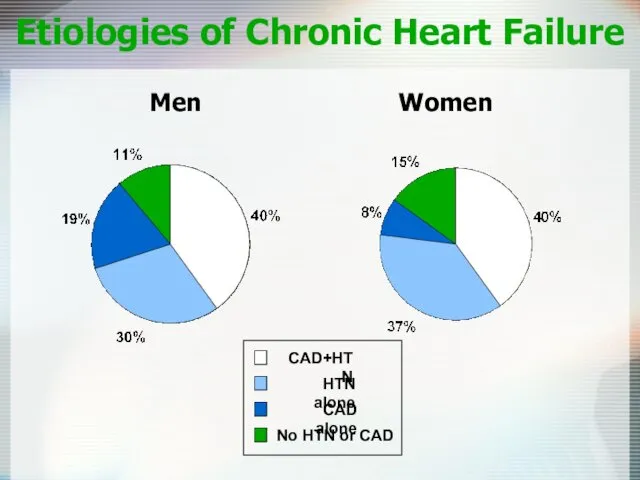
Etiologies of Chronic Heart Failure
Men Women
Etiologies of Chronic Heart Failure
Men Women
Stages of Heart Failure
NYHA Class
Class I : Symptoms with more than
Stages of Heart Failure
NYHA Class
Class I : Symptoms with more than
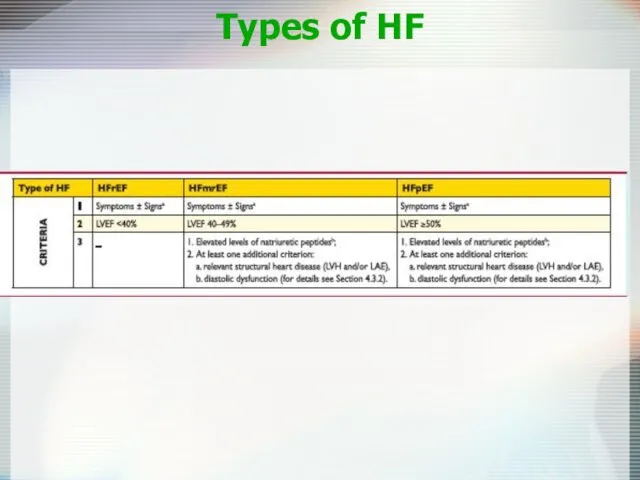
Types of HF
Types of HF
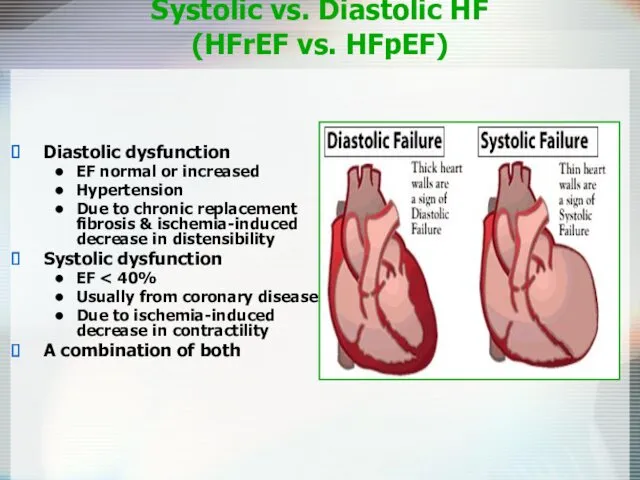
Systolic vs. Diastolic HF
(HFrEF vs. HFpEF)
Diastolic dysfunction
EF normal or increased
Hypertension
Due to
Systolic vs. Diastolic HF
(HFrEF vs. HFpEF)
Diastolic dysfunction
EF normal or increased
Hypertension
Due to
Subtypes of Systolic Heart Failure
Low cardiac output
High output
Severe anemia
AV malformations
Hyperthyroidism
Left
Subtypes of Systolic Heart Failure
Low cardiac output
High output
Severe anemia
AV malformations
Hyperthyroidism
Left
Principles of Treatment
Systolic HF
↓ Preload
↓ Afterload
↑ Inotropism
↓ Neurohumoral
activity
ACE-I, β-blockers,
Principles of Treatment
Systolic HF
↓ Preload
↓ Afterload
↑ Inotropism
↓ Neurohumoral
activity
ACE-I, β-blockers,
Management of Heart Failure
Therapies
ACE-Inhibitors
Beta Blockers
Aldactone
Diuretics
Digoxin
Recent non-Pharmacological Advances
Sudden death and ICD’s
Contractile dysynchrony
Management of Heart Failure
Therapies
ACE-Inhibitors
Beta Blockers
Aldactone
Diuretics
Digoxin
Recent non-Pharmacological Advances
Sudden death and ICD’s
Contractile dysynchrony
Diagnosis of HF
Anamnesis
Chest X-Ray
ECG
Echocardiography
Cardiac catheterization: coronary angiography and Rt heart catheterization
CMR
Myocardial
Diagnosis of HF
Anamnesis
Chest X-Ray
ECG
Echocardiography
Cardiac catheterization: coronary angiography and Rt heart catheterization
CMR
Myocardial
Aims of therapy
Reduce symptoms & improve QOL
Reduce hospitalization
Reduce mortality
Pump failure
Sudden cardiac
Aims of therapy
Reduce symptoms & improve QOL
Reduce hospitalization
Reduce mortality
Pump failure
Sudden cardiac
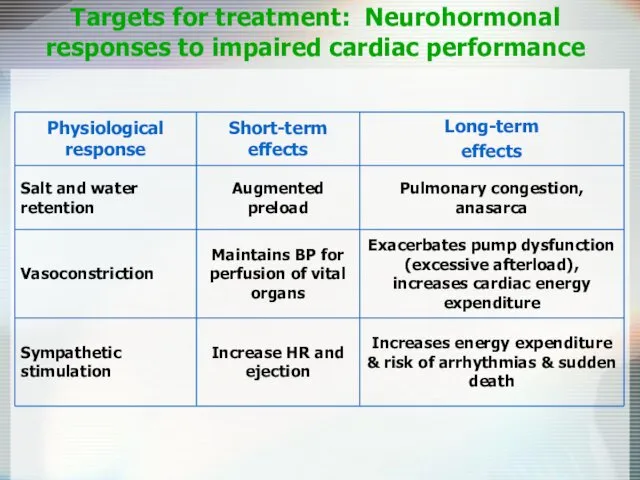
Targets for treatment: Neurohormonal responses to impaired cardiac performance
Targets for treatment: Neurohormonal responses to impaired cardiac performance
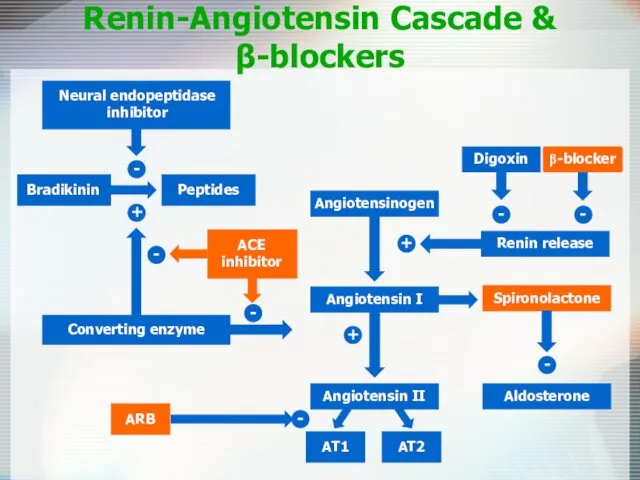
Renin-Angiotensin Cascade &
β-blockers
Angiotensinogen
Angiotensin II
AT1
AT2
Aldosterone
-
+
+
Spironolactone
-
-
-
Renin-Angiotensin Cascade &
β-blockers
Angiotensinogen
Angiotensin II
AT1
AT2
Aldosterone
-
+
+
Spironolactone
-
-
-
Purpose
To determine whether long-term therapy with the ACE inhibitor captopril reduces
Purpose
To determine whether long-term therapy with the ACE inhibitor captopril reduces
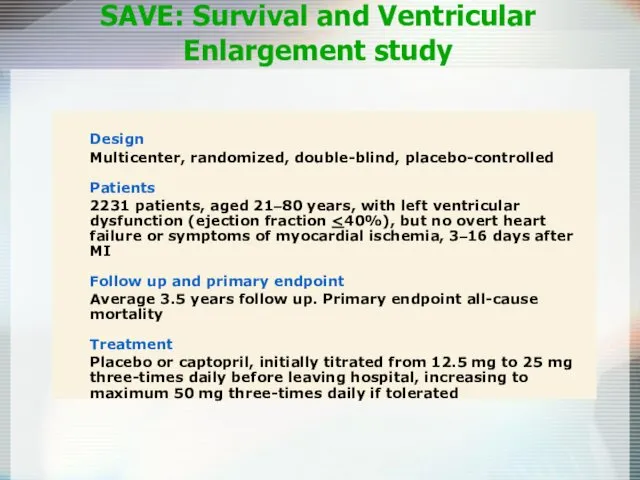
Design
Multicenter, randomized, double-blind, placebo-controlled
Patients
2231 patients, aged 21–80 years, with left ventricular
Design
Multicenter, randomized, double-blind, placebo-controlled
Patients
2231 patients, aged 21–80 years, with left ventricular
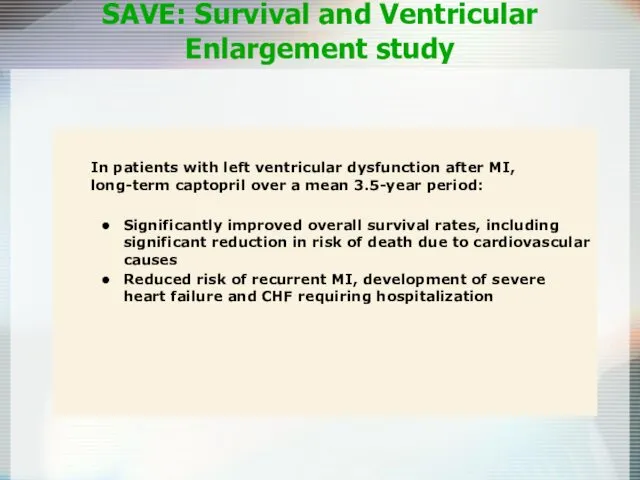
In patients with left ventricular dysfunction after MI, long-term captopril over
In patients with left ventricular dysfunction after MI, long-term captopril over
0
0
1
2
4
3
0.3
0.2
0.1
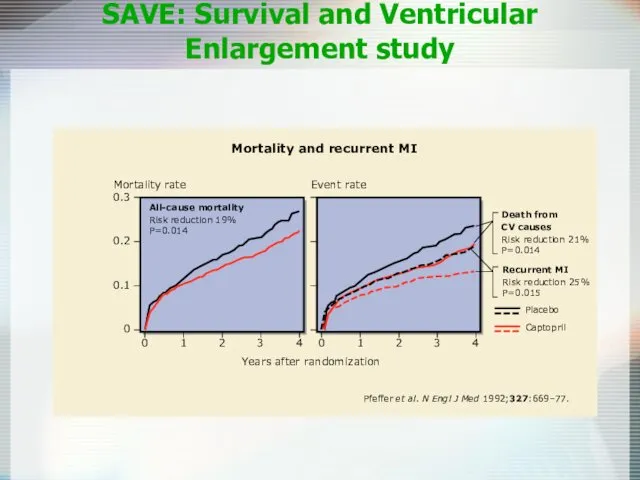
Mortality and recurrent MI
Years after randomization
All-cause mortality
Risk reduction 19%
P=0.014
Death from
CV causes
Risk
0
0
1
2
4
3
0.3
0.2
0.1
Mortality and recurrent MI
Years after randomization
All-cause mortality
Risk reduction 19%
P=0.014
Death from
CV causes
Risk
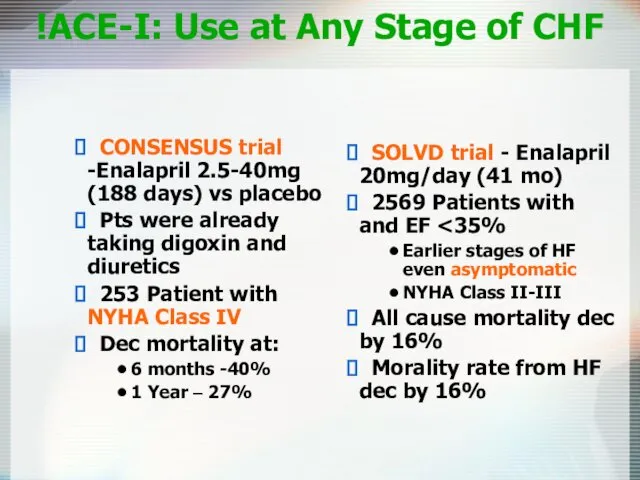
ACE-I: Use at Any Stage of CHF!
SOLVD trial - Enalapril
ACE-I: Use at Any Stage of CHF!
SOLVD trial - Enalapril
Mortality as a Function of Tx
Mortality as a Function of Tx
Angiotensin-Receptor Blockers
Comparable to ACE inhibitors
Reduce all-cause mortality
Suitable alternative for patient with
Angiotensin-Receptor Blockers
Comparable to ACE inhibitors
Reduce all-cause mortality
Suitable alternative for patient with
ACE + ARB
CHARM trial
2548 NYHA II-IV; LVEF < 40%
Decrease in
ACE + ARB
CHARM trial
2548 NYHA II-IV; LVEF < 40%
Decrease in
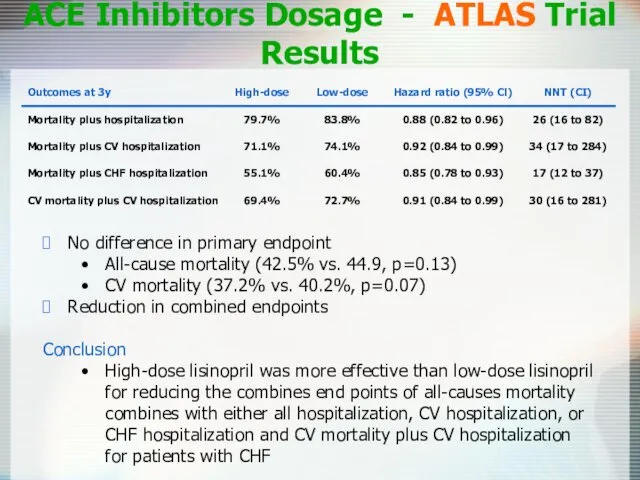
ACE Inhibitors Dosage - ATLAS Trial Results
No difference in primary endpoint
All-cause
ACE Inhibitors Dosage - ATLAS Trial Results
No difference in primary endpoint
All-cause
ACE-Inhibitors in CHF
In patients with CHF total mortality and mortality combined
ACE-Inhibitors in CHF
In patients with CHF total mortality and mortality combined
Entresto® - Sacubitril/Valsartan
Drug Facts
Pharmacology:
Sacubitril – prodrug metabolized to active metabolite
Entresto® - Sacubitril/Valsartan
Drug Facts
Pharmacology:
Sacubitril – prodrug metabolized to active metabolite
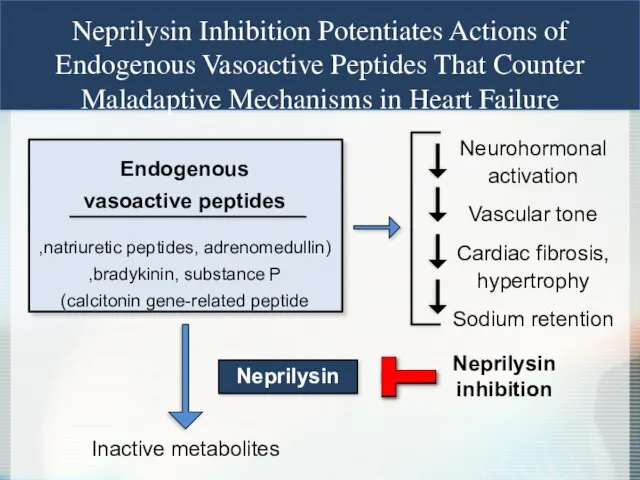
Neprilysin Inhibition Potentiates Actions of
Endogenous Vasoactive Peptides That Counter
Maladaptive Mechanisms
Neprilysin Inhibition Potentiates Actions of
Endogenous Vasoactive Peptides That Counter
Maladaptive Mechanisms
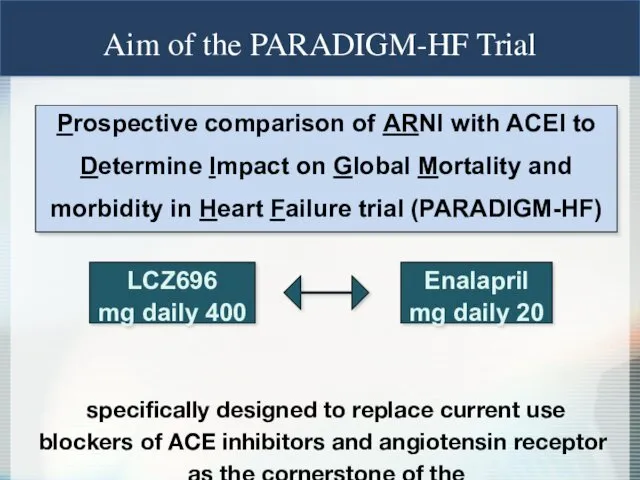
Prospective comparison of ARNI with ACEI to Determine Impact on Global
Prospective comparison of ARNI with ACEI to Determine Impact on Global
0
16
32
40
24
8
Enalapril
(n=4212)
360
720
1080
0
180
540
900
1260
Days After Randomization
4187
4212
3922
3883
3663
3579
3018
2922
2257
2123
1544
1488
896
853
249
236
LCZ696
Enalapril
Patients at Risk
1117
Kaplan-Meier Estimate of
Cumulative Rates (%)
914
Entresto
(n=4187)
HR = 0.80
0
16
32
40
24
8
Enalapril
(n=4212)
360
720
1080
0
180
540
900
1260
Days After Randomization
4187
4212
3922
3883
3663
3579
3018
2922
2257
2123
1544
1488
896
853
249
236
LCZ696
Enalapril
Patients at Risk
1117
Kaplan-Meier Estimate of
Cumulative Rates (%)
914
Entresto
(n=4187)
HR = 0.80
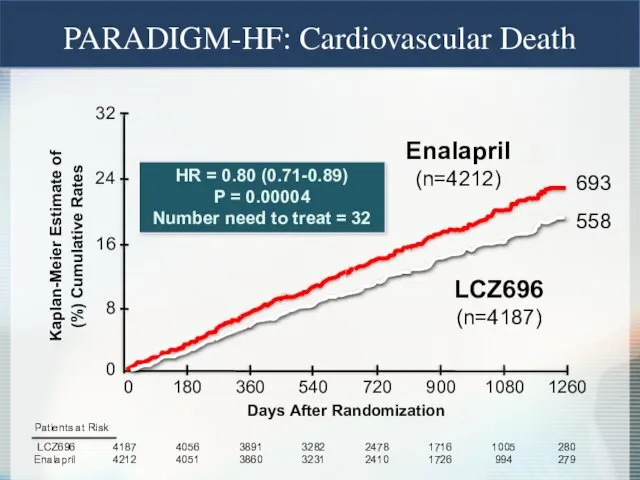
Enalapril
(n=4212)
LCZ696
(n=4187)
HR = 0.80 (0.71-0.89)
P = 0.00004
Number need to treat = 32
Kaplan-Meier
Enalapril
(n=4212)
LCZ696
(n=4187)
HR = 0.80 (0.71-0.89)
P = 0.00004
Number need to treat = 32
Kaplan-Meier
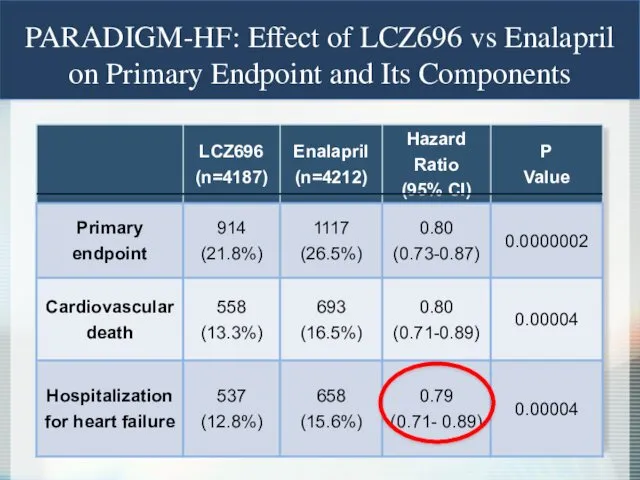
PARADIGM-HF: Effect of LCZ696 vs Enalapril on Primary Endpoint and Its
PARADIGM-HF: Effect of LCZ696 vs Enalapril on Primary Endpoint and Its
Hydralazine (Apresoline) Plus Isosorbide Dinitrate (Sorbitrate)
African-American Heart Failure Trial (A-HeFT)
Hydralazine
Reduces
Hydralazine (Apresoline) Plus Isosorbide Dinitrate (Sorbitrate)
African-American Heart Failure Trial (A-HeFT)
Hydralazine
Reduces
Beta-Blockers
Decrease cardiac sympathetic activity
34% reduction in all mortality with use
Beta-Blockers
Decrease cardiac sympathetic activity
34% reduction in all mortality with use
β-blocker - which to pick?
Three beta-blockers :
Bisoprolol (Zebeta) -Trial CIBIS-II
β-blocker - which to pick?
Three beta-blockers :
Bisoprolol (Zebeta) -Trial CIBIS-II
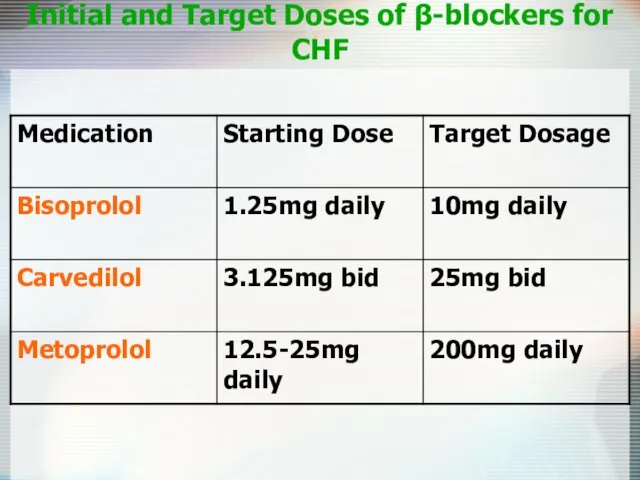
Initial and Target Doses of β-blockers for CHF
Initial and Target Doses of β-blockers for CHF
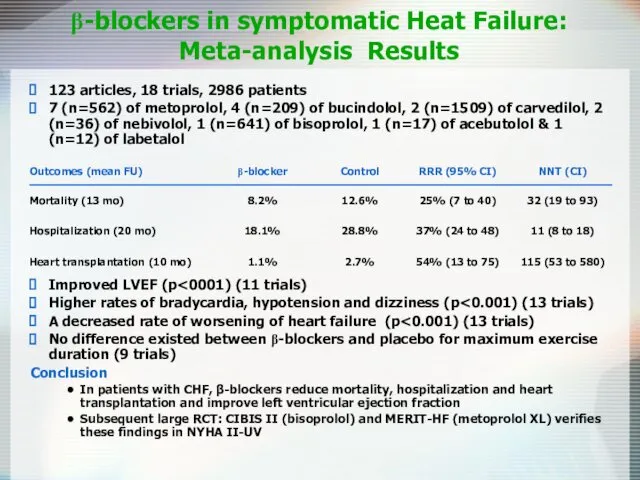
β-blockers in symptomatic Heat Failure:
Meta-analysis Results
123 articles, 18 trials, 2986
β-blockers in symptomatic Heat Failure:
Meta-analysis Results
123 articles, 18 trials, 2986
β-blockers therapy for congestive heart failure: a systematic overwiew and critical
β-blockers therapy for congestive heart failure: a systematic overwiew and critical
Digoxin
May relieve symptoms, does not reduce mortality
Pts taking digoxin are less
Digoxin
May relieve symptoms, does not reduce mortality
Pts taking digoxin are less
The Digitalis Investigation Group. The effect of digoxin on mortality and
The Digitalis Investigation Group. The effect of digoxin on mortality and
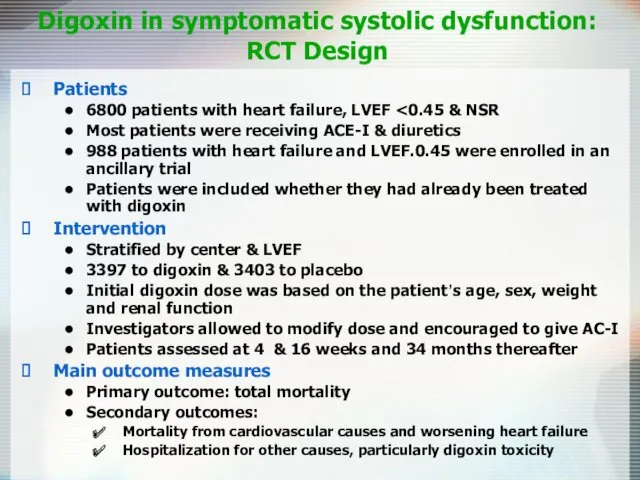
Digoxin in symptomatic systolic dysfunction:
RCT Design
Patients
6800 patients with heart failure,
Digoxin in symptomatic systolic dysfunction:
RCT Design
Patients
6800 patients with heart failure,
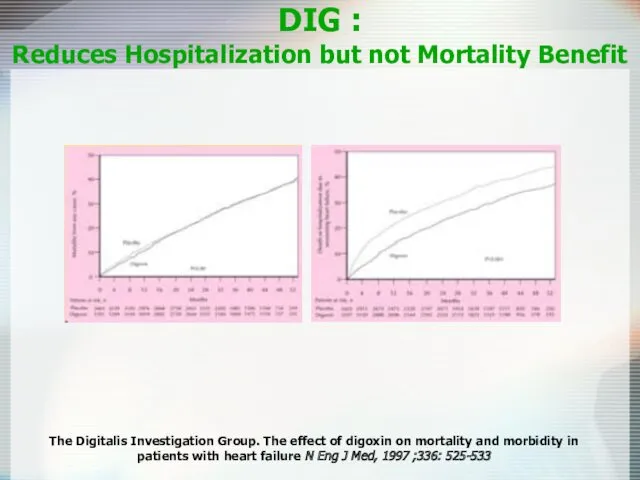
DIG :
Reduces Hospitalization but not Mortality Benefit
The Digitalis Investigation Group.
DIG :
Reduces Hospitalization but not Mortality Benefit
The Digitalis Investigation Group.
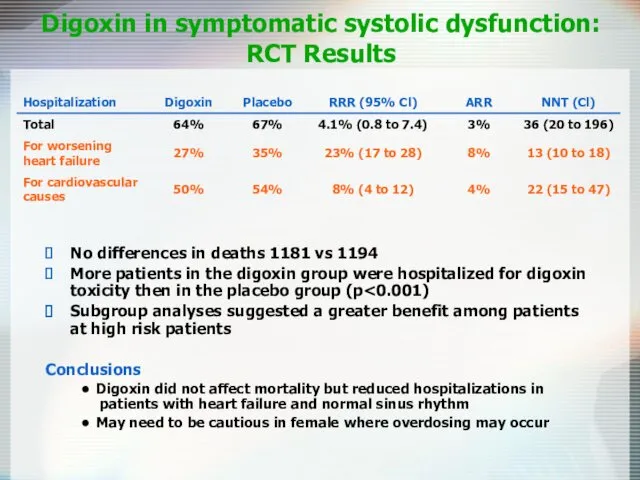
Digoxin in symptomatic systolic dysfunction: RCT Results
No differences in deaths 1181
Digoxin in symptomatic systolic dysfunction: RCT Results
No differences in deaths 1181
Ivabradin
Specifically binds the Funny channel
Reduces the slope for diastolic depolarization
Prolongs
Ivabradin
Specifically binds the Funny channel
Reduces the slope for diastolic depolarization
Prolongs
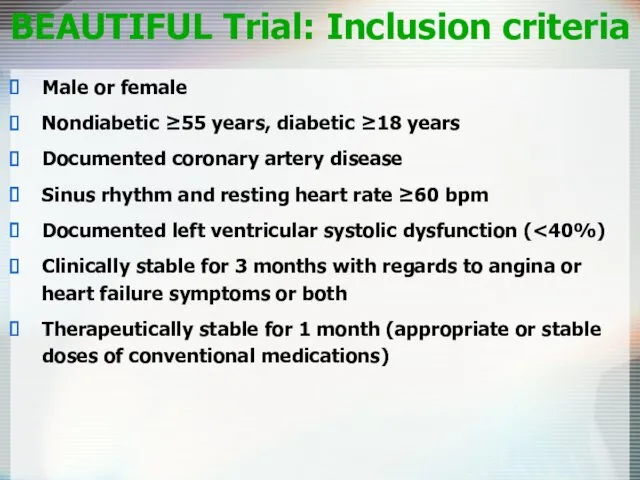
BEAUTIFUL Trial: Inclusion criteria
Male or female
Nondiabetic ≥55 years, diabetic ≥18 years
Documented
BEAUTIFUL Trial: Inclusion criteria
Male or female
Nondiabetic ≥55 years, diabetic ≥18 years
Documented
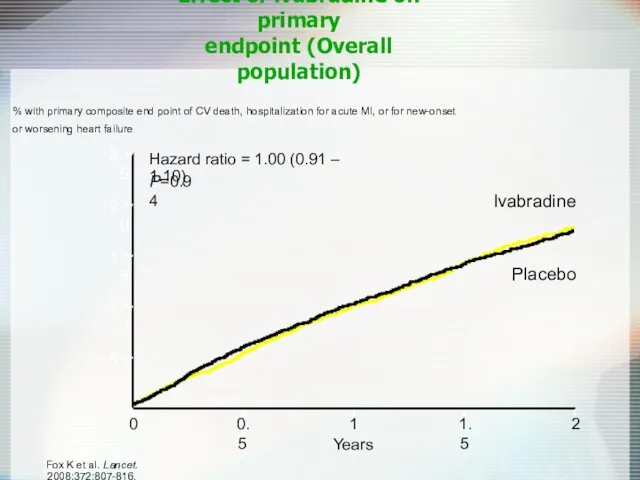
Effect of ivabradine on primary
endpoint (Overall population)
% with primary composite end
Effect of ivabradine on primary
endpoint (Overall population)
% with primary composite end
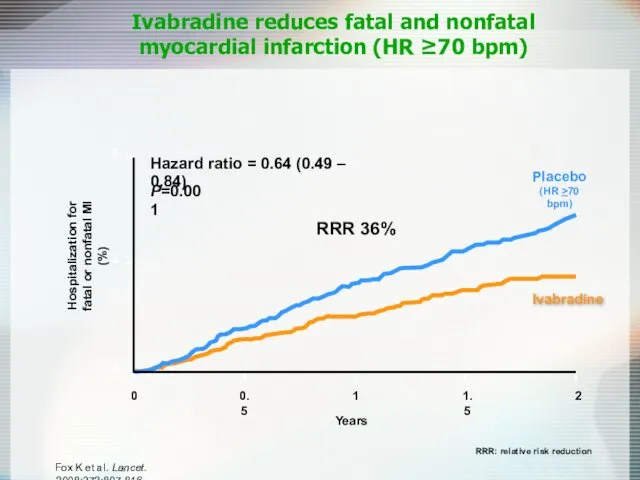
Ivabradine reduces fatal and nonfatal
myocardial infarction (HR ≥70 bpm)
Hospitalization for
Ivabradine reduces fatal and nonfatal
myocardial infarction (HR ≥70 bpm)
Hospitalization for
Ivabradine
In patients with coronary artery disease and left ventricular dysfunction, those
Ivabradine
In patients with coronary artery disease and left ventricular dysfunction, those
Spironolactone in Severe Heart Failure: RCT Design
Pitt B, Zannad F, Remme
Spironolactone in Severe Heart Failure: RCT Design
Pitt B, Zannad F, Remme
Spironolactone in Severe Heart Failure:
RCT Design
Patients
1663 patients (mean
Spironolactone in Severe Heart Failure:
RCT Design
Patients
1663 patients (mean
Spironolactone in Severe Heart Failure:
RCT Design
Main results
Greater improvement
Spironolactone in Severe Heart Failure:
RCT Design
Main results
Greater improvement
Eplerenone Post-AMI Heart Failure Efficacy and Survival Study
EPHESUS Trial
Eplerenone Post-AMI Heart Failure Efficacy and Survival Study
EPHESUS Trial
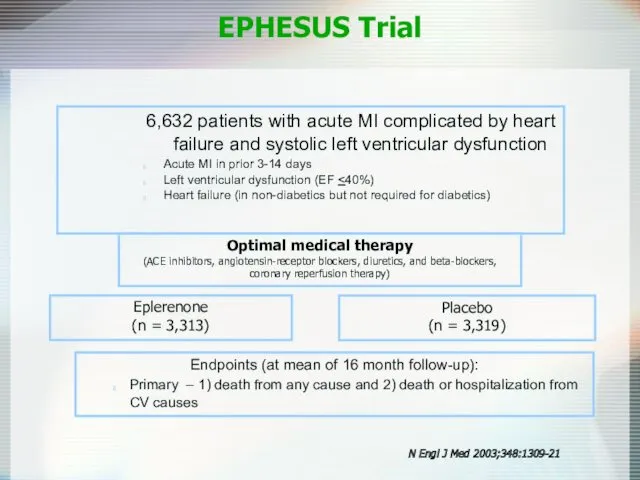
Eplerenone
(n = 3,313)
Placebo
(n = 3,319)
Endpoints (at mean of 16 month
Eplerenone
(n = 3,313)
Placebo
(n = 3,319)
Endpoints (at mean of 16 month
All-cause Mortality
RR 0.85
p=0.008
EPHESUS Trial: Primary Endpoints
CV Death or Hospitalization
RR 0.83
p=0.005
Eplerenone
Placebo
N Engl
All-cause Mortality
RR 0.85
p=0.008
EPHESUS Trial: Primary Endpoints
CV Death or Hospitalization
RR 0.83
p=0.005
Eplerenone
Placebo
N Engl
CV Death
RR 0.87
p=0.002
EPHESUS Trial: Secondary Endpoint
N Engl J Med 2003;348:1309-21
Eplerenone
Placebo
CV Death
RR 0.87
p=0.002
EPHESUS Trial: Secondary Endpoint
N Engl J Med 2003;348:1309-21
Eplerenone
Placebo
Serious hyperkalemia
p=0.002
EPHESUS Trial: Serious Adverse Events
Gynecomastia
p=0.70
Eplerenone
Placebo
N Engl J Med 2003;348:1309-21
Eplerenone
Placebo
Serious hyperkalemia
p=0.002
EPHESUS Trial: Serious Adverse Events
Gynecomastia
p=0.70
Eplerenone
Placebo
N Engl J Med 2003;348:1309-21
Eplerenone
Placebo
Loop Diuretics
Mainstay of symptomatic treatment
Improve fluid retention
Increase exercise tolerance
No effects on
Loop Diuretics
Mainstay of symptomatic treatment
Improve fluid retention
Increase exercise tolerance
No effects on
Diuretics in Heart Failure
Benefits
Improve symptoms
of congestion
Can improve cardiac output
Improved neurohormonal
Diuretics in Heart Failure
Benefits
Improve symptoms
of congestion
Can improve cardiac output
Improved neurohormonal
Antiplatelet Therapy and Anticoagulation
Increased risk of thromboembolic events, 1.6-3.2% per year
Antiplatelet
Antiplatelet Therapy and Anticoagulation
Increased risk of thromboembolic events, 1.6-3.2% per year
Antiplatelet
Nesiritide (Natrecor)
Recombinant form of human BNP
Causes venous and arterial
Nesiritide (Natrecor)
Recombinant form of human BNP
Causes venous and arterial
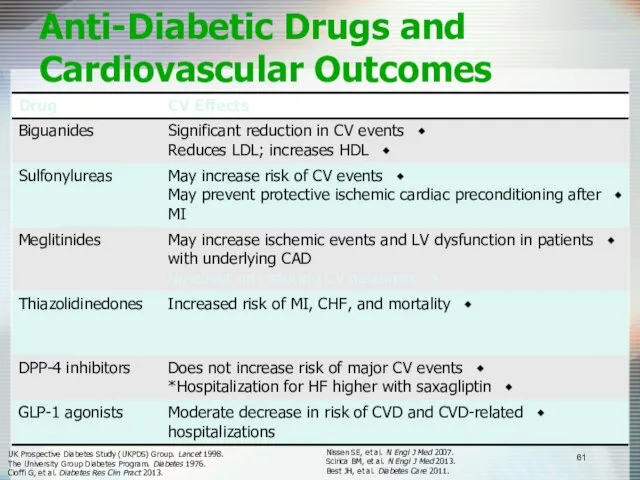
Anti-Diabetic Drugs and Cardiovascular Outcomes
UK Prospective Diabetes Study (UKPDS) Group. Lancet
Anti-Diabetic Drugs and Cardiovascular Outcomes
UK Prospective Diabetes Study (UKPDS) Group. Lancet
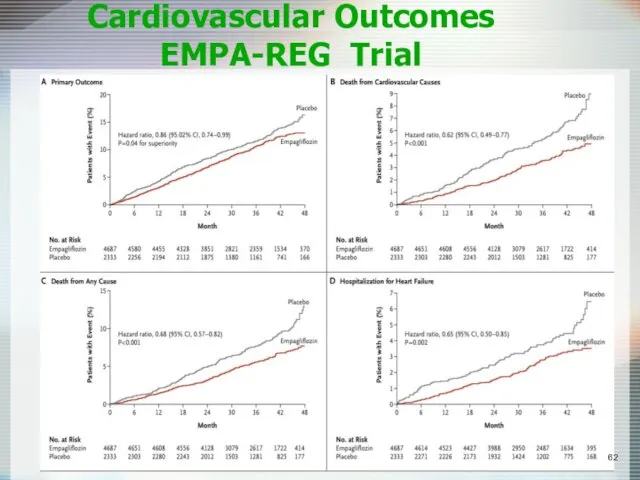
Cardiovascular Outcomes EMPA-REG Trial
Cardiovascular Outcomes EMPA-REG Trial
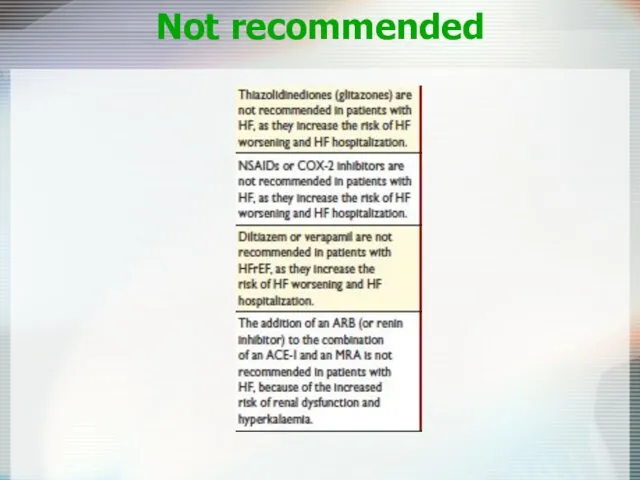
Not recommended
Not recommended
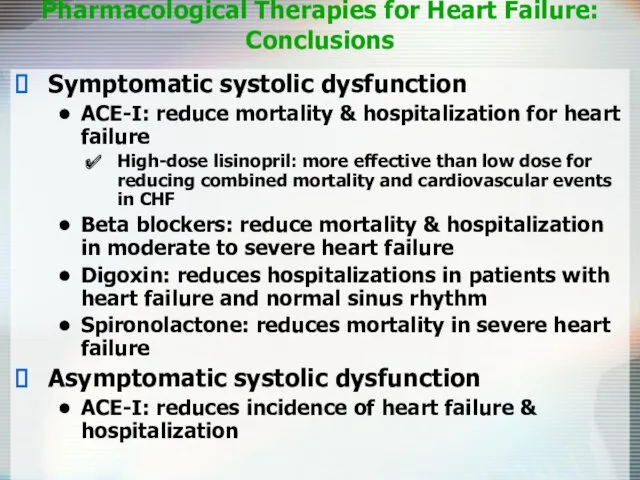
Pharmacological Therapies for Heart Failure:
Conclusions
Symptomatic systolic dysfunction
ACE-I: reduce
Pharmacological Therapies for Heart Failure:
Conclusions
Symptomatic systolic dysfunction
ACE-I: reduce
Device Therapy
Implantable Cardioverter-Defibrillators (ICD)
Cardiac Resynchronization Therapy (CRT)
Left Ventricular Assist Devices (LVAD)
Device Therapy
Implantable Cardioverter-Defibrillators (ICD)
Cardiac Resynchronization Therapy (CRT)
Left Ventricular Assist Devices (LVAD)
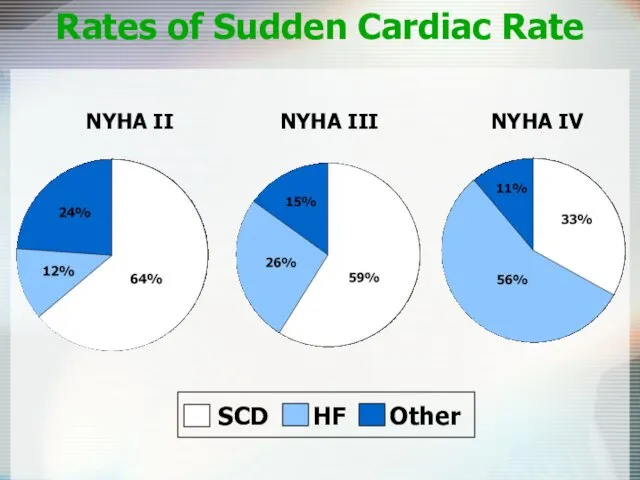
Rates of Sudden Cardiac Rate
NYHA II NYHA III NYHA IV
Rates of Sudden Cardiac Rate
NYHA II NYHA III NYHA IV
ICD
SCD-HeFT (sudden cardiac death)
2521 patients with depressed LV systolic function and
ICD
SCD-HeFT (sudden cardiac death)
2521 patients with depressed LV systolic function and
MADIT-II: Eligibility
Chronic CAD with prior MI
EF<0.30
No requirement for NSVT
MADIT-II: Eligibility
Chronic CAD with prior MI
EF<0.30
No requirement for NSVT
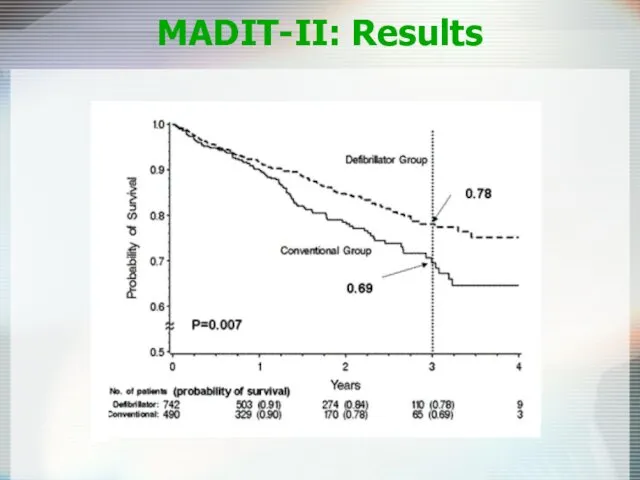
MADIT-II: Results
MADIT-II: Results
ICD
Recommended in pts with EF<30% and mild to moderate symptoms of
ICD
Recommended in pts with EF<30% and mild to moderate symptoms of
Cardiac Resynchronization Therapy
Patient Indications
CRT device:
Moderate to severe HF (NYHA
Cardiac Resynchronization Therapy
Patient Indications
CRT device:
Moderate to severe HF (NYHA
CRT
COMPANION trial
1520 patients, most with class III-IV HF,
QRS duration
CRT
COMPANION trial
1520 patients, most with class III-IV HF,
QRS duration
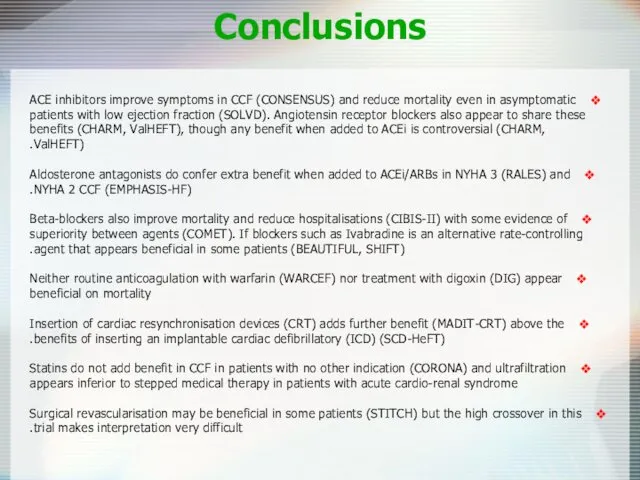
Conclusions
ACE inhibitors improve symptoms in CCF (CONSENSUS) and reduce mortality even
Conclusions
ACE inhibitors improve symptoms in CCF (CONSENSUS) and reduce mortality even
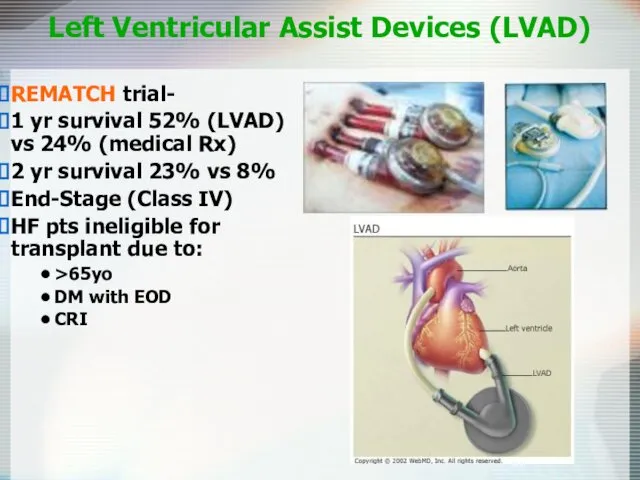
Left Ventricular Assist Devices (LVAD)
REMATCH trial-
1 yr survival 52% (LVAD) vs
Left Ventricular Assist Devices (LVAD)
REMATCH trial-
1 yr survival 52% (LVAD) vs
Diastolic Dysfunction
20-40% of presenting CHF syndrome
Risk of death lower than
Diastolic Dysfunction
20-40% of presenting CHF syndrome
Risk of death lower than
Diastolic Dysfunction
Acute Management is the SAME
Chronic Management is CONTROVERSIAL
Diuretics-dec fluid volume
CCB-promote
Diastolic Dysfunction
Acute Management is the SAME
Chronic Management is CONTROVERSIAL
Diuretics-dec fluid volume
CCB-promote
Heart Failure: More than just drugs
Dietary counseling
Patient education
Physical activity
Heart Failure: More than just drugs
Dietary counseling
Patient education
Physical activity
 Компоненты и основные этапы общей анестезии. Классификация видов обезболивания
Компоненты и основные этапы общей анестезии. Классификация видов обезболивания Хирургическая рана. Процесс заживления раны и его нарушения
Хирургическая рана. Процесс заживления раны и его нарушения Жоғарғы тыныс жолдарының аурулары. Ринит. Трахеит. Ларингит
Жоғарғы тыныс жолдарының аурулары. Ринит. Трахеит. Ларингит Заболевания желудка и двенадцатиперсной кишки. Лекция №3
Заболевания желудка и двенадцатиперсной кишки. Лекция №3 Колоректальный рак
Колоректальный рак Наркотики и беременность
Наркотики и беременность Көктамырға егу жасау техникасы жəне қан алу
Көктамырға егу жасау техникасы жəне қан алу Анестезиология и реаниматология. Введение в дисциплину
Анестезиология и реаниматология. Введение в дисциплину Терморегуляция организма. Закаливание
Терморегуляция организма. Закаливание Психотропные средства. Нейролептики. Транквилизакторы. Седативные средства
Психотропные средства. Нейролептики. Транквилизакторы. Седативные средства Папулосквамозні та бульозні дерматози
Папулосквамозні та бульозні дерматози Атопический дерматит
Атопический дерматит Гормоны
Гормоны Синдром эмоционального выгорания. Распространенность синдрома
Синдром эмоционального выгорания. Распространенность синдрома Травматизм. Виды травматизма. Травматический токсикоз. Травмы головы, груди, живота
Травматизм. Виды травматизма. Травматический токсикоз. Травмы головы, груди, живота Функциональные пробы и тесты, применяемые для оценки функционального состояния организма
Функциональные пробы и тесты, применяемые для оценки функционального состояния организма Основы эпидемиологии, инфекционные заболевания
Основы эпидемиологии, инфекционные заболевания Бактериальный вагиноз при беременности
Бактериальный вагиноз при беременности Ас қорыту жүйесі. Сүт тістерінің құрылыс ерекшелігі. Тіс алмасу
Ас қорыту жүйесі. Сүт тістерінің құрылыс ерекшелігі. Тіс алмасу Балалардағы хейлиттер
Балалардағы хейлиттер Миома матки
Миома матки Предмет и задачи патофизиологии
Предмет и задачи патофизиологии Процессы адаптации и компенсации. Регенерация и репарация. Склероз
Процессы адаптации и компенсации. Регенерация и репарация. Склероз Хроническая обструктивная болезнь легких
Хроническая обструктивная болезнь легких Одонтогенные флегмоны челюстно-лицевой области
Одонтогенные флегмоны челюстно-лицевой области Основные законы гемодинамики и их математическое выражение
Основные законы гемодинамики и их математическое выражение Weight Loss Challenge. Бросьте вызов лишнему весу. Углеводы, сахар и гликемический индекс
Weight Loss Challenge. Бросьте вызов лишнему весу. Углеводы, сахар и гликемический индекс Рак мочевого пузыря
Рак мочевого пузыря