- Drugs used in endocrine disorders

Содержание
- 3. Mechanism of action Once hormones reach a responsive cell, they bind with receptors in the cell
- 4. Second Messenger Systems Cyclic AMP is the 2nd messenger for many hormones, including Corticotropin, Glucagon, Thyroid
- 5. Ca2+ is the 2nd messenger for Gonadotropin-releasing hormone. This hormone binds to receptors to increase intracellular
- 6. Some hormones activate cell membrane receptors and transform them into phospholipase C, an enzyme that causes
- 7. Steroid Regulation of Protein Synthesis Steroid hormones are lipid soluble and cross cell membranes easily. Once
- 13. Thyroid Hormones: Thyroxine (Tetraiodothyronine,T4 -contains 4 atoms of iodine) Triiodothyronine (T3 - contains 3 atoms of
- 14. Antithyroid drugs: are used to lower the functional capacity of the hyperactive thyroid gland and have
- 15. INSULIN PREPARATIONS A. Rapid Acting Insulin - max effect per 1-4 hours short duration of action
- 16. C. Prolonged acting insulin: ∙ Ultralente Insulin max effect per 12-18 hours prolong duration of action
- 17. MECHANISM OF ACTION of INSULIN Insulin binds to receptor on the surface of its target cells.
- 20. Insulin is a fuel-storage hormone and affects cell growth and differentiation. Insulin ↓Blood Glucose by: ?Glucose
- 21. Actrapid (vial 10 ml : 40 and 100 IU/ml for SC or IV) - is a
- 22. Insulin Pens
- 24. Insulin Inhaling Device (Exubera)
- 25. CLINICAL USES of INSULIN: ⮚ Type 1 Diabetes: ■ Diabetic Ketoacidosis ■ Short-term treatment of patients
- 26. Oral (Synthetic) Hypoglycemic Agents: I. Stimulators of insulin release by beta cells: 1. Sulfonylurea derivatives: I.
- 27. Repaglinide and Nateglinide are non-sulfonylureas meglitinides that lower blood sugar by stimulating pancreatic secretion of insulin.
- 28. II. Inhibitors of hepatic gluconeogenesis: Biguanids: Metformin (Tab 0.5 g) Buformin Stimulate Anaerobic Glycolysis in peripheral
- 29. III. Alfa-glucosidase inhibitor Acarbose (Glucobay) inhibits alpha-glucosidases in the brush border of the small intestines and
- 30. Classification of Glucocorticoids: 1. Short-acting: Hydrocortisone acetate, Cortisone 2. Intermediate-acting: Prednisolone , Triamcinolone 3. Long-acting: Betametasone,
- 31. Action on mediators of inflammatory and immune response: GCs change Gene Expression: ? Production of prostanoids
- 32. Clinical uses of Glucocorticoids: 1. Replacement therapy for patients with adrenal failure - Addison’s disease 2.
- 33. Adverse effects: Cushing’s syndrome: Moon face, with red cheeks Thin arms and legs: muscle wasting ?BP,
- 35. OESTROGENS Natural: Estradiol - amp 0.1%-1 ml Estriol - Tab 1 mg Synthetic: Ethinylestradiol - Tab
- 36. CLINICAL USEs of OESTROGENS: Replacement therapy: - Primary Ovarian Failure (e.g., Turner’s syndrome) - Secondary Ovarian
- 37. ANTIOESTROGENS Clomiphene - Tab. 50 mg Tamoxifen - Tab. 20 mg Clomiphene: Interfering with the Negative
- 38. PROGESTOGENS 1. The naturally occurring hormone and its derivatives: Progesteron amp. 1% - 1 ml of
- 39. CLINICAL USE of PROGESTOGENS 1. CONTRACEPTION: - combined oral contraceptive pill - as progesterone-only contraceptive pill
- 43. Скачать презентацию

Mechanism of action
Once hormones reach a responsive cell, they bind with
Mechanism of action
Once hormones reach a responsive cell, they bind with
Second Messenger Systems
Cyclic AMP is the 2nd messenger for many hormones,
Second Messenger Systems
Cyclic AMP is the 2nd messenger for many hormones,
Ca2+ is the 2nd messenger for Gonadotropin-releasing hormone. This hormone binds
Ca2+ is the 2nd messenger for Gonadotropin-releasing hormone. This hormone binds
Some hormones activate cell membrane receptors and transform them into phospholipase
Some hormones activate cell membrane receptors and transform them into phospholipase
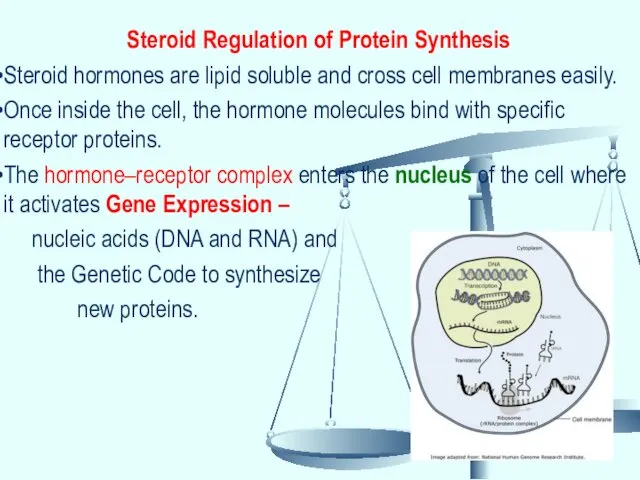
Steroid Regulation of Protein Synthesis
Steroid hormones are lipid soluble and cross
Steroid Regulation of Protein Synthesis
Steroid hormones are lipid soluble and cross

Thyroid Hormones:
Thyroxine (Tetraiodothyronine,T4 -contains 4 atoms of iodine)
Triiodothyronine (T3 -
Thyroid Hormones:
Thyroxine (Tetraiodothyronine,T4 -contains 4 atoms of iodine)
Triiodothyronine (T3 -
Antithyroid drugs:
are used to lower the functional capacity of the
Antithyroid drugs:
are used to lower the functional capacity of the
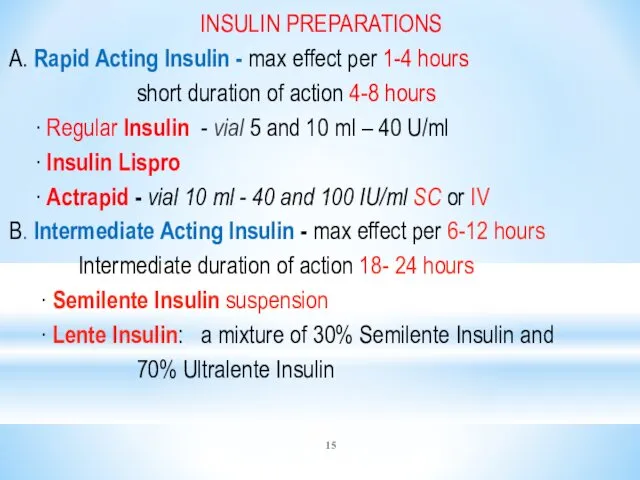
INSULIN PREPARATIONS
A. Rapid Acting Insulin - max effect per 1-4 hours
INSULIN PREPARATIONS
A. Rapid Acting Insulin - max effect per 1-4 hours
C. Prolonged acting insulin:
∙ Ultralente Insulin
max effect per
C. Prolonged acting insulin:
∙ Ultralente Insulin
max effect per
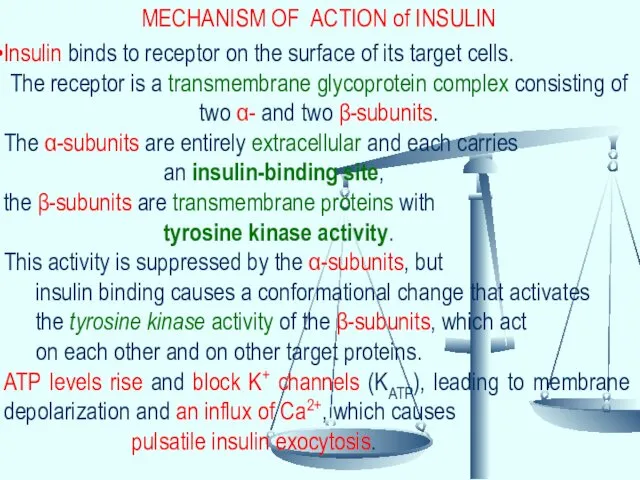
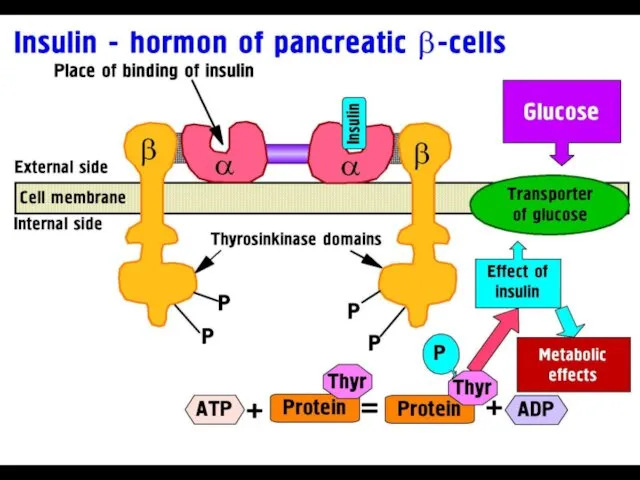
MECHANISM OF ACTION of INSULIN
Insulin binds to receptor on the surface
MECHANISM OF ACTION of INSULIN
Insulin binds to receptor on the surface
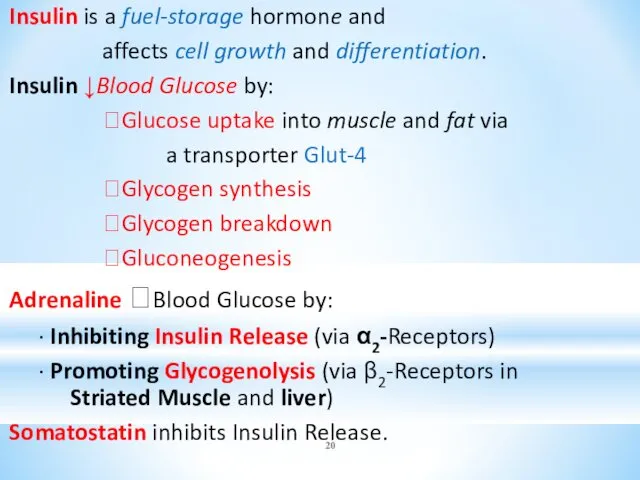
Insulin is a fuel-storage hormone and
affects cell growth and differentiation.
Insulin is a fuel-storage hormone and
affects cell growth and differentiation.
Actrapid (vial 10 ml : 40 and 100 IU/ml for SC
Actrapid (vial 10 ml : 40 and 100 IU/ml for SC

Insulin Pens
Insulin Pens
Insulin Inhaling Device (Exubera)
Insulin Inhaling Device (Exubera)
CLINICAL USES of INSULIN:
⮚ Type 1 Diabetes:
■ Diabetic Ketoacidosis
■ Short-term treatment
CLINICAL USES of INSULIN:
⮚ Type 1 Diabetes:
■ Diabetic Ketoacidosis
■ Short-term treatment
Oral (Synthetic) Hypoglycemic Agents:
I. Stimulators of insulin release by beta cells:
Oral (Synthetic) Hypoglycemic Agents:
I. Stimulators of insulin release by beta cells:
Repaglinide and Nateglinide are non-sulfonylureas meglitinides that lower blood sugar by
Repaglinide and Nateglinide are non-sulfonylureas meglitinides that lower blood sugar by
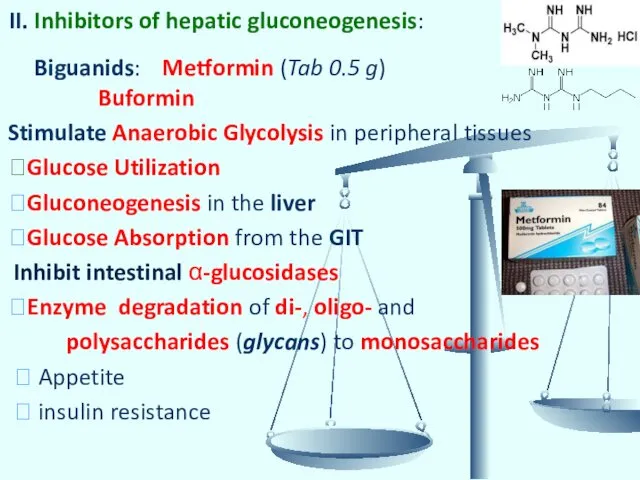
II. Inhibitors of hepatic gluconeogenesis:
Biguanids: Metformin (Tab 0.5 g)
Buformin
Stimulate
II. Inhibitors of hepatic gluconeogenesis:
Biguanids: Metformin (Tab 0.5 g)
Buformin
Stimulate
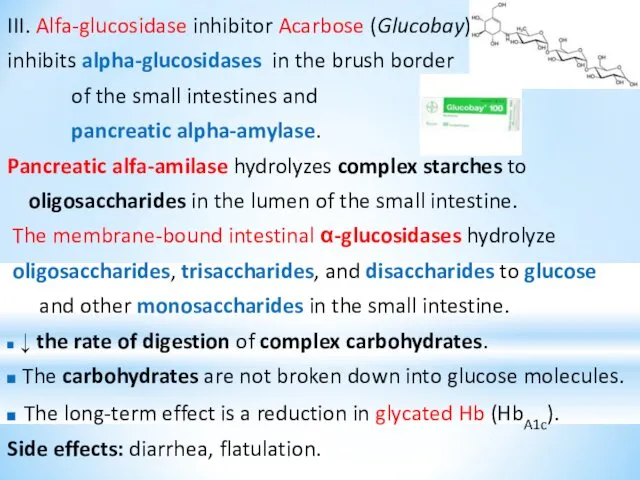
III. Alfa-glucosidase inhibitor Acarbose (Glucobay)
inhibits alpha-glucosidases in the brush border
of
III. Alfa-glucosidase inhibitor Acarbose (Glucobay)
inhibits alpha-glucosidases in the brush border
of
Classification of Glucocorticoids:
1. Short-acting: Hydrocortisone acetate, Cortisone
2. Intermediate-acting: Prednisolone , Triamcinolone
Classification of Glucocorticoids:
1. Short-acting: Hydrocortisone acetate, Cortisone
2. Intermediate-acting: Prednisolone , Triamcinolone
Action on mediators of inflammatory
and immune response:
GCs change Gene Expression:
Action on mediators of inflammatory
and immune response:
GCs change Gene Expression:
Clinical uses of Glucocorticoids:
1. Replacement therapy for patients with adrenal failure
Clinical uses of Glucocorticoids:
1. Replacement therapy for patients with adrenal failure
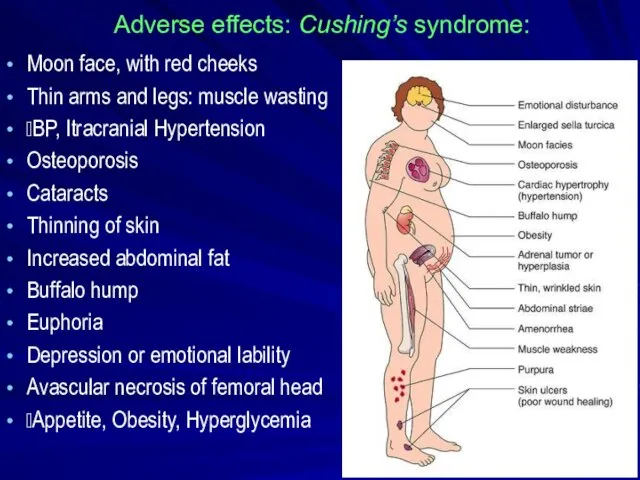
Adverse effects: Cushing’s syndrome:
Moon face, with red cheeks
Thin arms and
Adverse effects: Cushing’s syndrome:
Moon face, with red cheeks
Thin arms and

OESTROGENS
Natural:
Estradiol - amp 0.1%-1 ml
Estriol - Tab 1 mg
OESTROGENS
Natural:
Estradiol - amp 0.1%-1 ml
Estriol - Tab 1 mg
CLINICAL USEs of OESTROGENS:
Replacement therapy:
- Primary Ovarian Failure
(e.g., Turner’s syndrome)
-
CLINICAL USEs of OESTROGENS:
Replacement therapy:
- Primary Ovarian Failure
(e.g., Turner’s syndrome)
-
ANTIOESTROGENS
Clomiphene - Tab. 50 mg
Tamoxifen - Tab. 20 mg
Clomiphene:
Interfering with the
ANTIOESTROGENS
Clomiphene - Tab. 50 mg
Tamoxifen - Tab. 20 mg
Clomiphene:
Interfering with the
PROGESTOGENS
1. The naturally occurring hormone and its derivatives:
Progesteron amp. 1%
PROGESTOGENS
1. The naturally occurring hormone and its derivatives:
Progesteron amp. 1%
CLINICAL USE of PROGESTOGENS
1. CONTRACEPTION:
- combined oral contraceptive pill
CLINICAL USE of PROGESTOGENS
1. CONTRACEPTION:
- combined oral contraceptive pill
 Современные направления пластической хирургии в акушерстве и гинекологии
Современные направления пластической хирургии в акушерстве и гинекологии Неотложные состояния в офтальмологии
Неотложные состояния в офтальмологии Основы кардиохирургии. Введение
Основы кардиохирургии. Введение Патология органов речи. Стойкие нарушения речи. 2
Патология органов речи. Стойкие нарушения речи. 2 Болезнь Ниманна-Пика
Болезнь Ниманна-Пика Развитие стоматологической службы в России
Развитие стоматологической службы в России Классификация научных исследований в здравоохранении
Классификация научных исследований в здравоохранении Инфекционный процесс, диагностика и лечение при инфекционных заболеваниях
Инфекционный процесс, диагностика и лечение при инфекционных заболеваниях Повреждения слизистой полости рта у детей
Повреждения слизистой полости рта у детей Қария науқастардың күтімі
Қария науқастардың күтімі Естественное вскармливание ребенка первого года жизни
Естественное вскармливание ребенка первого года жизни Философия мен медицинадағы Болмыс және Сана ұғымдары
Философия мен медицинадағы Болмыс және Сана ұғымдары Хирургия паразитарных заболеваний
Хирургия паразитарных заболеваний History of medicine as science and subject for study. Prehistoric medicine
History of medicine as science and subject for study. Prehistoric medicine Морфологические, внешние признаки кожных заболеваний
Морфологические, внешние признаки кожных заболеваний Принципы преобразования органов хордовых
Принципы преобразования органов хордовых Острая печеночная недостаточность
Острая печеночная недостаточность СНК кафедры семейной медицины
СНК кафедры семейной медицины Методы инструментальной обработки корневых каналов
Методы инструментальной обработки корневых каналов Рациональное питание
Рациональное питание Ортодонтиялық емдеудің негізгі принциптер
Ортодонтиялық емдеудің негізгі принциптер Балаларда пародонт аурулары. Пародонт ауруларының жіктелісі. Этиологиясы, диагностика әдістері
Балаларда пародонт аурулары. Пародонт ауруларының жіктелісі. Этиологиясы, диагностика әдістері Рефлексотерапия. Показания и противопоказания к рефлексотерапии
Рефлексотерапия. Показания и противопоказания к рефлексотерапии Синдром раздраженного кишечника в амбулаторной практике
Синдром раздраженного кишечника в амбулаторной практике Влияние массажа с фототерапией у новорожденных с неонатальной желтухой на уровень билирубина
Влияние массажа с фототерапией у новорожденных с неонатальной желтухой на уровень билирубина Общая гнойная хирургическая инфекция. Сепсис
Общая гнойная хирургическая инфекция. Сепсис Жаңа туылған нәрестенің геморрагиялық синдром
Жаңа туылған нәрестенің геморрагиялық синдром Современный сосудистый доступ. Инфузионная терапия. Гемотрансфизионная терапия
Современный сосудистый доступ. Инфузионная терапия. Гемотрансфизионная терапия