- Ebola virus disease in pregnancy:

Содержание
- 2. Thanks to ... Atis Muehlenbachs, Olimpia de la Rosa Vázquez, Daniel G. Bausch, Ilana J. Schafer,
- 3. EBOLA VIRUS (EVD) An infectious Generally fetal disease marked by fever Severe internal bleeding Spread throughout
- 4. BACKGROUND Named because of Ebola River RIVER
- 5. FIRST APPEARANCE OF EVD In Sudan and Zaire in 1976 FIRST OUTBREAK In Sudan Infected over
- 6. AFFECT OF EBOLA VIRUS 1976-2014
- 7. Species of Ebolaviruses Ebolaviruses are closely related to species in the genus Marburgvirus, which was discovered
- 8. Ebola virus disease (EVD) and Marburg virus disease are caused by viruses of the Ebolavirus and
- 9. Despite the severity of filovirus infection in pregnancy for both mother and child, very little is
- 10. METHODS Patients Two pregnant women with EVD were cared for in Ebola treatment centers during ebolavirus
- 11. ELISA Rapid blood tests detect specific RNA sequences by reverse-transcription polymerase chain reaction (RT-PCR) or viral
- 12. Histopathologic Analysis, Immunohistochemical Analysis, and Transmission Electron Microscopy Placenta (Gulu and Isiro), fetal tissues (Gulu), and
- 13. RESULTS. Patient 1 Patient 1, Gulu, Uganda, 30-year-old housewife Symptoms: asthenia, anorexia, abdominal pain, nausea, vomiting,
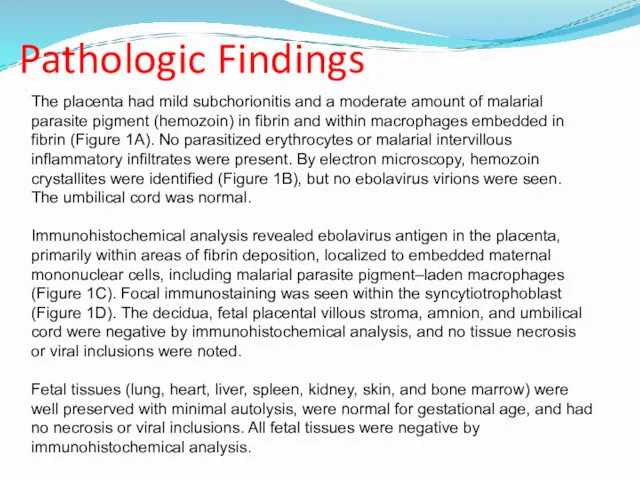
- 14. Pathologic Findings The placenta had mild subchorionitis and a moderate amount of malarial parasite pigment (hemozoin)
- 15. Placental findings from patient 1. A, Hemozoin (malarial parasite pigment) in fibrin (arrowheads). B, Transmission electron
- 16. RESULTS. Patient 2 Patient 2, 29-year-old housewife, who was transferred from a health center because of
- 17. The infant appeared healthy at birth, with Apgar scores of 8/10/10, and was clinically assessed to
- 18. Pathologic Findings In the placenta, scattered atypical maternal macrophages were seen within the intervillous space. These
- 19. Placental findings from patient 2. A, Circulating atypical maternal macrophages with vacuolated cytoplasm and eosinophilic cytoplasmic
- 20. DISCUSSION Vertical transmission of pathogens can be by transplacental, transvaginal, or by breastfeeding routes. Placenta sampling
- 21. COUNTRIES AFFECTED WITH EVD
- 22. Transmission of Ebola virus
- 23. Contd…
- 24. Types of Body Fluids That involves in transmission of Ebola virus BODY FLUIDS
- 25. Thanks for Attention!
- 26. CONTAMINATED OBJECTS THROUGH WHICH EBOLA VIRUS TRANSMITS
- 27. IN AFRICA,EBOLA VIRUS MAY BE SPREAD THROUGH BUSHMEAT
- 28. TRADITIONAL AFRICAN RITUALS PLAYED ROLE IN TRANSMISSION OF VIRUS
- 29. EBOLA VIRUS ENTRES INTO THE HUMAN’S CELL
- 30. OTHER WAYES IN WHICH EBOLA VIRUS CAN TRANSMIT
- 31. EBOLA VIRUS VICTIM’S BODY BURNED ON HUGE FUNERAL PYRE IN DESPERATE BATTLE TO STOP OUTBREAK MASS
- 32. THESE SHOCKING PICTURES SHOW THE BODIES OF EBOLA VICTIMS BEING BURNED ON HUGE FUNERAL PYRE
- 33. FRUIT BATS ARE MAJOR CAUSE FOR THE TRANSMISSION OF THE EBOLA VIRUS DISEASE
- 34. UNHYGIENIC ENVIRONMENT MAY ALSO BE A CAUSE OF TRANSMISSION OF EBOLA VIRUS IN WEST AFRICA
- 35. CDC WORKER INCINERATES MEDICAL WASTE FROM EBOLA PATIENTS IN ZAIRE
- 38. Early signs and symptoms of infections (7-9 Days) FEVER If there is no fever there is
- 39. HEADACHE Severe headaches start developing
- 40. NAUSEA Sickness in the stomach and involuntarily impulse to vomit is felt by patient.
- 41. MUSCULAR PAIN Joint and muscle pain leads to intense weakness throughout the body of the person.
- 42. TIREDNESS
- 44. Day 10th followed by: Vomiting An another major symptom to approve the person is infected by
- 45. Diarrhea
- 46. Rashes
- 47. Condition worsens on day 11th BRAIN DAMAGE Loss of consciousness , Seizures, Massive internal bleeding leads
- 48. Internal & External Bleeding Bleeding from body Openings (nose, gums ,gastrointestinal tract, etc) may be seen
- 49. Diagnosis Of Ebola Virus How it is diagnosed?
- 50. Diagnosis before testing is completed for Ebola, test for following disease must be completed Malaria Typhoid
- 51. It is difficult to distinguish EVD from other infectious diseases but it can be investigated by
- 52. Diagnostic Considerations Although there is no approved specific therapy for Ebola virus. Clinical Findings - include
- 53. A high risk exposure includes any of the following Percutaneous or mucous membrane exposure to blood
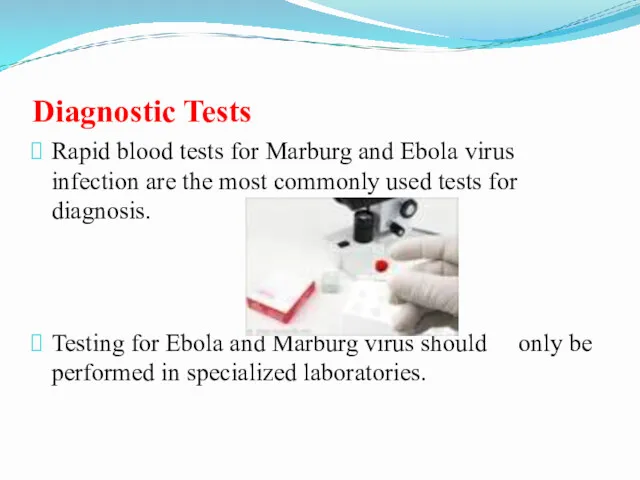
- 54. Diagnostic Tests Rapid blood tests for Marburg and Ebola virus infection are the most commonly used
- 55. Other Tests Antigen detection may be used as a confirmatory test for immediate diagnosis. For individuals,
- 56. Stages of symptoms of Ebola virus Stage 1 Headache, sore throat, fever, muscle soreness Stage 2
- 57. Hospital Protocol for Ebola hit Handling Personal Protective Equipment (PPE) Removal Isolation Fluid Control Disinfecting No
- 58. A new drug target for Ebola virus Researchers have recently developed a new drug target in
- 59. TREATMENT AND VACCINE FOR EBOLA VIRUS Coffee, Fermented Soy, homeopathic Spider Venom, And Vitamin C, May
- 60. Entry point Ebola infection enters there to be examined by medical staff in protective gear Patients
- 61. Patients could face a long wait until their test results from the lab come back, revealing
- 62. Patients suspected of having Ebola based on the initial medical examination remain here until official confirmation
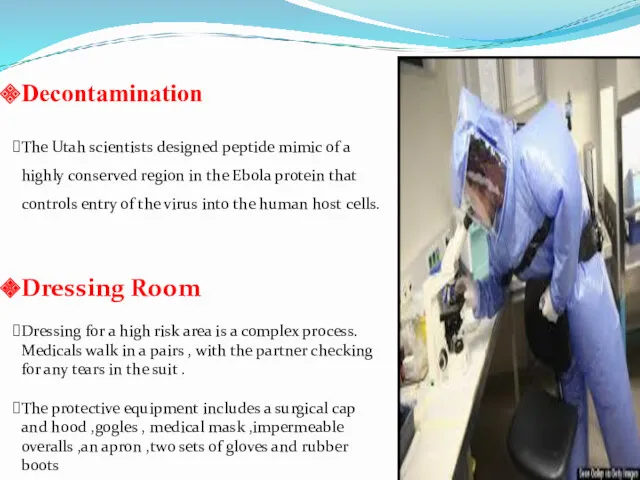
- 63. Decontamination The Utah scientists designed peptide mimic of a highly conserved region in the Ebola protein
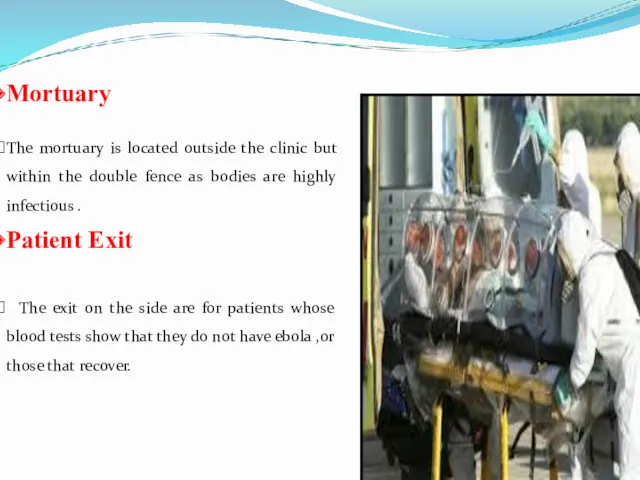
- 64. Mortuary The mortuary is located outside the clinic but within the double fence as bodies are
- 65. Statins should be considered as a possible treatment for Ebola Statins also have been suggested as
- 66. Experimental Canadian made Ebola vaccine is beginning clinical trials in healthy humans . The results are
- 68. If have sudden fever, diarrhoea, or vomiting, go to the nearest health facility Make no contact
- 70. QUICK ACCESS TO APPROPRIATE LABORATORY SERVICES
- 71. PROPER MANAGEMENT SERVICES FOR WHO ARE INFECTED
- 72. PROPER DISPOSAL OF DEAD THROUGH CREMATION OR BURIAL
- 74. Скачать презентацию
Thanks to ...
Atis Muehlenbachs, Olimpia de la Rosa Vázquez, Daniel G.
Thanks to ...
Atis Muehlenbachs, Olimpia de la Rosa Vázquez, Daniel G.
EBOLA VIRUS (EVD)
An infectious
Generally fetal disease marked by
fever
Severe internal bleeding
Spread
EBOLA VIRUS (EVD)
An infectious
Generally fetal disease marked by
fever
Severe internal bleeding
Spread
BACKGROUND
Named because of Ebola River RIVER
BACKGROUND
Named because of Ebola River RIVER
FIRST APPEARANCE OF EVD
In Sudan and Zaire in 1976
FIRST OUTBREAK
In Sudan
Infected
FIRST APPEARANCE OF EVD
In Sudan and Zaire in 1976
FIRST OUTBREAK
In Sudan
Infected
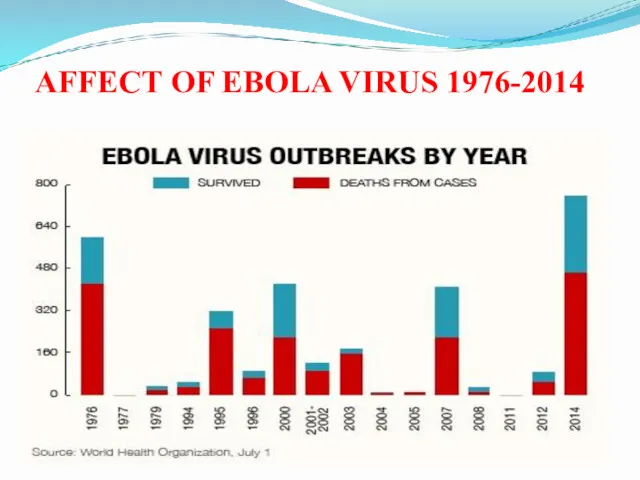
AFFECT OF EBOLA VIRUS 1976-2014
AFFECT OF EBOLA VIRUS 1976-2014
Species of Ebolaviruses
Ebolaviruses are closely related to species in the genus
Species of Ebolaviruses
Ebolaviruses are closely related to species in the genus
Ebola virus disease (EVD) and Marburg virus disease are caused by
Ebola virus disease (EVD) and Marburg virus disease are caused by
Despite the severity of filovirus infection in pregnancy for both mother
Despite the severity of filovirus infection in pregnancy for both mother
METHODS
Patients
Two pregnant women with EVD were cared for in Ebola treatment
METHODS
Patients
Two pregnant women with EVD were cared for in Ebola treatment
ELISA
Rapid blood tests detect specific RNA sequences by reverse-transcription polymerase chain
ELISA
Rapid blood tests detect specific RNA sequences by reverse-transcription polymerase chain
Histopathologic Analysis, Immunohistochemical Analysis, and Transmission Electron Microscopy
Placenta (Gulu and Isiro),
Histopathologic Analysis, Immunohistochemical Analysis, and Transmission Electron Microscopy
Placenta (Gulu and Isiro),
RESULTS. Patient 1
Patient 1, Gulu, Uganda, 30-year-old housewife
Symptoms: asthenia, anorexia, abdominal
RESULTS. Patient 1
Patient 1, Gulu, Uganda, 30-year-old housewife
Symptoms: asthenia, anorexia, abdominal
Pathologic Findings
The placenta had mild subchorionitis and a moderate amount of
Pathologic Findings
The placenta had mild subchorionitis and a moderate amount of
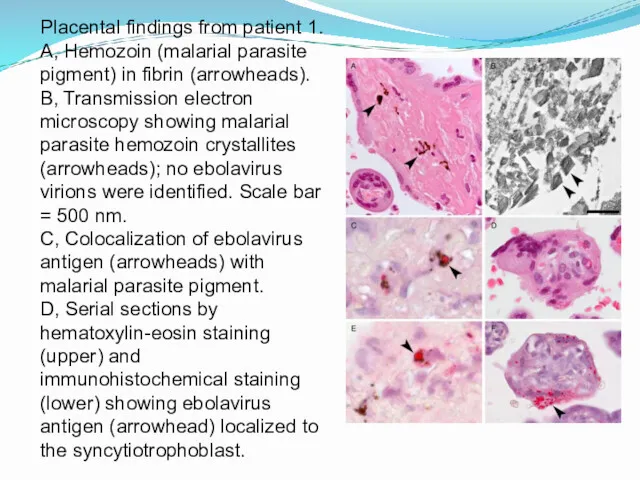
Placental findings from patient 1. A, Hemozoin (malarial parasite pigment) in
Placental findings from patient 1. A, Hemozoin (malarial parasite pigment) in
RESULTS. Patient 2
Patient 2, 29-year-old housewife, who was transferred from a
RESULTS. Patient 2
Patient 2, 29-year-old housewife, who was transferred from a
The infant appeared healthy at birth, with Apgar scores of 8/10/10,
The infant appeared healthy at birth, with Apgar scores of 8/10/10,
Pathologic Findings
In the placenta, scattered atypical maternal macrophages were seen within
Pathologic Findings
In the placenta, scattered atypical maternal macrophages were seen within
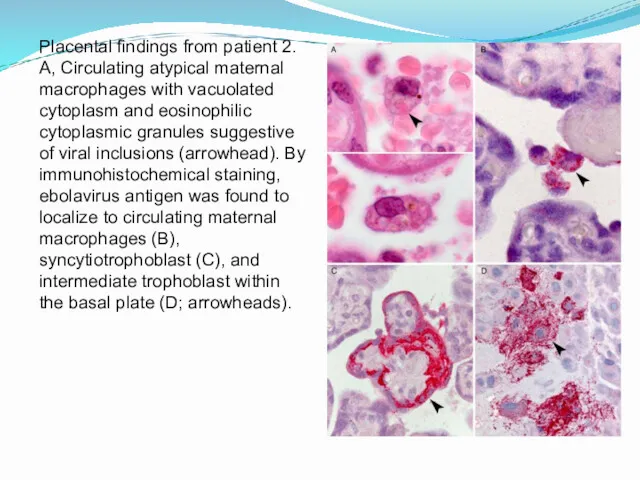
Placental findings from patient 2. A, Circulating atypical maternal macrophages with
Placental findings from patient 2. A, Circulating atypical maternal macrophages with
DISCUSSION
Vertical transmission of pathogens can be by transplacental, transvaginal, or by
DISCUSSION
Vertical transmission of pathogens can be by transplacental, transvaginal, or by

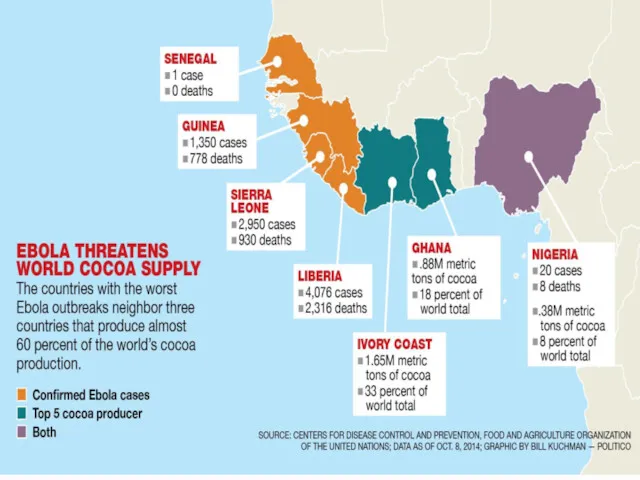
COUNTRIES AFFECTED WITH EVD
COUNTRIES AFFECTED WITH EVD
Transmission of Ebola virus
Transmission of Ebola virus
Contd…
Contd…
Types of Body Fluids That involves in transmission of Ebola virus
BODY
Types of Body Fluids That involves in transmission of Ebola virus
BODY
Thanks for Attention!
Thanks for Attention!
CONTAMINATED OBJECTS THROUGH WHICH EBOLA VIRUS TRANSMITS
CONTAMINATED OBJECTS THROUGH WHICH EBOLA VIRUS TRANSMITS

IN AFRICA,EBOLA VIRUS MAY BE SPREAD THROUGH BUSHMEAT
IN AFRICA,EBOLA VIRUS MAY BE SPREAD THROUGH BUSHMEAT
TRADITIONAL AFRICAN RITUALS PLAYED ROLE IN TRANSMISSION OF VIRUS
TRADITIONAL AFRICAN RITUALS PLAYED ROLE IN TRANSMISSION OF VIRUS
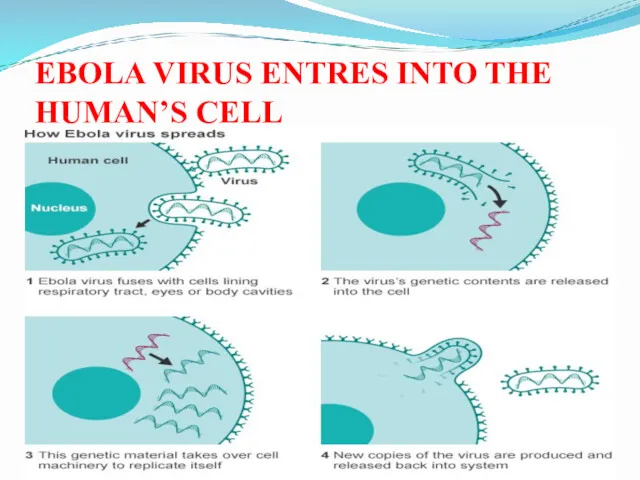
EBOLA VIRUS ENTRES INTO THE HUMAN’S CELL
EBOLA VIRUS ENTRES INTO THE HUMAN’S CELL
OTHER WAYES IN WHICH EBOLA VIRUS CAN TRANSMIT
OTHER WAYES IN WHICH EBOLA VIRUS CAN TRANSMIT
EBOLA VIRUS VICTIM’S BODY BURNED ON HUGE FUNERAL PYRE IN DESPERATE
EBOLA VIRUS VICTIM’S BODY BURNED ON HUGE FUNERAL PYRE IN DESPERATE
THESE SHOCKING PICTURES SHOW THE BODIES OF EBOLA VICTIMS BEING BURNED
THESE SHOCKING PICTURES SHOW THE BODIES OF EBOLA VICTIMS BEING BURNED
FRUIT BATS ARE MAJOR CAUSE FOR THE TRANSMISSION OF THE EBOLA
FRUIT BATS ARE MAJOR CAUSE FOR THE TRANSMISSION OF THE EBOLA
UNHYGIENIC ENVIRONMENT MAY ALSO BE A CAUSE OF TRANSMISSION OF EBOLA
UNHYGIENIC ENVIRONMENT MAY ALSO BE A CAUSE OF TRANSMISSION OF EBOLA
CDC WORKER INCINERATES MEDICAL WASTE FROM EBOLA PATIENTS IN ZAIRE
CDC WORKER INCINERATES MEDICAL WASTE FROM EBOLA PATIENTS IN ZAIRE
Early signs and symptoms of infections (7-9 Days)
FEVER
If there is
Early signs and symptoms of infections (7-9 Days)
FEVER
If there is
HEADACHE
Severe headaches start developing
HEADACHE
Severe headaches start developing
NAUSEA
Sickness in the stomach
and involuntarily impulse
to vomit is felt
NAUSEA
Sickness in the stomach
and involuntarily impulse
to vomit is felt
MUSCULAR PAIN
Joint and muscle pain leads to intense weakness throughout
MUSCULAR PAIN
Joint and muscle pain leads to intense weakness throughout
TIREDNESS
TIREDNESS
Day 10th followed by:
Vomiting
An another major
symptom to
approve the person
Day 10th followed by:
Vomiting
An another major
symptom to
approve the person

Diarrhea
Diarrhea

Rashes
Rashes
Condition worsens on day 11th
BRAIN DAMAGE
Loss of consciousness ,
Seizures,
Massive internal
Condition worsens on day 11th
BRAIN DAMAGE
Loss of consciousness ,
Seizures,
Massive internal
Internal & External Bleeding
Bleeding from body
Openings (nose, gums ,gastrointestinal tract,
Internal & External Bleeding
Bleeding from body
Openings (nose, gums ,gastrointestinal tract,
Diagnosis Of Ebola Virus
How it is diagnosed?
Diagnosis Of Ebola Virus
How it is diagnosed?
Diagnosis before testing is completed for Ebola, test for following disease
Diagnosis before testing is completed for Ebola, test for following disease
It is difficult to distinguish EVD from other infectious diseases but
It is difficult to distinguish EVD from other infectious diseases but
Diagnostic Considerations
Although there is no approved specific therapy for Ebola virus.
Clinical
Diagnostic Considerations
Although there is no approved specific therapy for Ebola virus.
Clinical
A high risk exposure includes any of the following
Percutaneous or mucous
A high risk exposure includes any of the following
Percutaneous or mucous
Diagnostic Tests
Rapid blood tests for Marburg and Ebola virus infection are
Diagnostic Tests
Rapid blood tests for Marburg and Ebola virus infection are
Other Tests
Antigen detection may be used as a confirmatory test for
Other Tests
Antigen detection may be used as a confirmatory test for
Stages of symptoms of Ebola virus
Stage 1
Headache, sore throat, fever,
Stages of symptoms of Ebola virus
Stage 1
Headache, sore throat, fever,
Hospital Protocol for Ebola hit
Handling Personal Protective Equipment (PPE)
Removal
Isolation
Fluid Control
Disinfecting
No Needles
Hospital Protocol for Ebola hit
Handling Personal Protective Equipment (PPE)
Removal
Isolation
Fluid Control
Disinfecting
No Needles
A new drug target for Ebola virus
Researchers have recently developed a
A new drug target for Ebola virus
Researchers have recently developed a
TREATMENT AND VACCINE FOR EBOLA VIRUS
Coffee, Fermented Soy, homeopathic Spider
TREATMENT AND VACCINE FOR EBOLA VIRUS
Coffee, Fermented Soy, homeopathic Spider
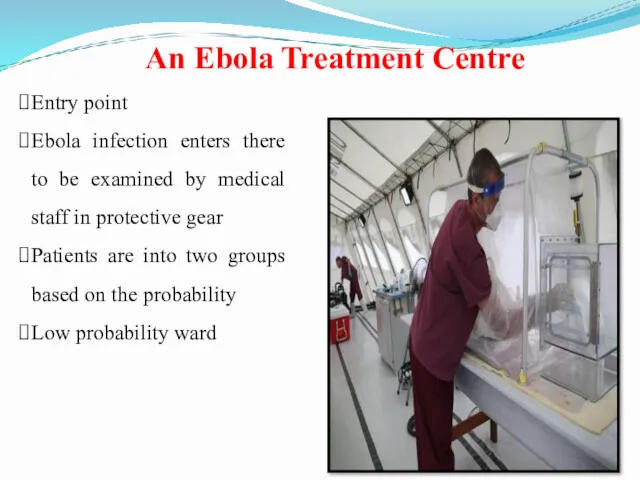
Entry point
Ebola infection enters there to be examined by medical
Entry point
Ebola infection enters there to be examined by medical
Patients could face a long wait until their test results from
Patients could face a long wait until their test results from
Patients suspected of having Ebola based on the initial medical examination
Patients suspected of having Ebola based on the initial medical examination
Decontamination
The Utah scientists designed peptide mimic of a highly conserved region
Decontamination
The Utah scientists designed peptide mimic of a highly conserved region
Mortuary
The mortuary is located outside the clinic but within the double
Mortuary
The mortuary is located outside the clinic but within the double
Statins should be considered as a possible treatment for Ebola
Statins also
Statins also
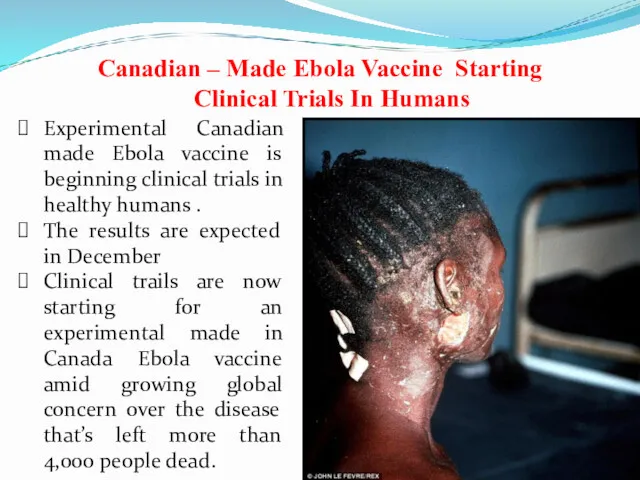
Experimental Canadian made Ebola vaccine is beginning clinical trials in healthy
Experimental Canadian made Ebola vaccine is beginning clinical trials in healthy
If have sudden fever, diarrhoea, or vomiting, go to the nearest
If have sudden fever, diarrhoea, or vomiting, go to the nearest

QUICK ACCESS TO APPROPRIATE LABORATORY SERVICES
QUICK ACCESS TO APPROPRIATE LABORATORY SERVICES

PROPER MANAGEMENT SERVICES FOR WHO ARE INFECTED
PROPER MANAGEMENT SERVICES FOR WHO ARE INFECTED
PROPER DISPOSAL OF DEAD THROUGH CREMATION OR BURIAL
PROPER DISPOSAL OF DEAD THROUGH CREMATION OR BURIAL
 Физиология системы кровообращения и работы сердца
Физиология системы кровообращения и работы сердца Leczenie systemowe nowotworów przewodu pokarmowego
Leczenie systemowe nowotworów przewodu pokarmowego Об особенностях планирования и проведения профилактических мероприятий в 2023 году на территории Астраханской области
Об особенностях планирования и проведения профилактических мероприятий в 2023 году на территории Астраханской области The Heart
The Heart Жатыр мойны және денесінің обыры тақырыбына презентация
Жатыр мойны және денесінің обыры тақырыбына презентация Анатомия и гистология зуба
Анатомия и гистология зуба Здоровые зубы
Здоровые зубы ЦД у вагітних
ЦД у вагітних Оказание первой помощи при несчастных случаях на производстве
Оказание первой помощи при несчастных случаях на производстве The Digestive system. Embryogenesis and congenital abnormalities. The Particularities of the child’s digestion
The Digestive system. Embryogenesis and congenital abnormalities. The Particularities of the child’s digestion Адам паппилома вирусы инфекциясына қарсы вакцинаның эффективтілігі мен қауіпсіздігі
Адам паппилома вирусы инфекциясына қарсы вакцинаның эффективтілігі мен қауіпсіздігі Лечение зоонозных инфекций. Бруцеллез
Лечение зоонозных инфекций. Бруцеллез Водолечение. Механизмы действия
Водолечение. Механизмы действия Физиология микроциркуляции. Особенности кровообращения в различных сосудистых областях
Физиология микроциркуляции. Особенности кровообращения в различных сосудистых областях Наследственные болезни человека
Наследственные болезни человека Проект intervertebral discs
Проект intervertebral discs Гепатобилиарлық жүйенің,ұйқы безінің аурулары кезіндегі емдік тамақтану
Гепатобилиарлық жүйенің,ұйқы безінің аурулары кезіндегі емдік тамақтану Вегетативные дисфункции у детей
Вегетативные дисфункции у детей Этапы формирования кроветворных органов в филогенезе
Этапы формирования кроветворных органов в филогенезе ДВС-синдром
ДВС-синдром Нестероидные противовоспалительные средства
Нестероидные противовоспалительные средства Ауруханаішілік инфекциялардың қоздырғыштары
Ауруханаішілік инфекциялардың қоздырғыштары Тіс жақ аппаратының биомеханикасы және жалпы түсінігі
Тіс жақ аппаратының биомеханикасы және жалпы түсінігі Желудочковые нарушения ритма сердца
Желудочковые нарушения ритма сердца Противотуберкулезные средства
Противотуберкулезные средства Клиническая анатомия уха
Клиническая анатомия уха Синдром Марфана
Синдром Марфана Туберкулёз и алкоголизм. Туберкулёз и наркомания
Туберкулёз и алкоголизм. Туберкулёз и наркомания