The Digestive system. Embryogenesis and congenital abnormalities. The Particularities of the child’s digestion презентация
- The Digestive system. Embryogenesis and congenital abnormalities. The Particularities of the child’s digestion

Содержание
- 2. Embryogenesis and congenital abnormalities. The shaping of the digestive organs occurs at early stage of the
- 3. Primary gut At 12- th day the primary gut divides on two parts. The first part
- 4. Oropharingeal and cloecal membranes The primary gut of embryo as a tube starts and finishes blindly
- 5. Cleft lip
- 6. Anocutaneous fistula. The bead of meconium became visible only at 36 hours of life. (From Wyllie
- 7. 1 mo old embryo The formation of differential divisions of the digestive tract begins after 4
- 8. The embryonic and postnatal features of digestive system organs.
- 9. The esophagus. The normally formed esophagus serves for transport of the food wad from oral cavity
- 10. Esophagal atresia. Folded feeding tube in the esophagus.
- 11. The stomach. The orderly formed stomach serves as reservoir for food and for its primary fermentation.
- 12. The further intensive development of the stomach occurs in period after child birth.
- 13. The stomach. It is a rule that the stomach physiological volume is smaller than its anatomical
- 14. The stomach. The anatomical parts of the stomach develop unevenly after birth. The stomach bottom and
- 15. In infancy, regurgitation is most commonly secondary to developmental gastroesophageal reflux and resolves spontaneously. This infant
- 16. The stomach. The pyloric sphincter of stomach is developed well since child`s delivery. The condition when
- 17. The stomach. The hypertrophic condition of pyloric sphincter (pylorostenosis) is the most common innate anomaly of
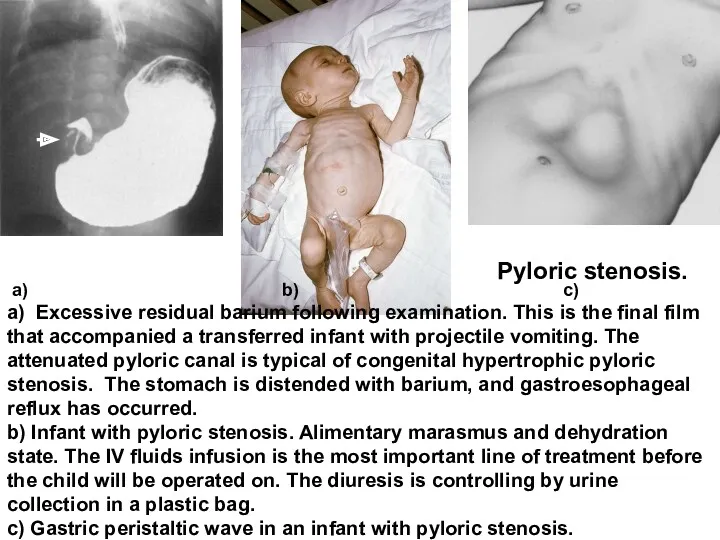
- 18. а) b) c) a) Excessive residual barium following examination. This is the final film that accompanied
- 19. GUT The Bowel is an organ in which the main processes of digestion occur. The bowel
- 20. Tumbling of the bowel The anterior knee develops most intensively and forms many flexures. At early
- 21. a) In embryo the bowel hungs in saggital plane before to begin a tumbling; it must
- 22. А. The abnormality of the first period of intestinal tumbling. 1. Hernia of the umbilical cord.
- 23. B. The abnormality of the second period of intestinal tumbling. 1. Abnormal insufficient tumbling of the
- 24. The mechanism of intestinal obstruction with incomplete rotation of the midgut (malrotation). The dotted lines show
- 25. Abdominal roentgenogram of a newborn infant held upright. Note the "double bubble" gas shadow above and
- 26. В. The abnormality of the third period of intestinal tumbling: 1. The High location of the
- 27. The relationship between the embryonic vitelline bag, vitelline stem and Mekkel’s diverticulum. The degree of vitelline
- 28. The small intestine The small intestine has 3 parts in proximal-distal direction: duodenum, jejunum and ileum.
- 29. Colon The large intestine (Colon). The development of large intestine (intestinum grassum) does not end with
- 30. Hirschsprung disease (megacolon). Roentgenogram showing extension into the ileum. Lesion at operation. а б
- 31. The Caecum. The caecum of newborn has a cone-shaped or cratered form and is situated higher
- 32. Intussusception in an infant. The obstruction is evident in the proximal transverse colon. Contrast material between
- 33. The Colon. The Colon surrounds the intestine loops in the manner of rim. The ascendant part
- 34. The Colon. The Transverse part of colon (colon transversum) takes its horizontal position only in 2
- 35. The Colon. S-figurative colon (colon sigmoid) in newborns is comparatively longer than other divisions of bowel
- 36. The rectum. Reсtum is also comparatively long and can occupy all the small pelvis in infants.
- 37. Intestinal microbiota as a personal digestive additional organ. The bowel of embryo is sterile in uteri.
- 38. rРНК-FISH hybridization. Bacteroides – orange color, Eubacterium rectale - red, others green (x400). The wall of
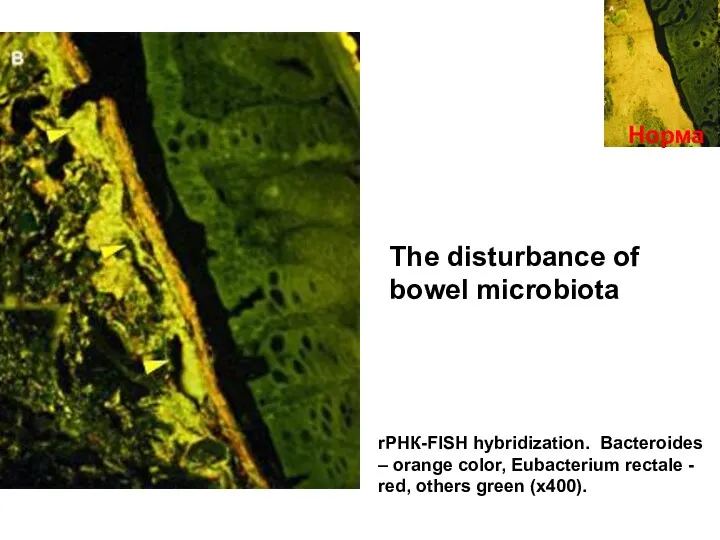
- 39. Норма The disturbance of bowel microbiota rРНК-FISH hybridization. Bacteroides – orange color, Eubacterium rectale - red,
- 40. catastrophe
- 41. The Digestive glands. Salivary glands. During the first months of life the physiological role of them
- 42. The Liver and bilious ducti. The Gall bladder The Liver with the system of bilious ducti
- 43. Atresia of the liver dusts Most common hereditary pathology of the liver is an atresia of
- 44. The Particularities of digestive processes in children. Evolutionary types of feeding.
- 45. Antenatal period. The several types of feeding. In embryo the main type of feeding is hysterothrophic.
- 46. Only breast or milk feeding! The condition of digestive organs at the moment of the human
- 47. What is the distant digestion? The distant digestion is a process realized by action of digestive
- 48. Salivary glands During the first months of life the physiological role of saliva in children is
- 49. Stomach After establishing of enteral feeding the capacity of stomach quickly increases. On 4th day after
- 50. Pancreas The exocrine (digestive) function of pancreas in small children is comparatively low, but it provides
- 51. Liver The liver is comparatively large in newborn but in its functional attitude it characterizes by
- 52. Considering limited possibilities of distant digestion in early infants the milk feeding is the important stage
- 53. Membranous digestion The bowel of infants compensates the enzymes insufficiency of organs which provide the distant
- 54. Particularities of the digestion in heterotrophic feeding stage. After full transition of the child to heterotrophic
- 55. Particularities of bowel motor functions in children. The bowel motor function is realized in children due
- 56. Meconium During the first days (before 72 hours) after the birth a well children discharge stool.
- 57. Anorectal plug from child who had not passed meconium for 2 days after birth. Pale end
- 58. Meconial aspiration Some times the fetus should do defecation in uteri before the birth or during
- 60. Скачать презентацию
Embryogenesis and congenital abnormalities.
The shaping of the digestive organs occurs at
Embryogenesis and congenital abnormalities.
The shaping of the digestive organs occurs at
Primary gut
At 12- th day the primary gut divides on two
Primary gut
At 12- th day the primary gut divides on two
Oropharingeal and cloecal membranes
The primary gut of embryo as a
Oropharingeal and cloecal membranes
The primary gut of embryo as a
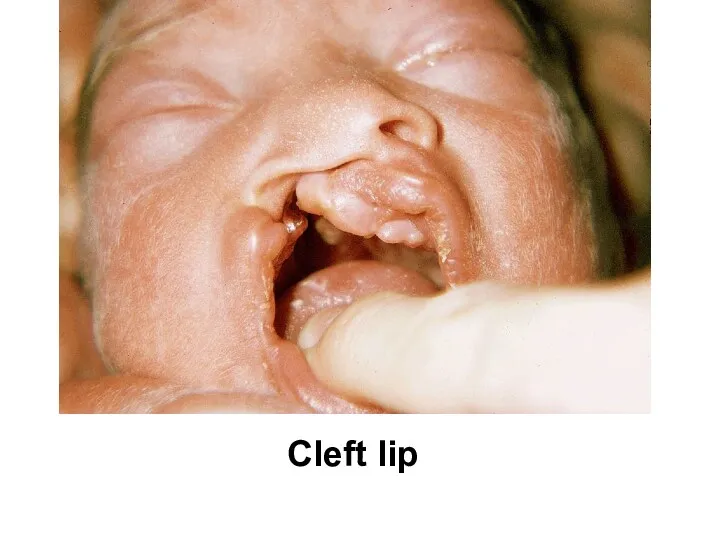
Cleft lip
Cleft lip
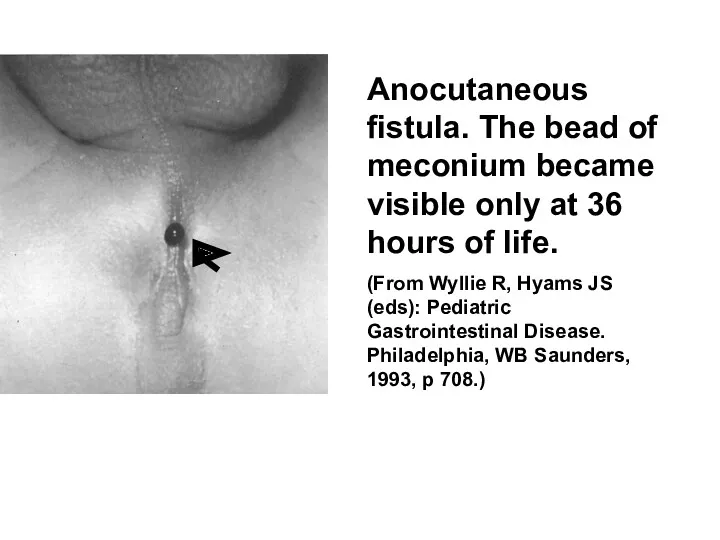
Anocutaneous fistula. The bead of meconium became visible only at 36
Anocutaneous fistula. The bead of meconium became visible only at 36
1 mo old embryo
The formation of differential divisions of the digestive
1 mo old embryo
The formation of differential divisions of the digestive
The embryonic and postnatal features of digestive system organs.
The embryonic and postnatal features of digestive system organs.
The esophagus.
The normally formed esophagus serves for transport of the food
The esophagus.
The normally formed esophagus serves for transport of the food
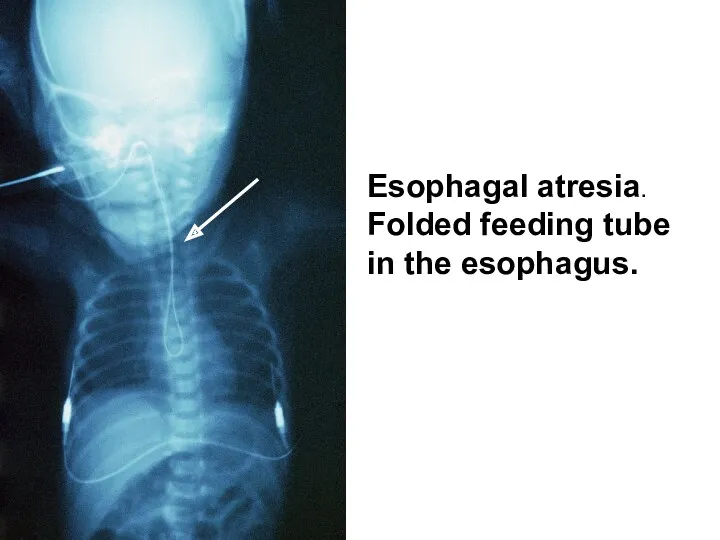
Esophagal atresia. Folded feeding tube in the esophagus.
Esophagal atresia. Folded feeding tube in the esophagus.
The stomach.
The orderly formed stomach serves as reservoir for food and
The stomach.
The orderly formed stomach serves as reservoir for food and
The further intensive development of the stomach occurs in period after
The further intensive development of the stomach occurs in period after
The stomach.
It is a rule that the stomach physiological volume is
The stomach.
It is a rule that the stomach physiological volume is
The stomach.
The anatomical parts of the stomach develop unevenly after birth.
The stomach.
The anatomical parts of the stomach develop unevenly after birth.
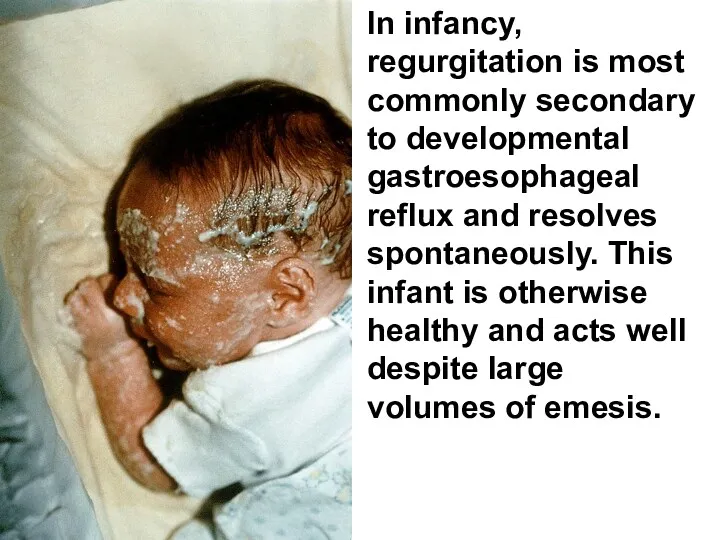
In infancy, regurgitation is most commonly secondary to developmental gastroesophageal reflux
In infancy, regurgitation is most commonly secondary to developmental gastroesophageal reflux
The stomach.
The pyloric sphincter of stomach is developed well since child`s
The stomach.
The pyloric sphincter of stomach is developed well since child`s
The stomach.
The hypertrophic condition of pyloric sphincter (pylorostenosis) is the most
The stomach.
The hypertrophic condition of pyloric sphincter (pylorostenosis) is the most
а) b) c)
a) Excessive residual barium following examination. This is
а) b) c)
a) Excessive residual barium following examination. This is
GUT
The Bowel is an organ in which the main processes of
GUT
The Bowel is an organ in which the main processes of
Tumbling of the bowel
The anterior knee develops most intensively and forms
Tumbling of the bowel
The anterior knee develops most intensively and forms
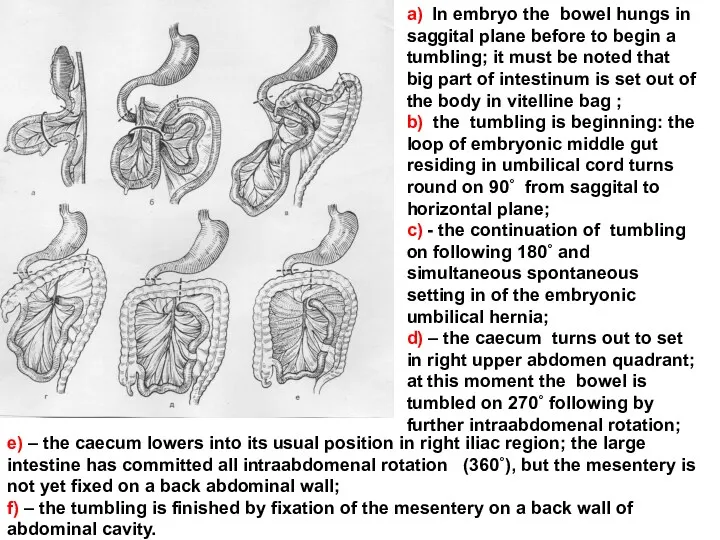
a) In embryo the bowel hungs in saggital plane before to
a) In embryo the bowel hungs in saggital plane before to
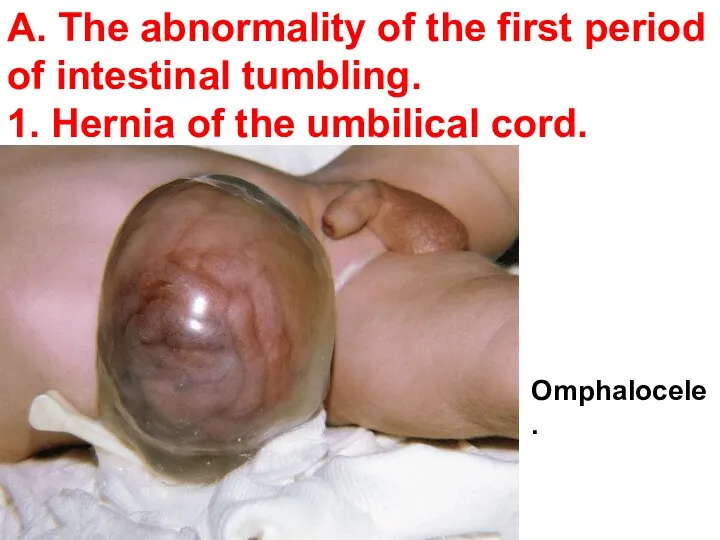
А. The abnormality of the first period of intestinal tumbling.
1. Hernia
А. The abnormality of the first period of intestinal tumbling.
1. Hernia
B. The abnormality of the second period of intestinal tumbling.
1. Abnormal insufficient
B. The abnormality of the second period of intestinal tumbling.
1. Abnormal insufficient
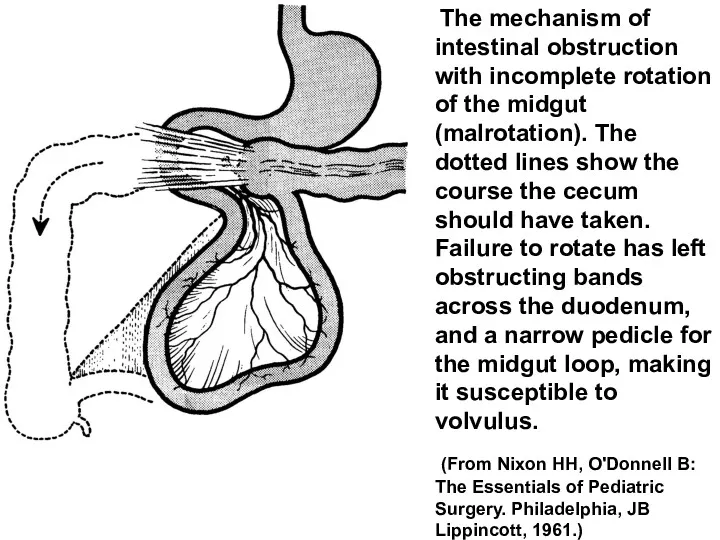
The mechanism of intestinal obstruction with incomplete rotation of the
The mechanism of intestinal obstruction with incomplete rotation of the
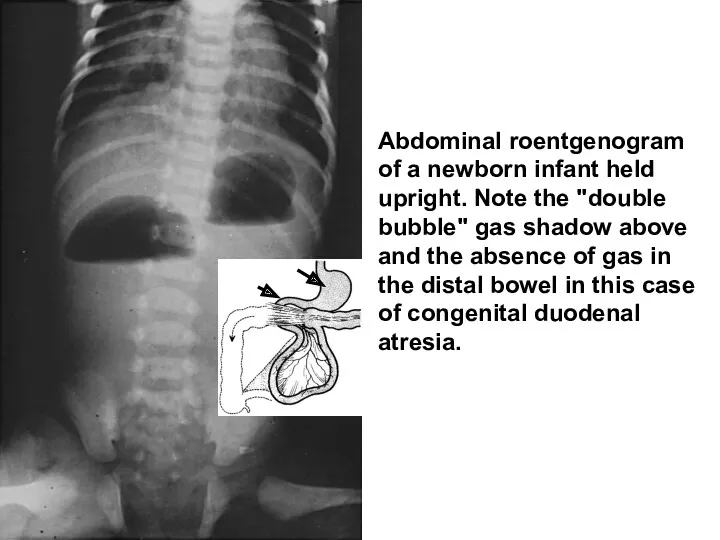
Abdominal roentgenogram of a newborn infant held upright. Note the "double
Abdominal roentgenogram of a newborn infant held upright. Note the "double
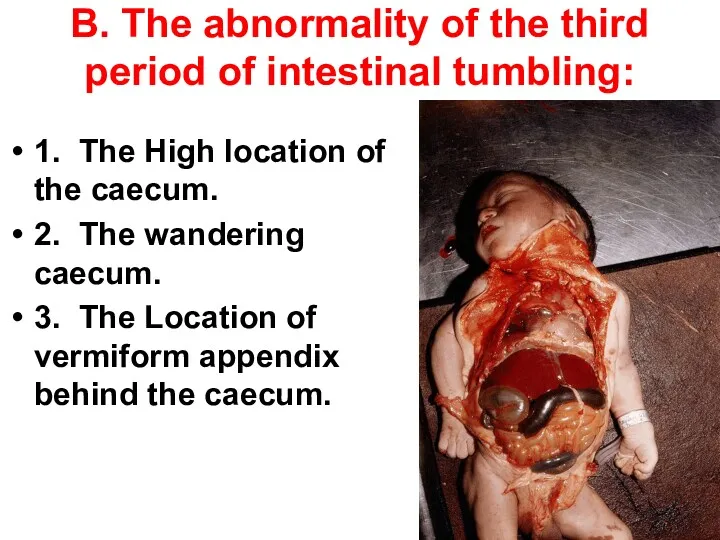
В. The abnormality of the third period of intestinal tumbling:
1. The High
В. The abnormality of the third period of intestinal tumbling:
1. The High
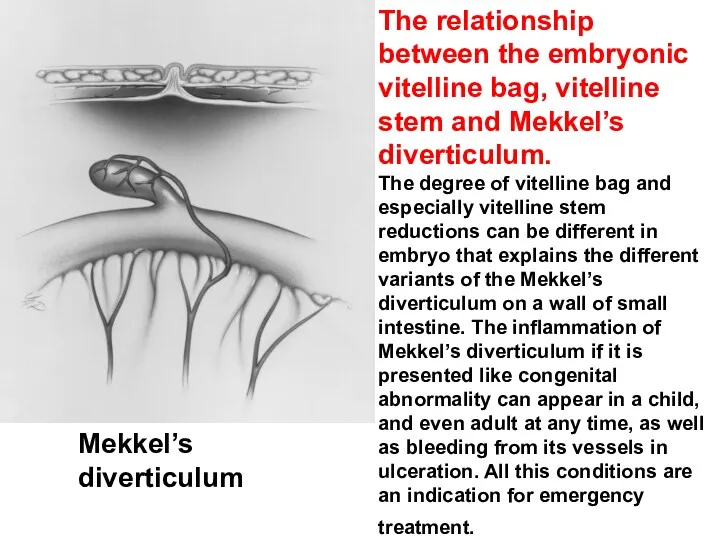
The relationship between the embryonic vitelline bag, vitelline stem and Mekkel’s
The relationship between the embryonic vitelline bag, vitelline stem and Mekkel’s
The small intestine
The small intestine has 3 parts in proximal-distal direction:
The small intestine
The small intestine has 3 parts in proximal-distal direction:
Colon
The large intestine (Colon). The development of large intestine (intestinum grassum)
Colon
The large intestine (Colon). The development of large intestine (intestinum grassum)
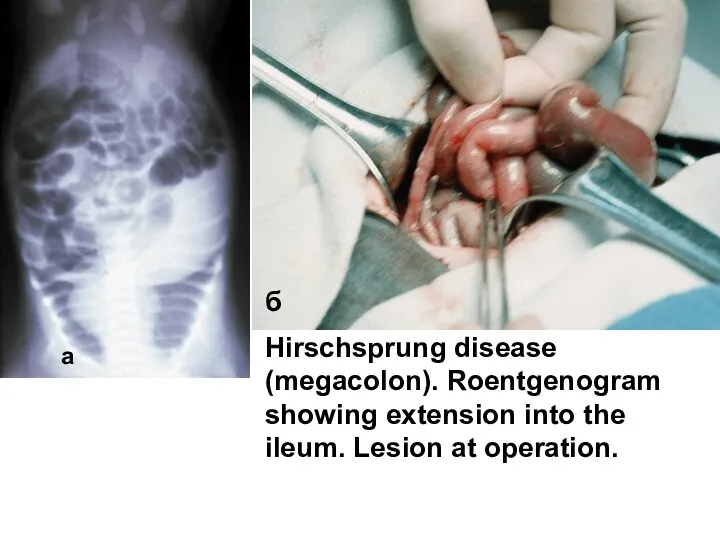
Hirschsprung disease (megacolon). Roentgenogram showing extension into the ileum. Lesion at
Hirschsprung disease (megacolon). Roentgenogram showing extension into the ileum. Lesion at
The Caecum.
The caecum of newborn has a cone-shaped or cratered form
The Caecum.
The caecum of newborn has a cone-shaped or cratered form
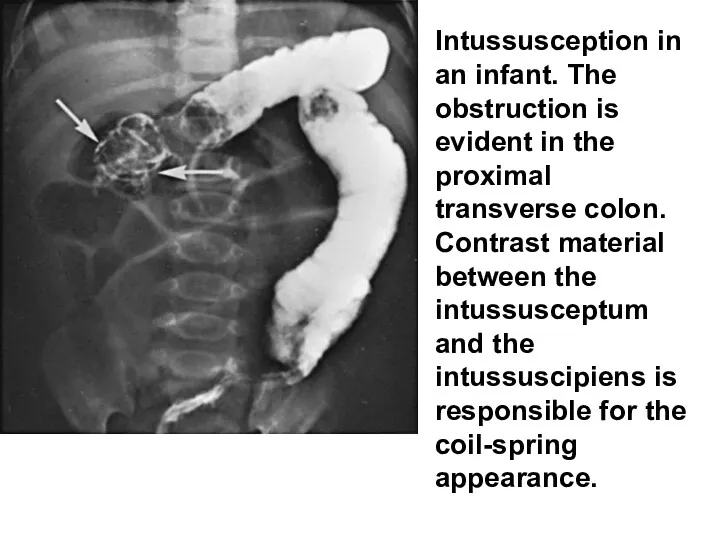
Intussusception in an infant. The obstruction is evident in the proximal
Intussusception in an infant. The obstruction is evident in the proximal
The Colon.
The Colon surrounds the intestine loops in the manner of
The Colon.
The Colon surrounds the intestine loops in the manner of
The Colon.
The Transverse part of colon (colon transversum) takes its horizontal
The Colon.
The Transverse part of colon (colon transversum) takes its horizontal
The Colon.
S-figurative colon (colon sigmoid) in newborns is comparatively longer than
The Colon.
S-figurative colon (colon sigmoid) in newborns is comparatively longer than
The rectum.
Reсtum is also comparatively long and can occupy all the
The rectum.
Reсtum is also comparatively long and can occupy all the
Intestinal microbiota as a personal digestive additional organ.
The bowel of embryo
Intestinal microbiota as a personal digestive additional organ.
The bowel of embryo
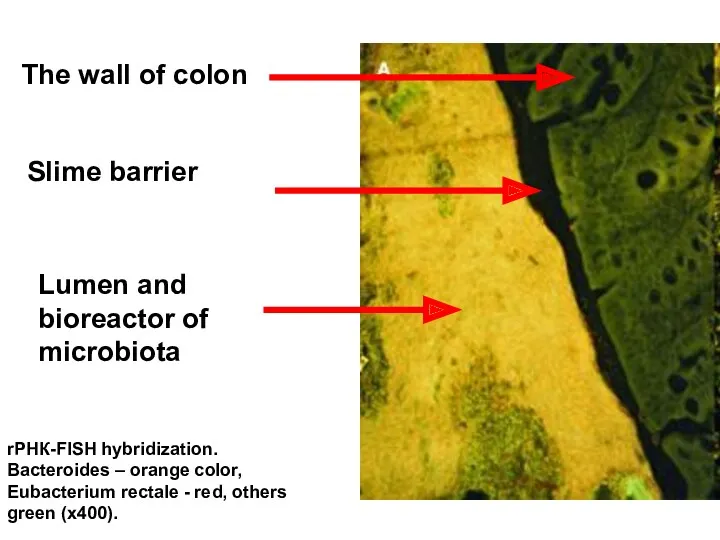
rРНК-FISH hybridization. Bacteroides – orange color, Eubacterium rectale - red, others
rРНК-FISH hybridization. Bacteroides – orange color, Eubacterium rectale - red, others
Норма
The disturbance of bowel microbiota
rРНК-FISH hybridization. Bacteroides – orange color, Eubacterium
Норма
The disturbance of bowel microbiota
rРНК-FISH hybridization. Bacteroides – orange color, Eubacterium
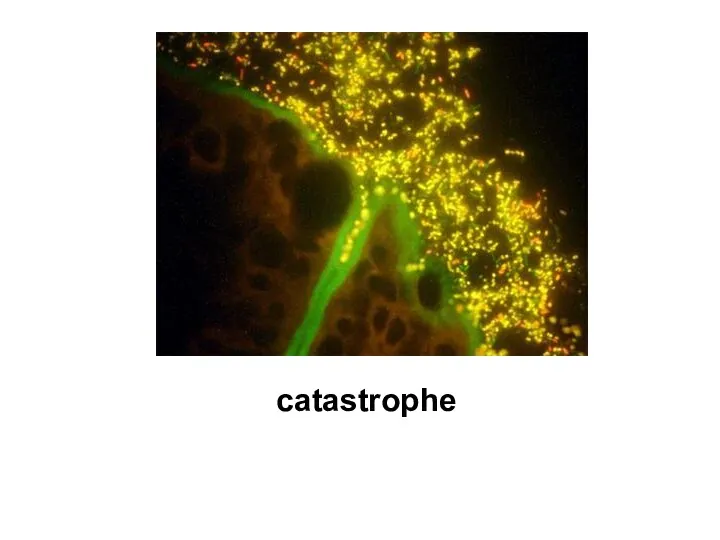
catastrophe
catastrophe
The Digestive glands.
Salivary glands. During the first months of life the
The Digestive glands.
Salivary glands. During the first months of life the
The Liver and bilious ducti. The Gall bladder
The Liver with
The Liver and bilious ducti. The Gall bladder
The Liver with
Atresia of the liver dusts
Most common hereditary pathology of the liver
Atresia of the liver dusts
Most common hereditary pathology of the liver
The Particularities of digestive processes in children. Evolutionary types of feeding.
The Particularities of digestive processes in children. Evolutionary types of feeding.
Antenatal period. The several types of feeding.
In embryo the main type
Antenatal period. The several types of feeding.
In embryo the main type
Only breast or milk feeding!
The condition of digestive organs at the
Only breast or milk feeding!
The condition of digestive organs at the
What is the distant digestion?
The distant digestion is a process realized
What is the distant digestion?
The distant digestion is a process realized
Salivary glands
During the first months of life the physiological role of
Salivary glands
During the first months of life the physiological role of
Stomach
After establishing of enteral feeding the capacity of stomach quickly
Stomach
After establishing of enteral feeding the capacity of stomach quickly
Pancreas
The exocrine (digestive) function of pancreas in small children is comparatively
Pancreas
The exocrine (digestive) function of pancreas in small children is comparatively
Liver
The liver is comparatively large in newborn but in its
Liver
The liver is comparatively large in newborn but in its
Considering limited possibilities of distant digestion in early infants the milk
Considering limited possibilities of distant digestion in early infants the milk
Membranous digestion
The bowel of infants compensates the enzymes insufficiency of organs
Membranous digestion
The bowel of infants compensates the enzymes insufficiency of organs
Particularities of the digestion in heterotrophic feeding stage.
After full transition of
Particularities of the digestion in heterotrophic feeding stage.
After full transition of
Particularities of bowel motor functions in children.
The bowel motor function is
Particularities of bowel motor functions in children.
The bowel motor function is
Meconium
During the first days (before 72 hours) after the birth a
Meconium
During the first days (before 72 hours) after the birth a
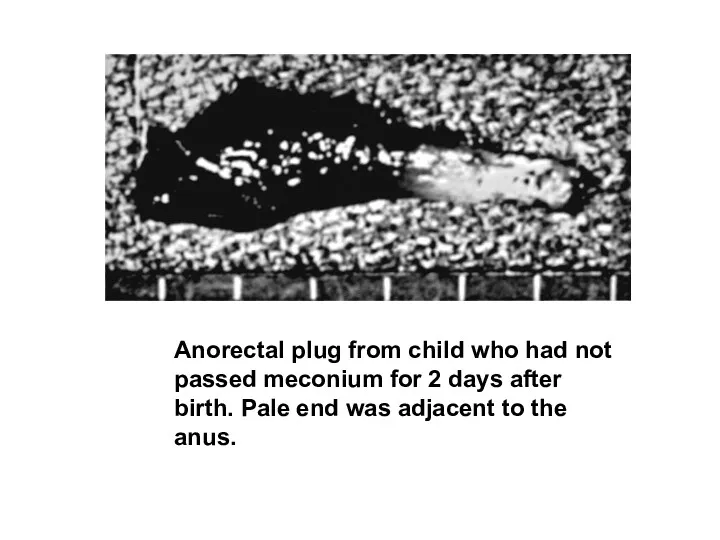
Anorectal plug from child who had not passed meconium for 2
Anorectal plug from child who had not passed meconium for 2
Meconial aspiration
Some times the fetus should do defecation in uteri before
Meconial aspiration
Some times the fetus should do defecation in uteri before
 Клинико-лабораторная и инструментальная диагностика основных синдромов при заболеваниях желудка и кишечника
Клинико-лабораторная и инструментальная диагностика основных синдромов при заболеваниях желудка и кишечника Профилактика внутрибольничных инфекций
Профилактика внутрибольничных инфекций Лидерские качества врача и их значение в профессиональной деятельности
Лидерские качества врача и их значение в профессиональной деятельности Витамин B1
Витамин B1 Безпека праці в фармацевтичних закладах
Безпека праці в фармацевтичних закладах Физиологические роды
Физиологические роды Патогенетическая терапия в лечении острых кишечных инфекций у детей
Патогенетическая терапия в лечении острых кишечных инфекций у детей Переменные электромагнитные поля высокой частоты. Дарсонвализация, УВЧ терапия, франклинизация, индуктотермия, СВЧ терапия
Переменные электромагнитные поля высокой частоты. Дарсонвализация, УВЧ терапия, франклинизация, индуктотермия, СВЧ терапия Общие принципы лечения переломов
Общие принципы лечения переломов Волонтеры-медики
Волонтеры-медики Коклюш у детей
Коклюш у детей Лихорадки у детей
Лихорадки у детей Психические расстройства при органических заболеваниях головного мозга
Психические расстройства при органических заболеваниях головного мозга Жыныс функциясының бұзылыстары. Климакс
Жыныс функциясының бұзылыстары. Климакс Клинико-диагностические и лечебные мероприятия при эрлихиозе собак в условиях ветеринарной клиники
Клинико-диагностические и лечебные мероприятия при эрлихиозе собак в условиях ветеринарной клиники Патохимия, диагностика и коррекция нарушений обмена углеводов у детей (сахарный диабет, галактоземия, фруктоземия)
Патохимия, диагностика и коррекция нарушений обмена углеводов у детей (сахарный диабет, галактоземия, фруктоземия) Медицина в Казахстане
Медицина в Казахстане Геморрагические заболевания у новорожденных
Геморрагические заболевания у новорожденных Дизартрия, коррекция. 1 этап
Дизартрия, коррекция. 1 этап Проблема життя та смерті у медичній етиці та деонтології. Евтаназія: морально-етичні проблеми
Проблема життя та смерті у медичній етиці та деонтології. Евтаназія: морально-етичні проблеми Врачебный контроль в физической культуре и спорте
Врачебный контроль в физической культуре и спорте Стресс. Симптомы стресса. Лечения и профилактика стресса
Стресс. Симптомы стресса. Лечения и профилактика стресса Неинфекционный энтерит и колит. Синдром раздраженного кишечника
Неинфекционный энтерит и колит. Синдром раздраженного кишечника Догляд за хворими з хірургічними захворюваннями і ушкодженнями хребта і таза
Догляд за хворими з хірургічними захворюваннями і ушкодженнями хребта і таза Профессиональная интоксикация пестицидами
Профессиональная интоксикация пестицидами Вчення про інфекційні хвороби. Загальна патологія інфекційних хвороб. Основи профілактики інфекційних хвороб
Вчення про інфекційні хвороби. Загальна патологія інфекційних хвороб. Основи профілактики інфекційних хвороб Пищевая аллергия
Пищевая аллергия Метод лактаційної аменореї
Метод лактаційної аменореї