- Endometriosis. Diagnostic method, treatment, prophylaxis

Содержание
- 2. Endometriosis is a disease in which endometrial glands and stroma implant and grow in areas outside
- 3. FEATURES OF ENDOMETRIOSIS •Prevalence 2-50% of women; 21-47% of infertility cases •Exposure to ovarian hormones appears
- 4. IS ENDOMETRIOSIS INCREASING? •1965-1984, endometriosis rose from 10 to 19% as primary indication for hysterectomy •Simultaneously,
- 5. ETIOLOGIES OF ENDOMETRIOSIS •Sampson's theory: Retrograde menses and peritoneal implantation –Most women retrograde menstruate •Meyer's theory:
- 6. NORMAL PELVIC STRUCTURES
- 7. ENDOMETRIOSIS
- 8. CLASSIFICATION OF ENDOMETRIOSIS
- 9. CLINICAL PRESENTATION Pelvic pain •Infertility •Pelvic mass
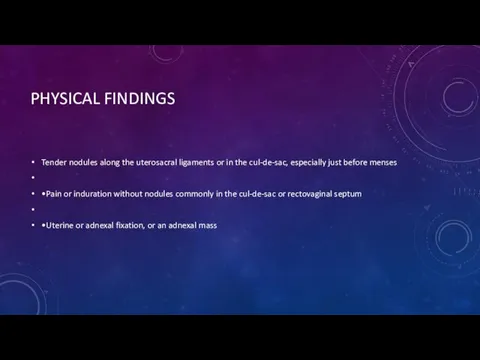
- 10. PHYSICAL FINDINGS Tender nodules along the uterosacral ligaments or in the cul-de-sac, especially just before menses
- 11. DIAGNOSIS OF ENDOMETRIOSIS Diagnosis of Endometriosis •Direct visualization of implants – Laparoscopically – Conscious pain mapping
- 12. ENDOMETRIOSIS
- 13. TREATMENT OF ENDOMETRIOSIS Management of pain – Surgery – Medical therapy •Treatment of infertility – Surgery
- 14. MANAGEMENT OF PAIN Surgical treatment – Ablation of endometrial implants – Lysis of adhesions – Ablation
- 15. LOCALIZATION on or under the ovaries behind the uterus on the tissues that hold the uterus
- 16. PROPHYLAXIS Research suggests that frequent and early pregnancy, use of oral contraceptives, and daily exercise may
- 17. TRAUMATIC AND ABNORMALITIES OF FEMALE GENITAL ORGAN
- 18. UTERINE ABNORMALITIES double vagina, double cervix and double uterus single vagina, single cervix and double single-horned
- 19. INVESTIGATIONS Ultrasound Hysterosalpingography, which allows evaluation of the uterine cavity and tubal patency. MRI scan, which
- 20. MANAGEMENT Decision for surgical intervention will depend on the effect of the abnormality on enabling a
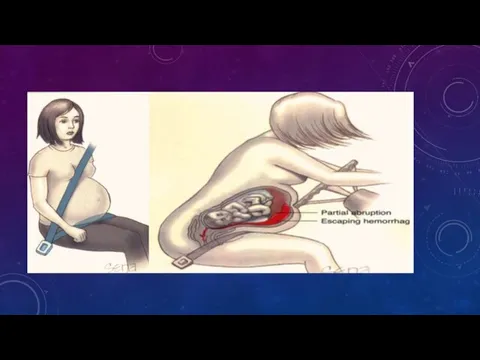
- 21. GENITAL TRAUMATIC A _ Obstetric Trauma Uterus (Blunt & Penetration) Genital Tract (delivery trauma) B _
- 23. DELIVERY TRAUMA Lacerations of the birth canal Raptures Hematomas Injuries to the cervix Vaginal laceration
- 24. GENITAL TRACT TRAUMA ?FOREIGN BODY ?SEXUAL ASSULT ?HEMATOMA
- 26. Скачать презентацию
Endometriosis is a disease in which endometrial glands and stroma implant
Endometriosis is a disease in which endometrial glands and stroma implant
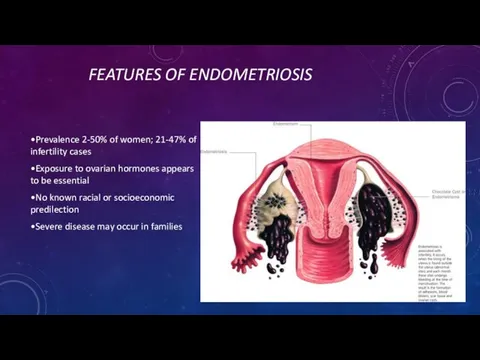
FEATURES OF ENDOMETRIOSIS
•Prevalence 2-50% of women; 21-47% of infertility cases
•Exposure to
FEATURES OF ENDOMETRIOSIS
•Prevalence 2-50% of women; 21-47% of infertility cases
•Exposure to
IS ENDOMETRIOSIS INCREASING?
•1965-1984, endometriosis rose from 10 to 19% as primary
IS ENDOMETRIOSIS INCREASING?
•1965-1984, endometriosis rose from 10 to 19% as primary
ETIOLOGIES OF ENDOMETRIOSIS
•Sampson's theory: Retrograde menses and peritoneal implantation
–Most women retrograde
ETIOLOGIES OF ENDOMETRIOSIS
•Sampson's theory: Retrograde menses and peritoneal implantation
–Most women retrograde
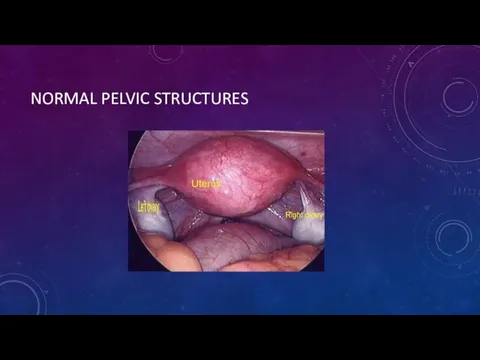
NORMAL PELVIC STRUCTURES
NORMAL PELVIC STRUCTURES
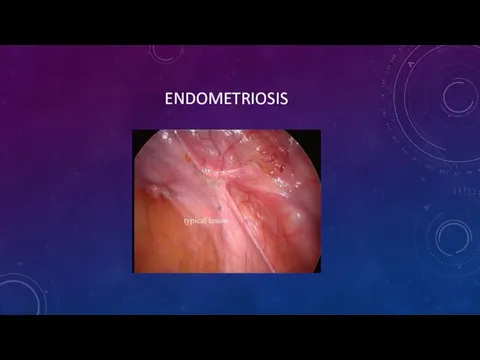
ENDOMETRIOSIS
ENDOMETRIOSIS
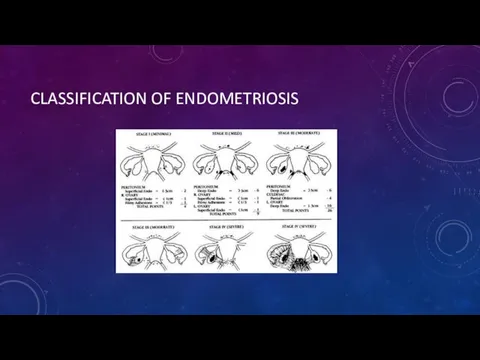
CLASSIFICATION OF ENDOMETRIOSIS
CLASSIFICATION OF ENDOMETRIOSIS

CLINICAL PRESENTATION
Pelvic pain
•Infertility
•Pelvic mass
CLINICAL PRESENTATION
Pelvic pain
•Infertility
•Pelvic mass
PHYSICAL FINDINGS
Tender nodules along the uterosacral ligaments or in the cul-de-sac,
PHYSICAL FINDINGS
Tender nodules along the uterosacral ligaments or in the cul-de-sac,
DIAGNOSIS OF ENDOMETRIOSIS
Diagnosis of Endometriosis
•Direct visualization of implants
– Laparoscopically
– Conscious pain
DIAGNOSIS OF ENDOMETRIOSIS
Diagnosis of Endometriosis
•Direct visualization of implants
– Laparoscopically
– Conscious pain

ENDOMETRIOSIS
ENDOMETRIOSIS
TREATMENT OF ENDOMETRIOSIS
Management of pain
– Surgery
– Medical therapy
•Treatment of infertility
– Surgery
–
TREATMENT OF ENDOMETRIOSIS
Management of pain
– Surgery
– Medical therapy
•Treatment of infertility
– Surgery
–
MANAGEMENT OF PAIN
Surgical treatment
– Ablation of endometrial implants
– Lysis of adhesions
MANAGEMENT OF PAIN
Surgical treatment
– Ablation of endometrial implants
– Lysis of adhesions
LOCALIZATION
on or under the ovaries
behind the uterus
on the tissues that
LOCALIZATION
on or under the ovaries
behind the uterus
on the tissues that
PROPHYLAXIS
Research suggests that frequent and early pregnancy, use of oral
PROPHYLAXIS
Research suggests that frequent and early pregnancy, use of oral
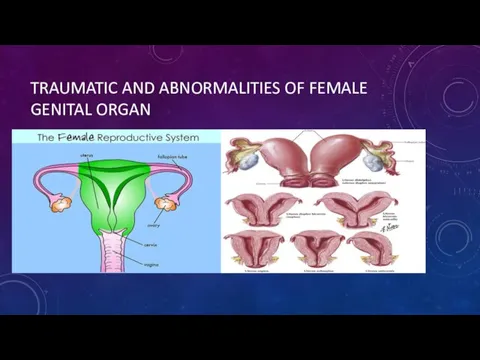
TRAUMATIC AND ABNORMALITIES OF FEMALE GENITAL ORGAN
TRAUMATIC AND ABNORMALITIES OF FEMALE GENITAL ORGAN
UTERINE ABNORMALITIES
double vagina, double cervix and double uterus
single vagina, single cervix
UTERINE ABNORMALITIES
double vagina, double cervix and double uterus
single vagina, single cervix
INVESTIGATIONS
Ultrasound
Hysterosalpingography, which allows evaluation of the uterine cavity and tubal patency.
MRI
INVESTIGATIONS
Ultrasound
Hysterosalpingography, which allows evaluation of the uterine cavity and tubal patency.
MRI
MANAGEMENT
Decision for surgical intervention will depend on the effect of the
MANAGEMENT
Decision for surgical intervention will depend on the effect of the
GENITAL TRAUMATIC
A _ Obstetric Trauma
Uterus (Blunt & Penetration)
Genital Tract
GENITAL TRAUMATIC
A _ Obstetric Trauma
Uterus (Blunt & Penetration)
Genital Tract
DELIVERY TRAUMA
Lacerations of the birth canal
Raptures
Hematomas
Injuries to
DELIVERY TRAUMA
Lacerations of the birth canal
Raptures
Hematomas
Injuries to

GENITAL TRACT TRAUMA
?FOREIGN BODY
?SEXUAL ASSULT
?HEMATOMA
GENITAL TRACT TRAUMA
?FOREIGN BODY
?SEXUAL ASSULT
?HEMATOMA
 Хирургическое лечение переломов костей голени
Хирургическое лечение переломов костей голени Физиология возбуждимых тканей
Физиология возбуждимых тканей Гипертонический криз
Гипертонический криз Строение органов дыхания у новорожденных и детей
Строение органов дыхания у новорожденных и детей Жүкті әйелдерді амбулаториялық жағдайда жүргізу
Жүкті әйелдерді амбулаториялық жағдайда жүргізу Особености травматологии детского возраста
Особености травматологии детского возраста Эмбриогенез, анатомо-физиологические особенности почек и мочевыделительной системы у детей
Эмбриогенез, анатомо-физиологические особенности почек и мочевыделительной системы у детей Special issues. Guidelines for the use of antiretroviral agents in adults and adolescents
Special issues. Guidelines for the use of antiretroviral agents in adults and adolescents Здоровье и болезнь. Факторы, определяющие здоровье. Методика сбора анамнеза. Периоды детского возраста. Оценка здоровья
Здоровье и болезнь. Факторы, определяющие здоровье. Методика сбора анамнеза. Периоды детского возраста. Оценка здоровья Физиология боли
Физиология боли ИБС. Стенокардия. Инфаркт миокарда
ИБС. Стенокардия. Инфаркт миокарда Основы травматологии и ортопедии
Основы травматологии и ортопедии Пародонтоз. Идиопатические заболевания пародонта
Пародонтоз. Идиопатические заболевания пародонта Filling’s material: permanent & temporary
Filling’s material: permanent & temporary Симптомы и методы обследования в урологии
Симптомы и методы обследования в урологии Организация гинекологической помощи детям
Организация гинекологической помощи детям Введение в медицинскую рецептуру
Введение в медицинскую рецептуру Опухоли головного и спинного мозга
Опухоли головного и спинного мозга Аборты. О вреде абортов
Аборты. О вреде абортов Эмоциональные расстройства
Эмоциональные расстройства Гепатит В
Гепатит В Общая фармакология. Фармакодинамика
Общая фармакология. Фармакодинамика Информатизация медицины
Информатизация медицины Методы иммунодиагностики и иммунопрофилактики инфекционных болезней
Методы иммунодиагностики и иммунопрофилактики инфекционных болезней Қабыну ауруларының асқынулары. Сепсис
Қабыну ауруларының асқынулары. Сепсис Дифференциальная диагностика абдоминального болевого синдрома у детей
Дифференциальная диагностика абдоминального болевого синдрома у детей Чума. Симптомы. Клиника. Лечение
Чума. Симптомы. Клиника. Лечение Мұрынның артқы тампонадасы
Мұрынның артқы тампонадасы