- Guidelines for the use of antiretroviral agents in adults and adolescents

Содержание
- 2. These slides were developed using the April 2015 treatment guidelines and were updated in July 2016.
- 3. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults & Adolescents Developed by the Department
- 4. Guidelines Outline Overview Initiation of Antiretroviral Therapy (ART) Management of the Treatment-Experienced Patient Special Issues
- 5. What the Guidelines Address Baseline evaluation Laboratory testing (HIV RNA, CD4 cell count, resistance) When to
- 6. What the Guidelines Address (2) Treatment of acute HIV infection Special considerations in adolescents, pregnant women,
- 7. Websites to Access the Guidelines http://aidsinfo.nih.gov http://www.aidsetc.org
- 8. Goals of Treatment Reduce HIV-related morbidity; prolong duration and quality of survival Restore and/or preserve immunologic
- 9. Tools to Achieve Treatment Goals Selection of ARV regimen Maximizing adherence Pretreatment resistance testing
- 10. Improving Adherence Support and reinforcement Simplified dosing strategies Reminders, alarms, timers, and pillboxes Ongoing patient education
- 11. CD4 Count Monitoring CD4 count The major indicator of immune function Most recent CD4 count is
- 12. CD4 Count Monitoring (2) CD4 monitoring Check at baseline (x2) and at least every 3-6 months
- 13. HIV RNA Monitoring HIV RNA May influence decision to start ART and help determine frequency of
- 14. HIV RNA Monitoring (2) RNA monitoring Check at baseline (x2) Monitoring in those not on ART
- 15. Testing for Drug Resistance Before initiation of ART: Transmitted resistance in 10-17% of HIV-infected patients In
- 16. Drug Resistance Testing: Recommendations
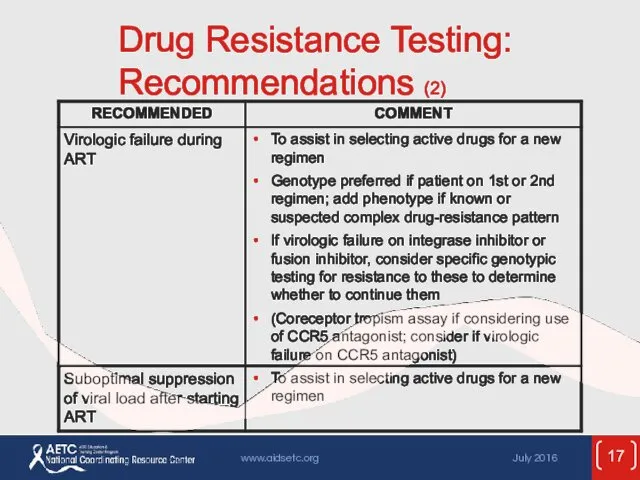
- 17. Drug Resistance Testing: Recommendations (2)
- 18. Drug Resistance Testing: Recommendations (3)
- 19. Drug Resistance Testing: Recommendations (4)
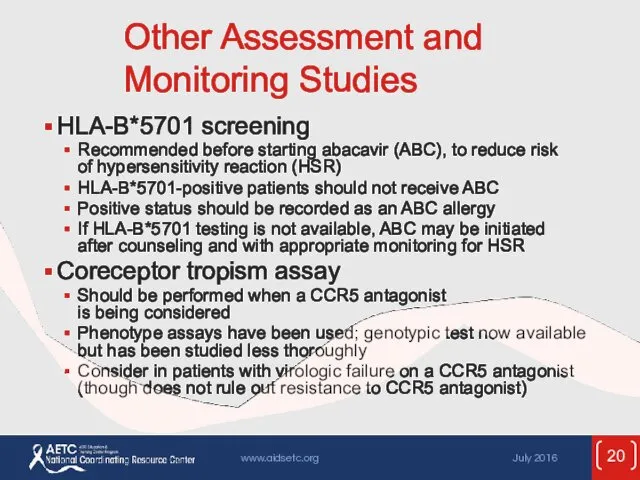
- 20. Other Assessment and Monitoring Studies HLA-B*5701 screening Recommended before starting abacavir (ABC), to reduce risk of
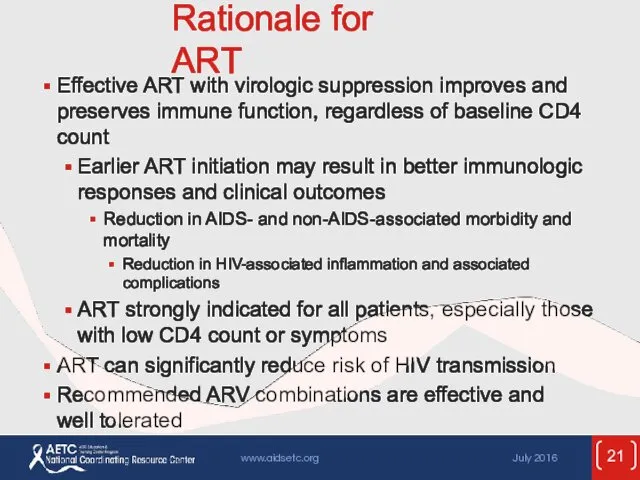
- 21. Rationale for ART Effective ART with virologic suppression improves and preserves immune function, regardless of baseline
- 22. When to Start ART Evidence supports starting at high CD4 counts Current recommendation: ART is strongly
- 23. Rating Scheme for Recommendations Strength of recommendation: A: Strong B: Moderate C: Optional Quality of evidence:
- 24. Recommendations for Initiating ART ART is recommended for treatment: “ART is recommended for all HIV-infected individuals,
- 25. Recommendations for Initiating ART (2) ART is recommended for prevention: “ART also is recommended for HIV-infected
- 26. Recommendations for Initiating ART: Considerations
- 27. Potential Benefits of Early Therapy Untreated HIV is associated with development of AIDS and non-AIDS-defining conditions.
- 28. Potential Benefits of Early Therapy (2) Potential decrease in risk of many complications, including: HIV-associated nephropathy
- 29. Potential Benefits of Early Therapy (3) Prevention of sexual transmission of HIV Prevention of perinatal transmission
- 30. Consider More-Rapid Initiation of ART Pregnancy AIDS-defining condition Acute opportunistic infection Lower CD4 count (eg, Acute/early
- 31. Considerations When Starting ART It is crucial to support adherence and retention in care Mental illness,
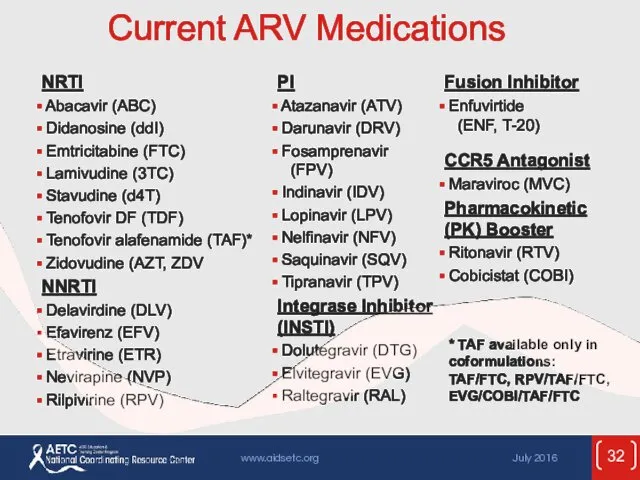
- 32. Current ARV Medications * TAF available only in coformulations: TAF/FTC, RPV/TAF/FTC, EVG/COBI/TAF/FTC
- 33. Initial ART Regimens: DHHS Categories Recommended Easy to use Durable virologic efficacy Favorable tolerability and toxicity
- 34. Initial Treatment: Choosing Regimens 3 main categories: 1 INSTI + 2 NRTIs 1 PK-boosted PI +
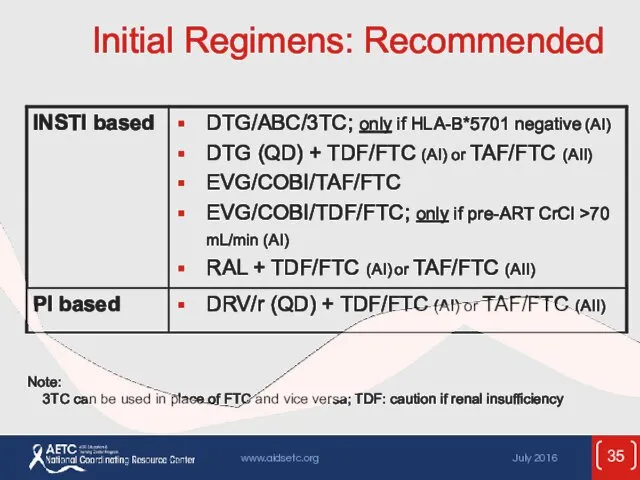
- 35. Initial Regimens: Recommended Note: 3TC can be used in place of FTC and vice versa; TDF:
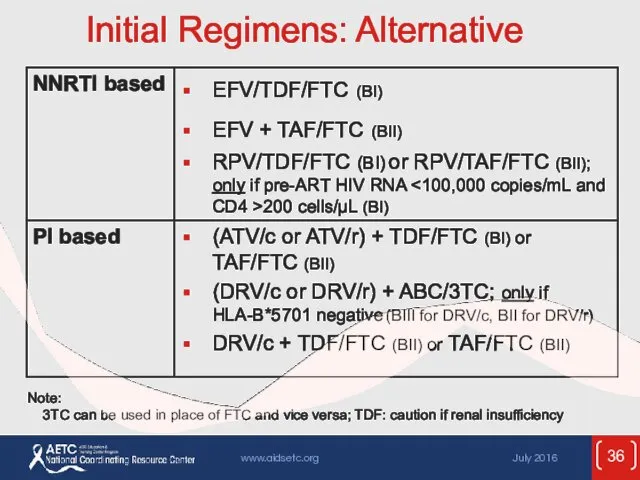
- 36. Initial Regimens: Alternative Note: 3TC can be used in place of FTC and vice versa; TDF:
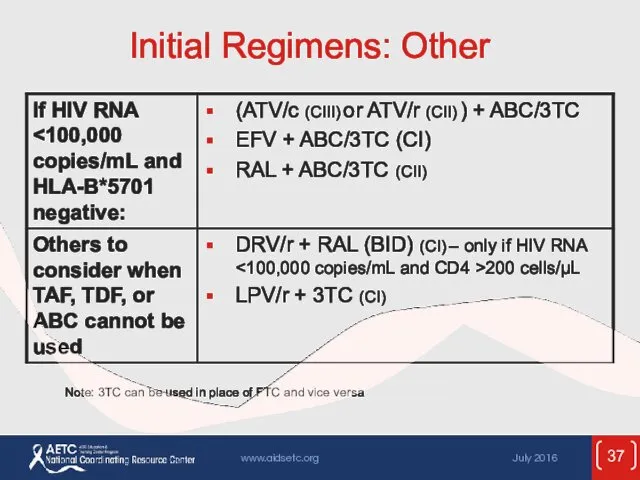
- 37. Initial Regimens: Other Note: 3TC can be used in place of FTC and vice versa
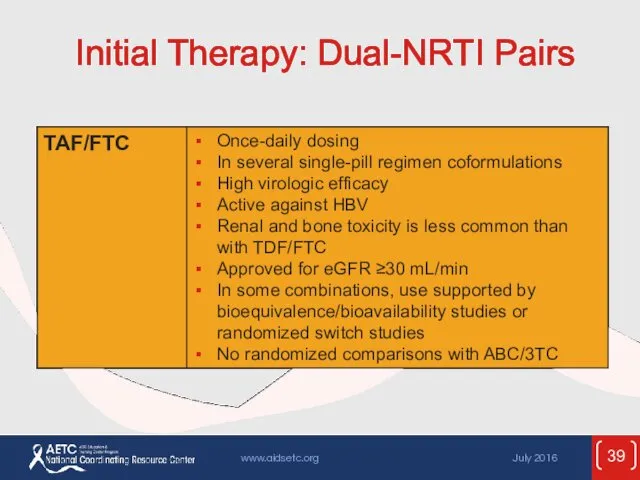
- 38. Initial Therapy: Dual-NRTI Pairs
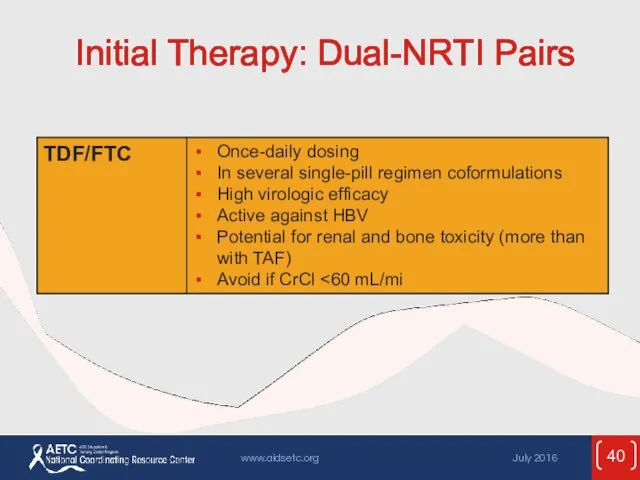
- 39. Initial Therapy: Dual-NRTI Pairs
- 40. Initial Therapy: Dual-NRTI Pairs
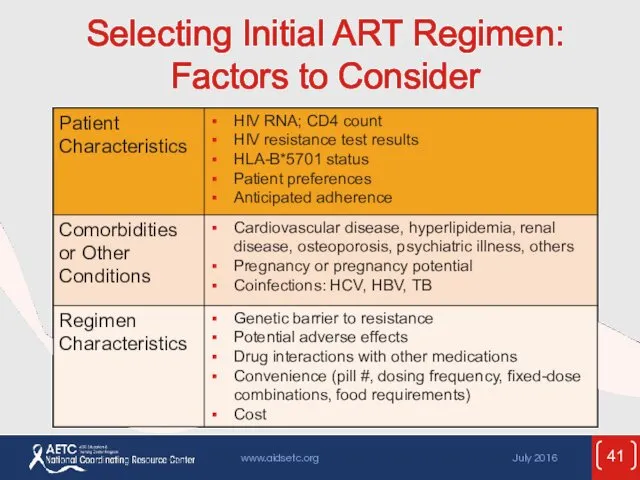
- 41. Selecting Initial ART Regimen: Factors to Consider
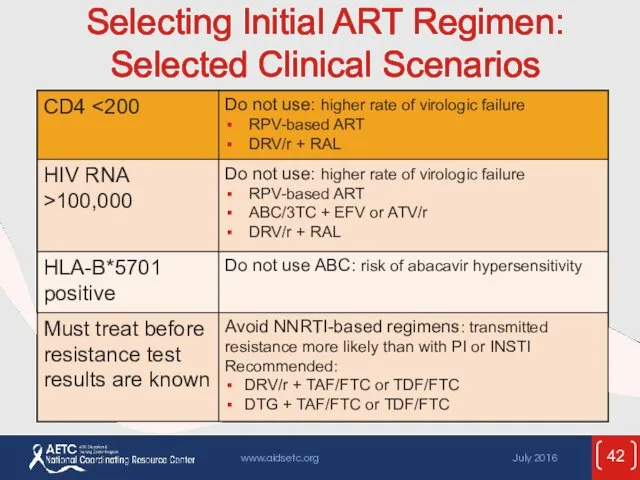
- 42. Selecting Initial ART Regimen: Selected Clinical Scenarios
- 43. Selecting Initial ART Regimen: Selected Clinical Scenarios (2)
- 44. Selecting Initial ART Regimen: Selected Clinical Scenarios (3)
- 45. Selecting Initial ART Regimen: Selected Clinical Scenarios (4)
- 46. Selecting Initial ART Regimen: Selected Clinical Scenarios (5)
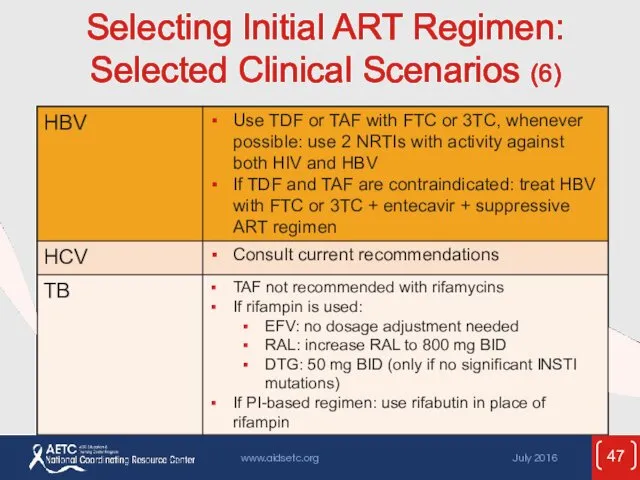
- 47. Selecting Initial ART Regimen: Selected Clinical Scenarios (6)
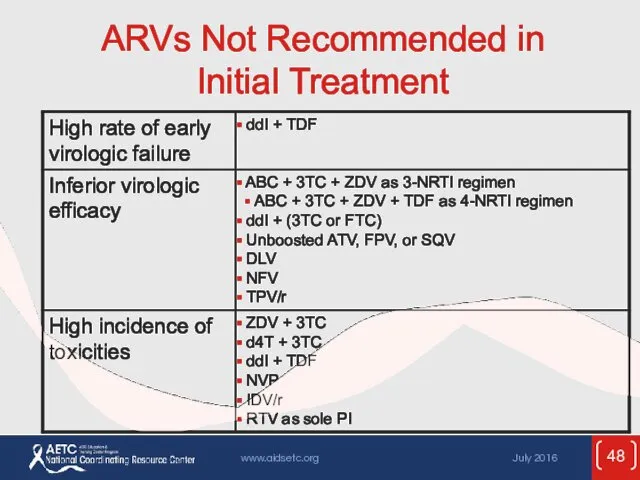
- 48. ARVs Not Recommended in Initial Treatment
- 49. ARVs Not Recommended in Initial Treatment (2)
- 50. ARV Medications: Should Not Be Offered at Any Time ARV regimens not recommended: Monotherapy with NRTI*
- 51. ARV Medications: Should Not Be Offered at Any Time (2) ARV components not recommended: ddI +
- 52. ARV Medications: Should Not Be Offered at Any Time (3) ARV components not recommended: EFV during
- 53. ARV Components in Initial Therapy: Dual-NRTI Pairs ADVANTAGES Established backbone of combination therapy Minimal drug interactions
- 54. ARV Components in Initial Therapy: INSTIs ADVANTAGES Virologic response noninferior to EFV Fewer adverse events than
- 55. ARV Components in Initial Therapy: PIs ADVANTAGES Higher genetic barrier to resistance PI resistance uncommon with
- 56. ARV Components in Initial Therapy: NNRTIs ADVANTAGES Long half-lives Less metabolic toxicity (dyslipidemia, insulin resistance) than
- 57. Adverse Effects Important to anticipate and overcome ART toxicities in order to achieve ART success over
- 58. Adverse Effects: NRTIs All NRTIs: Lactic acidosis and hepatic steatosis (highest incidence with d4T, then ddI
- 59. Adverse Effects: NRTIs (2) Emtricitabine (FTC) Minimal toxicity Hyperpigmentation In HBV coinfection, exacerbation of HBV if
- 60. Adverse Effects: NRTIs (3) Abacavir (ABC) Hypersensitivity reaction* Rash Possible increased risk of MI Tenofovir alafenamide
- 61. Adverse Effects: NRTIs (4) Didanosine (ddI) GI intolerance Peripheral neuropathy Possible increased risk of MI Pancreatitis
- 62. Adverse Effects: INSTIs All INSTIs: Rash, hypersensitivity reaction Depression and suicidal ideation (rare; usually in patients
- 63. Adverse Effects: INSTIs (2) Dolutegravir (DTG) Headache Insomnia Elvitegravir/cobicistat (EVG/c) Decreased CrCl Increased risk of TDF-related
- 64. Adverse Effects: PIs All PIs: Hyperlipidemia Lipodystrophy Hepatotoxicity GI intolerance Possibility of increased bleeding risk for
- 65. Adverse Effects: PIs (2) Atazanavir (ATV) Hyperbilirubinemia PR prolongation Nephrolithiasis, cholelithiasis Darunavir (DRV) Rash Liver toxicity
- 66. Adverse Effects: PIs (3) Indinavir (IDV) Nephrolithiasis GI intolerance Diabetes/insulin resistance Lopinavir/ritonavir (LPV/r) GI intolerance Diabetes/insulin
- 67. Adverse Effects: PIs (4) Saquinavir (SQV) GI intolerance PR and QT prolongation Tipranavir (TPV) GI intolerance
- 68. Adverse Effects: Pharmacokinetic Boosters Ritonavir (RTV, /r) GI intolerance Hyperlipidemia, hyperglycemia Hepatitis Cobicistat (COBI, /c) GI
- 69. Adverse Effects: NNRTIs All NNRTIs: Rash, including Stevens-Johnson syndrome Hepatotoxicity (especially NVP) Drug-drug interactions
- 70. Adverse Effects: NNRTIs (2) Efavirenz (EFV) Neuropsychiatric Teratogenic in nonhuman primates + cases of neural tube
- 71. Adverse Effects: CCR5 Antagonist Maraviroc (MVC) Drug-drug interactions Rash Abdominal pain Upper respiratory tract infections Cough
- 72. Adverse Effects: Fusion Inhibitor Enfuvirtide (ENF, T-20) Injection-site reactions HSR Increased risk of bacterial pneumonia
- 73. Treatment-Experienced Patients The recommended ARV regimens should suppress HIV to below the lower level of detection
- 74. Treatment-Experienced Patients: Virologic Failure, Definitions Virologic suppression: Confirmed HIV RNA below LLOD (eg, Virologic failure: Inability
- 75. Treatment-Experienced Patients: Virologic Failure (2) Failure of current first-line regimens usually caused by suboptimal adherence or
- 76. Treatment-Experienced Patients: Causes of Virologic Failure Patient factors Higher pretreatment HIV RNA (depending on the ART
- 77. Treatment-Experienced Patients: Causes of Virologic Failure (2) ARV regimen factors Toxicity and adverse effects Pharmacokinetic problems
- 78. Treatment-Experienced Patients: Management of Virologic Failure Carefully assess causes of virologic failure; management will vary according
- 79. Treatment-Experienced Patients: Management of Virologic Failure (2) Goal of treatment: to establish virologic suppression (HIV RNA
- 80. Treatment-Experienced Patients: Management of Virologic Failure (3) New regimen should contain at least 2 (preferably 3)
- 81. Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression Morbidity and mortality are higher in HIV-infected
- 82. Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression (2) Poor CD4 recovery Persistently low CD4
- 83. Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression (3) Management: Evaluate for underlying causes (eg,
- 84. Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression (4) Persistent immune activation and inflammation Systemic
- 85. Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression (5) Causes of persistent immune activation not
- 86. Regimen Switching in Setting of Virologic Suppression Changing a suppressive ARV regimen to: Reduce pill burden
- 87. Regimen Switching in Setting of Virologic Suppression (2) Principles (cont.) Absent drug resistance, switching from a
- 88. Regimen Switching in Setting of Virologic Suppression (3) Principles: Maintain viral suppression and avoid jeopardizing future
- 89. Regimen Switching in Setting of Virologic Suppression (4) Specific considerations Within-class switches: Usually maintain viral suppression
- 90. Regimen Switching in Setting of Virologic Suppression (5) Switch strategies not recommended: RTV-boosted PI monotherapy Less
- 91. Regimen Switching in Setting of Virologic Suppression (6) Closely monitor tolerability, viral suppression, adherence, and toxicity
- 92. Websites to Access the Guidelines http://www.aidsetc.org http://aidsinfo.nih.gov
- 94. Скачать презентацию
These slides were developed using the April 2015 treatment guidelines and
These slides were developed using the April 2015 treatment guidelines and
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults &
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults &
Guidelines Outline
Overview
Initiation of Antiretroviral Therapy (ART)
Management of the Treatment-Experienced Patient
Special Issues
Guidelines Outline
Overview
Initiation of Antiretroviral Therapy (ART)
Management of the Treatment-Experienced Patient
Special Issues
What the Guidelines Address
Baseline evaluation
Laboratory testing (HIV RNA, CD4 cell count,
What the Guidelines Address
Baseline evaluation
Laboratory testing (HIV RNA, CD4 cell count,
What the Guidelines Address (2)
Treatment of acute HIV infection
Special considerations in
What the Guidelines Address (2)
Treatment of acute HIV infection
Special considerations in
Websites to Access the Guidelines
http://aidsinfo.nih.gov
http://www.aidsetc.org
Websites to Access the Guidelines
http://aidsinfo.nih.gov
http://www.aidsetc.org
Goals of Treatment
Reduce HIV-related morbidity; prolong duration and quality of survival
Restore
Goals of Treatment
Reduce HIV-related morbidity; prolong duration and quality of survival
Restore
Tools to Achieve Treatment Goals
Selection of ARV regimen
Maximizing adherence
Pretreatment resistance testing
Tools to Achieve Treatment Goals
Selection of ARV regimen
Maximizing adherence
Pretreatment resistance testing
Improving Adherence
Support and reinforcement
Simplified dosing strategies
Reminders, alarms, timers, and pillboxes
Ongoing patient
Improving Adherence
Support and reinforcement
Simplified dosing strategies
Reminders, alarms, timers, and pillboxes
Ongoing patient
CD4 Count Monitoring
CD4 count
The major indicator of immune function
Most recent
CD4 Count Monitoring
CD4 count
The major indicator of immune function
Most recent
CD4 Count Monitoring (2)
CD4 monitoring
Check at baseline (x2) and at least
CD4 Count Monitoring (2)
CD4 monitoring
Check at baseline (x2) and at least
HIV RNA Monitoring
HIV RNA
May influence decision to start ART and help
HIV RNA Monitoring
HIV RNA
May influence decision to start ART and help
HIV RNA Monitoring (2)
RNA monitoring
Check at baseline (x2)
Monitoring in those
HIV RNA Monitoring (2)
RNA monitoring
Check at baseline (x2)
Monitoring in those
Testing for Drug Resistance
Before initiation of ART:
Transmitted resistance in 10-17% of
Testing for Drug Resistance
Before initiation of ART:
Transmitted resistance in 10-17% of
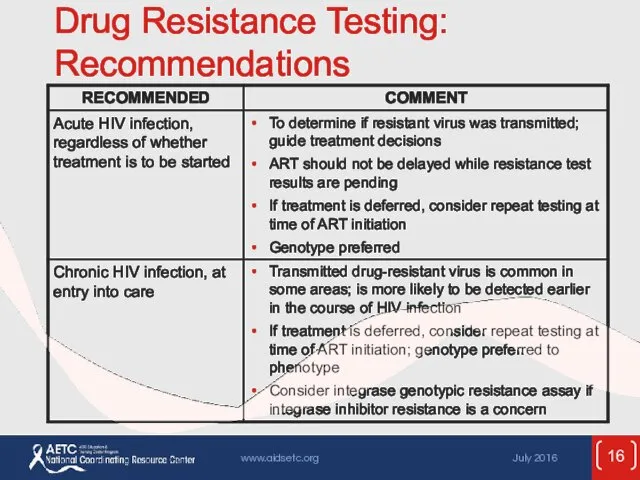
Drug Resistance Testing: Recommendations
Drug Resistance Testing: Recommendations
Drug Resistance Testing: Recommendations (2)
Drug Resistance Testing: Recommendations (2)
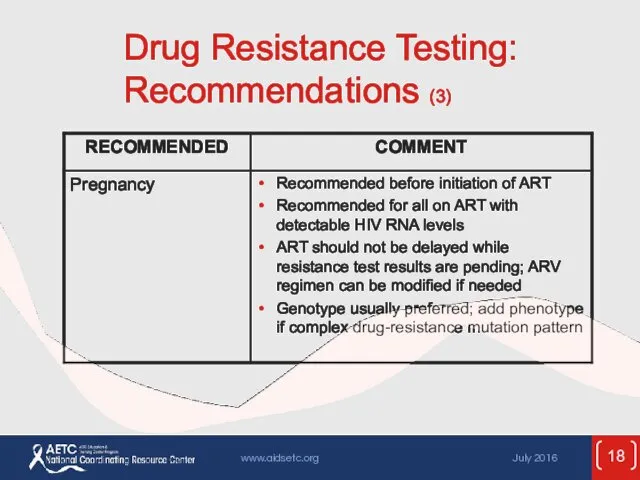
Drug Resistance Testing: Recommendations (3)
Drug Resistance Testing: Recommendations (3)
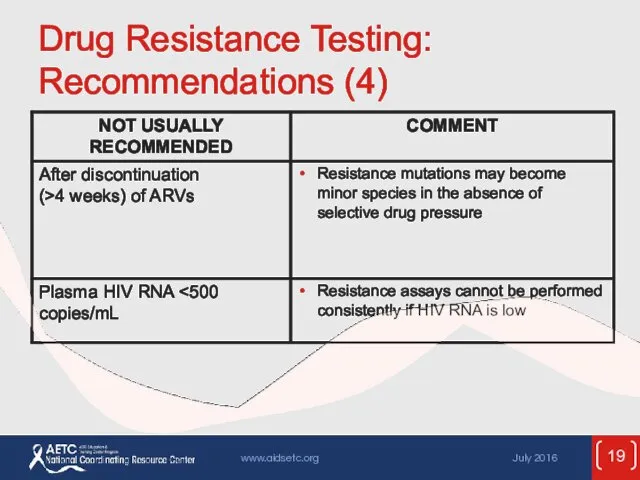
Drug Resistance Testing: Recommendations (4)
Drug Resistance Testing: Recommendations (4)
Other Assessment and
Monitoring Studies
HLA-B*5701 screening
Recommended before starting abacavir (ABC), to reduce
Other Assessment and
Monitoring Studies
HLA-B*5701 screening
Recommended before starting abacavir (ABC), to reduce
Rationale for ART
Effective ART with virologic suppression improves and preserves immune
Rationale for ART
Effective ART with virologic suppression improves and preserves immune
When to Start ART
Evidence supports starting at high CD4 counts
Current recommendation:
When to Start ART
Evidence supports starting at high CD4 counts
Current recommendation:
Rating Scheme for Recommendations
Strength of recommendation:
A: Strong
B: Moderate
C: Optional
Quality
Rating Scheme for Recommendations
Strength of recommendation:
A: Strong
B: Moderate
C: Optional
Quality
Recommendations for Initiating ART
ART is recommended for treatment:
“ART is recommended
Recommendations for Initiating ART
ART is recommended for treatment:
“ART is recommended
Recommendations for Initiating ART (2)
ART is recommended for prevention:
“ART also
Recommendations for Initiating ART (2)
ART is recommended for prevention:
“ART also
Recommendations for Initiating ART: Considerations
Recommendations for Initiating ART: Considerations
Potential Benefits of Early Therapy
Untreated HIV is associated with development
Potential Benefits of Early Therapy
Untreated HIV is associated with development
Potential Benefits of Early Therapy (2)
Potential decrease in risk of many
Potential Benefits of Early Therapy (2)
Potential decrease in risk of many

Potential Benefits of Early Therapy (3)
Prevention of sexual transmission of HIV
Prevention
Potential Benefits of Early Therapy (3)
Prevention of sexual transmission of HIV
Prevention
Consider More-Rapid Initiation of ART
Pregnancy
AIDS-defining condition
Acute opportunistic infection
Lower CD4 count
Consider More-Rapid Initiation of ART
Pregnancy
AIDS-defining condition
Acute opportunistic infection
Lower CD4 count
Considerations When Starting ART
It is crucial to support adherence and retention
Considerations When Starting ART
It is crucial to support adherence and retention
Current ARV Medications
* TAF available only in coformulations:
TAF/FTC, RPV/TAF/FTC,
EVG/COBI/TAF/FTC
Current ARV Medications
* TAF available only in coformulations:
TAF/FTC, RPV/TAF/FTC,
EVG/COBI/TAF/FTC
Initial ART Regimens: DHHS Categories
Recommended
Easy to use
Durable virologic efficacy
Favorable tolerability
Initial ART Regimens: DHHS Categories
Recommended
Easy to use
Durable virologic efficacy
Favorable tolerability
Initial Treatment: Choosing Regimens
3 main categories:
1 INSTI + 2 NRTIs
1 PK-boosted
Initial Treatment: Choosing Regimens
3 main categories:
1 INSTI + 2 NRTIs
1 PK-boosted
Initial Regimens: Recommended
Note:
3TC can be used in place
Initial Regimens: Recommended
Note:
3TC can be used in place
Initial Regimens: Alternative
Note:
3TC can be used in place of
Initial Regimens: Alternative
Note:
3TC can be used in place of
Initial Regimens: Other
Note: 3TC can be used in place of FTC
Initial Regimens: Other
Note: 3TC can be used in place of FTC
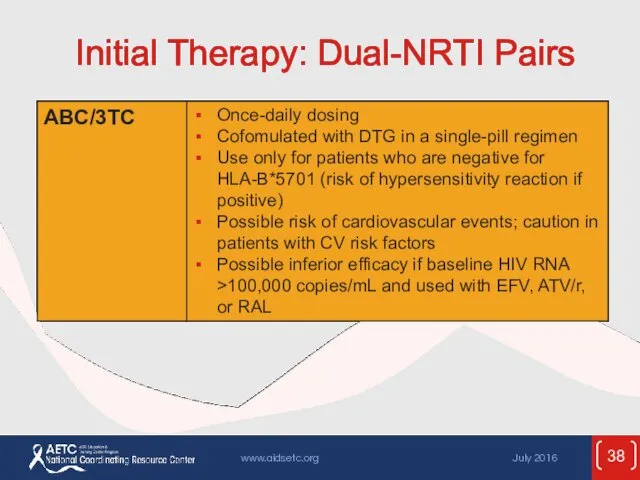
Initial Therapy: Dual-NRTI Pairs
Initial Therapy: Dual-NRTI Pairs
Initial Therapy: Dual-NRTI Pairs
Initial Therapy: Dual-NRTI Pairs
Initial Therapy: Dual-NRTI Pairs
Initial Therapy: Dual-NRTI Pairs
Selecting Initial ART Regimen: Factors to Consider
Selecting Initial ART Regimen: Factors to Consider
Selecting Initial ART Regimen: Selected Clinical Scenarios
Selecting Initial ART Regimen: Selected Clinical Scenarios
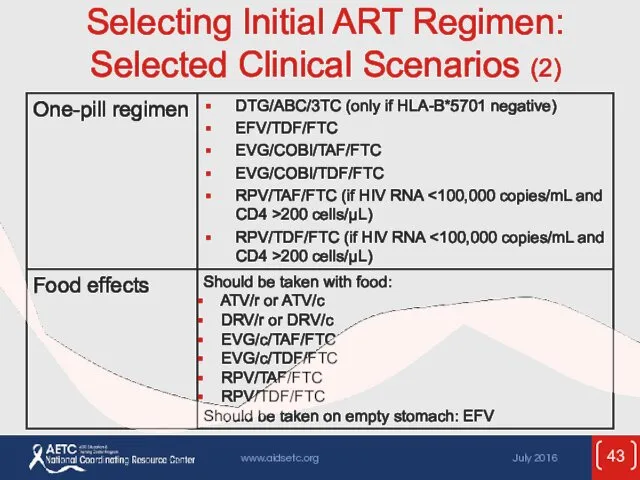
Selecting Initial ART Regimen: Selected Clinical Scenarios (2)
Selecting Initial ART Regimen: Selected Clinical Scenarios (2)
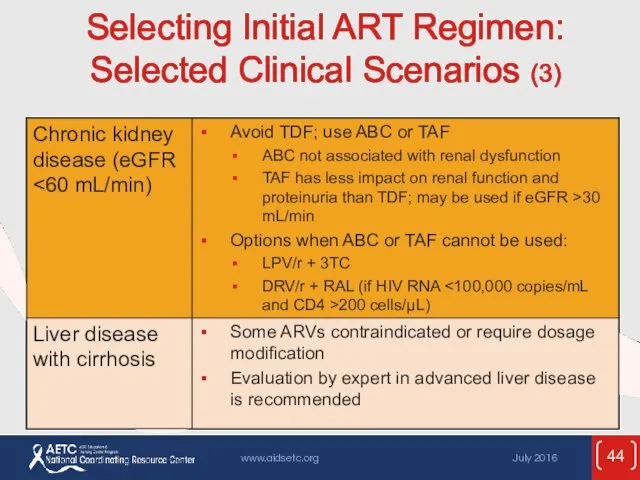
Selecting Initial ART Regimen: Selected Clinical Scenarios (3)
Selecting Initial ART Regimen: Selected Clinical Scenarios (3)
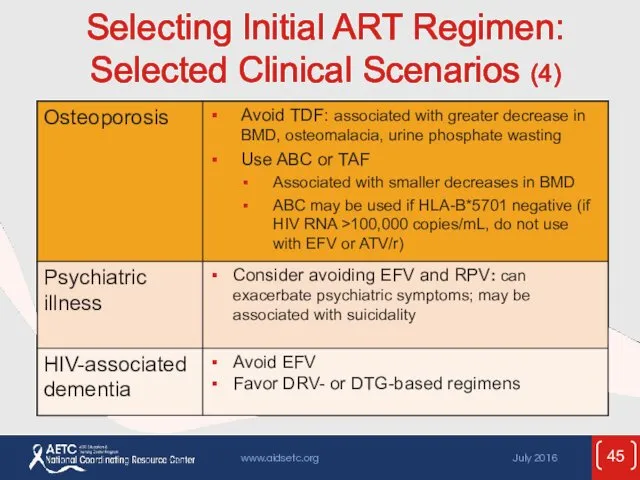
Selecting Initial ART Regimen: Selected Clinical Scenarios (4)
Selecting Initial ART Regimen: Selected Clinical Scenarios (4)
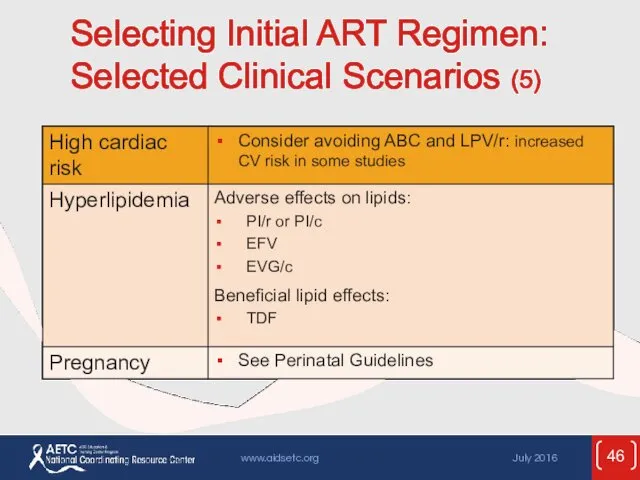
Selecting Initial ART Regimen: Selected Clinical Scenarios (5)
Selecting Initial ART Regimen: Selected Clinical Scenarios (5)
Selecting Initial ART Regimen: Selected Clinical Scenarios (6)
Selecting Initial ART Regimen: Selected Clinical Scenarios (6)
ARVs Not Recommended in
Initial Treatment
ARVs Not Recommended in
Initial Treatment

ARVs Not Recommended in
Initial Treatment (2)
ARVs Not Recommended in
Initial Treatment (2)
ARV Medications: Should Not Be Offered at Any Time
ARV regimens not
ARV Medications: Should Not Be Offered at Any Time
ARV regimens not

ARV Medications: Should Not Be Offered at Any Time (2)
ARV components
ARV Medications: Should Not Be Offered at Any Time (2)
ARV components
ARV Medications: Should Not Be Offered at Any Time (3)
ARV components
ARV Medications: Should Not Be Offered at Any Time (3)
ARV components
ARV Components in Initial Therapy: Dual-NRTI Pairs
ADVANTAGES
Established backbone of combination therapy
Minimal
ARV Components in Initial Therapy: Dual-NRTI Pairs
ADVANTAGES
Established backbone of combination therapy
Minimal
ARV Components in Initial Therapy: INSTIs
ADVANTAGES
Virologic response noninferior to EFV
Fewer adverse
ARV Components in Initial Therapy: INSTIs
ADVANTAGES
Virologic response noninferior to EFV
Fewer adverse
ARV Components in Initial Therapy: PIs
ADVANTAGES
Higher genetic barrier to resistance
PI
ARV Components in Initial Therapy: PIs
ADVANTAGES
Higher genetic barrier to resistance
PI
ARV Components in Initial Therapy: NNRTIs
ADVANTAGES
Long half-lives
Less metabolic toxicity (dyslipidemia,
ARV Components in Initial Therapy: NNRTIs
ADVANTAGES
Long half-lives
Less metabolic toxicity (dyslipidemia,
Adverse Effects
Important to anticipate and overcome ART toxicities in order to
Adverse Effects
Important to anticipate and overcome ART toxicities in order to
Adverse Effects: NRTIs
All NRTIs:
Lactic acidosis and hepatic steatosis (highest incidence
Adverse Effects: NRTIs
All NRTIs:
Lactic acidosis and hepatic steatosis (highest incidence
Adverse Effects: NRTIs (2)
Emtricitabine (FTC)
Minimal toxicity
Hyperpigmentation
In HBV coinfection, exacerbation of
Adverse Effects: NRTIs (2)
Emtricitabine (FTC)
Minimal toxicity
Hyperpigmentation
In HBV coinfection, exacerbation of
Adverse Effects: NRTIs (3)
Abacavir (ABC)
Hypersensitivity reaction*
Rash
Possible increased risk of MI
Tenofovir alafenamide
Adverse Effects: NRTIs (3)
Abacavir (ABC)
Hypersensitivity reaction*
Rash
Possible increased risk of MI
Tenofovir alafenamide
Adverse Effects: NRTIs (4)
Didanosine (ddI)
GI intolerance
Peripheral neuropathy
Possible increased risk of
Adverse Effects: NRTIs (4)
Didanosine (ddI)
GI intolerance
Peripheral neuropathy
Possible increased risk of
Adverse Effects: INSTIs
All INSTIs:
Rash, hypersensitivity reaction
Depression and suicidal ideation (rare; usually
Adverse Effects: INSTIs
All INSTIs:
Rash, hypersensitivity reaction
Depression and suicidal ideation (rare; usually
Adverse Effects: INSTIs (2)
Dolutegravir (DTG)
Headache
Insomnia
Elvitegravir/cobicistat (EVG/c)
Decreased CrCl
Increased risk of TDF-related nephrotoxicity
Nausea,
Adverse Effects: INSTIs (2)
Dolutegravir (DTG)
Headache
Insomnia
Elvitegravir/cobicistat (EVG/c)
Decreased CrCl
Increased risk of TDF-related nephrotoxicity
Nausea,
Adverse Effects: PIs
All PIs:
Hyperlipidemia
Lipodystrophy
Hepatotoxicity
GI intolerance
Possibility of increased bleeding
Adverse Effects: PIs
All PIs:
Hyperlipidemia
Lipodystrophy
Hepatotoxicity
GI intolerance
Possibility of increased bleeding
Adverse Effects: PIs (2)
Atazanavir (ATV)
Hyperbilirubinemia
PR prolongation
Nephrolithiasis, cholelithiasis
Darunavir (DRV)
Rash
Liver toxicity
Fosamprenavir (FPV)
GI intolerance
Rash
Possible
Adverse Effects: PIs (2)
Atazanavir (ATV)
Hyperbilirubinemia
PR prolongation
Nephrolithiasis, cholelithiasis
Darunavir (DRV)
Rash
Liver toxicity
Fosamprenavir (FPV)
GI intolerance
Rash
Possible
Adverse Effects: PIs (3)
Indinavir (IDV)
Nephrolithiasis
GI intolerance
Diabetes/insulin resistance
Lopinavir/ritonavir (LPV/r)
GI intolerance
Diabetes/insulin resistance
Possible
Adverse Effects: PIs (3)
Indinavir (IDV)
Nephrolithiasis
GI intolerance
Diabetes/insulin resistance
Lopinavir/ritonavir (LPV/r)
GI intolerance
Diabetes/insulin resistance
Possible
Adverse Effects: PIs (4)
Saquinavir (SQV)
GI intolerance
PR and QT prolongation
Tipranavir (TPV)
GI intolerance
Rash
Hyperlipidemia
Liver
Adverse Effects: PIs (4)
Saquinavir (SQV)
GI intolerance
PR and QT prolongation
Tipranavir (TPV)
GI intolerance
Rash
Hyperlipidemia
Liver
Adverse Effects: Pharmacokinetic Boosters
Ritonavir (RTV, /r)
GI intolerance
Hyperlipidemia, hyperglycemia
Hepatitis
Cobicistat (COBI, /c)
GI intolerance
Increase
Adverse Effects: Pharmacokinetic Boosters
Ritonavir (RTV, /r)
GI intolerance
Hyperlipidemia, hyperglycemia
Hepatitis
Cobicistat (COBI, /c)
GI intolerance
Increase
Adverse Effects: NNRTIs
All NNRTIs:
Rash, including Stevens-Johnson syndrome
Hepatotoxicity (especially NVP)
Drug-drug interactions
Adverse Effects: NNRTIs
All NNRTIs:
Rash, including Stevens-Johnson syndrome
Hepatotoxicity (especially NVP)
Drug-drug interactions
Adverse Effects: NNRTIs (2)
Efavirenz (EFV)
Neuropsychiatric
Teratogenic in nonhuman primates + cases of
Adverse Effects: NNRTIs (2)
Efavirenz (EFV)
Neuropsychiatric
Teratogenic in nonhuman primates + cases of
Adverse Effects: CCR5 Antagonist
Maraviroc (MVC)
Drug-drug interactions
Rash
Abdominal pain
Upper respiratory tract infections
Cough
Hepatotoxicity
Musculoskeletal symptoms
Orthostatic
Adverse Effects: CCR5 Antagonist
Maraviroc (MVC)
Drug-drug interactions
Rash
Abdominal pain
Upper respiratory tract infections
Cough
Hepatotoxicity
Musculoskeletal symptoms
Orthostatic

Adverse Effects: Fusion Inhibitor
Enfuvirtide (ENF, T-20)
Injection-site reactions
HSR
Increased risk of bacterial
Adverse Effects: Fusion Inhibitor
Enfuvirtide (ENF, T-20)
Injection-site reactions
HSR
Increased risk of bacterial
Treatment-Experienced Patients
The recommended ARV regimens should suppress HIV to below the
Treatment-Experienced Patients
The recommended ARV regimens should suppress HIV to below the
Treatment-Experienced Patients: Virologic Failure, Definitions
Virologic suppression:
Confirmed HIV RNA below LLOD (eg,
Treatment-Experienced Patients: Virologic Failure, Definitions
Virologic suppression:
Confirmed HIV RNA below LLOD (eg,
Treatment-Experienced Patients: Virologic Failure (2)
Failure of current first-line regimens usually caused
Treatment-Experienced Patients: Virologic Failure (2)
Failure of current first-line regimens usually caused
Treatment-Experienced Patients: Causes of Virologic Failure
Patient factors
Higher pretreatment HIV RNA
Treatment-Experienced Patients: Causes of Virologic Failure
Patient factors
Higher pretreatment HIV RNA
Treatment-Experienced Patients: Causes of Virologic Failure (2)
ARV regimen factors
Toxicity and adverse
Treatment-Experienced Patients: Causes of Virologic Failure (2)
ARV regimen factors
Toxicity and adverse
Treatment-Experienced Patients: Management of Virologic Failure
Carefully assess causes of virologic failure;
Treatment-Experienced Patients: Management of Virologic Failure
Carefully assess causes of virologic failure;
Treatment-Experienced Patients: Management of Virologic Failure (2)
Goal of treatment: to establish
Treatment-Experienced Patients: Management of Virologic Failure (2)
Goal of treatment: to establish
Treatment-Experienced Patients: Management of Virologic Failure (3)
New regimen should contain at
Treatment-Experienced Patients: Management of Virologic Failure (3)
New regimen should contain at
Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression
Morbidity and mortality
Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression
Morbidity and mortality
Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression (2)
Poor CD4
Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression (2)
Poor CD4
Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression
(3)
Management:
Evaluate for underlying
Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression
(3)
Management:
Evaluate for underlying
Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression (4)
Persistent immune
Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression (4)
Persistent immune
Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression (5)
Causes of
Poor CD4 Recovery and Persistent Inflammation Despite Viral Suppression (5)
Causes of
Regimen Switching in Setting of Virologic Suppression
Changing a suppressive ARV regimen
Regimen Switching in Setting of Virologic Suppression
Changing a suppressive ARV regimen
Regimen Switching in Setting of Virologic Suppression (2)
Principles (cont.)
Absent drug resistance,
Regimen Switching in Setting of Virologic Suppression (2)
Principles (cont.)
Absent drug resistance,
Regimen Switching in Setting of Virologic Suppression (3)
Principles:
Maintain viral suppression and
Regimen Switching in Setting of Virologic Suppression (3)
Principles:
Maintain viral suppression and
Regimen Switching in Setting of Virologic Suppression (4)
Specific considerations
Within-class switches:
Usually maintain
Regimen Switching in Setting of Virologic Suppression (4)
Specific considerations
Within-class switches:
Usually maintain
Regimen Switching in Setting of Virologic Suppression (5)
Switch strategies not recommended:
RTV-boosted
Regimen Switching in Setting of Virologic Suppression (5)
Switch strategies not recommended:
RTV-boosted
Regimen Switching in Setting of Virologic Suppression (6)
Closely monitor tolerability, viral
Regimen Switching in Setting of Virologic Suppression (6)
Closely monitor tolerability, viral
Websites to Access the Guidelines
http://www.aidsetc.org
http://aidsinfo.nih.gov
Websites to Access the Guidelines
http://www.aidsetc.org
http://aidsinfo.nih.gov
 Күйік және оны емдеудің иновациялық әдістері
Күйік және оны емдеудің иновациялық әдістері Бронхиальная астма. Сестринский процесс
Бронхиальная астма. Сестринский процесс Балалардың стоматологиялық ауруларын функциональды диагностикалау әдістері
Балалардың стоматологиялық ауруларын функциональды диагностикалау әдістері Питание детей старше года
Питание детей старше года Аускультация сердца и фонокардиография
Аускультация сердца и фонокардиография История и перспективы развития лечебно-оздоровительного туризма в Западном рекреационном районе Крыма
История и перспективы развития лечебно-оздоровительного туризма в Западном рекреационном районе Крыма Издержки обращения аптечной организации. (Тема 20)
Издержки обращения аптечной организации. (Тема 20) Травматизм. Социально-экономическая значимость. Диагностика и лечение переломов и вывихов
Травматизм. Социально-экономическая значимость. Диагностика и лечение переломов и вывихов Коронароангиография. Введение в анатомию коронарных артерий. Техника проведения. Оценка поражений
Коронароангиография. Введение в анатомию коронарных артерий. Техника проведения. Оценка поражений Эпилепсия и эпилептические синдромы
Эпилепсия и эпилептические синдромы Сердечно-легочная реанимация
Сердечно-легочная реанимация Иммунный ответ организма. Связывание антител с антигеном. (Лекция 6)
Иммунный ответ организма. Связывание антител с антигеном. (Лекция 6) Миома матки
Миома матки Гипертермический синдром
Гипертермический синдром Микроволновая терапия (СВЧ –терапия)
Микроволновая терапия (СВЧ –терапия) Желшешек
Желшешек Балалардағы хейлиттер
Балалардағы хейлиттер Кератоконус. Классификация, симптомы
Кератоконус. Классификация, симптомы Центр медицинской профилактики
Центр медицинской профилактики Аллергиялық жағдайлар, ауыз қуысындағы көрінісі
Аллергиялық жағдайлар, ауыз қуысындағы көрінісі Применение, нежелательное действие лекарственных средств при беременности и в период грудного кормления детей
Применение, нежелательное действие лекарственных средств при беременности и в период грудного кормления детей Приёмы исправления нарушенных звуков речи
Приёмы исправления нарушенных звуков речи Уход за пациентом. ГОСТ Р 56819-2015. Профилактика пролежней
Уход за пациентом. ГОСТ Р 56819-2015. Профилактика пролежней Физиология труда
Физиология труда Функциональная диспепсия: клиника, лечение
Функциональная диспепсия: клиника, лечение Врождённые пороки развития женской половой системы
Врождённые пороки развития женской половой системы Эксперименты врачей на себе – причины, значение и опыт. Светя другим, сгораю
Эксперименты врачей на себе – причины, значение и опыт. Светя другим, сгораю Место и роль медицинской сестры в системе первичного звена здравоохранения
Место и роль медицинской сестры в системе первичного звена здравоохранения