- Ханс Бийлсма. Актуальные вопросы ревматологии

Содержание
- 2. ITEMS TO DISCUSS NEW GUIDELINES 2016 Q & A NEW BIOLOGICALS / BIOSIMILARS Q & A
- 3. ITEMS TO DISCUSS NEW GUIDELINES 2016 NEW BIOLOGICALS / BIOSIMILARS NEWS ON GLUCOCORTICOIDS JAK-inhibitors
- 4. Process of recommendations Proposal to EULAR by convenor and epidemiologist Selection of the group (15-20): rheumatologists,
- 5. Process of recommendations Second meeting: evidence on research questions presented; recommendations confirmed / adapted; explaining text
- 6. Process of recommendations
- 7. 2016 EULAR recommendations for management of early arthritis
- 8. Overarching principles A] Management of early arthritis should aim at the best care and must be
- 9. 2016 EULAR recommendations for management of early arthritis Patients presenting with arthritis (any joint swelling, associated
- 10. 2016 EULAR recommendations for management of early arthritis 3. If a definite diagnosis cannot be reached
- 11. 2016 update recommendations treatment of RA with DMARDs
- 12. EULAR GUIDELINES UPDATE 2016: Overarching principles
- 13. EULAR GUIDELINES UPDATE 2016: Overarching principles
- 14. Algorithm phase I
- 15. Algorithm phase II
- 16. Algorithm phase III
- 17. 2016 update ASAS/EULAR recommendations on the management of axSpA
- 21. Recommendation 9: biological therapy bDMARDs should be considered in patients with persistently high disease activity despite
- 22. Treatment of axSpA patients with bDMARDs Rheumatologist’s diagnosis of axial SpA And Elevated CRP and/or positive
- 23. Continuation of bDMARDs Consider to continue bDMARDs if after at least 12 weeks of treatment: ASDAS
- 24. Recommendation 10: TNFi failure If TNFi therapy fails, switching to another TNFi or IL17i therapy should
- 26. ITEMS TO DISCUSS NEW GUIDELINES 2016 NEW BIOLOGICALS / BIOSIMILARS NEWS ON GLUCOCORTICOIDS JAK-inhibitors
- 27. RA: Immune and Inflammatory Responses Synovitis: inflammation of the synovial membrane that invades and destroys adjacent
- 28. Different immune cells
- 29. Cytokine mediated synovial interaction
- 30. Mechanisms of action of biologicals TNF-α IL-1 IL-6 B cell T cell Hep EC Ab Fb
- 31. Cytokines implicated
- 32. Therapeutic targets
- 33. Window of opportunity close relationship in active RA Therapy early in the course of RA may
- 34. WINDOW OF OPPORTUNITY
- 35. THE U-ACT-EARLY STRATEGY STUDY: RAPID AND SUSTAINED REMISSION IN EARLY RA, TREATED TO TARGET WITH TOCILIZUMAB,
- 36. Study design: Multicenter, randomized, 3 parallel arms, double-blind, placebo-controlled, 2-year study Primary Objective: To assess efficacy
- 37. Treatment Strategies Bijlsma JWJ et al, Lancet 2016 .
- 38. Tight control strategy: T2T Initial regimen: MTX or placebo-MTX: start 10 mg once weekly; increased every
- 39. Step-down Therapy (when SR achieved) MTX/placebo-MTX reduced 5mg/wk every 4 wks down to 10mg/wk and then
- 40. Baseline demographics Bijlsma JWJ et al, Lancet 2016
- 41. Primary Endpoint: SR – initial regimen (ITT ) Bijlsma JWJ et al, Lancet 2016
- 42. Time to sustained remission: initial regimen Bijlsma JWJ et al, Lancet 2016
- 43. Time to sustained remission: whole study Bijlsma JWJ et al, Lancet 2016
- 44. AEs of Particular Interest Differences not statistically significant Bijlsma JWJ et al, Lancet 2016
- 45. Pathway to clinical RA
- 46. PREVENTION OF RHEUMATOID ARTHRITIS BY B CELL DIRECTED THERAPY IN THE EARLIEST PHASE OF THE DISEASE:
- 47. Time-to-clinically manifest arthritis A single shot of rituximab in patients ‘prone to develop RA’: does NOT
- 48. Arthritis prevention in seropositive arthralgia POINTS FOR DISCUSSION: Rituximab is currently not approved for treatment of
- 49. BIOSIMILARs
- 50. The Ethics of Biosimilarity Will RCTs give resolution??
- 51. RANDOMIZED, DOUBLE-BLIND STUDY COMPARING CHS-0214 WITH ETANERCEPT IN PATIENTS WITH ACTIVE RHEUMATOID ARTHRITIS (RA) DESPITE METHOTREXATE
- 53. ITEMS TO DISCUSS NEW GUIDELINES 2016 NEW BIOLOGICALS / BIOSIMILARS NEWS ON GLUCOCORTICOIDS JAK-inhibitors
- 54. Glucocorticoids: risks & benefits Hoes, Nature Rheumatology, 2011.
- 55. EULAR Task Force Defining conditions where long-term glucocorticoid treatment has an acceptably low level of harm
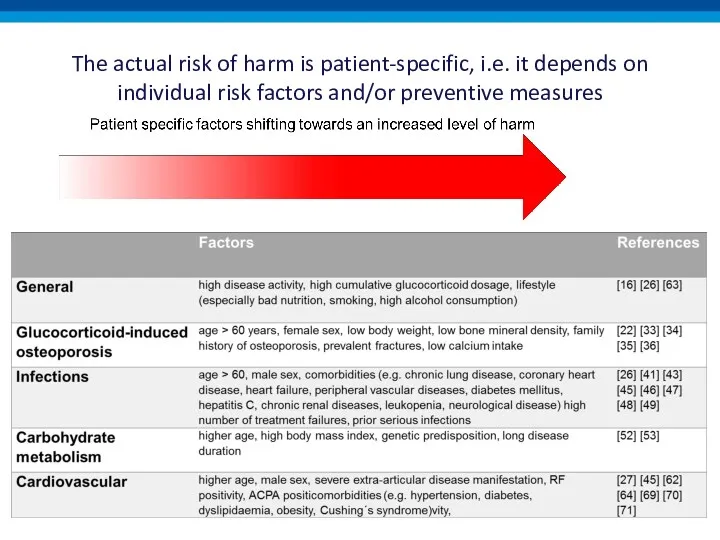
- 57. The actual risk of harm is patient-specific, i.e. it depends on individual risk factors and/or preventive
- 58. The actual risk of harm is patient-specific, i.e. it depends on individual risk factors and/or preventive
- 60. ITEMS TO DISCUSS NEW GUIDELINES 2016 NEW BIOLOGICALS / BIOSIMILARS NEWS ON GLUCOCORTICOIDS JAK-inhibitors
- 61. Cytokines Signal Through Different Intracellular Pathways CYTOPLASM NUCLEUS Kinases Kinases p38 JNK ERK Syk IKK NFκB
- 62. JAK Pathways JAK JAK STAT STAT STAT STAT STAT Figure adapted from Shuai K, et al.
- 63. Oral JAK inhibitors for RA
- 64. Clinical efficacy tofacitinib
- 65. Clinical efficacy baricitinib
- 68. Скачать презентацию
ITEMS TO DISCUSS
NEW GUIDELINES 2016
Q & A
NEW BIOLOGICALS / BIOSIMILARS
Q &
ITEMS TO DISCUSS
NEW GUIDELINES 2016
Q & A
NEW BIOLOGICALS / BIOSIMILARS
Q &
ITEMS TO DISCUSS
NEW GUIDELINES 2016
NEW BIOLOGICALS / BIOSIMILARS
NEWS ON GLUCOCORTICOIDS
JAK-inhibitors
ITEMS TO DISCUSS
NEW GUIDELINES 2016
NEW BIOLOGICALS / BIOSIMILARS
NEWS ON GLUCOCORTICOIDS
JAK-inhibitors
Process of recommendations
Proposal to EULAR by convenor and epidemiologist
Selection of the
Process of recommendations
Proposal to EULAR by convenor and epidemiologist
Selection of the
Process of recommendations
Second meeting: evidence on research questions presented; recommendations confirmed
Process of recommendations
Second meeting: evidence on research questions presented; recommendations confirmed
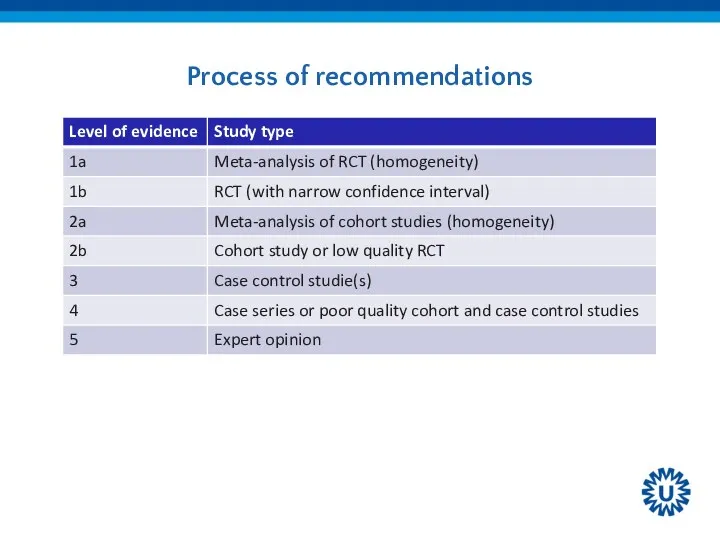
Process of recommendations
Process of recommendations

2016 EULAR recommendations for management of early arthritis
2016 EULAR recommendations for management of early arthritis
![Overarching principles A] Management of early arthritis should aim at](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/370748/slide-7.jpg)
Overarching principles
A] Management of early arthritis should aim at the best
Overarching principles
A] Management of early arthritis should aim at the best
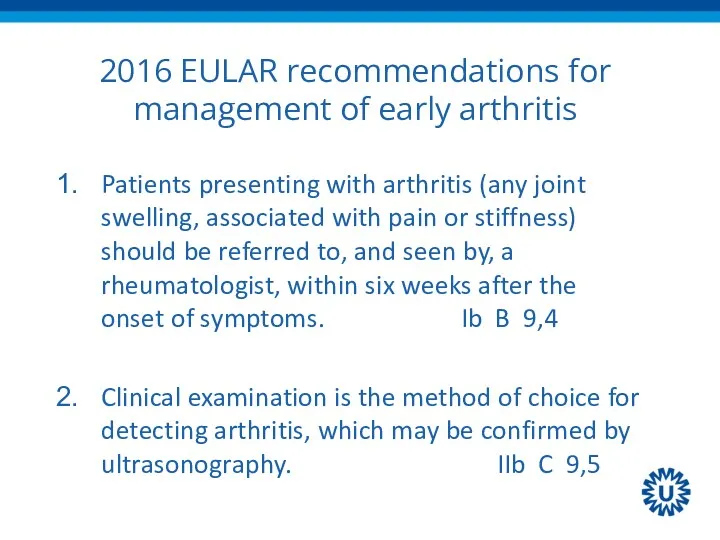
2016 EULAR recommendations for management of early arthritis
Patients presenting with arthritis
2016 EULAR recommendations for management of early arthritis
Patients presenting with arthritis
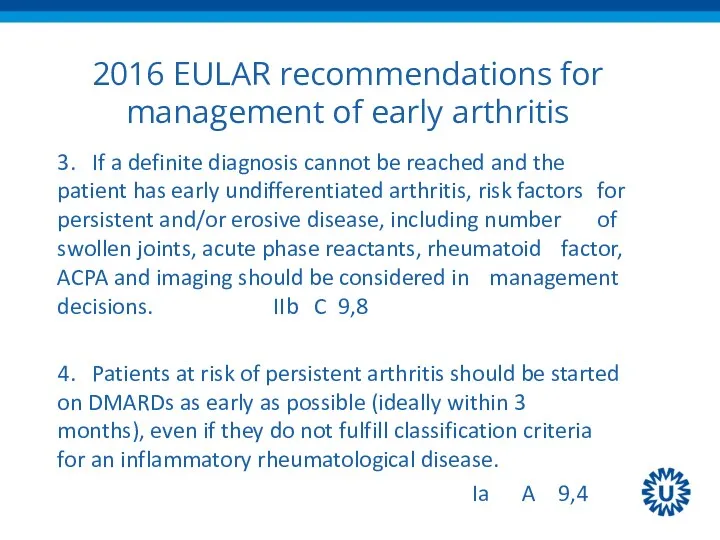
2016 EULAR recommendations for management of early arthritis
3. If a definite
2016 EULAR recommendations for management of early arthritis
3. If a definite

2016 update recommendations treatment of RA with DMARDs
2016 update recommendations treatment of RA with DMARDs
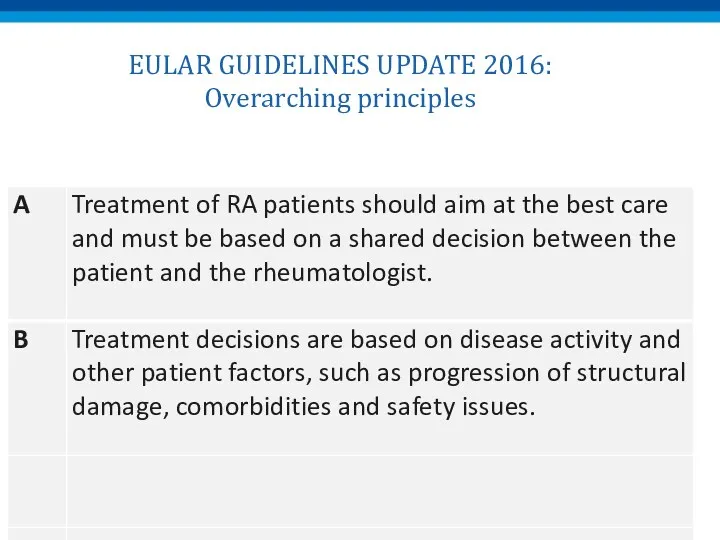
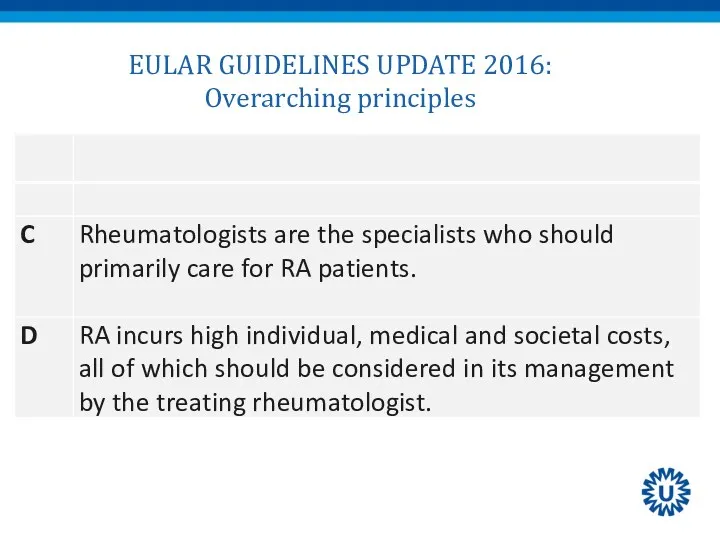
EULAR GUIDELINES UPDATE 2016:
Overarching principles
EULAR GUIDELINES UPDATE 2016:
Overarching principles
EULAR GUIDELINES UPDATE 2016:
Overarching principles
EULAR GUIDELINES UPDATE 2016:
Overarching principles
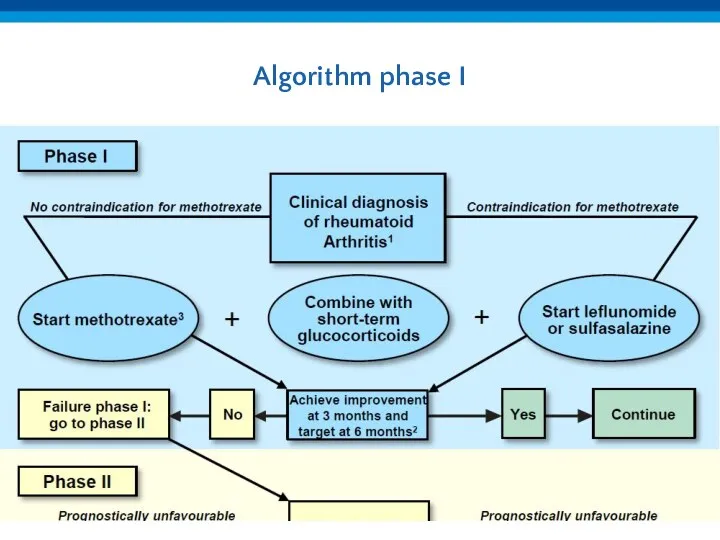
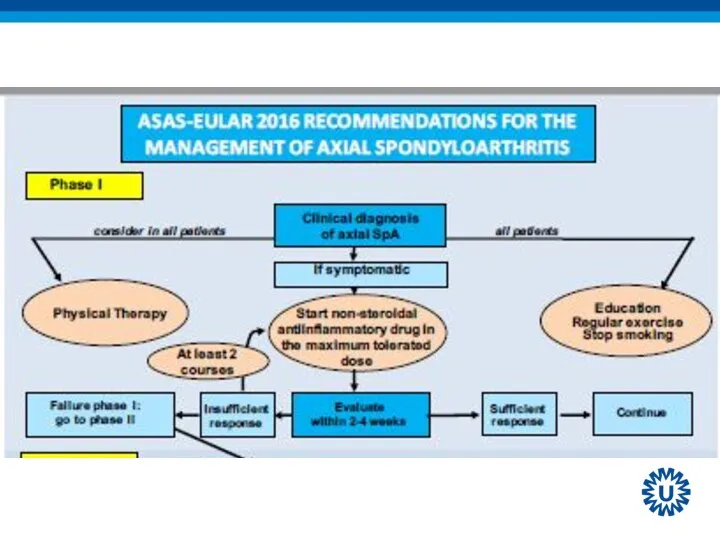
Algorithm phase I
Algorithm phase I
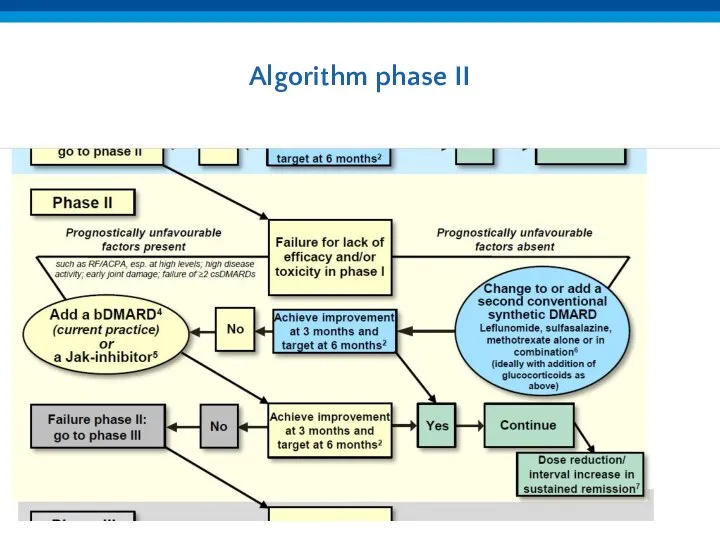
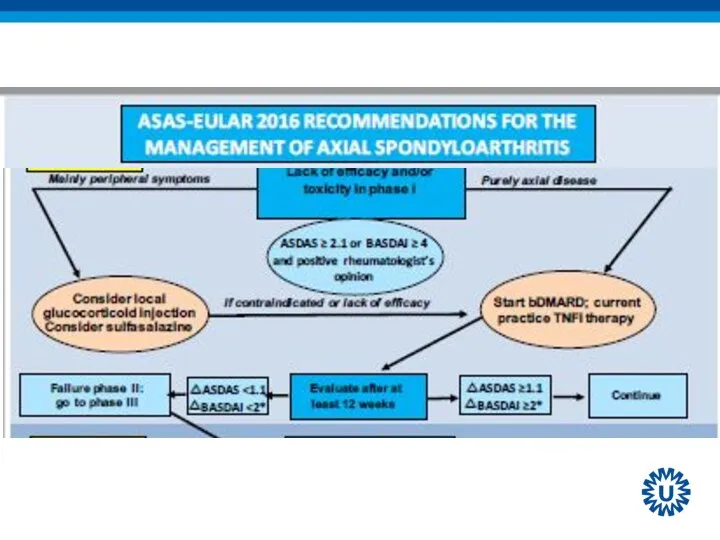
Algorithm phase II
Algorithm phase II
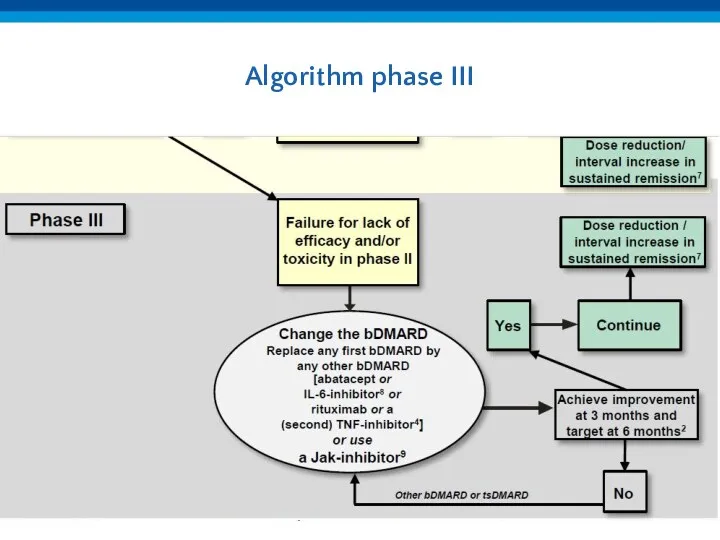
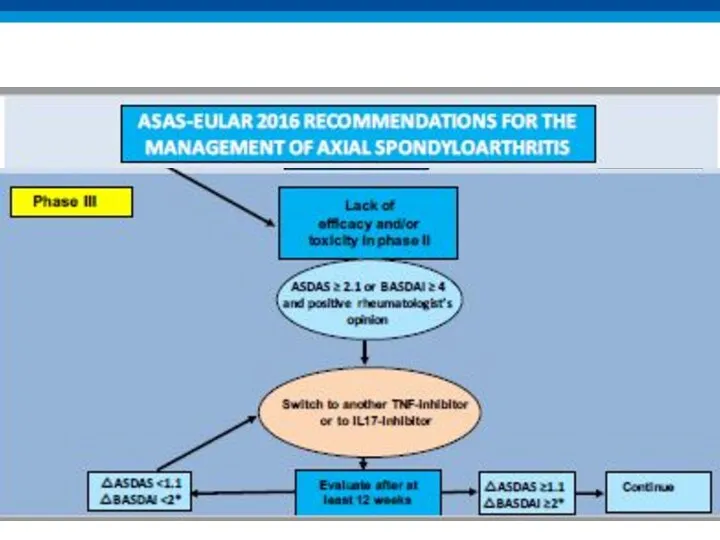
Algorithm phase III
Algorithm phase III

2016 update ASAS/EULAR recommendations on the management of axSpA
2016 update ASAS/EULAR recommendations on the management of axSpA
Recommendation 9: biological therapy
bDMARDs should be considered in patients with persistently
Recommendation 9: biological therapy
bDMARDs should be considered in patients with persistently
Treatment of axSpA patients with bDMARDs
Rheumatologist’s diagnosis of axial SpA
And
Elevated CRP
Treatment of axSpA patients with bDMARDs
Rheumatologist’s diagnosis of axial SpA
And
Elevated CRP
Continuation of bDMARDs
Consider to continue bDMARDs if after at least 12
Continuation of bDMARDs
Consider to continue bDMARDs if after at least 12
Recommendation 10: TNFi failure
If TNFi therapy fails, switching to another TNFi
Recommendation 10: TNFi failure
If TNFi therapy fails, switching to another TNFi
ITEMS TO DISCUSS
NEW GUIDELINES 2016
NEW BIOLOGICALS / BIOSIMILARS
NEWS ON GLUCOCORTICOIDS
JAK-inhibitors
ITEMS TO DISCUSS
NEW GUIDELINES 2016
NEW BIOLOGICALS / BIOSIMILARS
NEWS ON GLUCOCORTICOIDS
JAK-inhibitors
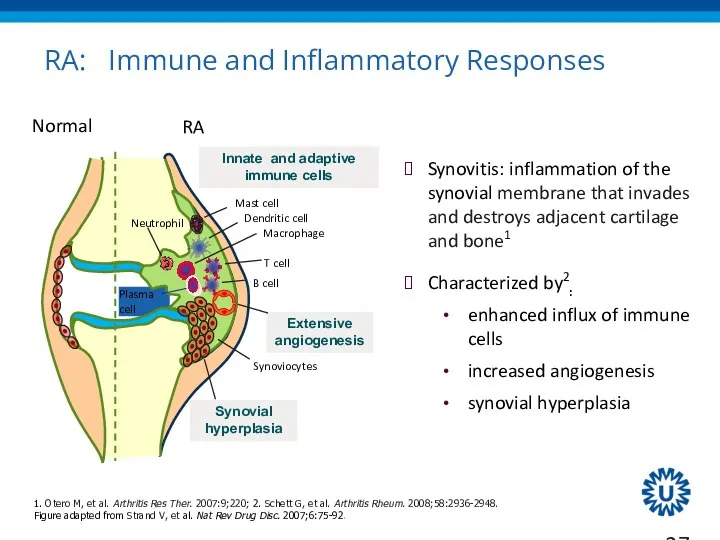
RA: Immune and Inflammatory Responses
Synovitis: inflammation of the synovial membrane that
RA: Immune and Inflammatory Responses
Synovitis: inflammation of the synovial membrane that
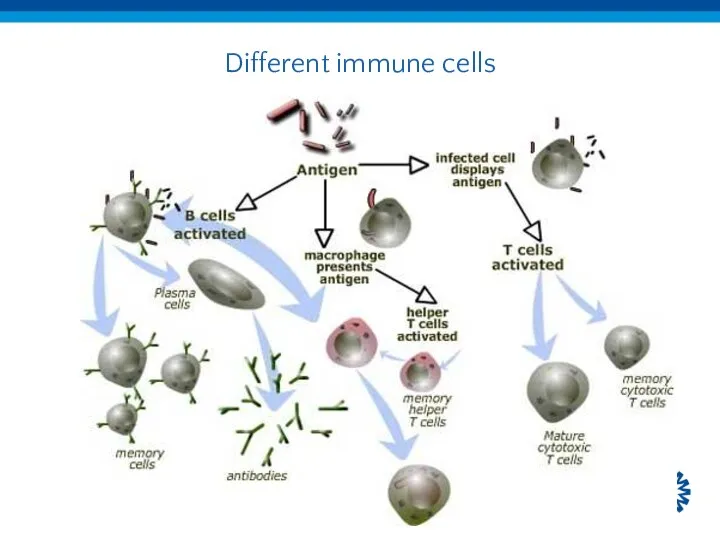
Different immune cells
Different immune cells
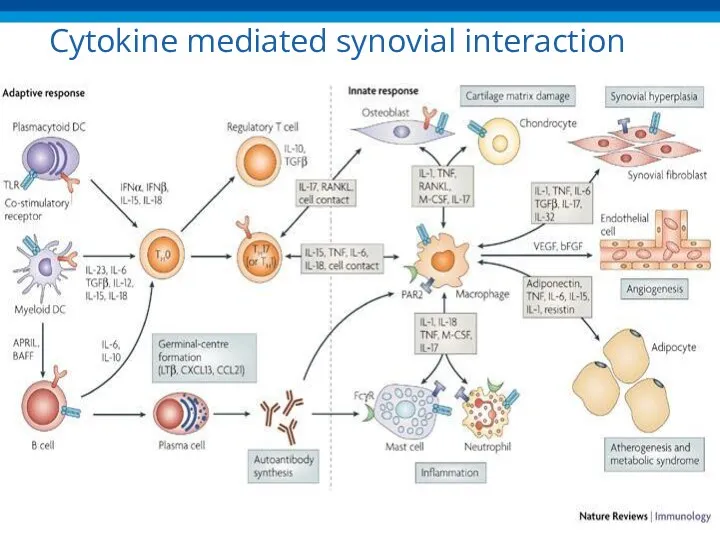
Cytokine mediated synovial interaction
Cytokine mediated synovial interaction
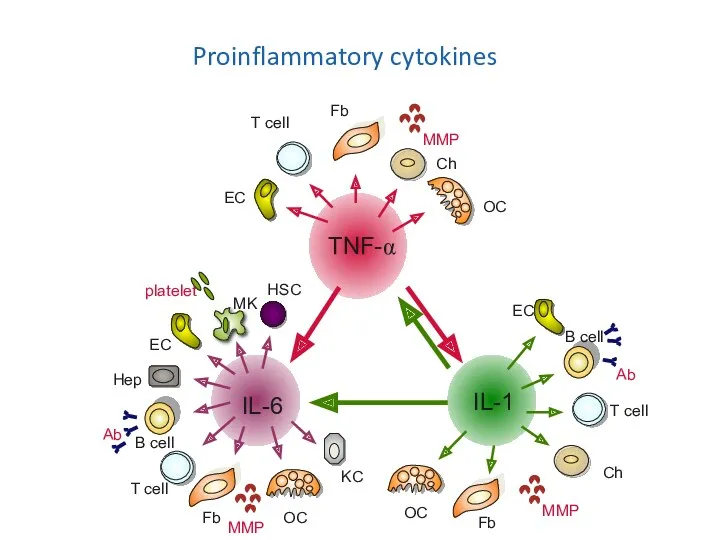
Mechanisms of action of biologicals
TNF-α
IL-1
IL-6
B cell
T cell
Hep
EC
Ab
Fb
MMP
OC
Fb
MMP
Ch
OC
T cell
B cell
Ab
MMP
T cell
Fb
Ch
OC
EC
EC
MK
platelet
KC
HSC
Proinflammatory cytokines
Mechanisms of action of biologicals
TNF-α
IL-1
IL-6
B cell
T cell
Hep
EC
Ab
Fb
MMP
OC
Fb
MMP
Ch
OC
T cell
B cell
Ab
MMP
T cell
Fb
Ch
OC
EC
EC
MK
platelet
KC
HSC
Proinflammatory cytokines
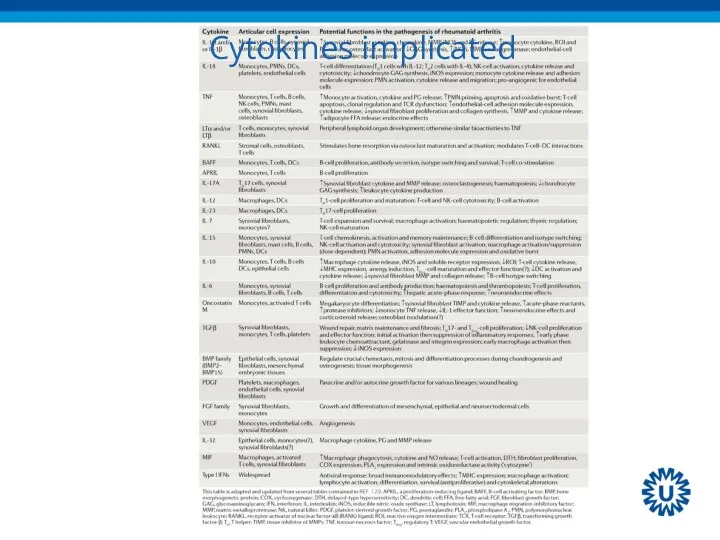
Cytokines implicated
Cytokines implicated
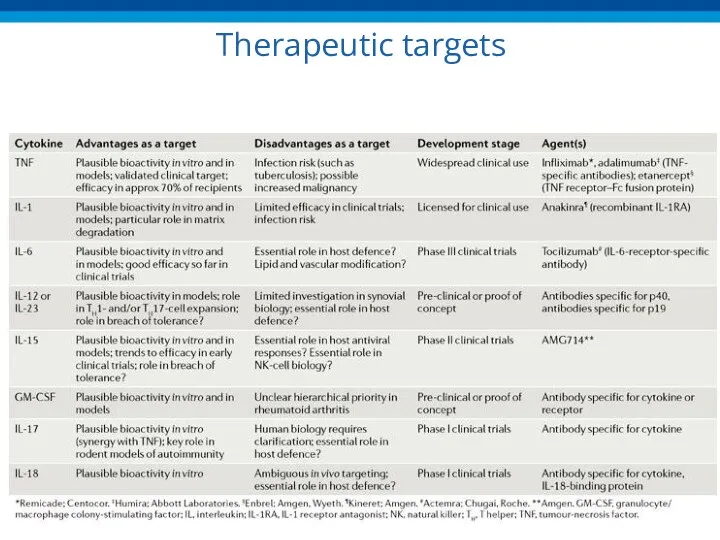
Therapeutic targets
Therapeutic targets
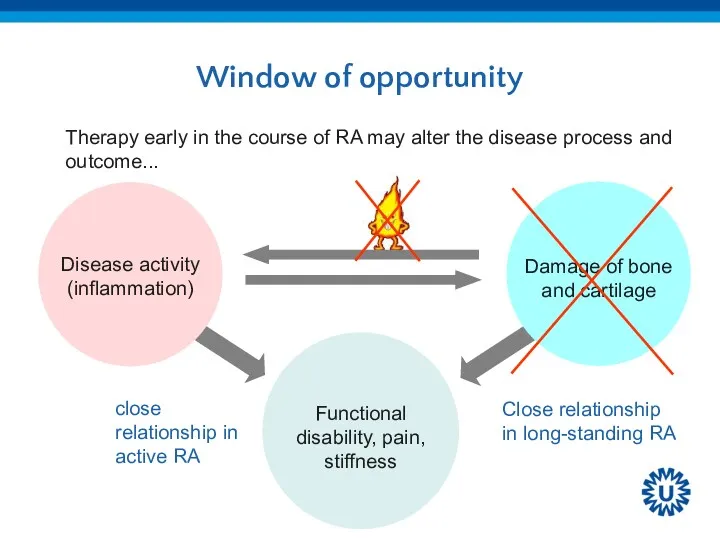
Window of opportunity
close relationship in active RA
Therapy early in the course
Window of opportunity
close relationship in active RA
Therapy early in the course
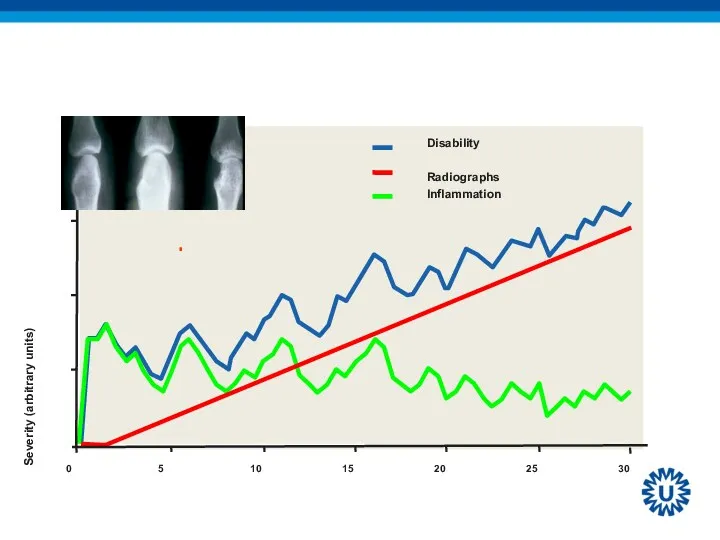
WINDOW OF OPPORTUNITY
WINDOW OF OPPORTUNITY
THE U-ACT-EARLY STRATEGY STUDY:
RAPID AND SUSTAINED REMISSION IN EARLY RA,
THE U-ACT-EARLY STRATEGY STUDY: RAPID AND SUSTAINED REMISSION IN EARLY RA,
Study design:
Multicenter, randomized, 3 parallel arms, double-blind, placebo-controlled, 2-year study
Primary
Study design:
Multicenter, randomized, 3 parallel arms, double-blind, placebo-controlled, 2-year study
Primary
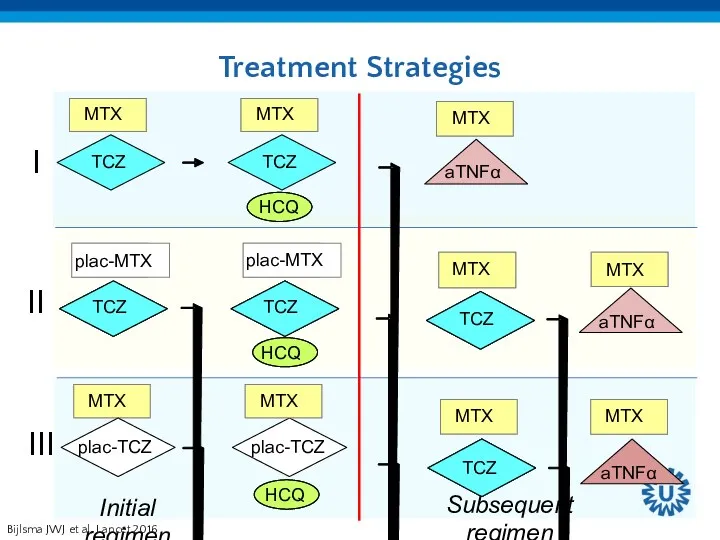
Treatment Strategies
Bijlsma JWJ et al, Lancet 2016
.
Treatment Strategies
Bijlsma JWJ et al, Lancet 2016
.

Tight control strategy: T2T
Initial regimen:
MTX or placebo-MTX: start 10 mg once
Tight control strategy: T2T
Initial regimen:
MTX or placebo-MTX: start 10 mg once
Step-down Therapy (when SR achieved)
MTX/placebo-MTX reduced 5mg/wk every 4 wks down
Step-down Therapy (when SR achieved)
MTX/placebo-MTX reduced 5mg/wk every 4 wks down
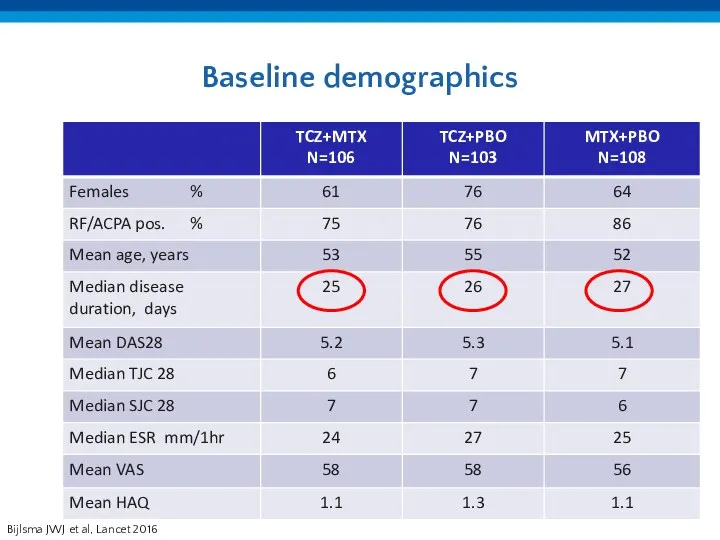
Baseline demographics
Bijlsma JWJ et al, Lancet 2016
Baseline demographics
Bijlsma JWJ et al, Lancet 2016
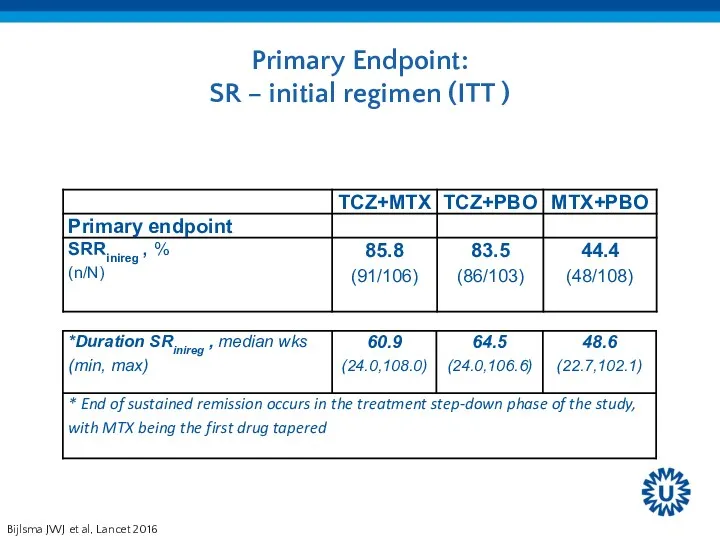
Primary Endpoint:
SR – initial regimen (ITT )
Bijlsma JWJ et
Primary Endpoint:
SR – initial regimen (ITT )
Bijlsma JWJ et
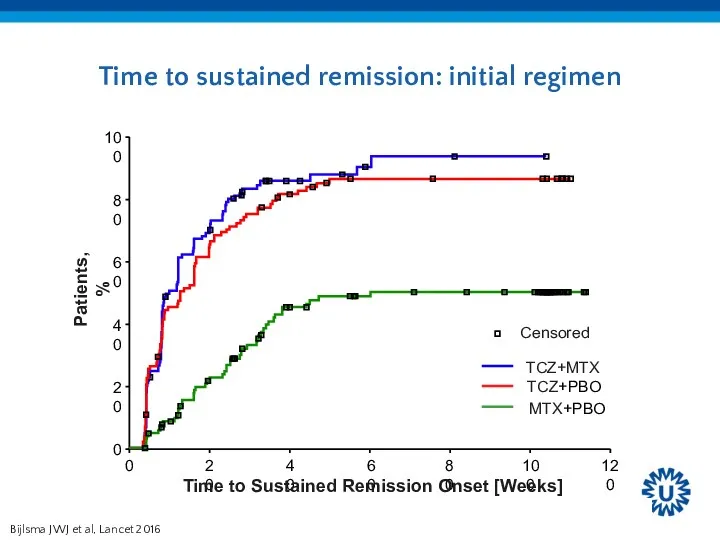
Time to sustained remission: initial regimen
Bijlsma JWJ et al, Lancet 2016
Time to sustained remission: initial regimen
Bijlsma JWJ et al, Lancet 2016
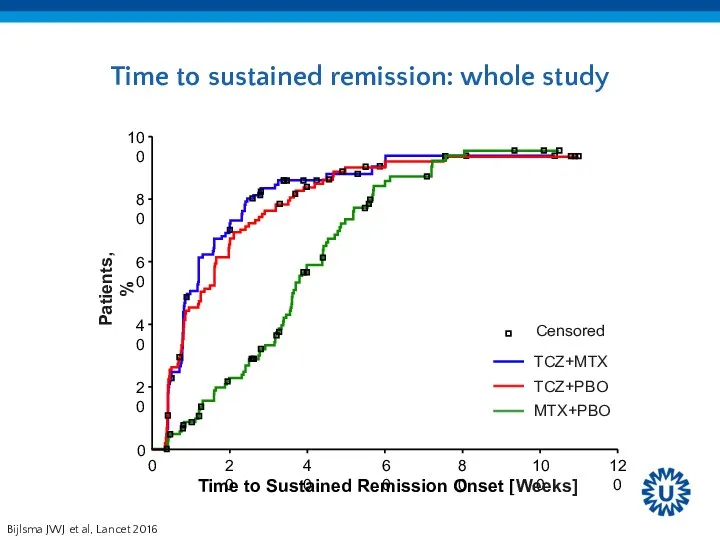
Time to sustained remission: whole study
Bijlsma JWJ et al, Lancet 2016
Time to sustained remission: whole study
Bijlsma JWJ et al, Lancet 2016
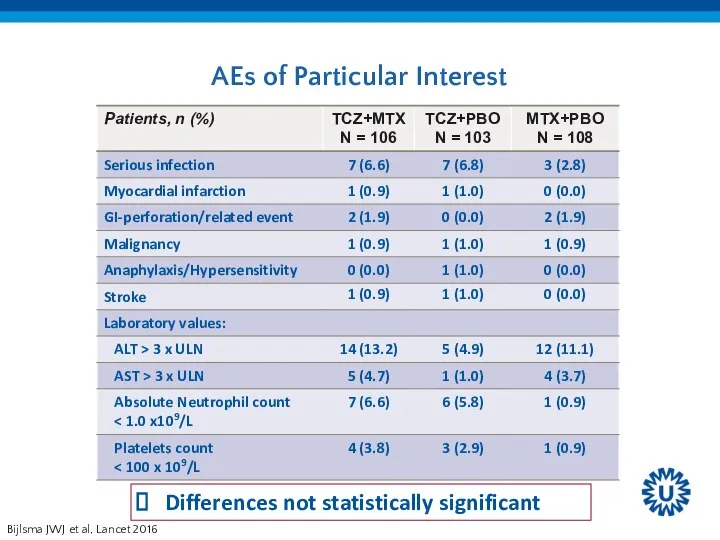
AEs of Particular Interest
Differences not statistically significant
Bijlsma JWJ et al, Lancet
AEs of Particular Interest
Differences not statistically significant
Bijlsma JWJ et al, Lancet
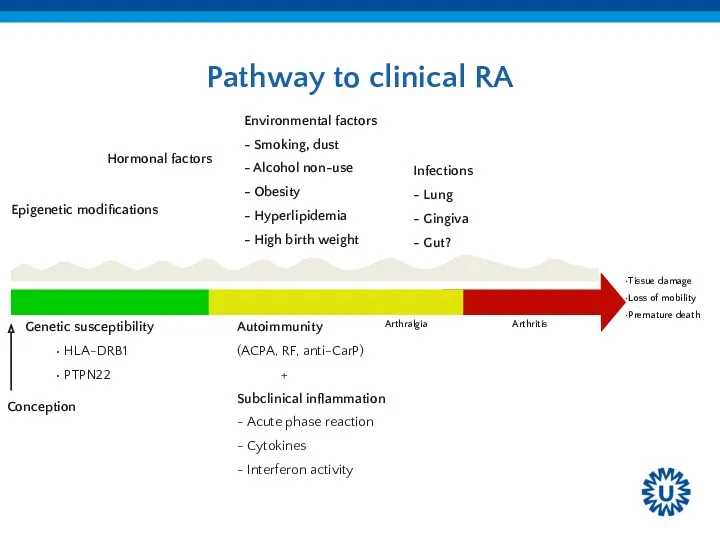
Pathway to clinical RA
Pathway to clinical RA
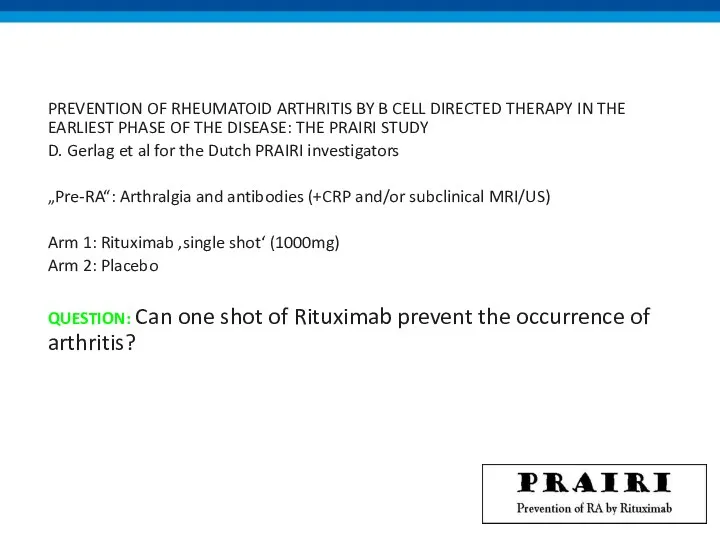
PREVENTION OF RHEUMATOID ARTHRITIS BY B CELL DIRECTED THERAPY IN THE
PREVENTION OF RHEUMATOID ARTHRITIS BY B CELL DIRECTED THERAPY IN THE
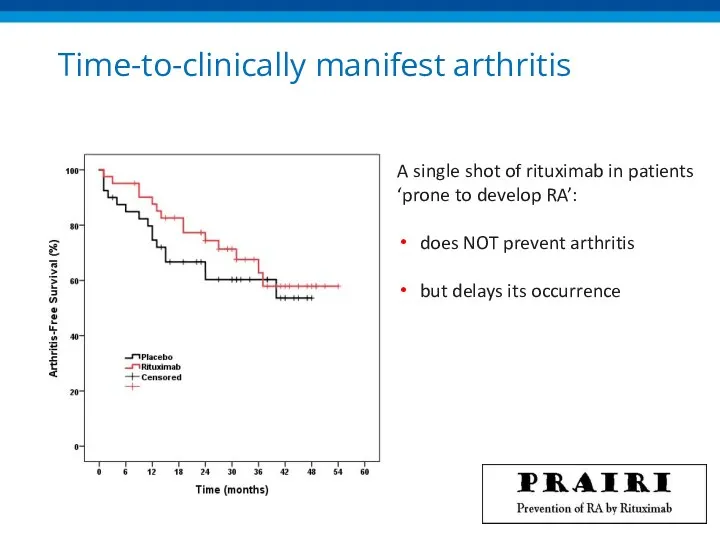
Time-to-clinically manifest arthritis
A single shot of rituximab in patients
‘prone to
Time-to-clinically manifest arthritis
A single shot of rituximab in patients ‘prone to
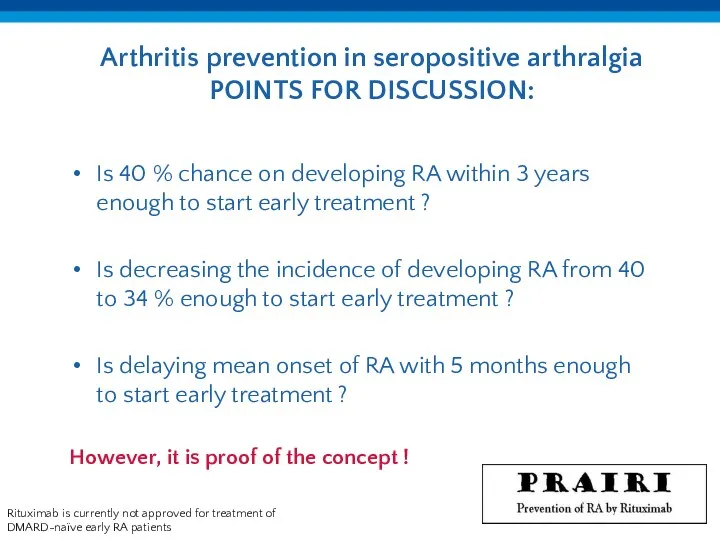
Arthritis prevention in seropositive arthralgia
POINTS FOR DISCUSSION:
Rituximab is currently not approved
Arthritis prevention in seropositive arthralgia
POINTS FOR DISCUSSION:
Rituximab is currently not approved
BIOSIMILARs
BIOSIMILARs
The Ethics of Biosimilarity
Will RCTs give resolution??
The Ethics of Biosimilarity
Will RCTs give resolution??
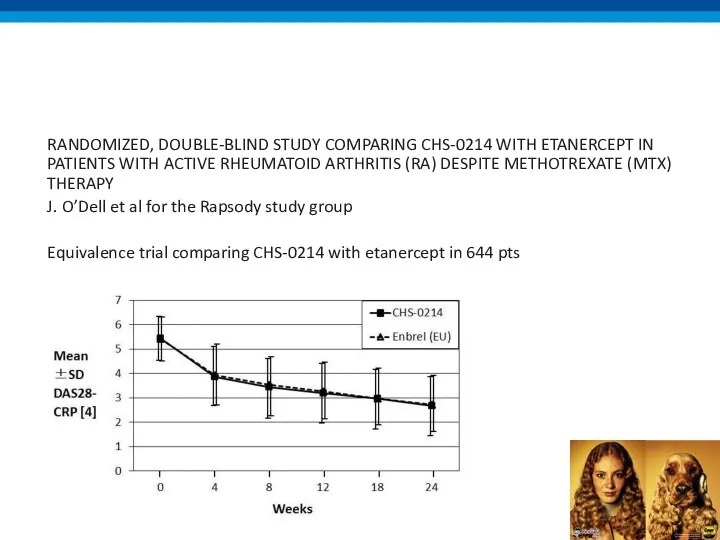
RANDOMIZED, DOUBLE-BLIND STUDY COMPARING CHS-0214 WITH ETANERCEPT IN PATIENTS WITH ACTIVE
RANDOMIZED, DOUBLE-BLIND STUDY COMPARING CHS-0214 WITH ETANERCEPT IN PATIENTS WITH ACTIVE
ITEMS TO DISCUSS
NEW GUIDELINES 2016
NEW BIOLOGICALS / BIOSIMILARS
NEWS ON GLUCOCORTICOIDS
JAK-inhibitors
ITEMS TO DISCUSS
NEW GUIDELINES 2016
NEW BIOLOGICALS / BIOSIMILARS
NEWS ON GLUCOCORTICOIDS
JAK-inhibitors
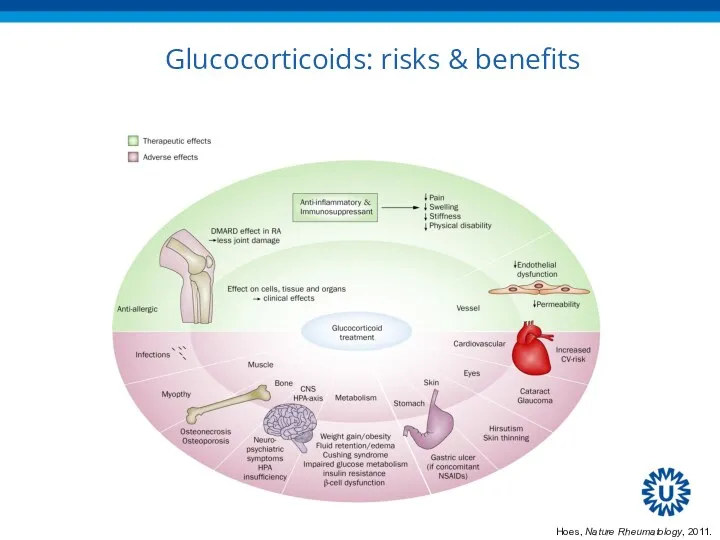
Glucocorticoids: risks & benefits
Hoes, Nature Rheumatology, 2011.
Glucocorticoids: risks & benefits
Hoes, Nature Rheumatology, 2011.
EULAR Task Force
Defining conditions where long-term glucocorticoid treatment has an acceptably
EULAR Task Force
Defining conditions where long-term glucocorticoid treatment has an acceptably
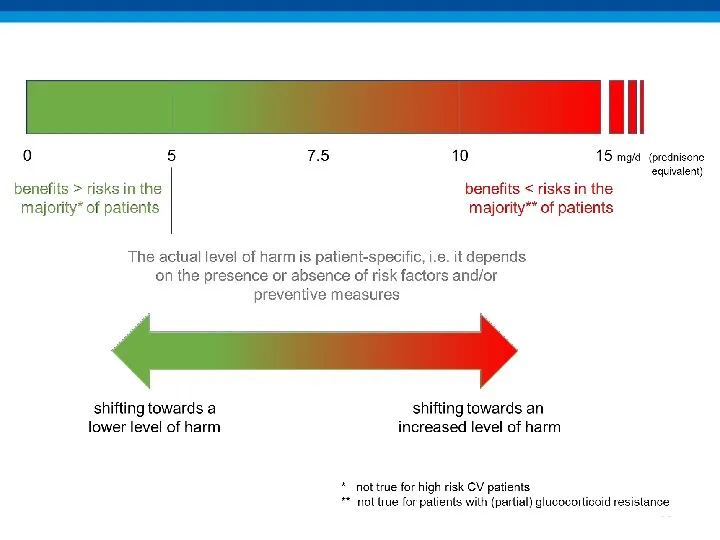
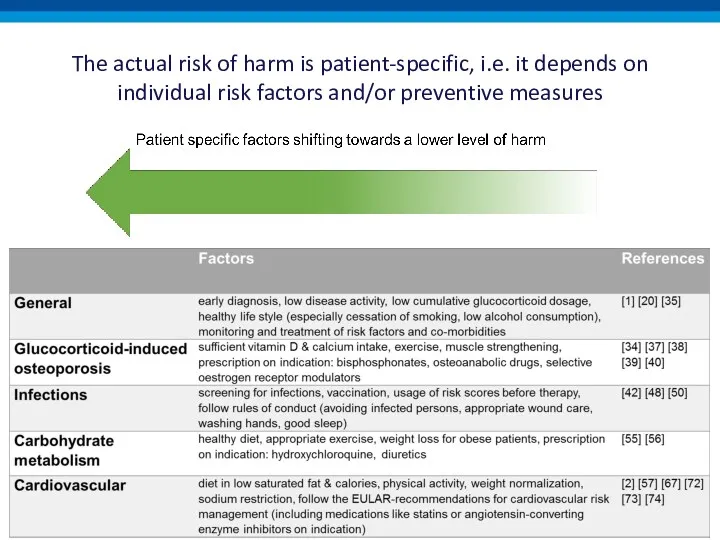
The actual risk of harm is patient-specific, i.e. it depends on
The actual risk of harm is patient-specific, i.e. it depends on
The actual risk of harm is patient-specific, i.e. it depends on
The actual risk of harm is patient-specific, i.e. it depends on
ITEMS TO DISCUSS
NEW GUIDELINES 2016
NEW BIOLOGICALS / BIOSIMILARS
NEWS ON GLUCOCORTICOIDS
JAK-inhibitors
ITEMS TO DISCUSS
NEW GUIDELINES 2016
NEW BIOLOGICALS / BIOSIMILARS
NEWS ON GLUCOCORTICOIDS
JAK-inhibitors
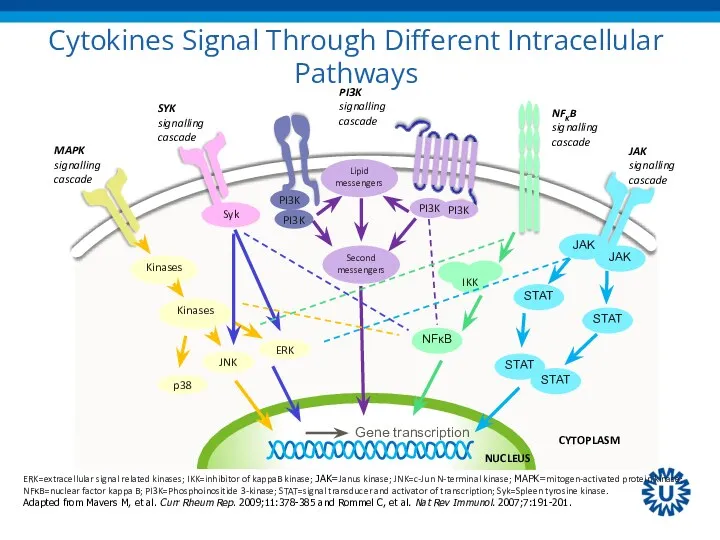
Cytokines Signal Through Different Intracellular Pathways
CYTOPLASM
NUCLEUS
Kinases
Kinases
p38
JNK
ERK
Syk
IKK
NFκB
JAK
JAK
STAT
STAT
STAT
STAT
ERK=extracellular signal related kinases; IKK=inhibitor of
Cytokines Signal Through Different Intracellular Pathways
CYTOPLASM
NUCLEUS
Kinases
Kinases
p38
JNK
ERK
Syk
IKK
NFκB
JAK
JAK
STAT
STAT
STAT
STAT
ERK=extracellular signal related kinases; IKK=inhibitor of
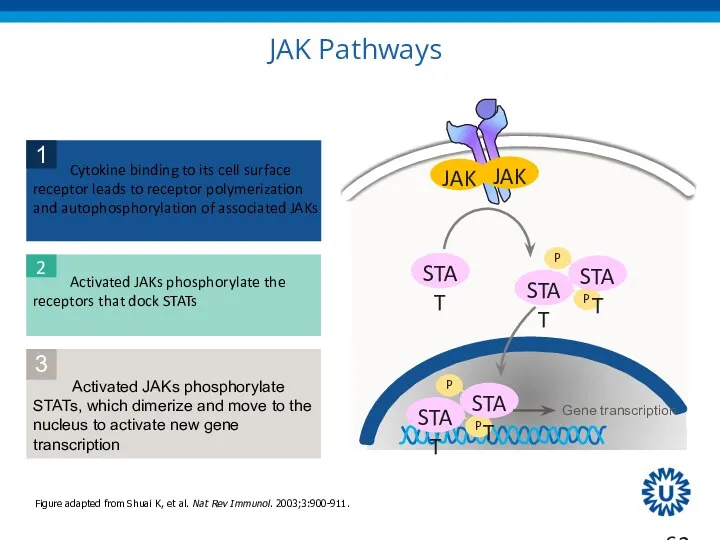
JAK Pathways
JAK
JAK
STAT
STAT
STAT
STAT
STAT
Figure adapted from Shuai K, et al. Nat Rev Immunol.
JAK Pathways
JAK
JAK
STAT
STAT
STAT
STAT
STAT
Figure adapted from Shuai K, et al. Nat Rev Immunol.
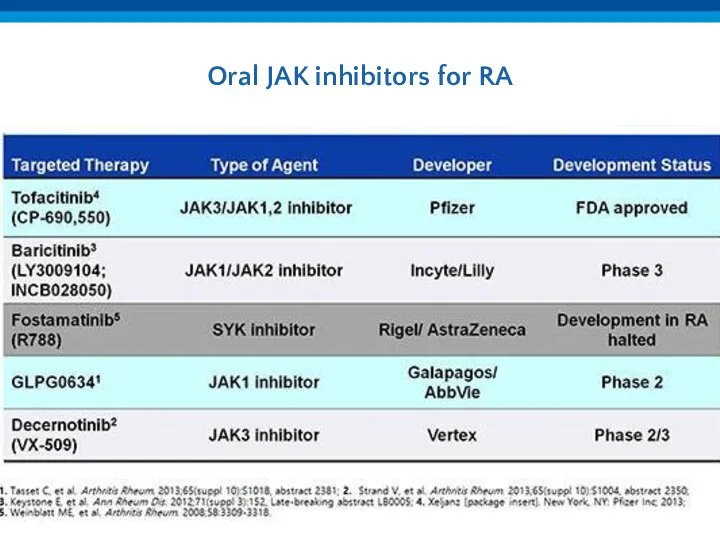
Oral JAK inhibitors for RA
Oral JAK inhibitors for RA
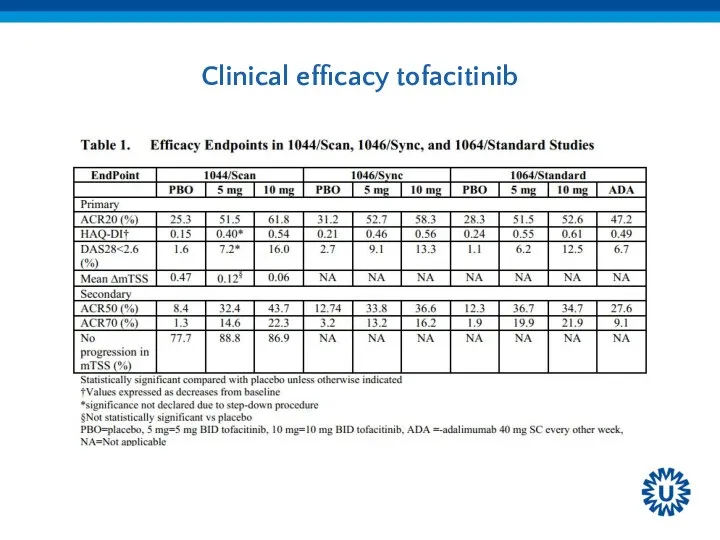
Clinical efficacy tofacitinib
Clinical efficacy tofacitinib
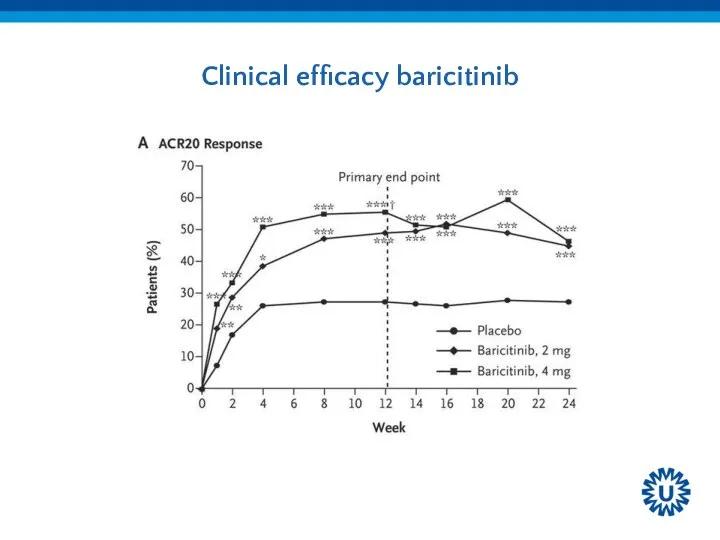
Clinical efficacy baricitinib
Clinical efficacy baricitinib
 Здоров’я людини і навколишне середовище
Здоров’я людини і навколишне середовище Морально-этические проблемы медицинской генетики
Морально-этические проблемы медицинской генетики Эссенциальная артериальная гипертензия
Эссенциальная артериальная гипертензия Бауыр эхинококкозы
Бауыр эхинококкозы Первая помощь при отравлениях
Первая помощь при отравлениях Телемедицина. Основные области применения телемедицинских систем
Телемедицина. Основные области применения телемедицинских систем Сестринская помощь при заболеваниях желудка и двенадцатиперстной кишки
Сестринская помощь при заболеваниях желудка и двенадцатиперстной кишки Валидация очистки помещения и оборудования
Валидация очистки помещения и оборудования Средний отдел пищеварительной системы. Гистология
Средний отдел пищеварительной системы. Гистология Этиололия хронических гастритов и гастродуоденитов
Этиололия хронических гастритов и гастродуоденитов Коллапсотерапия. Виды
Коллапсотерапия. Виды Понятие о микробиологии, иммунологии и эпидемиологии. Меры профилактики инфекционных заболеваний
Понятие о микробиологии, иммунологии и эпидемиологии. Меры профилактики инфекционных заболеваний Дүниежүзілік денсаулық сақтау ұйымы
Дүниежүзілік денсаулық сақтау ұйымы Аневризма грудной аорты
Аневризма грудной аорты Инновационная экономика и технологическое предпринимательство
Инновационная экономика и технологическое предпринимательство Искусственное кровообращение у новорожденных
Искусственное кровообращение у новорожденных Этиологические факторы возникновения неинфекционных заболеваний и деятельность медицинской сестры по их профилактике
Этиологические факторы возникновения неинфекционных заболеваний и деятельность медицинской сестры по их профилактике Общая семиотика экстрапирамидных нарушений
Общая семиотика экстрапирамидных нарушений Патогенность и вирулентность. Факторы патогенности микроорганизмов
Патогенность и вирулентность. Факторы патогенности микроорганизмов Клінічна та біологічна смерть
Клінічна та біологічна смерть Диспансеризация населения
Диспансеризация населения Гиперандрогения у женщин
Гиперандрогения у женщин Клиническая фармакокинетика и фармакодинамика лекарственных средств. Побочное действие
Клиническая фармакокинетика и фармакодинамика лекарственных средств. Побочное действие Денсаулық 2020 бағдарламасы
Денсаулық 2020 бағдарламасы Брюшной тиф. Этиология
Брюшной тиф. Этиология Ризикована поведінка
Ризикована поведінка Хирургическая инфекция. Лекция по общей хирургии
Хирургическая инфекция. Лекция по общей хирургии Опухоли. Этиология, патогенез, морфогенез опухоли
Опухоли. Этиология, патогенез, морфогенез опухоли