- Heart failure

Содержание
- 2. HEART FAILURE (HF) Heart failure is a syndrome manifesting as the inability of the heart to
- 3. A state in which the heart cannot provide sufficient cardiac output to satisfy the metabolic needs
- 4. ESC GUIDELINES FOR DIAGNOSTIC AND TREATMENT OF ACUTE AND CHRONIC HF (2016) HF is a clinical
- 5. HF – is an imprecise term used to describe the pathological state that develops when the
- 6. STATISTICS HF afflicts 2,1% of population At 40 years of age, the lifetime risk of developing
- 7. Final common pathway for many cardiovascular diseases whose natural history results in symptomatic or asymptomatic left
- 8. PROGNOSIS HF is a strong predictor of the sudden cardiac death The 5-year mortality rate for
- 9. AETHIOLOGY OF HF The three major contributors are: hypertension, coronary ar tery disease, dilated cardiomyopathy, heart
- 10. RISK FACTORS Hypertension Diabetes Age Obesity Heart valve problems Unhealthy lifestyle (smoking, physical inactivity, etc.)
- 11. NORMAL PHYSIOLOGY OF THE HEART Cardiac output depends on: Contractility Preload (the volume and pressure in
- 12. FRANK-STARLINGS LAW:
- 13. NEUROHUMORAL ACTIVATION Decreased contractility Sympathetic nervous system Renin-angiotensin system Increased release of vasopressin Endothelin arterial and
- 14. COMPENSATORY CHANGES IN HEART FAILURE Activation of СNS Activation of RAS Increased heart rate Release of
- 15. CLASSIFICATION Heart failure can be classified in several ways 1 - Acute and chronic HF 2
- 16. ACCF/AHA STAGES OF HF Stage A: At high risk for HF but without structural heart disease
- 17. ESC GUIDELINES FOR DIAGNOSTIC AND TREATMENT OF ACUTE AND CHRONIC HF (2016) Definition of heart failure
- 18. ESC GUIDELINES FOR DIAGNOSTIC AND TREATMENT OF ACUTE AND CHRONIC HF (2016) In previous guidelines it
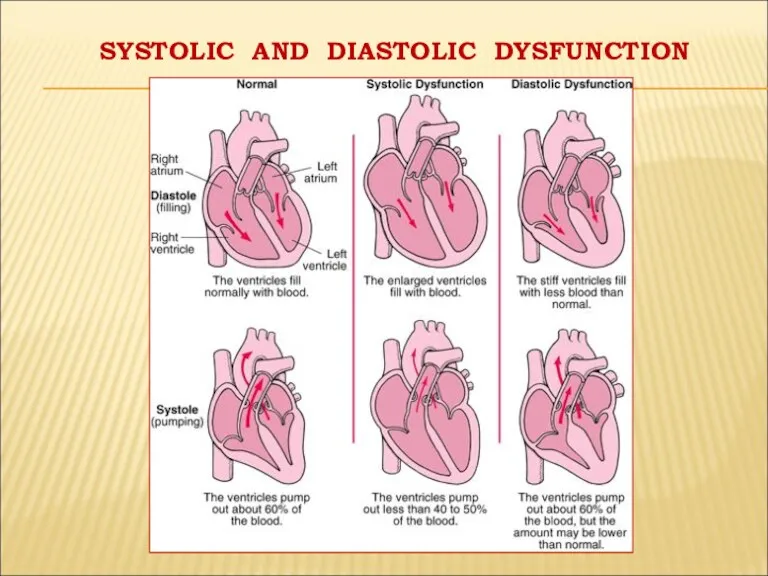
- 19. SYSTOLIC AND DIASTOLIC DYSFUNCTION
- 20. « FORWARD AND BACKWARD HF» In some patients with HF the predominant problem is an inadequate
- 21. "HIGH OUTPUT CARDIAC FAILURE” This can occur from: Severe anemia, Gram negative septicaemia, Beriberi (vitamin B1/thiamine
- 22. Decrease of pump function decrease cardiac output, heart volume per minute decrease arterial pressure increase activity
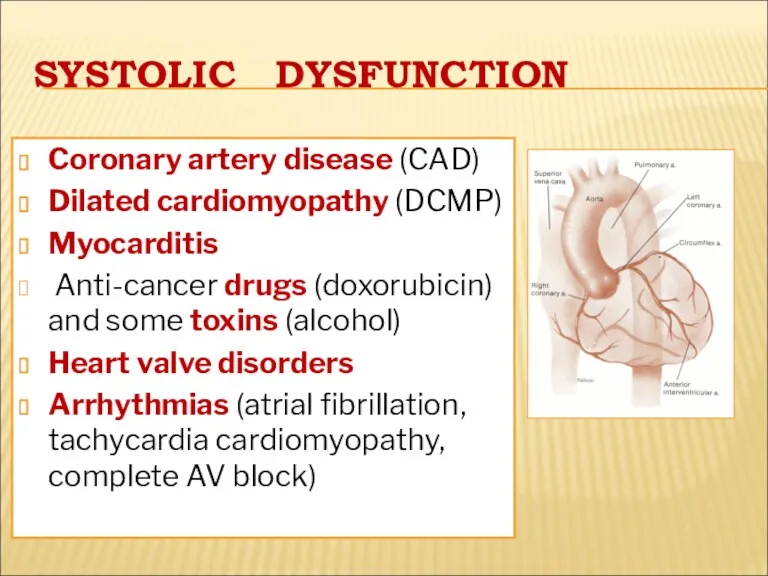
- 23. SYSTOLIC DYSFUNCTION Coronary artery disease (CAD) Dilated cardiomyopathy (DCMP) Myocarditis Anti-cancer drugs (doxorubicin) and some toxins
- 24. DIASTOLIC DYSFUNCTION Constrictive pericarditis, cardiac tamponade LV hypertrophy (hypertension) Restrictive cardiomyopathy
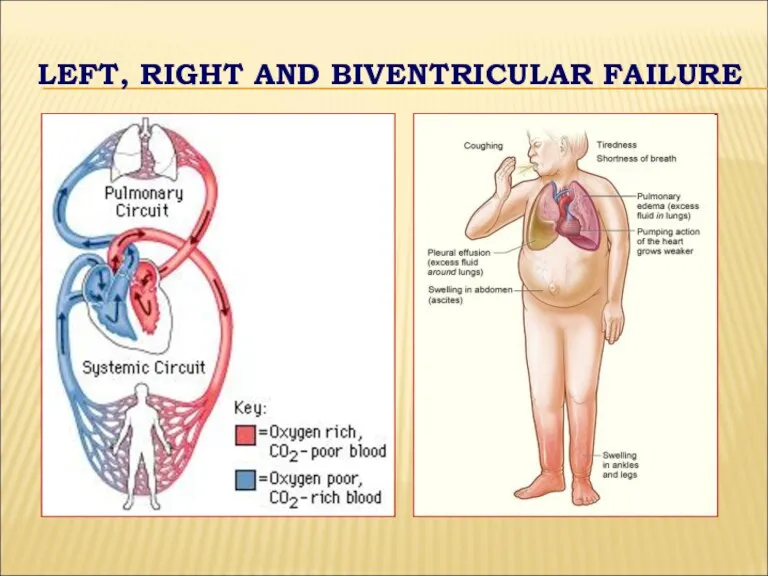
- 25. LEFT, RIGHT AND BIVENTRICULAR FAILURE
- 26. LEFT-SIDED FAILURE Dyspnea and suffocation Orthopnea Paroxysmal nocturnal dyspnea Peripheral cyanosis and coldness Tiredness, weakness, anxiety
- 27. PERIPHERAL CYANOSIS
- 28. RIGHT-SIDED FAILURE Fluid accumulation and swelling (edema) in the feet, ankles, legs Hepatomegaly Enlargement of abdomen
- 29. NEW YORK НЕАRT ASSOCIATION (NYHA) FUNCTIONAL CLASSIFICATION OF CHF
- 30. DIAGNOSIS OF HF Symptoms (underlying disease + HF) Physical examination (pulse, BP, abnormal heart sounds and
- 31. X-RAY EXAMINATION LUNGS: - RETICULAR SHADOWING - SEPTAL (‘KERLEY B’ LINES) - ENLARGED HILAR VESSELS -
- 33. ECHOCARDIOGRAPHY Ejection fraction LA > 40 mm EDV-LV > 55 mm EDV-RV > 26 mm IVS
- 34. BLOOD TESTS B-type natriuretic peptide (BNP) is a specific test indicative of heart failure. BNP >
- 35. FRAMINGHAM CRITERIA requires the simultaneous presence of at least 2 of the following major criteria or
- 36. FRAMINGHAM CRITERIA Minor criteria: Tachycardia of more than 120 beats per minute Nocturnal cough Dyspnea on
- 37. THE COURSE OF CHF Symptoms of heart failure may begin suddenly, especially if the cause is
- 38. TREATMENT OF HEART FAILURE Acute and chronic management strategies in heart failure are aimed at improving
- 39. MANAGEMENT OF THE HEART FAILURE The main purposes: To reduce mortality !!! To relieve HF symptoms
- 40. GOALS OF TREATMENT To improve symptoms and quality of life To decrease likelihood of disease progression
- 41. THE MAIN PRINCIPLES OF HF MANAGEMENT To reveal and exclude triggering factors To normalise cardiac output
- 42. METHODS OF HF MANAGEMENT Non-medical (changing lifestyle) Pharmacotherapy (ACE inhibitors or ARBs, beta-blockers, aldosterone antagonists, diuretics,
- 43. PHARMACOTHERAPY FOR HF 1 DRUGS PROVED TO BE ABLE TO REDUCE MORBIDITY AND MORTALITY RATES IN
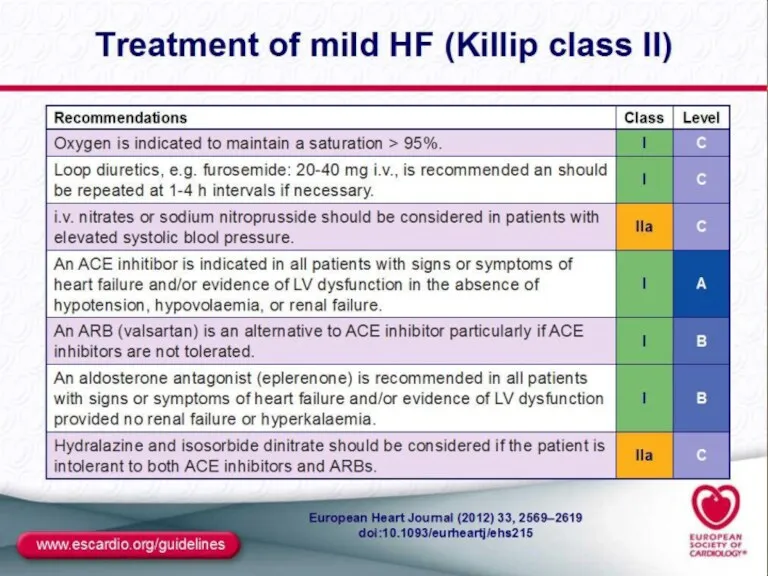
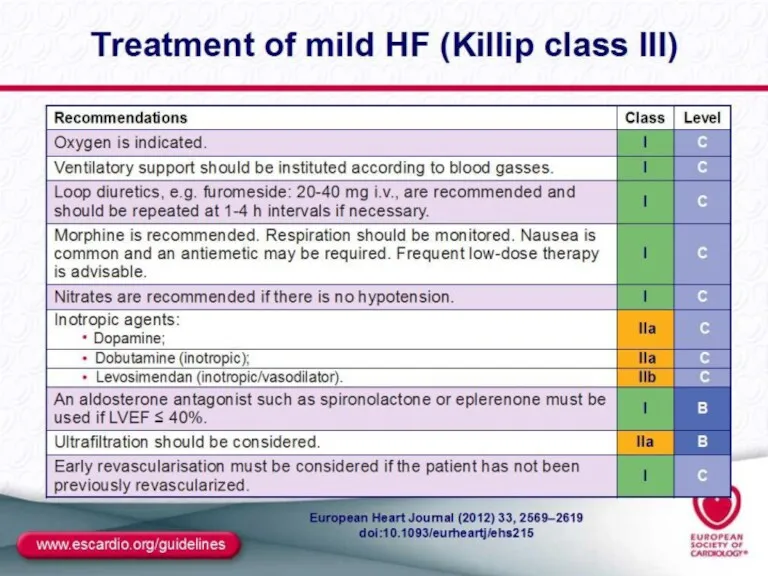
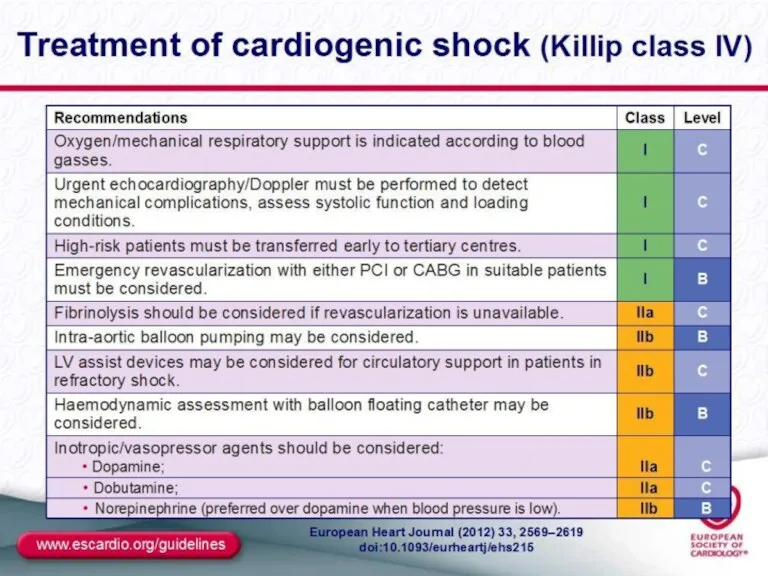
- 44. MANAGEMENT OF ACUTE LV FAILURE
- 45. MANAGEMENT OF ACUTE LV FAILURE
- 49. GENERAL MANAGEMENT OF CHRONIC HF Education of patient and relatives Diet: decrease of salt intake, good
- 50. MANAGEMENT OF CHF WITH SYSTOLIC DYSFUNCTION OF LV (ESC GUIDELINES ,2016)
- 51. Management of CHF with systolic dysfunction of LV
- 52. №2 MANAGEMENT OF CHF WITH SYSTOLIC DYSFUNCTION OF LV 3.. Aldosterone receptor blockers: Eplerenone 12,5 –
- 53. №3 Management of CHF with systolic dysfunction of LV 6.Diuretcs:Loop diuretics: Furosemide 40-500 mg daily, Ethacrynic
- 54. ADDITIONAL DRUGS Anti-aggregants: aspirin (100-300 mg daily) Anti-coagulants: warfarin (3-9 mg daily) Statins: atorvastatin (10-80 mg
- 55. MANAGEMENT OF CHF WITH NORMAL SYSTOLIC FUNCTION OF LV Main group: Angiotensin-converting enzyme inhibitors Beta-blockers Angiotensin
- 56. SURGICAL TREATMENT The following procedures decrease the risk of sudden death and cardiac mortality: Implantation of
- 58. Скачать презентацию
HEART FAILURE (HF)
Heart failure is a syndrome manifesting as the inability of the heart
HEART FAILURE (HF)
Heart failure is a syndrome manifesting as the inability of the heart
A state in which the heart cannot provide sufficient cardiac output
A state in which the heart cannot provide sufficient cardiac output
ESC GUIDELINES FOR DIAGNOSTIC AND TREATMENT OF ACUTE AND CHRONIC HF
ESC GUIDELINES FOR DIAGNOSTIC AND TREATMENT OF ACUTE AND CHRONIC HF
HF – is an imprecise term used to describe the pathological
HF – is an imprecise term used to describe the pathological
STATISTICS
HF afflicts 2,1% of population
At 40 years of
STATISTICS
HF afflicts 2,1% of population
At 40 years of
Final common pathway for many cardiovascular diseases whose natural history results
Final common pathway for many cardiovascular diseases whose natural history results
PROGNOSIS
HF is a strong predictor of the sudden cardiac death
The
PROGNOSIS
HF is a strong predictor of the sudden cardiac death
The
AETHIOLOGY OF HF
The three major contributors are:
hypertension, coronary ar
tery disease,
dilated
AETHIOLOGY OF HF
The three major contributors are:
hypertension, coronary ar
tery disease,
dilated
RISK FACTORS
Hypertension
Diabetes
Age
Obesity
Heart valve problems
Unhealthy lifestyle (smoking, physical inactivity, etc.)
RISK FACTORS
Hypertension
Diabetes
Age
Obesity
Heart valve problems
Unhealthy lifestyle (smoking, physical inactivity, etc.)
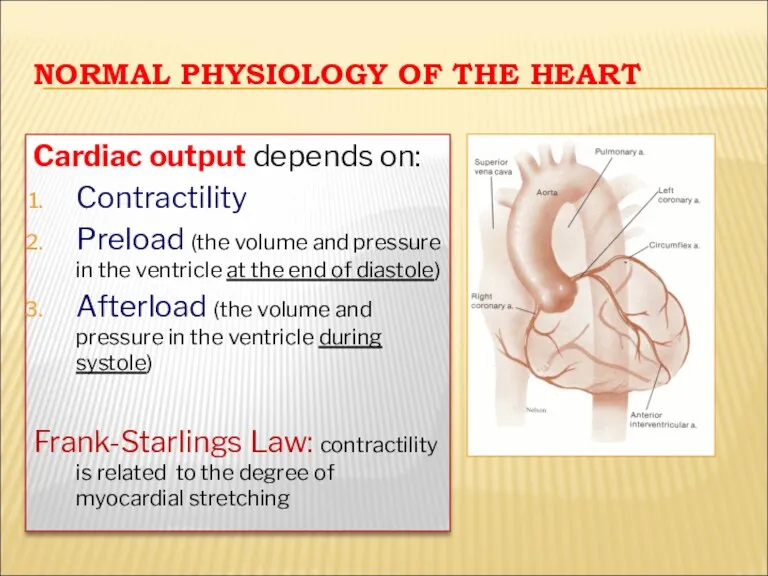
NORMAL PHYSIOLOGY OF THE HEART
Cardiac output depends on:
Contractility
Preload (the volume and
NORMAL PHYSIOLOGY OF THE HEART
Cardiac output depends on:
Contractility
Preload (the volume and
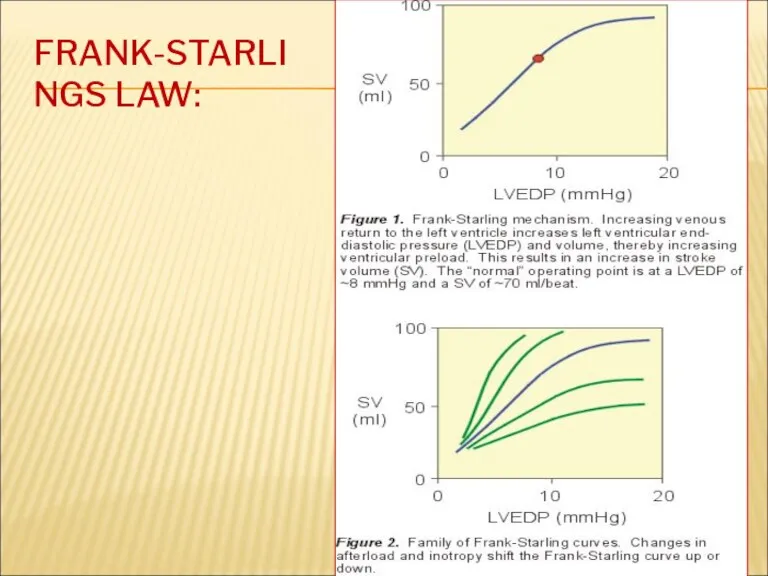
FRANK-STARLINGS LAW:
FRANK-STARLINGS LAW:
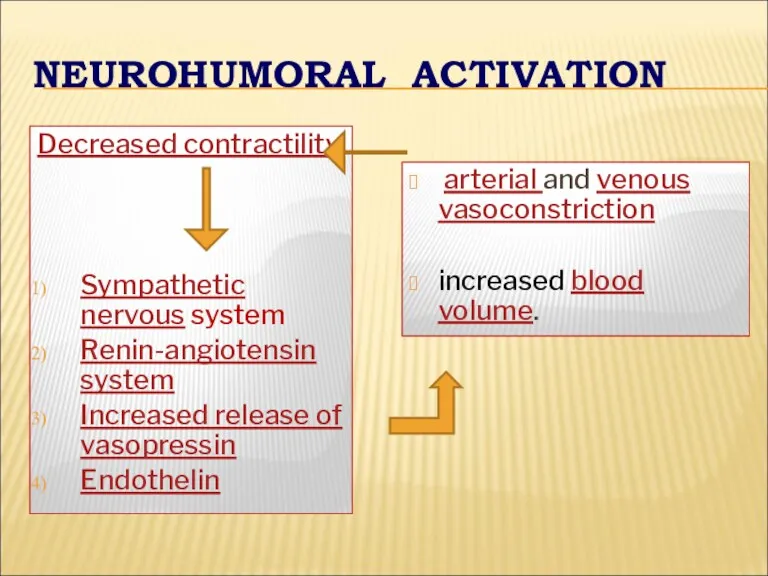
NEUROHUMORAL ACTIVATION
Decreased contractility
Sympathetic nervous system
Renin-angiotensin system
Increased release of vasopressin
Endothelin
NEUROHUMORAL ACTIVATION
Decreased contractility
Sympathetic nervous system
Renin-angiotensin system
Increased release of vasopressin
Endothelin
COMPENSATORY CHANGES IN HEART FAILURE
Activation of СNS
Activation of RAS
Increased heart rate
Release
COMPENSATORY CHANGES IN HEART FAILURE
Activation of СNS
Activation of RAS
Increased heart rate
Release
CLASSIFICATION
Heart failure can be classified in several ways 1 -
CLASSIFICATION
Heart failure can be classified in several ways 1 -
ACCF/AHA STAGES OF HF
Stage A: At high risk for HF
ACCF/AHA STAGES OF HF
Stage A: At high risk for HF
ESC GUIDELINES FOR DIAGNOSTIC AND TREATMENT OF ACUTE AND CHRONIC HF
ESC GUIDELINES FOR DIAGNOSTIC AND TREATMENT OF ACUTE AND CHRONIC HF
ESC GUIDELINES FOR DIAGNOSTIC AND TREATMENT OF ACUTE AND CHRONIC
ESC GUIDELINES FOR DIAGNOSTIC AND TREATMENT OF ACUTE AND CHRONIC
SYSTOLIC AND DIASTOLIC DYSFUNCTION
SYSTOLIC AND DIASTOLIC DYSFUNCTION
« FORWARD AND BACKWARD HF»
In some patients with HF the
« FORWARD AND BACKWARD HF»
In some patients with HF the
"HIGH OUTPUT CARDIAC FAILURE”
This can occur from:
Severe anemia,
Gram negative septicaemia,
"HIGH OUTPUT CARDIAC FAILURE”
This can occur from:
Severe anemia,
Gram negative septicaemia,
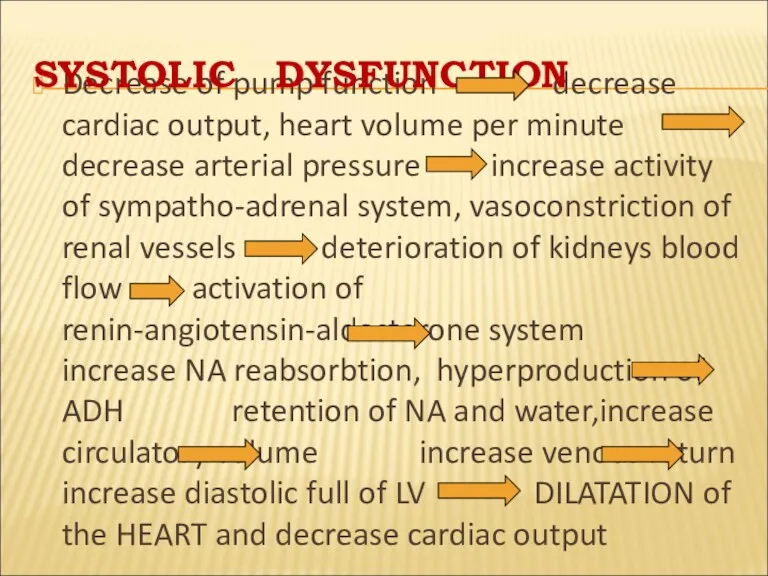
Decrease of pump function decrease cardiac output, heart volume per minute
Decrease of pump function decrease cardiac output, heart volume per minute
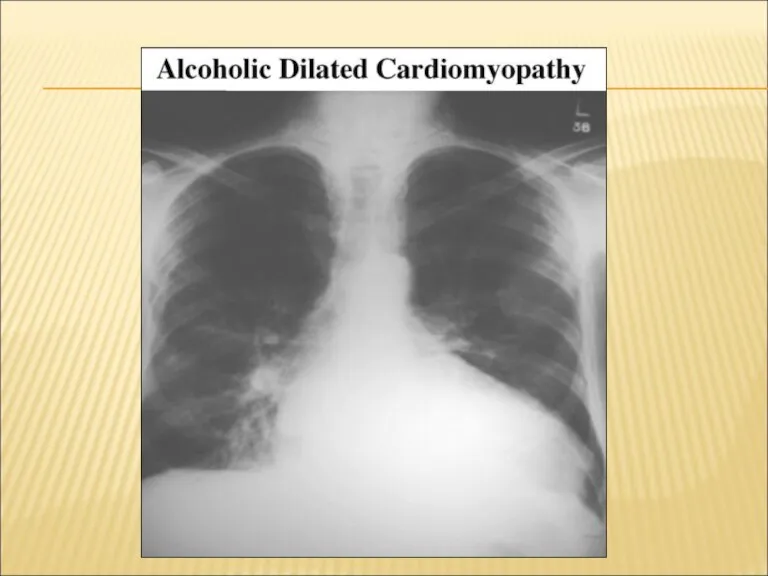
SYSTOLIC DYSFUNCTION
Coronary artery disease (CAD)
Dilated cardiomyopathy (DCMP)
Myocarditis
Anti-cancer drugs (doxorubicin) and
SYSTOLIC DYSFUNCTION
Coronary artery disease (CAD)
Dilated cardiomyopathy (DCMP)
Myocarditis
Anti-cancer drugs (doxorubicin) and
DIASTOLIC DYSFUNCTION
Constrictive pericarditis, cardiac tamponade
LV hypertrophy (hypertension)
Restrictive cardiomyopathy
DIASTOLIC DYSFUNCTION
Constrictive pericarditis, cardiac tamponade
LV hypertrophy (hypertension)
Restrictive cardiomyopathy
LEFT, RIGHT AND BIVENTRICULAR FAILURE
LEFT, RIGHT AND BIVENTRICULAR FAILURE
LEFT-SIDED FAILURE
Dyspnea and suffocation
Orthopnea
Paroxysmal nocturnal dyspnea
Peripheral cyanosis and coldness
Tiredness, weakness, anxiety
A
LEFT-SIDED FAILURE
Dyspnea and suffocation
Orthopnea
Paroxysmal nocturnal dyspnea
Peripheral cyanosis and coldness
Tiredness, weakness, anxiety
A
PERIPHERAL CYANOSIS
PERIPHERAL CYANOSIS
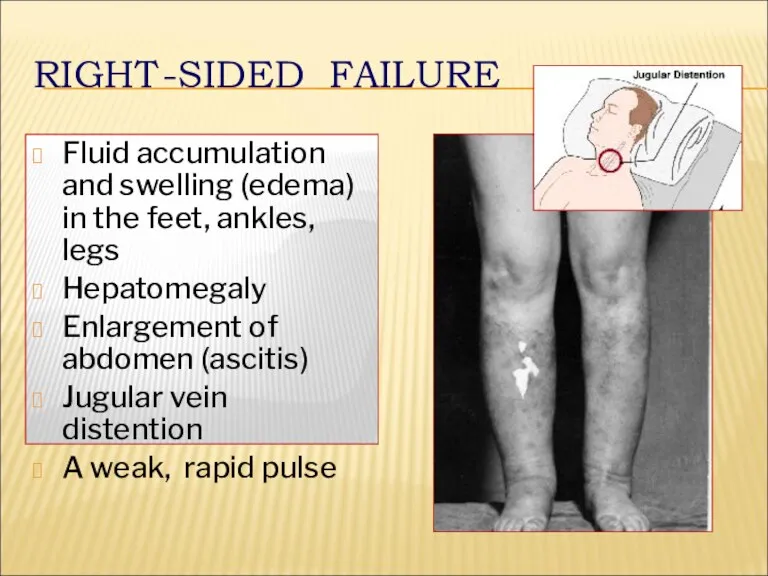
RIGHT-SIDED FAILURE
Fluid accumulation and swelling (edema) in the feet, ankles, legs
RIGHT-SIDED FAILURE
Fluid accumulation and swelling (edema) in the feet, ankles, legs
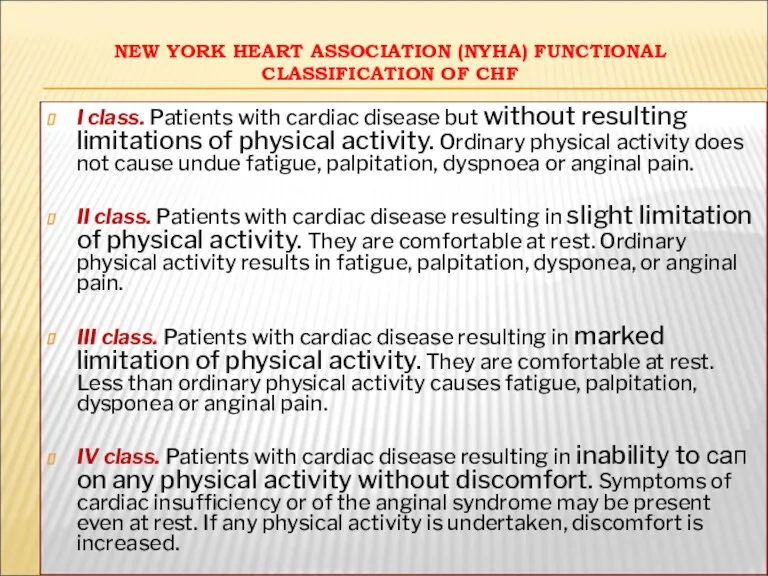
NEW YORK НЕАRT ASSOCIATION (NYHA) FUNCTIONAL CLASSIFICATION OF CHF
NEW YORK НЕАRT ASSOCIATION (NYHA) FUNCTIONAL CLASSIFICATION OF CHF
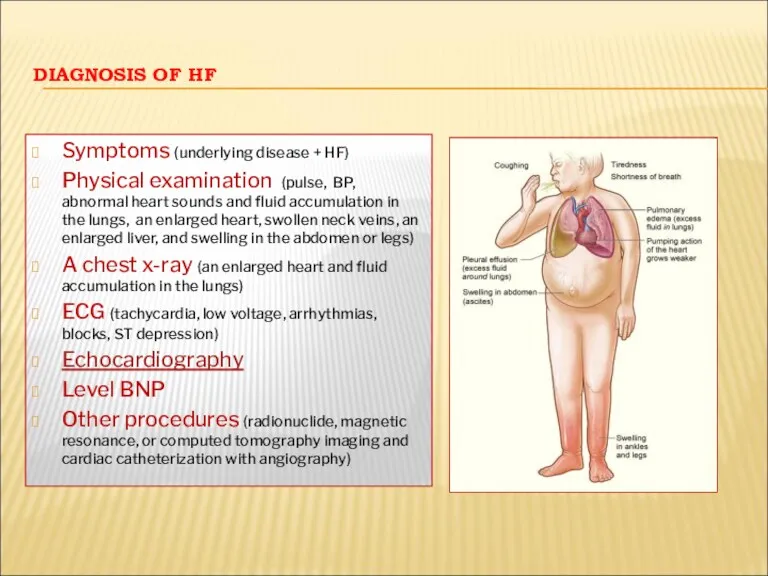
DIAGNOSIS OF HF
Symptoms (underlying disease + HF)
Physical examination (pulse, BP, abnormal
DIAGNOSIS OF HF
Symptoms (underlying disease + HF)
Physical examination (pulse, BP, abnormal
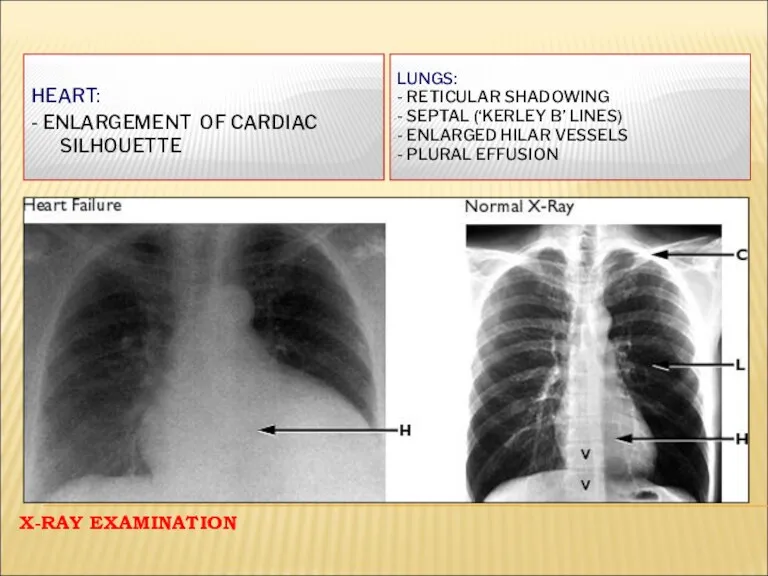
X-RAY EXAMINATION
LUNGS:
- RETICULAR SHADOWING
- SEPTAL (‘KERLEY B’ LINES)
- ENLARGED HILAR
X-RAY EXAMINATION
LUNGS:
- RETICULAR SHADOWING
- SEPTAL (‘KERLEY B’ LINES)
- ENLARGED HILAR
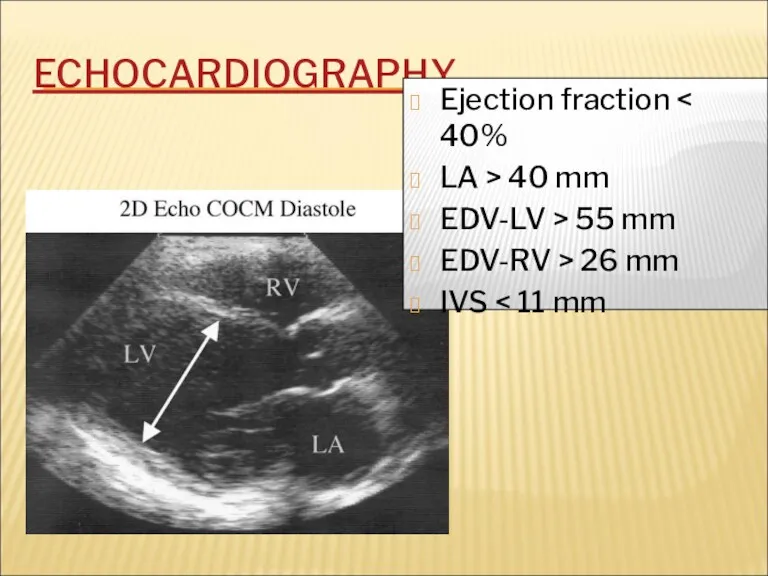
ECHOCARDIOGRAPHY
Ejection fraction < 40%
LA > 40 mm
EDV-LV > 55 mm
EDV-RV >
ECHOCARDIOGRAPHY
Ejection fraction < 40%
LA > 40 mm
EDV-LV > 55 mm
EDV-RV >
BLOOD TESTS
B-type natriuretic peptide (BNP) is a specific test indicative of
BLOOD TESTS
B-type natriuretic peptide (BNP) is a specific test indicative of
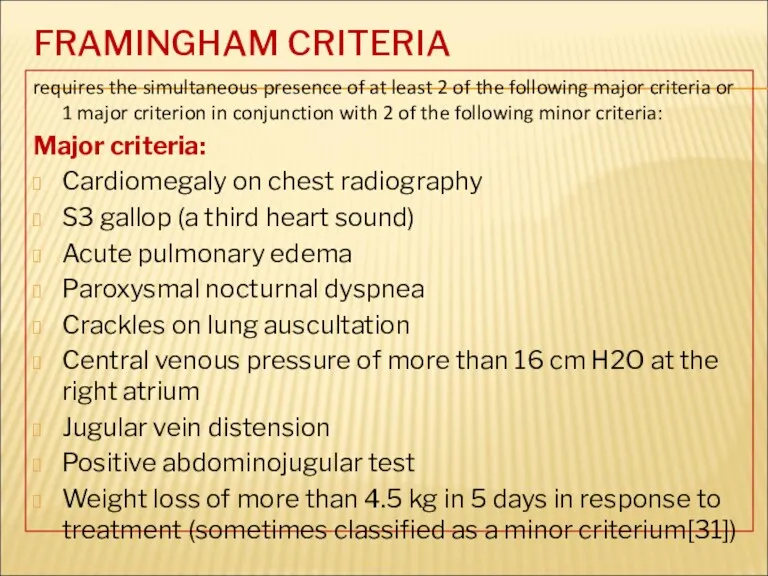
FRAMINGHAM CRITERIA
requires the simultaneous presence of at least 2 of the
FRAMINGHAM CRITERIA
requires the simultaneous presence of at least 2 of the
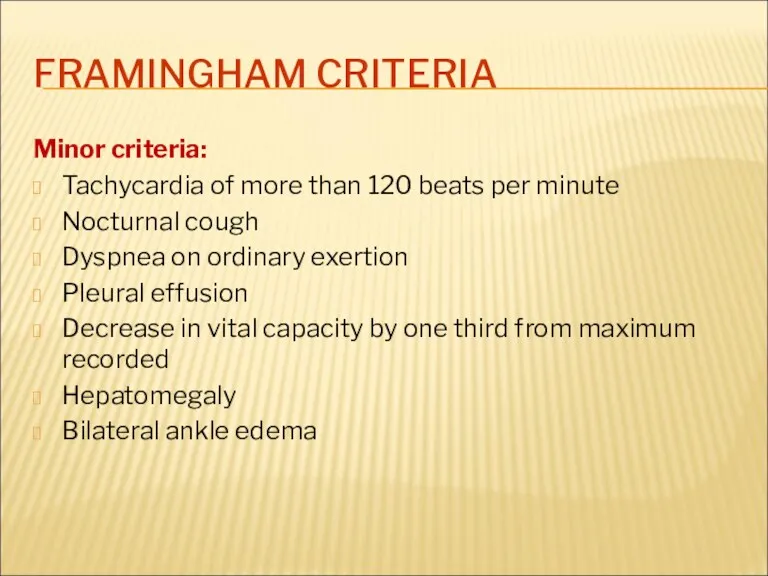
FRAMINGHAM CRITERIA
Minor criteria:
Tachycardia of more than 120 beats per minute
Nocturnal cough
Dyspnea
FRAMINGHAM CRITERIA
Minor criteria:
Tachycardia of more than 120 beats per minute
Nocturnal cough
Dyspnea
THE COURSE OF CHF
Symptoms of heart failure may begin suddenly, especially
THE COURSE OF CHF
Symptoms of heart failure may begin suddenly, especially
TREATMENT OF HEART FAILURE
Acute and chronic management strategies in heart failure
TREATMENT OF HEART FAILURE
Acute and chronic management strategies in heart failure
MANAGEMENT OF THE HEART FAILURE
The main purposes:
To reduce mortality
MANAGEMENT OF THE HEART FAILURE
The main purposes:
To reduce mortality
GOALS OF TREATMENT
To improve symptoms and quality of life
To
GOALS OF TREATMENT
To improve symptoms and quality of life
To
THE MAIN PRINCIPLES OF
HF MANAGEMENT
To reveal and exclude triggering factors
To
THE MAIN PRINCIPLES OF
HF MANAGEMENT
To reveal and exclude triggering factors
To
METHODS OF HF MANAGEMENT
Non-medical (changing lifestyle)
Pharmacotherapy (ACE inhibitors or ARBs, beta-blockers,
METHODS OF HF MANAGEMENT
Non-medical (changing lifestyle)
Pharmacotherapy (ACE inhibitors or ARBs, beta-blockers,
PHARMACOTHERAPY FOR HF
1 DRUGS PROVED TO BE ABLE TO REDUCE MORBIDITY
PHARMACOTHERAPY FOR HF
1 DRUGS PROVED TO BE ABLE TO REDUCE MORBIDITY
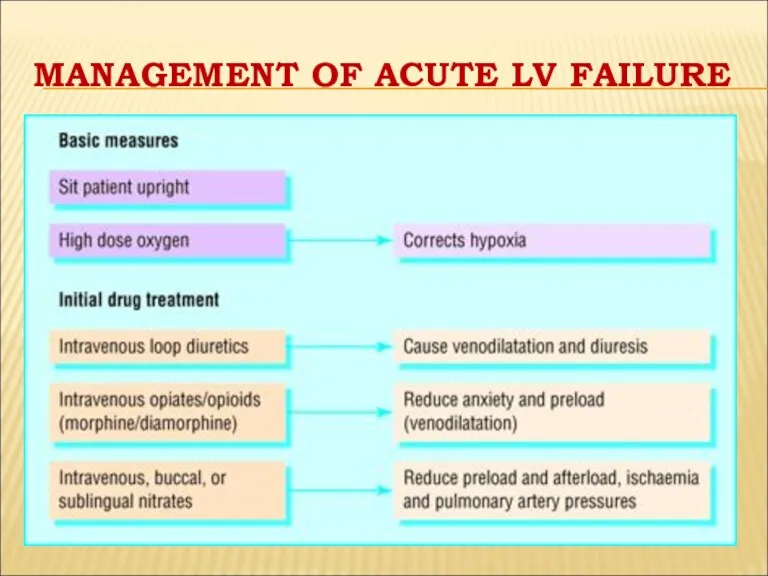
MANAGEMENT OF ACUTE LV FAILURE
MANAGEMENT OF ACUTE LV FAILURE
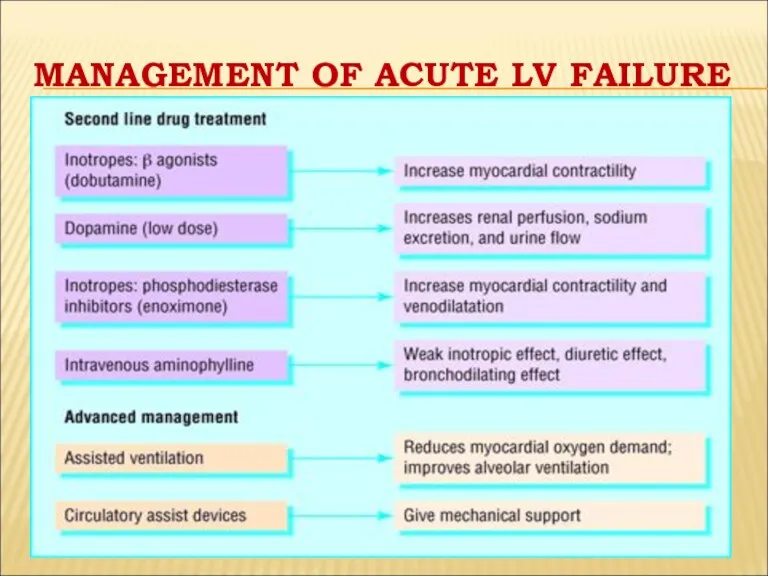
MANAGEMENT OF ACUTE LV FAILURE
MANAGEMENT OF ACUTE LV FAILURE
GENERAL MANAGEMENT OF CHRONIC HF
Education of patient and relatives
Diet: decrease of
GENERAL MANAGEMENT OF CHRONIC HF
Education of patient and relatives
Diet: decrease of
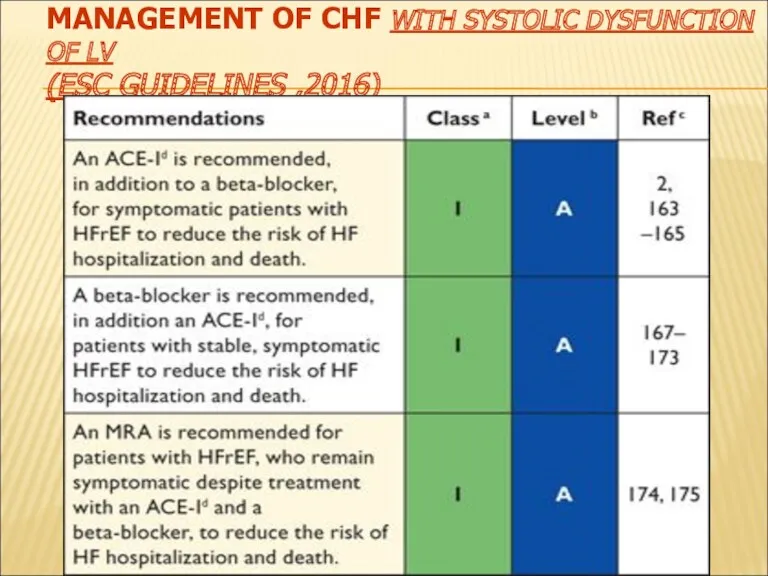
MANAGEMENT OF CHF WITH SYSTOLIC DYSFUNCTION OF LV
(ESC GUIDELINES ,2016)
MANAGEMENT OF CHF WITH SYSTOLIC DYSFUNCTION OF LV
(ESC GUIDELINES ,2016)
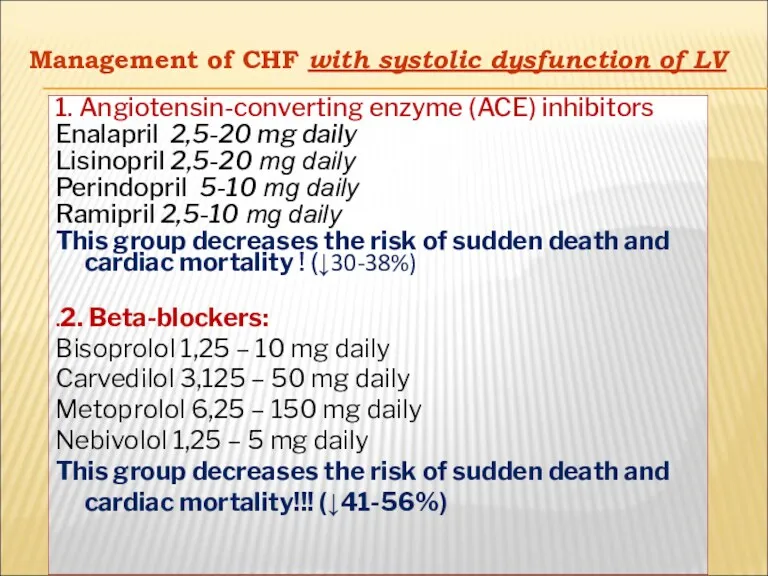
Management of CHF with systolic dysfunction of LV
Management of CHF with systolic dysfunction of LV
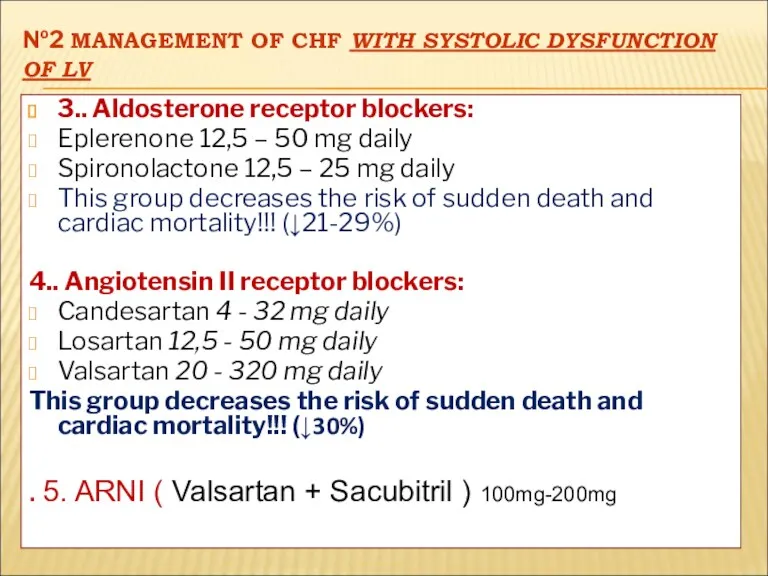
№2 MANAGEMENT OF CHF WITH SYSTOLIC DYSFUNCTION OF LV
3.. Aldosterone receptor
№2 MANAGEMENT OF CHF WITH SYSTOLIC DYSFUNCTION OF LV
3.. Aldosterone receptor
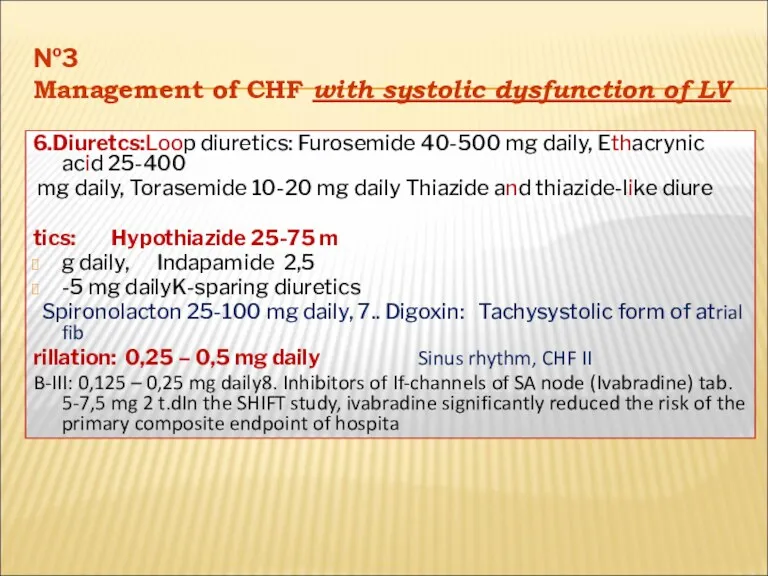
№3
Management of CHF with systolic dysfunction of LV
6.Diuretcs:Loop diuretics: Furosemide 40-500
№3
Management of CHF with systolic dysfunction of LV
6.Diuretcs:Loop diuretics: Furosemide 40-500
ADDITIONAL DRUGS
Anti-aggregants: aspirin (100-300 mg daily)
Anti-coagulants: warfarin (3-9 mg daily)
Statins: atorvastatin
ADDITIONAL DRUGS
Anti-aggregants: aspirin (100-300 mg daily)
Anti-coagulants: warfarin (3-9 mg daily)
Statins: atorvastatin
MANAGEMENT OF CHF WITH NORMAL SYSTOLIC FUNCTION OF LV
Main group:
Angiotensin-converting enzyme
MANAGEMENT OF CHF WITH NORMAL SYSTOLIC FUNCTION OF LV
Main group:
Angiotensin-converting enzyme
SURGICAL TREATMENT
The following procedures decrease the risk of sudden death and
SURGICAL TREATMENT
The following procedures decrease the risk of sudden death and
 Dental clinic
Dental clinic Воспаление. Этиологические факторы воспаления
Воспаление. Этиологические факторы воспаления Первая помощь при растяжении связок, вывихах суставов, переломах костей
Первая помощь при растяжении связок, вывихах суставов, переломах костей Тромбоз подключичной вены
Тромбоз подключичной вены Введение в пропедевтику внутренних болезней
Введение в пропедевтику внутренних болезней Дифференциальный диагноз анемий
Дифференциальный диагноз анемий Эндодонтиялық тәжірибеде лазерлі сәулені қолдан
Эндодонтиялық тәжірибеде лазерлі сәулені қолдан Введение в психиатрию, предмет, задачи, основные направления развития психиатрии
Введение в психиатрию, предмет, задачи, основные направления развития психиатрии Предраковые процессы
Предраковые процессы Психология детей с расстройствами эмоционально-волевой сферы и поведения
Психология детей с расстройствами эмоционально-волевой сферы и поведения Збудники анаеробних інфекцій
Збудники анаеробних інфекцій Неправильные положения плода (поперечное, косое). Причины. Диагностика. Ведение беременности и родов
Неправильные положения плода (поперечное, косое). Причины. Диагностика. Ведение беременности и родов Медициналық психология
Медициналық психология Современные методы фармацевтического анализа
Современные методы фармацевтического анализа Цитология (биология клетки)
Цитология (биология клетки) Питание детей с муковисцидозом
Питание детей с муковисцидозом Сальмонеллез у кошек и собак
Сальмонеллез у кошек и собак Лечение отеков до появления диуретиков
Лечение отеков до появления диуретиков Теміртапшылықты анемия
Теміртапшылықты анемия Сүйек кемігі
Сүйек кемігі Менингококковая инфекция
Менингококковая инфекция Коронарлық жеткіліксіздік
Коронарлық жеткіліксіздік Роль иммунной системы при беременности
Роль иммунной системы при беременности Теория и организация адаптивной физической культуры
Теория и организация адаптивной физической культуры Синдром поражения миокарда
Синдром поражения миокарда Мышечная система. Скелетные мышцы
Мышечная система. Скелетные мышцы Методы определения центрального соотношения челюстей в стоматологии
Методы определения центрального соотношения челюстей в стоматологии The body’s defenses. Types of acquired immunity
The body’s defenses. Types of acquired immunity