- Heart pathology. (Subject 13)

Содержание
- 2. Lecture Plan Signs and symptoms of MI Cardiogenic shock Arrhythmia classification Characteristic of arrhythmia’s types
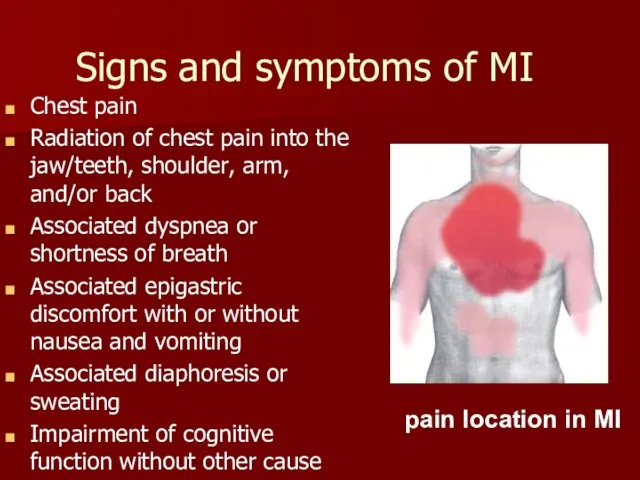
- 3. Signs and symptoms of MI Chest pain Radiation of chest pain into the jaw/teeth, shoulder, arm,
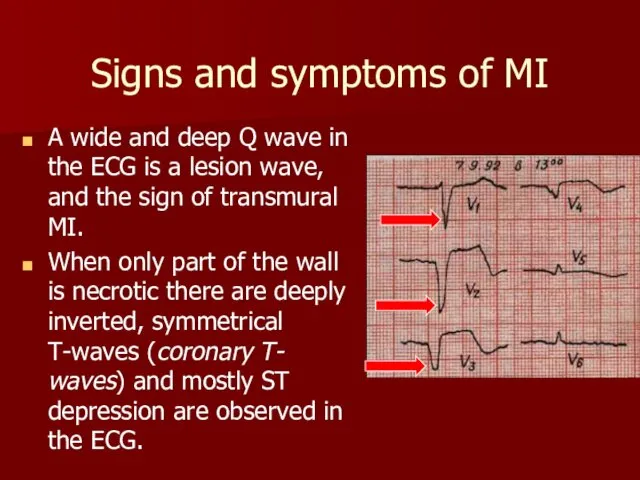
- 4. Signs and symptoms of MI A wide and deep Q wave in the ECG is a
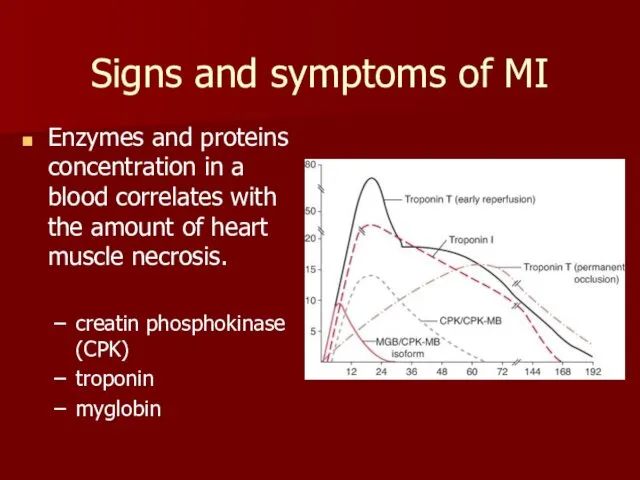
- 5. Signs and symptoms of MI Enzymes and proteins concentration in a blood correlates with the amount
- 6. Reperfusion of MI circulation brings neutrophils to re-perfused tissues that release toxic oxygen radicals and cytokines
- 7. Cardiogenic shock Cardiogenic shock is a severe reduction of cardiac output The pulmonary capillary wedge pressure
- 8. Cardiogenic shock symptoms Anxiety, restlessness, altered mental state Hypotension A rapid, weak, thready pulse Cool, clammy,
- 9. Arrhythmia classification
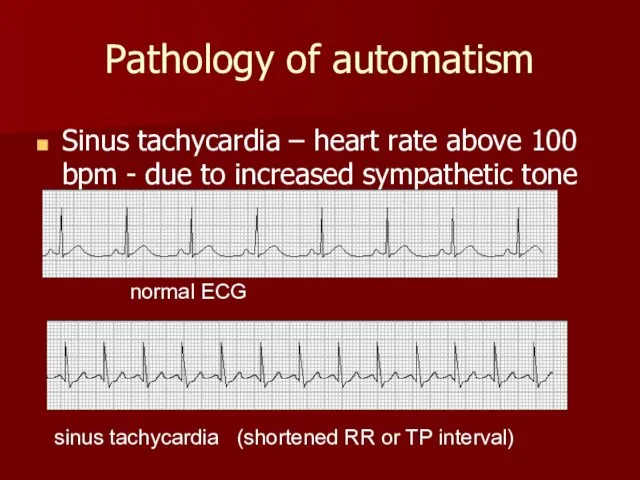
- 10. Pathology of automatism Sinus tachycardia – heart rate above 100 bpm - due to increased sympathetic
- 11. Pathology of automatism Sinus bradycardia – less than 60 bpm due to decreased sympathetic and increased
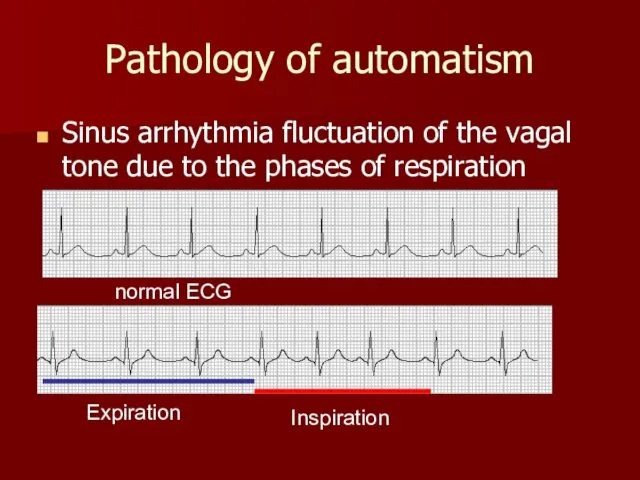
- 12. Pathology of automatism Sinus arrhythmia fluctuation of the vagal tone due to the phases of respiration
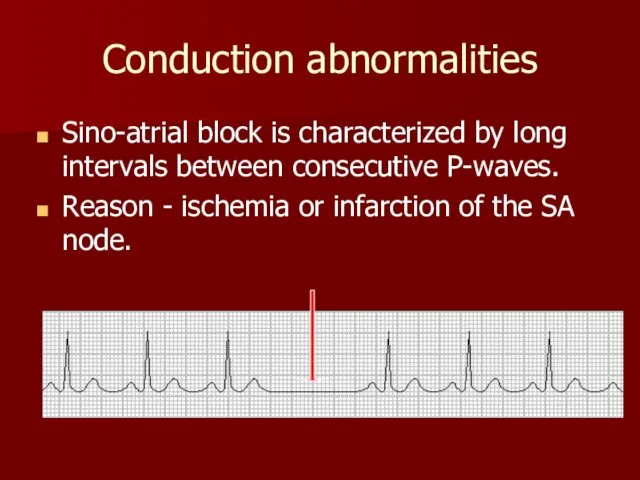
- 13. Conduction abnormalities Sino-atrial block is characterized by long intervals between consecutive P-waves. Reason - ischemia or
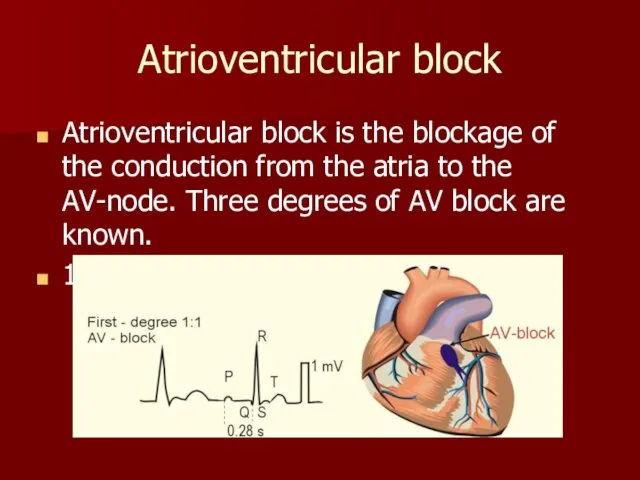
- 14. Atrioventricular block Atrioventricular block is the blockage of the conduction from the atria to the AV-node.
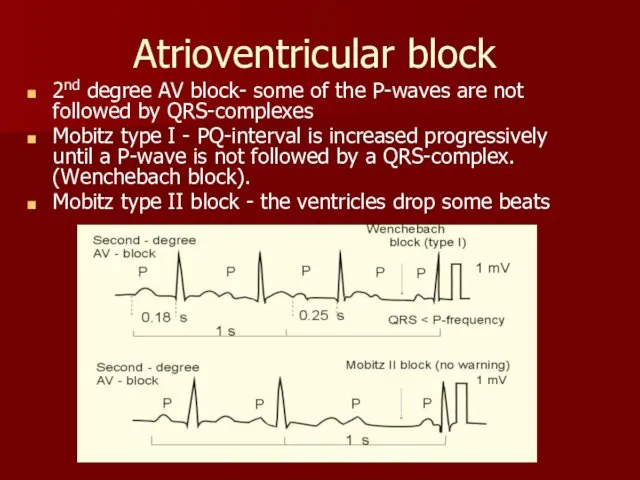
- 15. Atrioventricular block 2nd degree AV block- some of the P-waves are not followed by QRS-complexes Mobitz
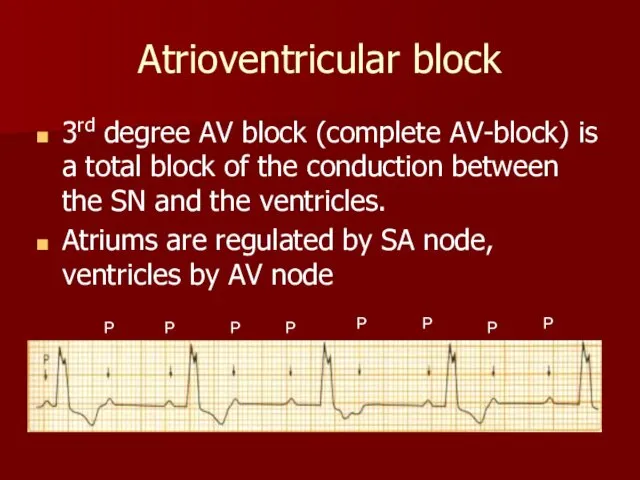
- 16. Atrioventricular block 3rd degree AV block (complete AV-block) is a total block of the conduction between
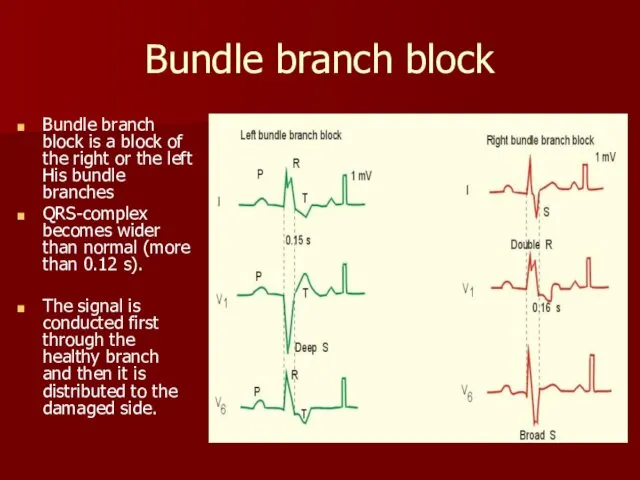
- 17. Bundle branch block Bundle branch block is a block of the right or the left His
- 18. Pathology of excitability Pathology of excitability is usually manifested with ectopic beats (outside the sinus node).
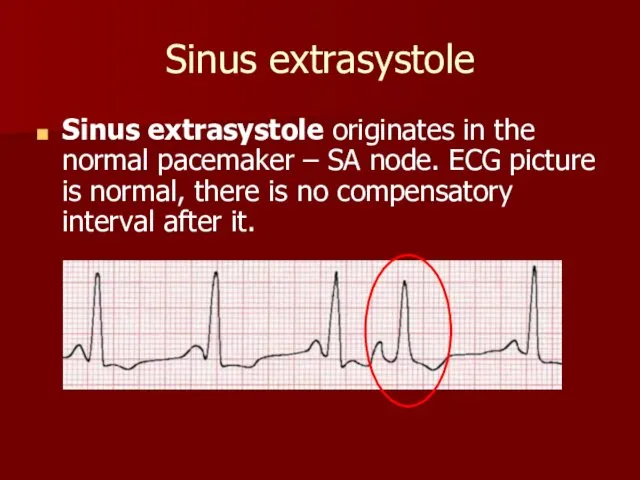
- 19. Sinus extrasystole Sinus extrasystole originates in the normal pacemaker – SA node. ECG picture is normal,
- 20. Atrial ectopic beat Atrial ectopic beats have abnormal P-waves and are usually followed by normal QRS-complexes.
- 21. Premature junctional contractions Ectopic beat originate in the atrio-ventricular node. P-wave is negative Compensatory interval a
- 22. Ventricular ectopic beat wide QRS-complex (above 0.12 s), long compensatory interval (2RR)
- 23. Paroxysmal ectopic tachycardia Paroxysmal atrial tachycardia is elicited in the atrial tissue outside the SA node
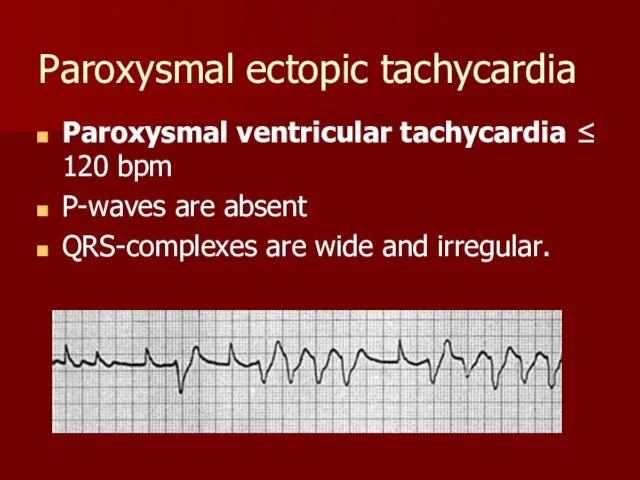
- 24. Paroxysmal ectopic tachycardia Paroxysmal ventricular tachycardia ≤ 120 bpm P-waves are absent QRS-complexes are wide and
- 25. Disorders of hemodynamic in the pathology of excitability Single extrasystole clinically manifests in the feeling of
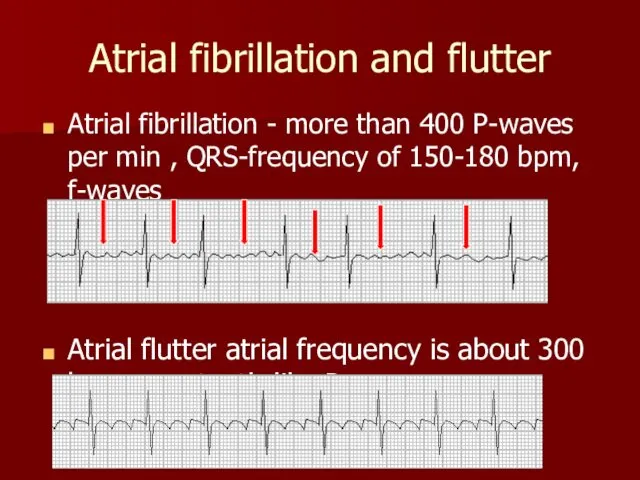
- 26. Atrial fibrillation and flutter Atrial fibrillation - more than 400 P-waves per min , QRS-frequency of
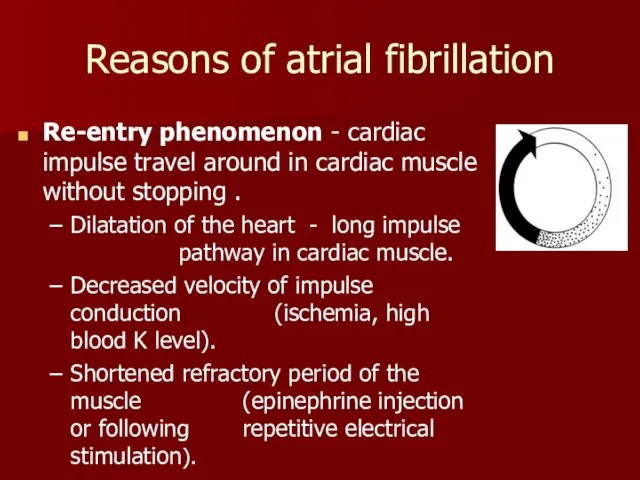
- 27. Reasons of atrial fibrillation Re-entry phenomenon - cardiac impulse travel around in cardiac muscle without stopping
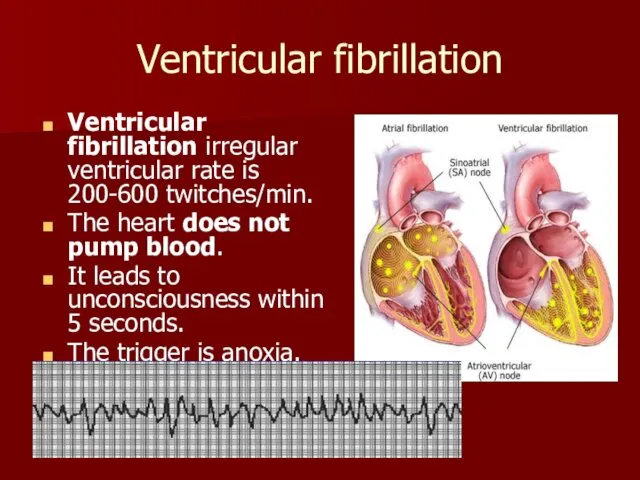
- 28. Ventricular fibrillation Ventricular fibrillation irregular ventricular rate is 200-600 twitches/min. The heart does not pump blood.
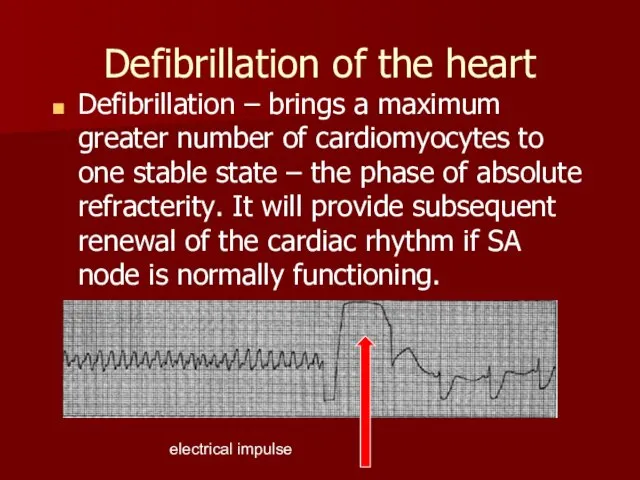
- 29. Defibrillation of the heart Defibrillation – brings a maximum greater number of cardiomyocytes to one stable
- 31. Скачать презентацию
Lecture Plan
Signs and symptoms of MI
Cardiogenic shock
Arrhythmia classification
Characteristic of arrhythmia’s types
Lecture Plan
Signs and symptoms of MI
Cardiogenic shock
Arrhythmia classification
Characteristic of arrhythmia’s types
Signs and symptoms of MI
Chest pain
Radiation of chest pain into the
Signs and symptoms of MI
Chest pain
Radiation of chest pain into the
Signs and symptoms of MI
A wide and deep Q wave in
Signs and symptoms of MI
A wide and deep Q wave in
Signs and symptoms of MI
Enzymes and proteins concentration in a blood
Signs and symptoms of MI
Enzymes and proteins concentration in a blood
Reperfusion of MI
circulation brings neutrophils to re-perfused tissues that release
Reperfusion of MI
circulation brings neutrophils to re-perfused tissues that release
Cardiogenic shock
Cardiogenic shock is a severe reduction of cardiac output
Cardiogenic shock
Cardiogenic shock is a severe reduction of cardiac output

Cardiogenic shock symptoms
Anxiety, restlessness, altered mental state
Hypotension
A rapid, weak, thready pulse
Cardiogenic shock symptoms
Anxiety, restlessness, altered mental state
Hypotension
A rapid, weak, thready pulse
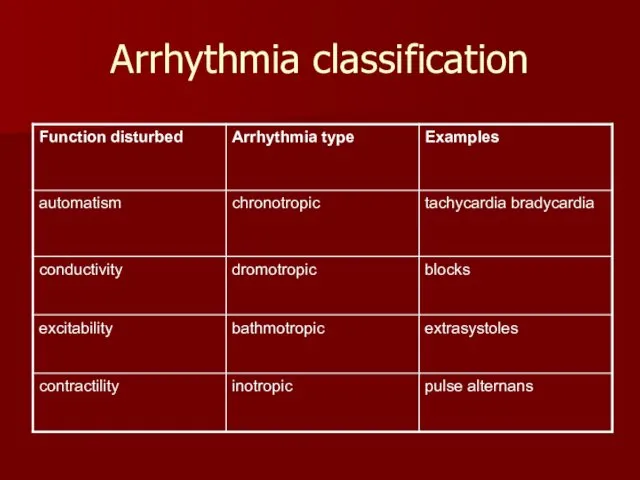
Arrhythmia classification
Arrhythmia classification
Pathology of automatism
Sinus tachycardia – heart rate above 100 bpm
Pathology of automatism
Sinus tachycardia – heart rate above 100 bpm

Pathology of automatism
Sinus bradycardia – less than 60 bpm due
Pathology of automatism
Sinus bradycardia – less than 60 bpm due
Pathology of automatism
Sinus arrhythmia fluctuation of the vagal tone due to
Pathology of automatism
Sinus arrhythmia fluctuation of the vagal tone due to
Conduction abnormalities
Sino-atrial block is characterized by long intervals between consecutive
Conduction abnormalities
Sino-atrial block is characterized by long intervals between consecutive
Atrioventricular block
Atrioventricular block is the blockage of the conduction from the
Atrioventricular block
Atrioventricular block is the blockage of the conduction from the
Atrioventricular block
2nd degree AV block- some of the P-waves are not
Atrioventricular block
2nd degree AV block- some of the P-waves are not
Atrioventricular block
3rd degree AV block (complete AV-block) is a total block
Atrioventricular block
3rd degree AV block (complete AV-block) is a total block
Bundle branch block
Bundle branch block is a block of the
Bundle branch block
Bundle branch block is a block of the
Pathology of excitability
Pathology of excitability is usually manifested with ectopic
Pathology of excitability
Pathology of excitability is usually manifested with ectopic
Sinus extrasystole
Sinus extrasystole originates in the normal pacemaker – SA
Sinus extrasystole
Sinus extrasystole originates in the normal pacemaker – SA
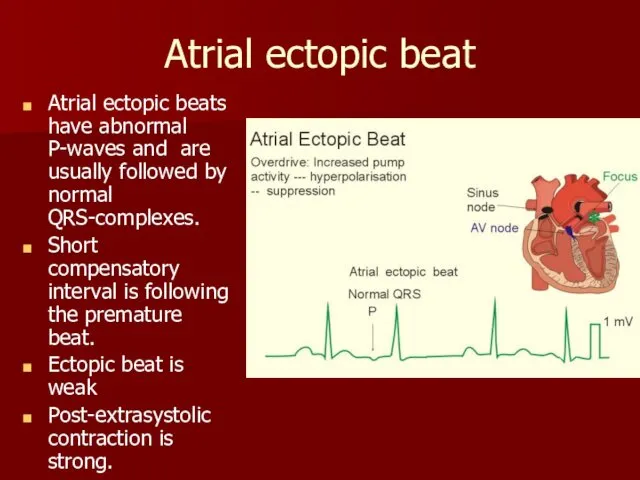
Atrial ectopic beat
Atrial ectopic beats have abnormal P-waves and are
Atrial ectopic beat
Atrial ectopic beats have abnormal P-waves and are

Premature junctional contractions
Ectopic beat originate in the atrio-ventricular node.
P-wave is
Premature junctional contractions
Ectopic beat originate in the atrio-ventricular node.
P-wave is
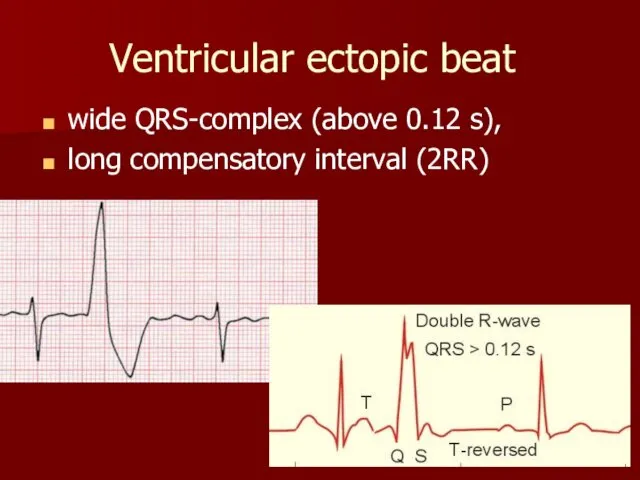
Ventricular ectopic beat
wide QRS-complex (above 0.12 s),
long compensatory interval
Ventricular ectopic beat
wide QRS-complex (above 0.12 s),
long compensatory interval

Paroxysmal ectopic tachycardia
Paroxysmal atrial tachycardia is elicited in the atrial
Paroxysmal ectopic tachycardia
Paroxysmal atrial tachycardia is elicited in the atrial
Paroxysmal ectopic tachycardia
Paroxysmal ventricular tachycardia ≤ 120 bpm
P-waves are absent
QRS-complexes are
Paroxysmal ectopic tachycardia
Paroxysmal ventricular tachycardia ≤ 120 bpm
P-waves are absent
QRS-complexes are
Disorders of hemodynamic in the pathology of excitability
Single extrasystole clinically manifests
Disorders of hemodynamic in the pathology of excitability
Single extrasystole clinically manifests
Atrial fibrillation and flutter
Atrial fibrillation - more than 400 P-waves per
Atrial fibrillation and flutter
Atrial fibrillation - more than 400 P-waves per
Reasons of atrial fibrillation
Re-entry phenomenon - cardiac impulse travel around in
Reasons of atrial fibrillation
Re-entry phenomenon - cardiac impulse travel around in
Ventricular fibrillation
Ventricular fibrillation irregular ventricular rate is 200-600 twitches/min.
The heart
Ventricular fibrillation
Ventricular fibrillation irregular ventricular rate is 200-600 twitches/min.
The heart
Defibrillation of the heart
Defibrillation – brings a maximum greater number of
Defibrillation of the heart
Defibrillation – brings a maximum greater number of
 Теоретические основы фармацевтической информации. Документальные источники информации
Теоретические основы фармацевтической информации. Документальные источники информации Вторичные иммунодефициты
Вторичные иммунодефициты Влияние приобретенного дальтонизма на социальную адаптацию (социализацию) молодежи в России
Влияние приобретенного дальтонизма на социальную адаптацию (социализацию) молодежи в России Өкпенің интерстициалды аурулары. Пневмофиброз. Патанатомиясы, ақыры
Өкпенің интерстициалды аурулары. Пневмофиброз. Патанатомиясы, ақыры Пищевые отравления и их профилактика
Пищевые отравления и их профилактика Особенности культуры и медицины Древней Греции и Древнего Рима. Роль Гиппократа. Лекция 4
Особенности культуры и медицины Древней Греции и Древнего Рима. Роль Гиппократа. Лекция 4 Асфиксии новорождённых
Асфиксии новорождённых Пароксизмальды жағдай. Шұғыл көмек көрсету. Дифференциальды диагностикасы
Пароксизмальды жағдай. Шұғыл көмек көрсету. Дифференциальды диагностикасы Эхокардиография (УЗИ) сердца
Эхокардиография (УЗИ) сердца Безгек. Этиологиясы
Безгек. Этиологиясы Структура детской городской клинической поликлиники
Структура детской городской клинической поликлиники хейлиты дерма
хейлиты дерма Кора головного мозга. Симптомы поражения
Кора головного мозга. Симптомы поражения Электротерапия постоянным импульсным током
Электротерапия постоянным импульсным током Эндокринная система. Общие свойства и функции. Лекция № 17
Эндокринная система. Общие свойства и функции. Лекция № 17 Общие вопросы стоматологии. Организация работы врача - стоматолога-терапевта
Общие вопросы стоматологии. Организация работы врача - стоматолога-терапевта Паразитические черви
Паразитические черви Шигельоз
Шигельоз СП при острой сердечной недостаточности
СП при острой сердечной недостаточности Дисграфия. Диагностика и коррекция
Дисграфия. Диагностика и коррекция Клінічна фармація в ревматології (І)
Клінічна фармація в ревматології (І) Анықталмаған қызбаның дифференциалды диагностикасы
Анықталмаған қызбаның дифференциалды диагностикасы Основы организации обеспечения медицинским имуществом и техникой
Основы организации обеспечения медицинским имуществом и техникой Медицинская и психосоциальная реабилитация при отдельных болезнях у детей. Цели и задачи паллиативной помощи
Медицинская и психосоциальная реабилитация при отдельных болезнях у детей. Цели и задачи паллиативной помощи Атеросклероз
Атеросклероз Заболевания щитовидной железы. Этиопатогенез
Заболевания щитовидной железы. Этиопатогенез Методы лечения психофармакотерапии с позиции доказательной медицины
Методы лечения психофармакотерапии с позиции доказательной медицины Тұқым қуалайтын ауруларды емдеу принциптері
Тұқым қуалайтын ауруларды емдеу принциптері