- Human immunodeficiency virus

Содержание
- 2. Plan of lecture Overview Etiology Epidemiology Pathogenesis Manifestations Diagnosis Therapy and Prevention
- 3. Human Immunodeficiency Virus
- 4. The first indication of new disease – Acquired Immunodificiency Syndrom (AIDS) began in the summer of
- 6. Pneumocystis carinii
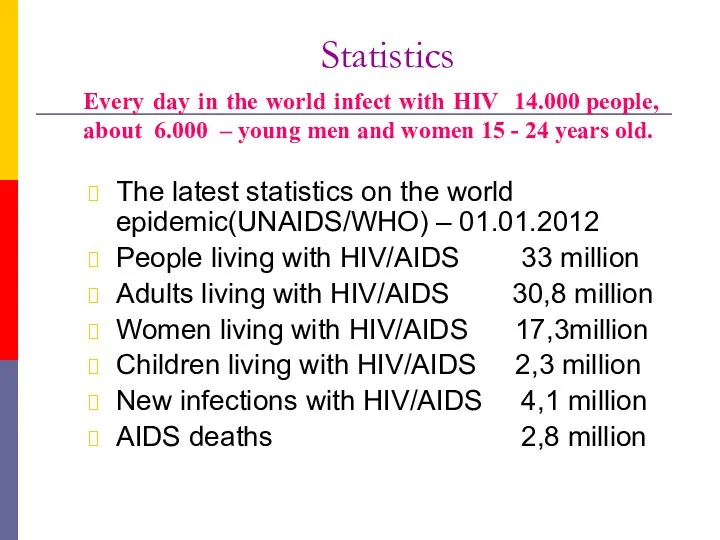
- 7. Statistics The latest statistics on the world epidemic(UNAIDS/WHO) – 01.01.2012 People living with HIV/AIDS 33 million
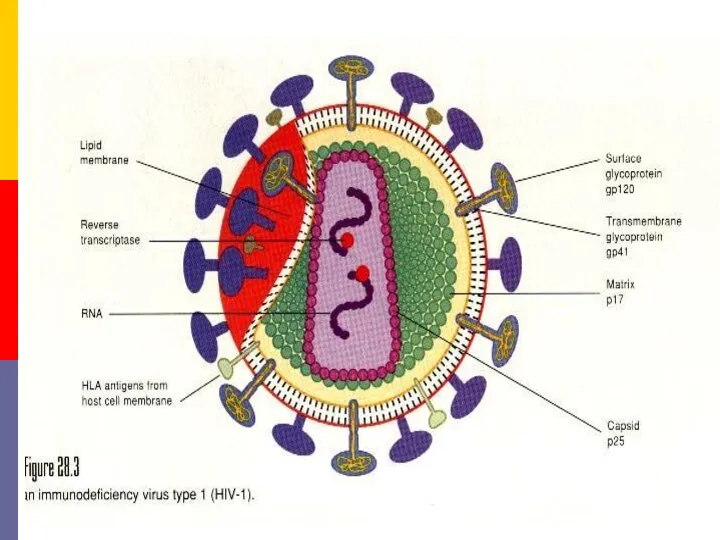
- 8. HIV, the etiologjcal agent of AIDS, belongs to the lentivirus subgroup of the family Retroviridae. Structure.
- 10. Types of HIV Virus HIV 1 Most common in sub-Saharan Africa and throughout the world Groups
- 11. Viral genes and antigens. The genome of HIV contains the three structural genes (gag, pol and
- 12. Pathogenesis. The receptor for the virus is the CD4 antigen and therefore the virus may infect
- 13. Specific binding of the virus to CD4 is by the envelope glycoprotein gp120. However, for infection
- 14. In an infected individual, HIV can be isolated from the blood, lymphocytes, cell free plasma, semen,
- 15. The primary pathogenic mechanism in HIV infection is the damage caused to the T4 lymphocyte. The
- 16. Window Period Time from initial infection with HIV until antibodies are detected by a single test
- 17. Disease Progression Severity of illness is determined by amount of virus in the body (increasing viral
- 18. What body fluid transmit HIV? blood semen vaginal fluid breast milk
- 19. AIDS is primarily a sexually transmitted infection. In the USA it was transmitted predominantly among male
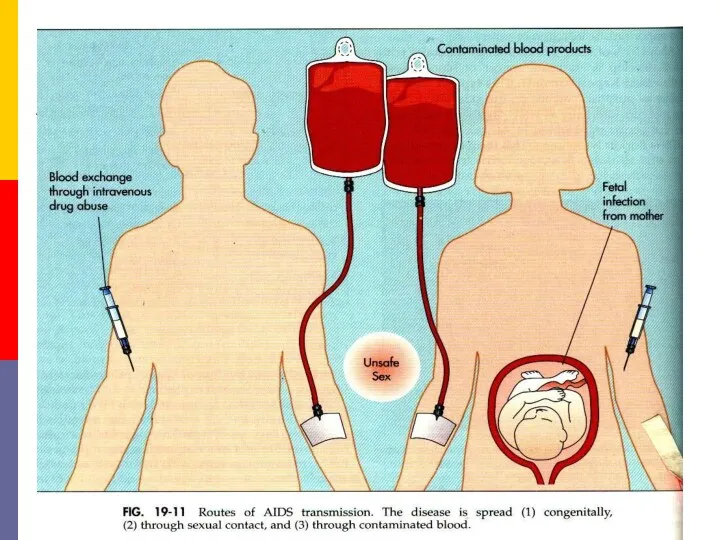
- 21. The second mode of transmission is through blood and blood products. Before the danger of HIV
- 23. This restriction also applies to the donation of semen, cornea, bone marrow, kidney and other organs
- 24. Contaminated needles can transmit the infection. This is particularly relevant in drug addicts who share syringes
- 26. The danger of needlestick injury is present in medical and paramedical personnel, though the chances of
- 27. Transmission of infection from mother to baby can take place before, during or after birth. As
- 28. Normal social and domestic contact does not transmit the infection. Shaking hands, hugging, putting cheeks together
- 30. ACQUIRED DEFICIENCY SYNDROME (AIDS) Clinical features of HIV infection. AIDS is only the last stage in
- 31. Acute HIV infection. Within a few weeks of infection with HIV, about 10-15 per cent of
- 32. Asymptomatic infection. All persons infected with HIV, whether they experience seroconversion illness or not, pass through
- 33. Persistant Generalised Liphadenopathy (PGL). This has been defined as the presence of enlarged lymph nodes, at
- 34. AIDS Related Complex (ARC). This group inc1udes patients with considerable immunodeficiency, suffering from various constitutional symptoms
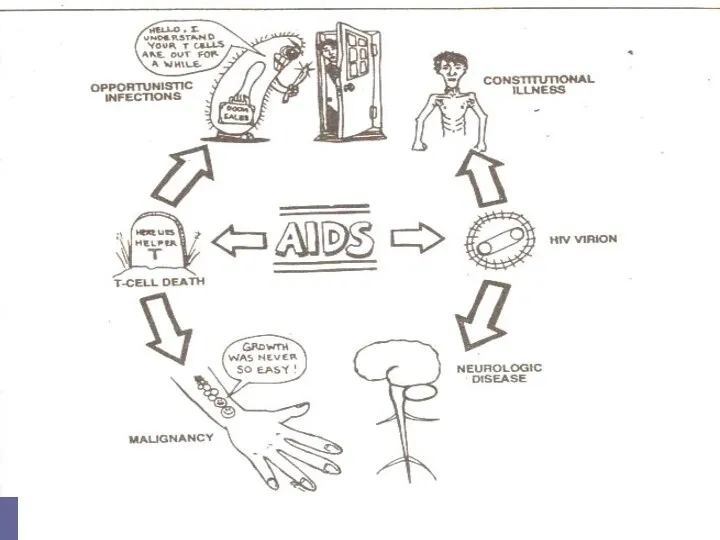
- 35. AIDS. This is the end stage disease representing the irreversible breakdown of immune defense mechanisms, leaving
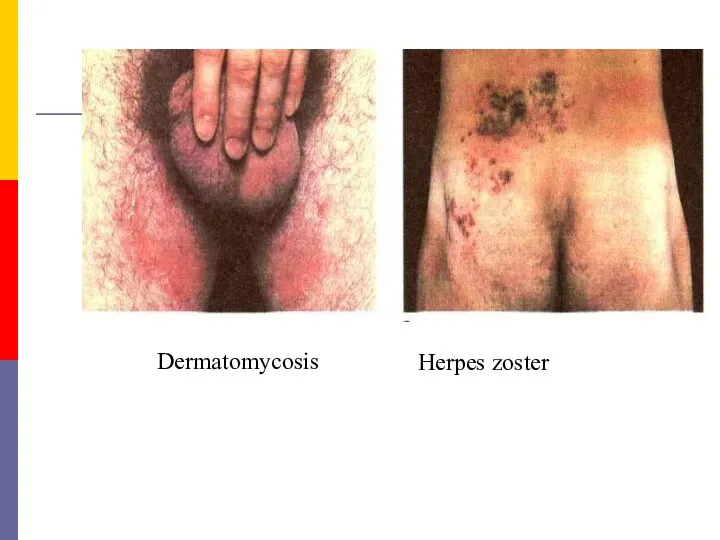
- 36. Dermatomycosis Herpes zoster
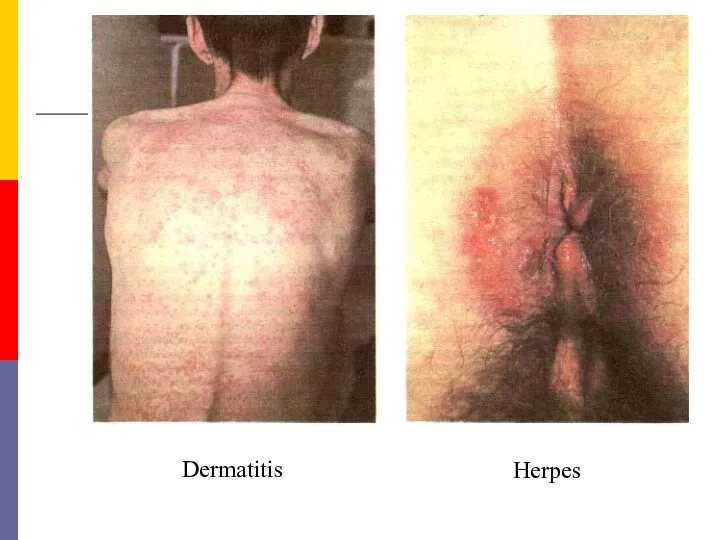
- 37. Dermatitis Herpes
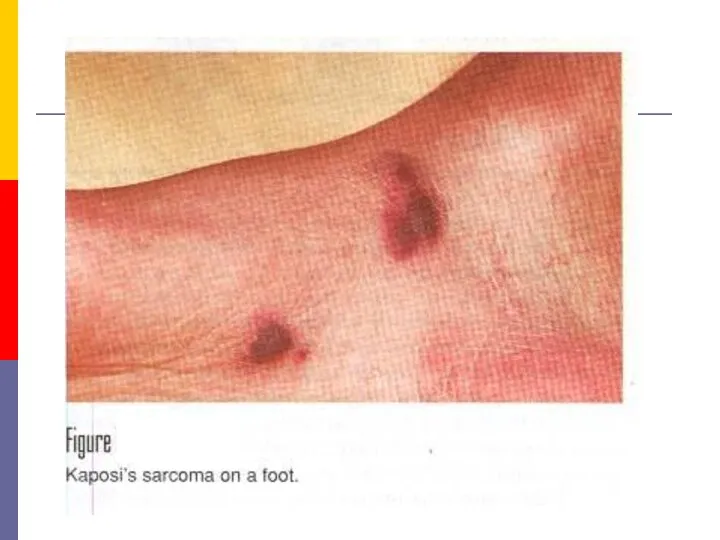
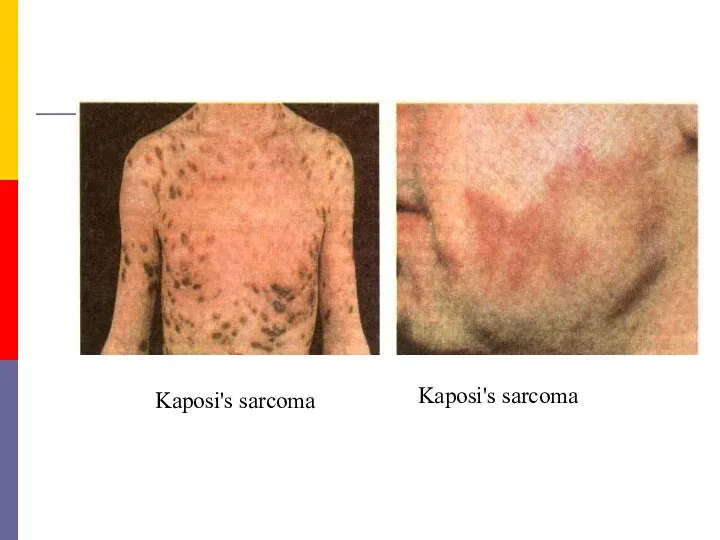
- 38. Kaposi's sarcoma Kaposi's sarcoma
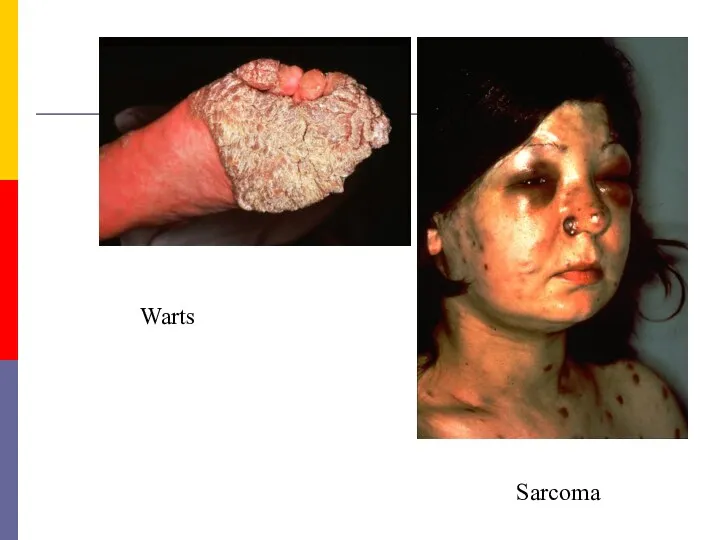
- 40. Warts Sarcoma
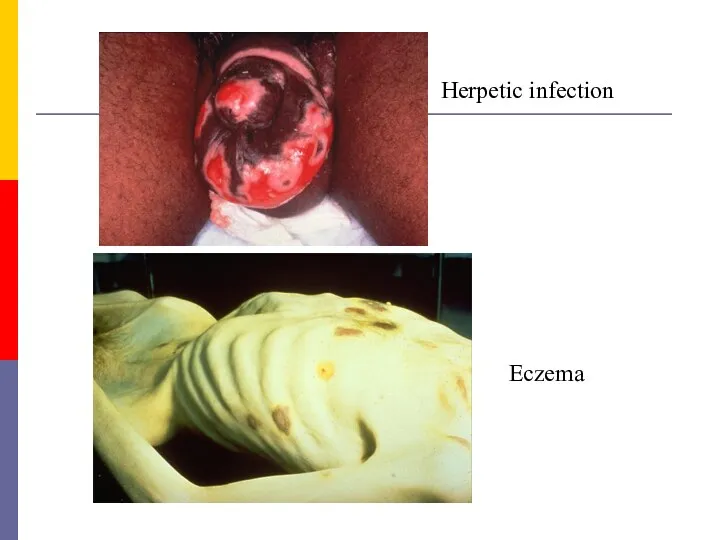
- 41. Herpetic infection Еczema
- 43. Dementia. HIV may cause direct cytopathogenic damage in tire central nervous system. It can cross the
- 44. There are many differences between adult and pediatric AIDS. Children develop humora1 immunodeficiency early, leading to
- 45. Laboratory diagnosis Laboratory procedures for the diagnosis of HIV infection include tests for immunodificiency as well
- 46. B. Specific tests for HIV infection. These inc1ude demonstration of HIV antigens and antibodies and isolation
- 47. If the infecting dose is small, as following a needlestick injury, the process may be considerably
- 48. 2. Virus isolation. Once infected with HIV, a person remains infected for life. The virus is
- 49. 3. Antibody detection. Demonstration of antibodies is the simplest and most widely employed technique for the
- 50. Once antibodies appear they increase in titre and broaden in spectrum for the next several months.
- 51. Screening tests possess high sensitivity, have a broadly reactive spectrum, are simple to perform and can
- 52. ELISA tests. Direct solid phase antiglobulin ELISA is the method most commonly used. The antigen obtained
- 53. The confirmatory test commonly employed is immunoblotting (the Western Blot test). In this test, I-IIV proteins
- 54. The confirmatory test In a positive serum, bands will be seen with multiple proteins, typically with
- 55. Applications of serological tests. Serological tests for HIV infection are employed in the following situations. A
- 56. Therapy of HIV Infection: Several distinct classes of drugs are now used to treat HIV infection:
- 57. Therapy of HIV Infection: Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs). In contrast to NRTIs, NNRTIs are not
- 58. Therapy of HIV Infection: Protease Inhibitors. These drugs are specific for the HIV-1 protease and competitively
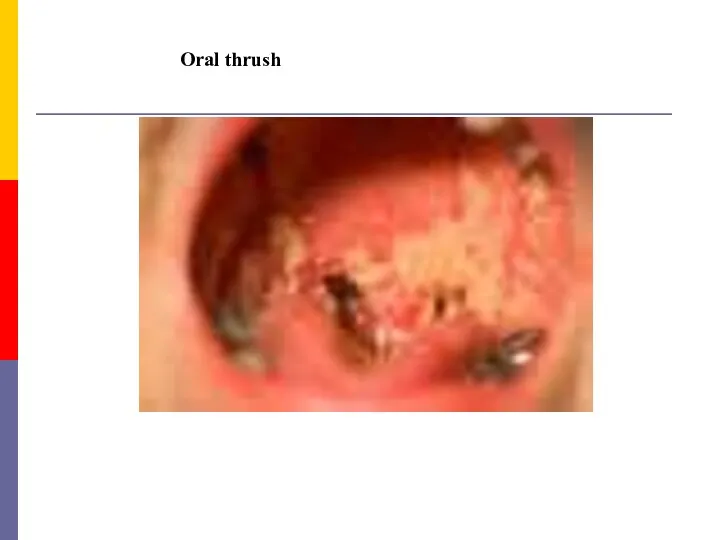
- 59. Oral thrush
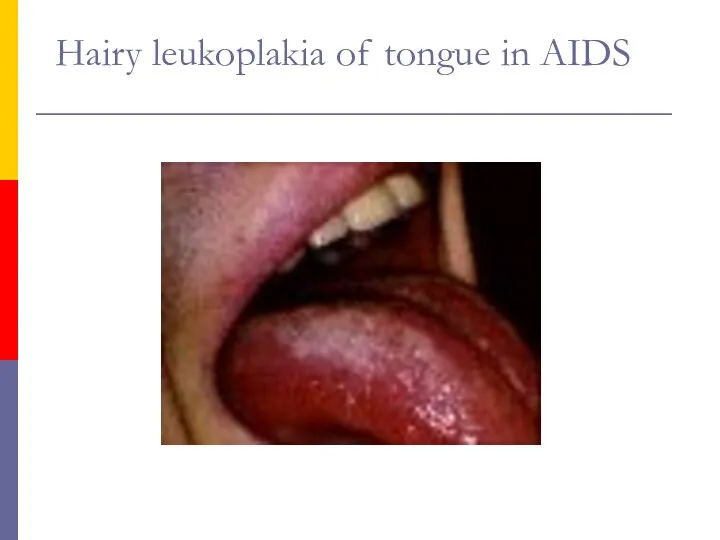
- 60. Hairy leukoplakia of tongue in AIDS
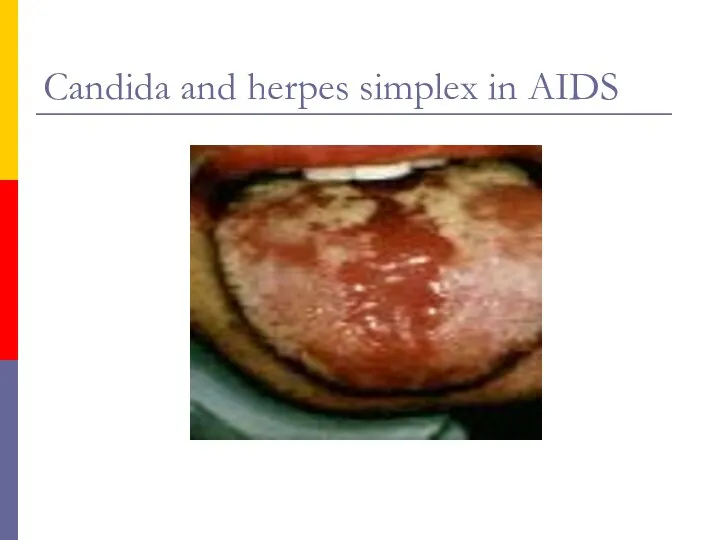
- 61. Candida and herpes simplex in AIDS
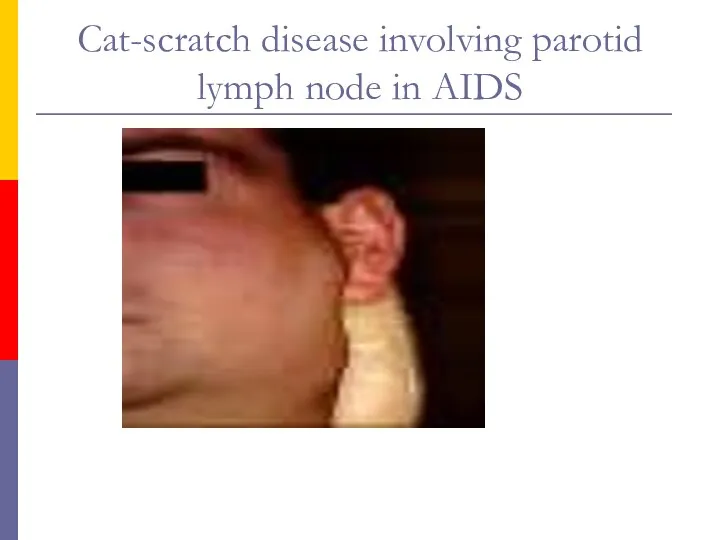
- 62. Cat-scratch disease involving parotid lymph node in AIDS
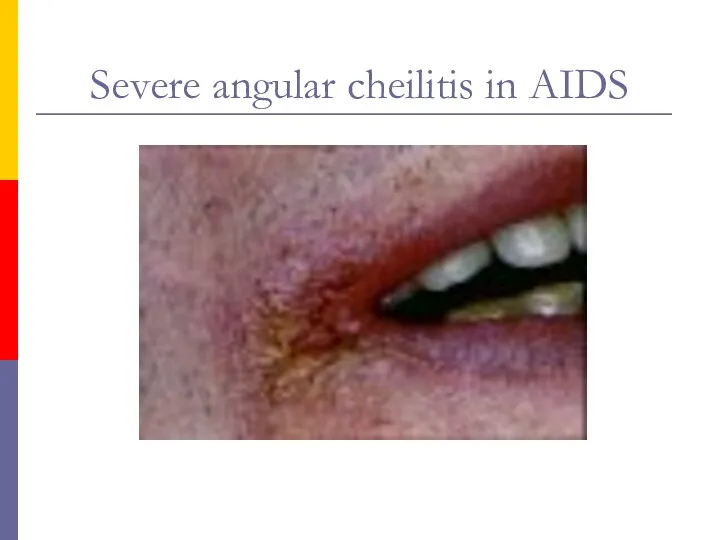
- 63. Severe angular cheilitis in AIDS
- 64. Orofacial granulomatosis with cobble stone mucosa in AIDS
- 65. Facial sarcoidosis in AIDS
- 68. Скачать презентацию
Plan of lecture
Overview
Etiology
Epidemiology
Pathogenesis
Manifestations
Diagnosis
Therapy and Prevention
Plan of lecture
Overview
Etiology
Epidemiology
Pathogenesis
Manifestations
Diagnosis
Therapy and Prevention
Human Immunodeficiency Virus
Human Immunodeficiency Virus
The first indication of new disease –
Acquired Immunodificiency Syndrom (AIDS)
The first indication of new disease –
Acquired Immunodificiency Syndrom (AIDS)
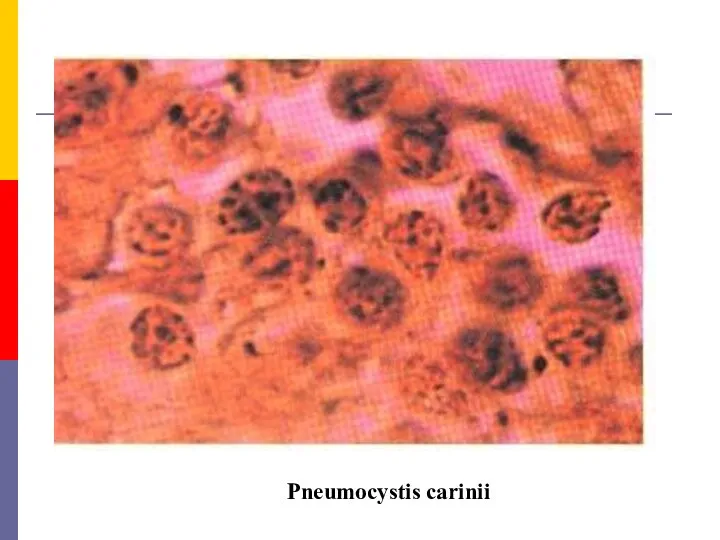
Pneumocystis carinii
Pneumocystis carinii
Statistics
The latest statistics on the world epidemic(UNAIDS/WHO) – 01.01.2012
People living with
Statistics
The latest statistics on the world epidemic(UNAIDS/WHO) – 01.01.2012
People living with
HIV, the etiologjcal agent of AIDS, belongs to the lentivirus subgroup
HIV, the etiologjcal agent of AIDS, belongs to the lentivirus subgroup
Types of HIV Virus
HIV 1
Most common in sub-Saharan Africa and throughout
Types of HIV Virus
HIV 1
Most common in sub-Saharan Africa and throughout
Viral genes and antigens. The genome of HIV contains the three
Viral genes and antigens. The genome of HIV contains the three
Pathogenesis.
The receptor for the virus is the CD4 antigen
and
Pathogenesis.
The receptor for the virus is the CD4 antigen
and
Specific binding of the virus to CD4 is by the envelope
Specific binding of the virus to CD4 is by the envelope
In an infected individual,
HIV can be isolated from
the blood,
In an infected individual,
HIV can be isolated from
the blood,
The primary pathogenic mechanism in HIV infection is the damage caused
The primary pathogenic mechanism in HIV infection is the damage caused
Window Period
Time from initial infection with HIV until antibodies are detected
Window Period
Time from initial infection with HIV until antibodies are detected
Disease Progression
Severity of illness is determined by amount of virus in
Disease Progression
Severity of illness is determined by amount of virus in
What body fluid transmit HIV?
blood
semen
vaginal fluid
breast milk
What body fluid transmit HIV?
blood
semen
vaginal fluid
breast milk
AIDS is primarily a sexually transmitted infection.
In the USA it
AIDS is primarily a sexually transmitted infection.
In the USA it

The second mode of transmission is through blood and blood products.
The second mode of transmission is through blood and blood products.
This restriction also applies to the donation of semen, cornea, bone
This restriction also applies to the donation of semen, cornea, bone
Contaminated needles can transmit the infection. This is particularly relevant in
Contaminated needles can transmit the infection. This is particularly relevant in

The danger of needlestick injury is present in medical and paramedical
The danger of needlestick injury is present in medical and paramedical
Transmission of infection from mother to baby can take place before,
Transmission of infection from mother to baby can take place before,
Normal social and domestic contact does not transmit the infection. Shaking
Normal social and domestic contact does not transmit the infection. Shaking
ACQUIRED DEFICIENCY SYNDROME (AIDS)
Clinical features of HIV infection. AIDS is
ACQUIRED DEFICIENCY SYNDROME (AIDS)
Clinical features of HIV infection. AIDS is
Acute HIV infection.
Within a few weeks of infection with
Acute HIV infection.
Within a few weeks of infection with
Asymptomatic infection.
All persons infected with HIV, whether they experience
Asymptomatic infection.
All persons infected with HIV, whether they experience
Persistant Generalised Liphadenopathy (PGL).
This has been defined as the presence
Persistant Generalised Liphadenopathy (PGL).
This has been defined as the presence
AIDS Related Complex (ARC).
This group inc1udes patients with considerable immunodeficiency,
AIDS Related Complex (ARC).
This group inc1udes patients with considerable immunodeficiency,
AIDS.
This is the end stage disease representing the irreversible breakdown
AIDS.
This is the end stage disease representing the irreversible breakdown
Dermatomycosis
Herpes zoster
Dermatomycosis
Herpes zoster
Dermatitis
Herpes
Dermatitis
Herpes
Kaposi's sarcoma
Kaposi's sarcoma
Kaposi's sarcoma
Kaposi's sarcoma
Warts
Sarcoma
Warts
Sarcoma
Herpetic infection
Еczema
Herpetic infection
Еczema
Dementia. HIV may cause direct cytopathogenic damage in tire central nervous
Dementia. HIV may cause direct cytopathogenic damage in tire central nervous
There are many differences between adult and pediatric AIDS.
Children develop
There are many differences between adult and pediatric AIDS.
Children develop
Laboratory diagnosis
Laboratory procedures for the diagnosis of HIV infection include
Laboratory diagnosis
Laboratory procedures for the diagnosis of HIV infection include
B. Specific tests for HIV infection. These inc1ude demonstration of HIV
B. Specific tests for HIV infection. These inc1ude demonstration of HIV
If the infecting dose is small, as following a needlestick injury,
2. Virus isolation. Once infected with HIV, a person remains infected
2. Virus isolation. Once infected with HIV, a person remains infected
3. Antibody detection. Demonstration of antibodies is the simplest and most
3. Antibody detection. Demonstration of antibodies is the simplest and most
Once antibodies appear they increase in titre and broaden in spectrum
Once antibodies appear they increase in titre and broaden in spectrum
Screening tests possess high sensitivity, have a broadly reactive spectrum, are
Screening tests possess high sensitivity, have a broadly reactive spectrum, are
ELISA tests. Direct solid phase antiglobulin ELISA is the method most
ELISA tests. Direct solid phase antiglobulin ELISA is the method most
The confirmatory test commonly employed is immunoblotting (the Western Blot test).
The confirmatory test commonly employed is immunoblotting (the Western Blot test).
The confirmatory test
In a positive serum, bands will be seen
The confirmatory test
In a positive serum, bands will be seen
Applications of serological tests.
Serological tests for HIV infection are employed
Applications of serological tests.
Serological tests for HIV infection are employed
Therapy of HIV Infection:
Several distinct classes of drugs are now used
Therapy of HIV Infection:
Several distinct classes of drugs are now used
Therapy of HIV Infection:
Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs). In contrast to
Therapy of HIV Infection:
Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs). In contrast to
Therapy of HIV Infection:
Protease Inhibitors. These drugs are specific for the
Therapy of HIV Infection:
Protease Inhibitors. These drugs are specific for the
Oral thrush
Oral thrush
Hairy leukoplakia of tongue in AIDS
Hairy leukoplakia of tongue in AIDS
Candida and herpes simplex in AIDS
Candida and herpes simplex in AIDS
Cat-scratch disease involving parotid lymph node in AIDS
Cat-scratch disease involving parotid lymph node in AIDS
Severe angular cheilitis in AIDS
Severe angular cheilitis in AIDS
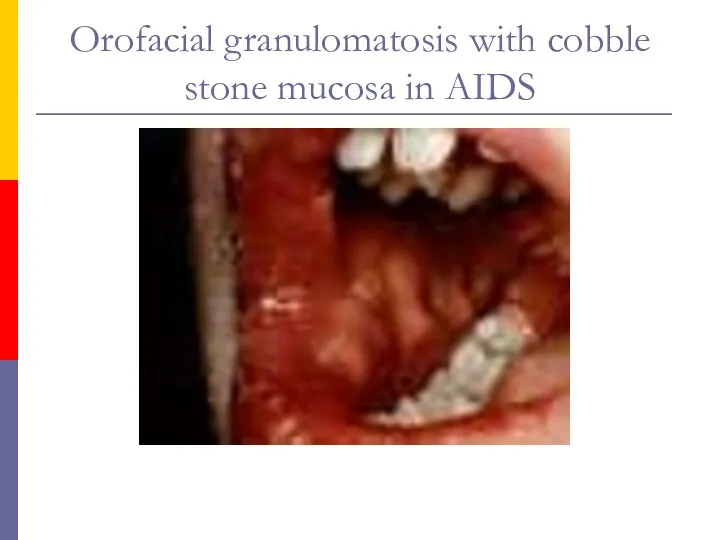
Orofacial granulomatosis with cobble stone mucosa in AIDS
Orofacial granulomatosis with cobble stone mucosa in AIDS
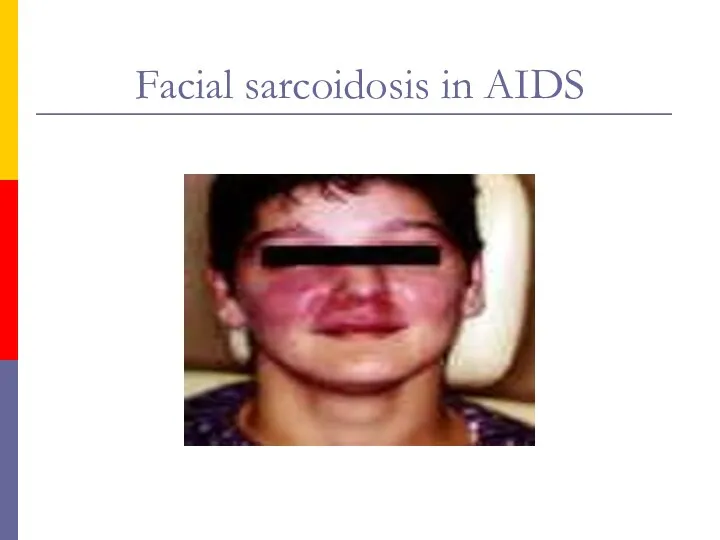
Facial sarcoidosis in AIDS
Facial sarcoidosis in AIDS

 АФО нервной системы и органов чувств ребенка. НПР детей раннего детского возраста
АФО нервной системы и органов чувств ребенка. НПР детей раннего детского возраста Развитие медицины в Древнем Египте
Развитие медицины в Древнем Египте Pelvic аnatomy
Pelvic аnatomy Лимфомы. Лимфогранулематоз
Лимфомы. Лимфогранулематоз Нарушение сна и бодрствования
Нарушение сна и бодрствования Профилактика туберкулеза. Диспансерное наблюдение, группы учета. Вакцинация БЦЖ и ее осложнения
Профилактика туберкулеза. Диспансерное наблюдение, группы учета. Вакцинация БЦЖ и ее осложнения Гиперкинезы. Некоторые виды гиперкинезов
Гиперкинезы. Некоторые виды гиперкинезов История развития сестринского дела
История развития сестринского дела Микроорганизмы, возбудители антропозоонозных инфекций
Микроорганизмы, возбудители антропозоонозных инфекций Понятия о ВИЧ-инфекции и СПИДе
Понятия о ВИЧ-инфекции и СПИДе Анемиялар
Анемиялар Паращитовидные железы
Паращитовидные железы Акупунктура. Акупунктураны медицинада қолдану. Биологиялық активті үктелер
Акупунктура. Акупунктураны медицинада қолдану. Биологиялық активті үктелер Желтушный синдром. Вирусный и токсический гепатит
Желтушный синдром. Вирусный и токсический гепатит Кариес и его профилактика
Кариес и его профилактика Клиника дифференцированных олигофрении
Клиника дифференцированных олигофрении ҚР 2016-2020 ж.арналған Денсаулық мемлекеттік бағдарламасы
ҚР 2016-2020 ж.арналған Денсаулық мемлекеттік бағдарламасы Ранняя помощь детям с ОВЗ
Ранняя помощь детям с ОВЗ Возбудители брюшного тифа и паратифов
Возбудители брюшного тифа и паратифов Патология слюнных желез
Патология слюнных желез Реабилитация пациентов при инфекционных и паразитарных заболеваниях
Реабилитация пациентов при инфекционных и паразитарных заболеваниях Трихофития
Трихофития Профессия Ветеринар
Профессия Ветеринар Угрожающее неотложное состояние у детей
Угрожающее неотложное состояние у детей Неходжкинские лимфомы у ВИЧ-инфицированных больных
Неходжкинские лимфомы у ВИЧ-инфицированных больных Ревматоидный артрит
Ревматоидный артрит Анемиялардың патоморфологиясы
Анемиялардың патоморфологиясы Определение арт-терапии
Определение арт-терапии