- Interactive case. The New England Journal of Medicine

Содержание
- 2. Presentation of patient 33-year-old man He complained of pain in the right side of his chest
- 3. Medical history Patient underwent colonoscopy with biopsy 4 years ago because of chronic diarrhea and unexplained
- 4. Social history Is married, with 2 children under 10 years of age Works as a health
- 5. Family history Mother suffered from systemic lupus erythematosus without renal involvement Father and brother are well,
- 6. Physical examination Temperature - 36.9˚C Pulse - 110 beats per minute and regular Blood pressure -
- 7. Symptom-oriented examination? Chest Heart Lungs Abdomen Lower extremities Skin Joints Lymph nodes
- 8. Which of the following tests are indicated to evaluate the patient’s symptoms? (3) 1. Cardiac ultrasonography
- 9. D-dimer level was elevated
- 10. ECG S1 Q3 T3 S1Q3T3-pattern
- 11. CT
- 12. Diagnosis The diagnosis of pulmonary embolism have been confirmed What should we do? Embolectomy Fibrinolytic therapy
- 13. Blood test What kind of anemia? Hypochromic 1) Microcytic Hyperchromic 2) Macrocytic
- 14. Urine test
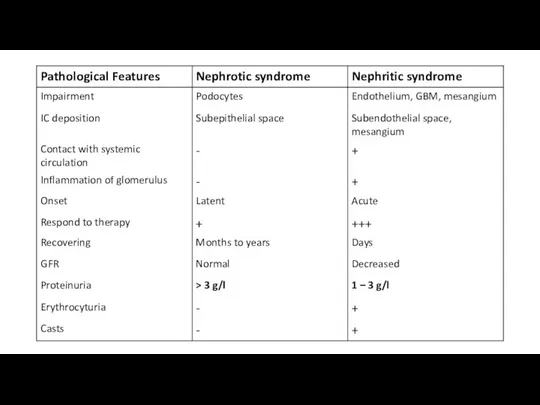
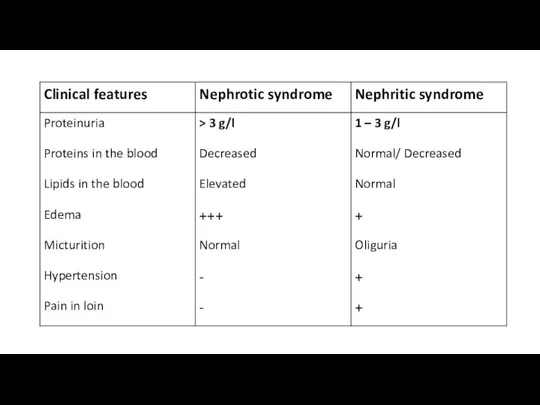
- 15. What is the most likely diagnosis according to urine test? Nephritic syndrome Nephrotic syndrome What is
- 16. Biochemistry blood test
- 17. Glomerular filtration rate - Male - Negroid race - 33-years-old - Creatinine = 80 μmol/L GFR
- 18. Fenestrated vascular endothelial cells
- 19. Glomerular basement membrane
- 20. Mesangium
- 21. Visceral epithelial cells (Podocytes)
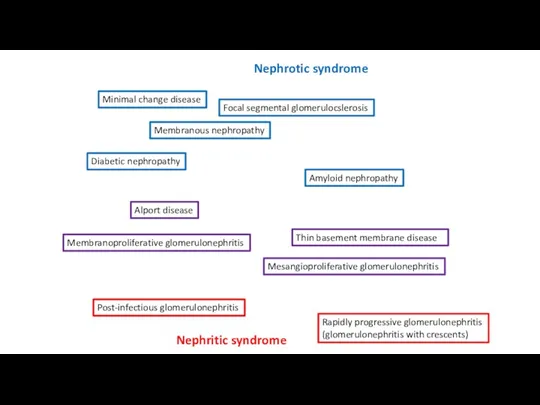
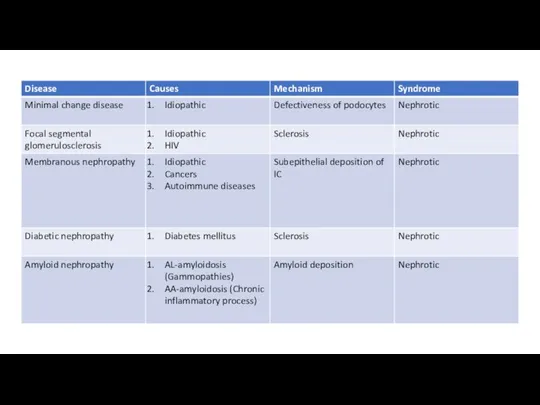
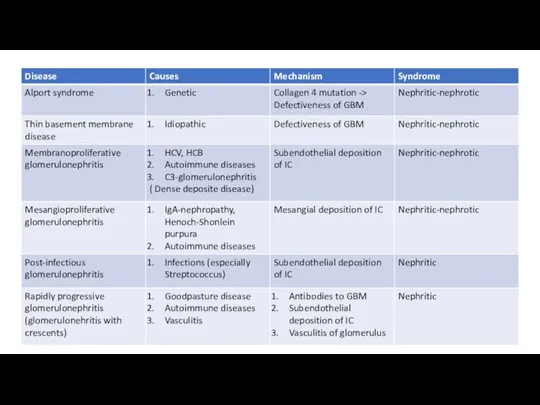
- 24. Minimal change disease Focal segmental glomerulocslerosis Membranous nephropathy Diabetic nephropathy Amyloid nephropathy Membranoproliferative glomerulonephritis Mesangioproliferative glomerulonephritis
- 28. Lupus nephritis Acute Rapidly progressive glomerulonephritis Chronic
- 29. Which of the following tests or procedures should be performed to further evaluate the cause of
- 30. Serological blood test
- 31. Renal biopsy
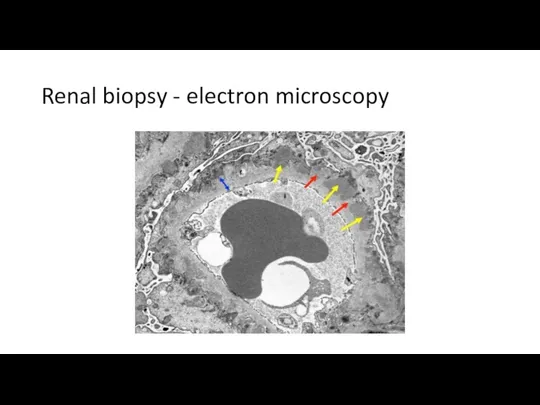
- 32. Renal biopsy - electron microscopy
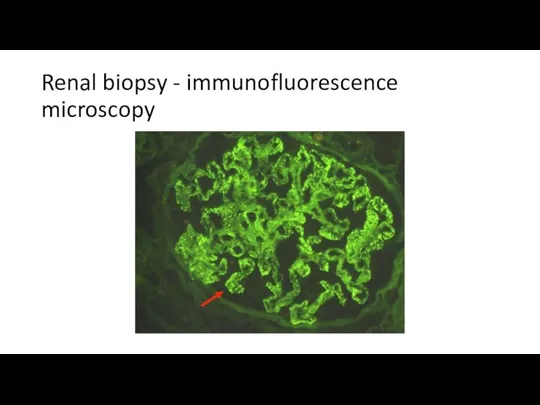
- 33. Renal biopsy - immunofluorescence microscopy
- 34. Renal biopsy The biopsy specimens reveal a membranous pattern of injury that is consistent with the
- 35. Pulmonary embolism Nephrotic syndrome Membranous nephropathy ??? Ulcerative colitis Elevated alkaline phosphatase and GGTP Hypochromic microcytic
- 36. The patient’s abnormal level of alkaline phosphatase is most suggestive of which one of the following
- 37. Which of the following procedures are now indicated? (2) 1) Cholangiopgraphy 2) Endoscopic ultrasonography of the
- 38. Colonoscopy
- 39. ERCP
- 40. Primary sclerosing cholangitis
- 41. Primary sclerosing cholangitis Autoimmune disease Progressive inflammation and fibrosis of the intrahepatic and extrahepatic bile ducts
- 42. Primary sclerosing cholangitis Elevated level of alkaline phosphatase is very common, even in early stages >
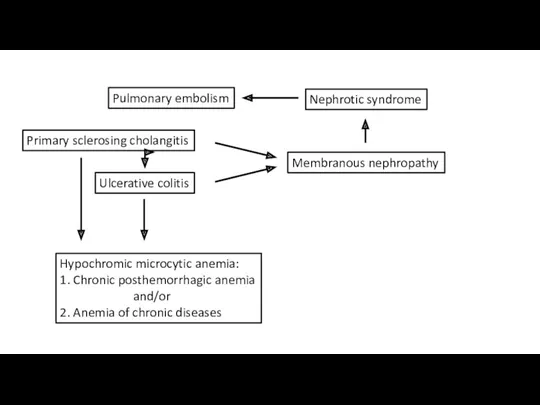
- 43. Pulmonary embolism Nephrotic syndrome Membranous nephropathy Primary sclerosing cholangitis Ulcerative colitis Hypochromic microcytic anemia: 1. Chronic
- 44. Ig4-related diseases
- 45. Outcomes The level of IgG4 was elevated The diagnosis has been changed to IgG4-related sclerosing cholangitis
- 47. Скачать презентацию
Presentation of patient
33-year-old man
He complained of pain in the right side
Presentation of patient
33-year-old man
He complained of pain in the right side
Medical history
Patient underwent colonoscopy with biopsy 4 years ago because of
Medical history
Patient underwent colonoscopy with biopsy 4 years ago because of
Social history
Is married, with 2 children under 10 years of age
Works
Social history
Is married, with 2 children under 10 years of age
Works
Family history
Mother suffered from systemic lupus erythematosus without renal involvement
Father and
Family history
Mother suffered from systemic lupus erythematosus without renal involvement
Father and
Physical examination
Temperature - 36.9˚C
Pulse - 110 beats per minute and regular
Blood
Physical examination
Temperature - 36.9˚C
Pulse - 110 beats per minute and regular
Blood
Symptom-oriented examination?
Chest
Heart
Lungs
Abdomen
Lower extremities
Skin
Joints
Lymph nodes
Symptom-oriented examination?
Chest
Heart
Lungs
Abdomen
Lower extremities
Skin
Joints
Lymph nodes
Which of the following tests are indicated to evaluate the patient’s
Which of the following tests are indicated to evaluate the patient’s
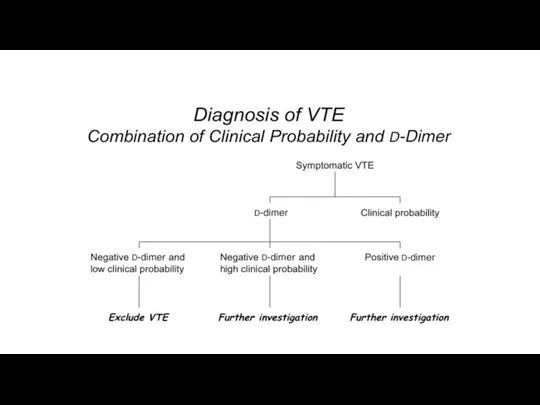
D-dimer level was elevated
D-dimer level was elevated
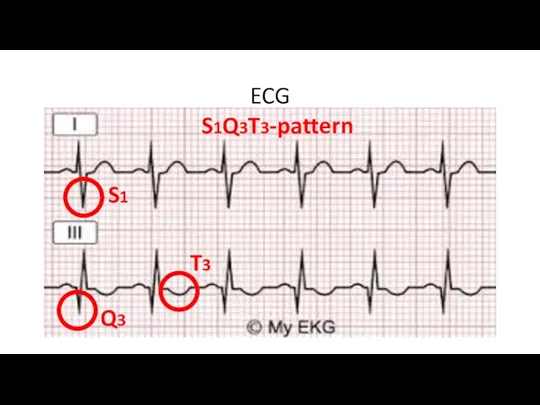
ECG
S1
Q3
T3
S1Q3T3-pattern
ECG
S1
Q3
T3
S1Q3T3-pattern
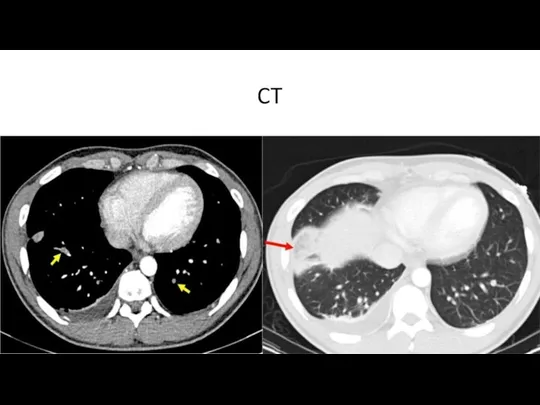
CT
CT
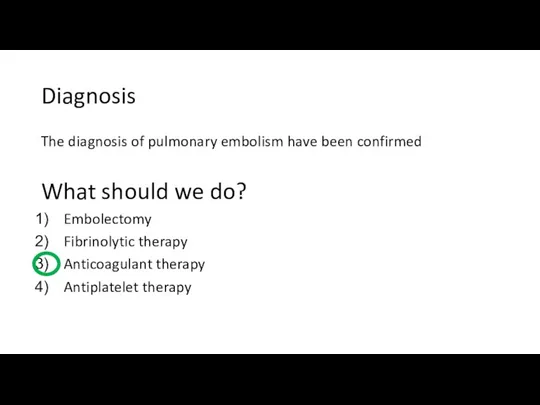
Diagnosis
The diagnosis of pulmonary embolism have been confirmed
What should we
Diagnosis
The diagnosis of pulmonary embolism have been confirmed
What should we
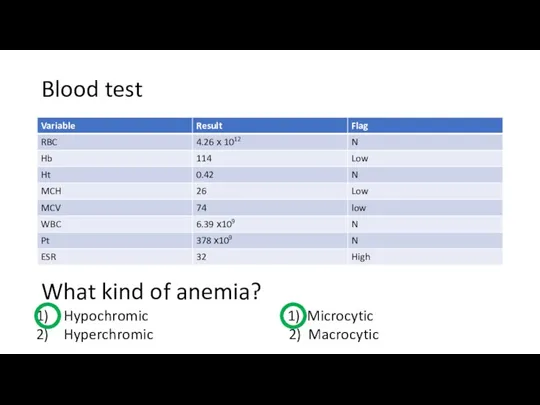
Blood test
What kind of anemia?
Hypochromic 1) Microcytic
Hyperchromic 2) Macrocytic
Blood test
What kind of anemia?
Hypochromic 1) Microcytic
Hyperchromic 2) Macrocytic
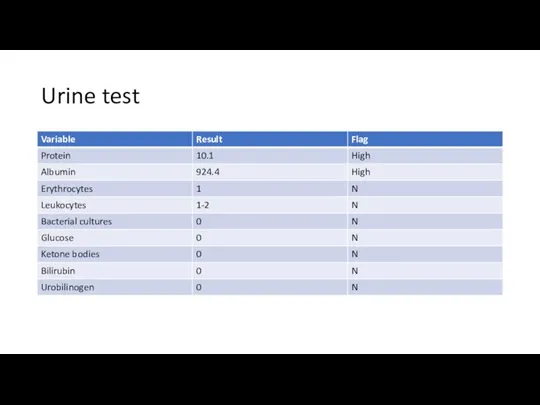
Urine test
Urine test
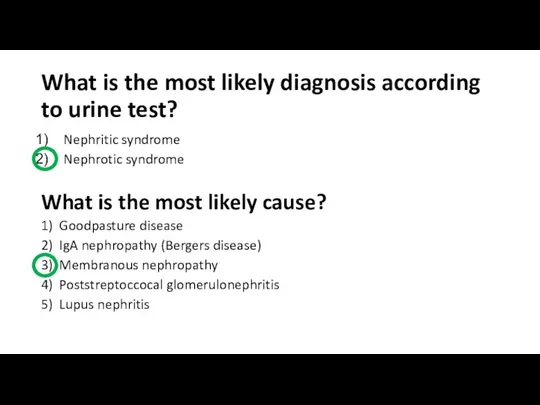
What is the most likely diagnosis according to urine test?
Nephritic syndrome
Nephrotic
What is the most likely diagnosis according to urine test?
Nephritic syndrome
Nephrotic
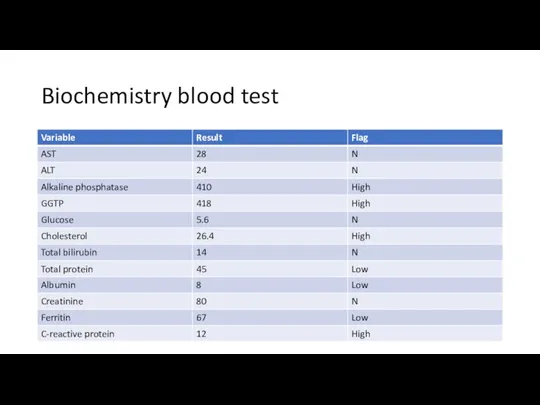
Biochemistry blood test
Biochemistry blood test
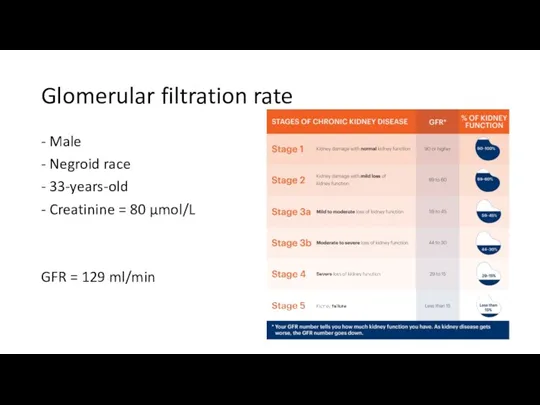
Glomerular filtration rate
- Male
- Negroid race
- 33-years-old
- Creatinine = 80 μmol/L
GFR
Glomerular filtration rate
- Male
- Negroid race
- 33-years-old
- Creatinine = 80 μmol/L
GFR
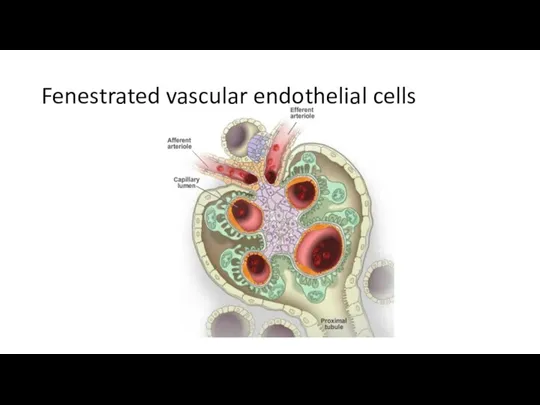
Fenestrated vascular endothelial cells
Fenestrated vascular endothelial cells
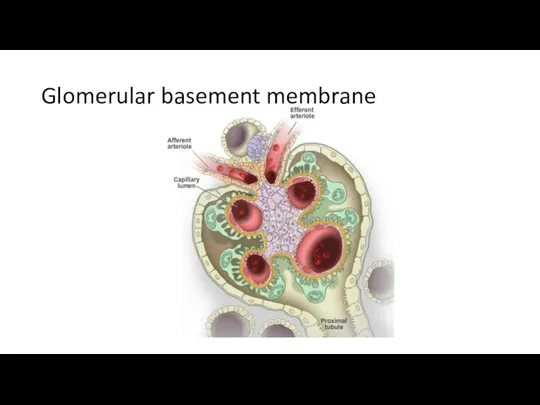
Glomerular basement membrane
Glomerular basement membrane
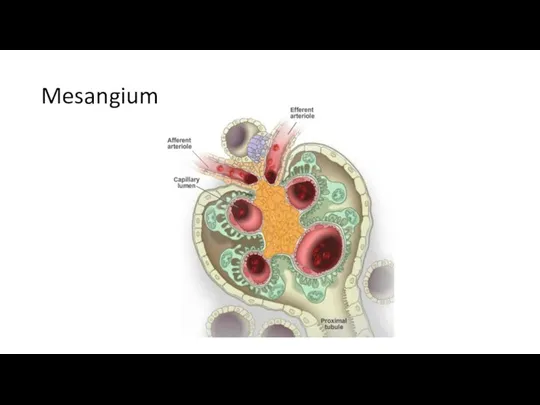
Mesangium
Mesangium
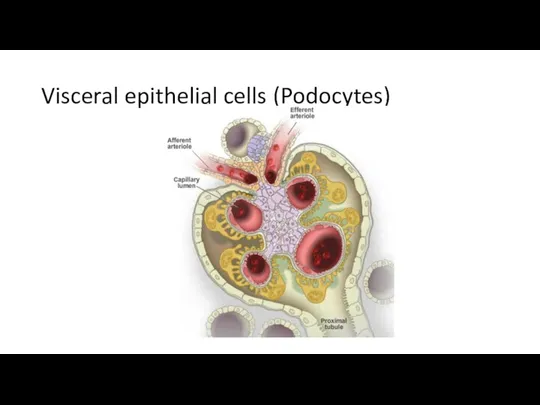
Visceral epithelial cells (Podocytes)
Visceral epithelial cells (Podocytes)
Minimal change disease
Focal segmental glomerulocslerosis
Membranous nephropathy
Diabetic nephropathy
Amyloid nephropathy
Membranoproliferative glomerulonephritis
Mesangioproliferative glomerulonephritis
Post-infectious glomerulonephritis
Rapidly
Minimal change disease
Focal segmental glomerulocslerosis
Membranous nephropathy
Diabetic nephropathy
Amyloid nephropathy
Membranoproliferative glomerulonephritis
Mesangioproliferative glomerulonephritis
Post-infectious glomerulonephritis
Rapidly
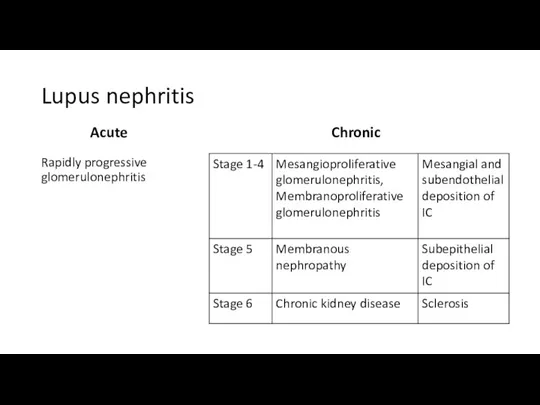
Lupus nephritis
Acute
Rapidly progressive glomerulonephritis
Chronic
Lupus nephritis
Acute
Rapidly progressive glomerulonephritis
Chronic
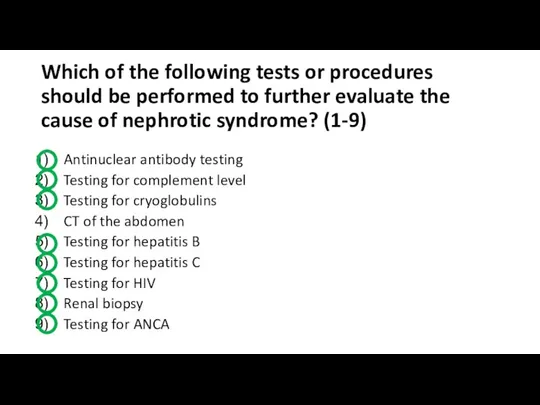
Which of the following tests or procedures should be performed to
Which of the following tests or procedures should be performed to
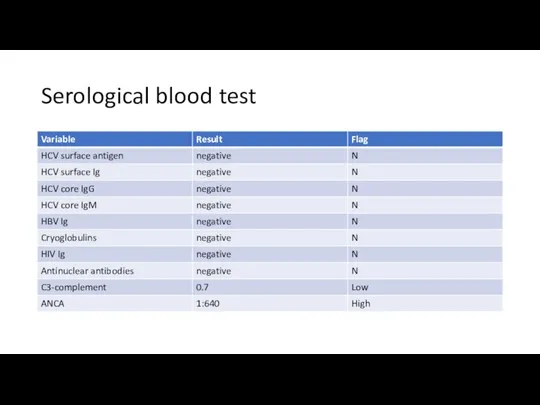
Serological blood test
Serological blood test

Renal biopsy
Renal biopsy
Renal biopsy - electron microscopy
Renal biopsy - electron microscopy
Renal biopsy - immunofluorescence microscopy
Renal biopsy - immunofluorescence microscopy
Renal biopsy
The biopsy specimens reveal a membranous pattern of injury that
Renal biopsy
The biopsy specimens reveal a membranous pattern of injury that
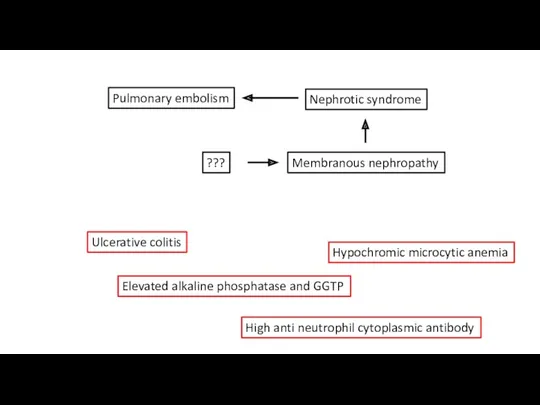
Pulmonary embolism
Nephrotic syndrome
Membranous nephropathy
???
Ulcerative colitis
Elevated alkaline phosphatase and GGTP
Hypochromic microcytic anemia
High
Pulmonary embolism
Nephrotic syndrome
Membranous nephropathy
???
Ulcerative colitis
Elevated alkaline phosphatase and GGTP
Hypochromic microcytic anemia
High
The patient’s abnormal level of alkaline phosphatase is most suggestive of
The patient’s abnormal level of alkaline phosphatase is most suggestive of
Which of the following procedures are now indicated? (2)
1) Cholangiopgraphy
2) Endoscopic
Which of the following procedures are now indicated? (2)
1) Cholangiopgraphy
2) Endoscopic
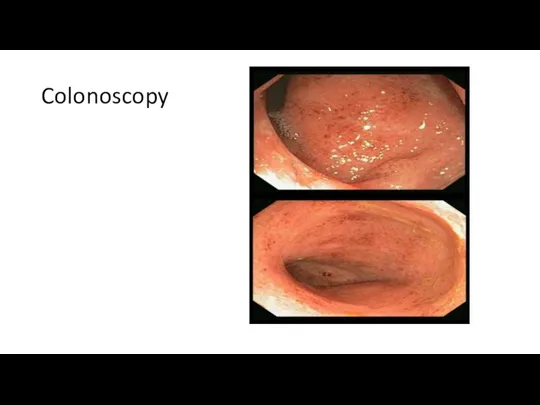
Colonoscopy
Colonoscopy
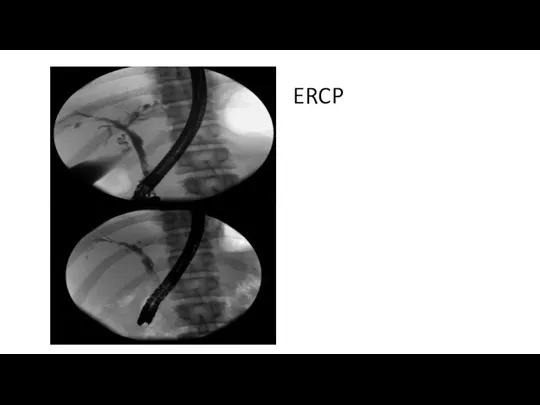
ERCP
ERCP
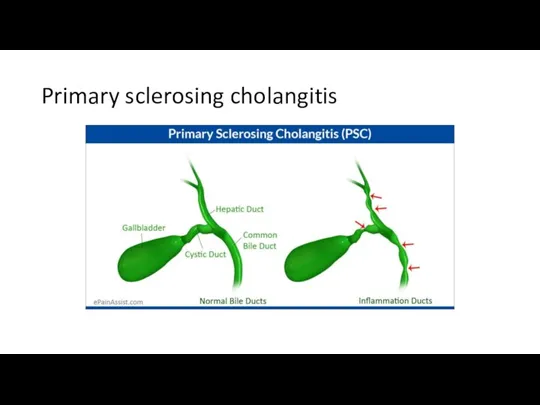
Primary sclerosing cholangitis
Primary sclerosing cholangitis
Primary sclerosing cholangitis
Autoimmune disease
Progressive inflammation and fibrosis of the intrahepatic and
Primary sclerosing cholangitis
Autoimmune disease
Progressive inflammation and fibrosis of the intrahepatic and
Primary sclerosing cholangitis
Elevated level of alkaline phosphatase is very common, even
Primary sclerosing cholangitis
Elevated level of alkaline phosphatase is very common, even
Pulmonary embolism
Nephrotic syndrome
Membranous nephropathy
Primary sclerosing cholangitis
Ulcerative colitis
Hypochromic microcytic anemia:
1. Chronic posthemorrhagic
Pulmonary embolism
Nephrotic syndrome
Membranous nephropathy
Primary sclerosing cholangitis
Ulcerative colitis
Hypochromic microcytic anemia:
1. Chronic posthemorrhagic
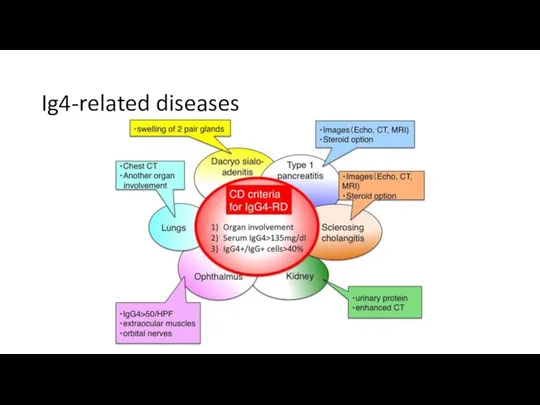
Ig4-related diseases
Ig4-related diseases
Outcomes
The level of IgG4 was elevated
The diagnosis has been changed to
Outcomes
The level of IgG4 was elevated
The diagnosis has been changed to
 Temporary fillings
Temporary fillings Диагностика и лечение инфаркта миокарда
Диагностика и лечение инфаркта миокарда Пиодермии. Определение
Пиодермии. Определение Ана сүтімен қоректендірудің маңызы
Ана сүтімен қоректендірудің маңызы Сосудистый шов
Сосудистый шов Иммунология даму тарихы. Иммунитет теориясы
Иммунология даму тарихы. Иммунитет теориясы Жедел гастрит
Жедел гастрит Принципы диагностики и лечения инфекционных заболеваний
Принципы диагностики и лечения инфекционных заболеваний железа
железа Острые эмболии и тромбозы магистральных артерий конечностей. Консервативное лечение. Показания и виды оперативных вмешательств
Острые эмболии и тромбозы магистральных артерий конечностей. Консервативное лечение. Показания и виды оперативных вмешательств Огнестрельные ранения. Хирургическая обработка огнестрельных ран
Огнестрельные ранения. Хирургическая обработка огнестрельных ран Шок. Патофизиология и принципы интенсивной терапии
Шок. Патофизиология и принципы интенсивной терапии Клинический случай
Клинический случай Вирусные дерматозы
Вирусные дерматозы Проводящая система сердца. ЭКГ
Проводящая система сердца. ЭКГ Особенности обеспечения проходимости дыхательных путей у детей. Интубация трахеи
Особенности обеспечения проходимости дыхательных путей у детей. Интубация трахеи Деваскурялизация матки при применении компрессионного шва по B-Linch
Деваскурялизация матки при применении компрессионного шва по B-Linch Гигиенические требования к выбору и планировке больничного участка. Системы строительства больниц, их преимущества и недостатки
Гигиенические требования к выбору и планировке больничного участка. Системы строительства больниц, их преимущества и недостатки Общая фармакология. Введение в фармакологию
Общая фармакология. Введение в фармакологию Боткин Сергей Петрович
Боткин Сергей Петрович Иық буынының жарақаттары
Иық буынының жарақаттары Респираторный дистресс-синдром взрослых
Респираторный дистресс-синдром взрослых Врождённые пороки развития женской половой системы
Врождённые пороки развития женской половой системы Анатомо-физиологические особенности строения полости рта новорожденного
Анатомо-физиологические особенности строения полости рта новорожденного Дифференциальный диагноз анемий
Дифференциальный диагноз анемий Сухожильный шов
Сухожильный шов Клинико-экономические исследования
Клинико-экономические исследования Дифференциальный диагноз суставного синдрома (один день из жизни врача общей практики)
Дифференциальный диагноз суставного синдрома (один день из жизни врача общей практики)