- Interesting case

Содержание
- 2. A 12-year-old girl CC: Blurred vision 1 day History taking
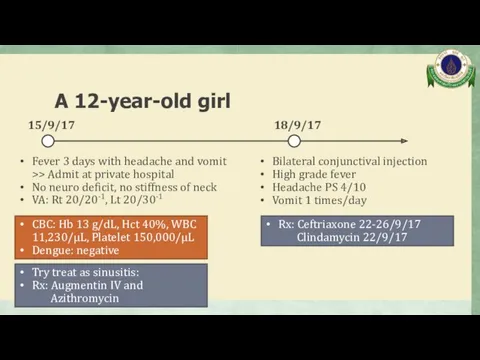
- 3. A 12-year-old girl Fever 3 days with headache and vomit >> Admit at private hospital No
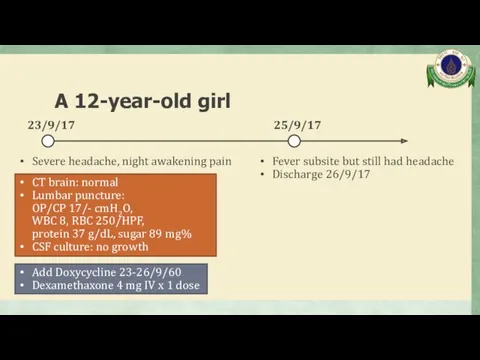
- 4. A 12-year-old girl Severe headache, night awakening pain 23/9/17 25/9/17 Fever subsite but still had headache
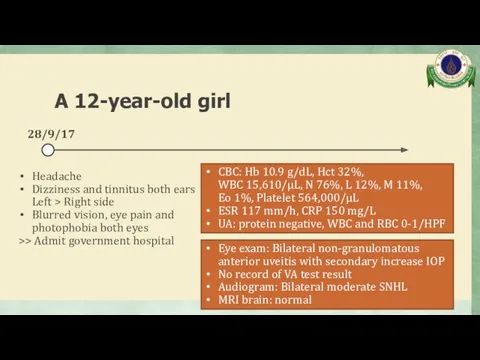
- 5. A 12-year-old girl Headache Dizziness and tinnitus both ears Left > Right side Blurred vision, eye
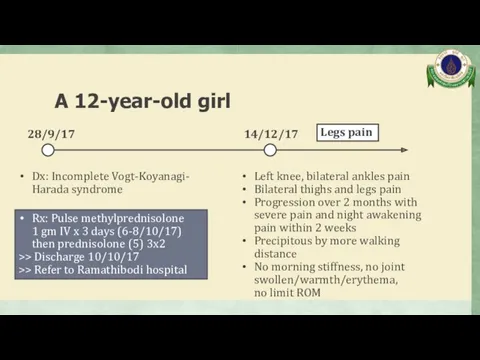
- 6. A 12-year-old girl Dx: Incomplete Vogt-Koyanagi- Harada syndrome 28/9/17 Rx: Pulse methylprednisolone 1 gm IV x
- 7. Past history No history of eye trauma No history of anorexia/weight loss No history of photosensitivity
- 8. A 12-year-old girl Physical examination
- 9. Physical examination GA: active, cushingoid appearance V/S: BT 36.7°C, PR 118/min, RR 20/min BP 4 extremities:
- 10. Physical examination LNs: negative Heart: no heave/thrill, normal S1S2, no murmur Lungs: clear both lungs Abdomen:
- 11. Physical examination Neuro signs: Good consciousness Intact CN functions Normal tone, Motor power gr.V all extremities
- 12. A 12-year-old girl Problem list
- 13. Problem list Hypertension with arterial insufficiency: Lower limb claudication with different BP between upper and lower
- 14. A 12-year-old girl Differential diagnosis
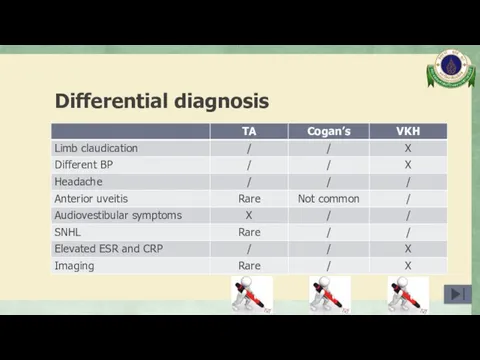
- 15. Differential diagnosis Takayasu arteritis Cogan’s syndrome Vogt-Koyanagi-Harada syndrome
- 16. A 12-year-old girl Investigation
- 17. Investigation
- 18. Complete blood count Hb 13.6 g/dL, Hct 43.3% WBC 13,300/µL, N 75%, L 15%, M 9%,
- 19. Blood chemistry BUN 19, Cr 0.35 mg/dL Na 142, K 3.93, Cl 107, HCO3 22.2 mmol/L
- 20. Inflammatory markers ESR 8 mm/hr CRP
- 21. Urinalysis Sp. gr. 1.019, pH 5, protein negative, blood negative WBC 0-1, RBC 0-1 /HPF
- 22. Immunology ANA negative
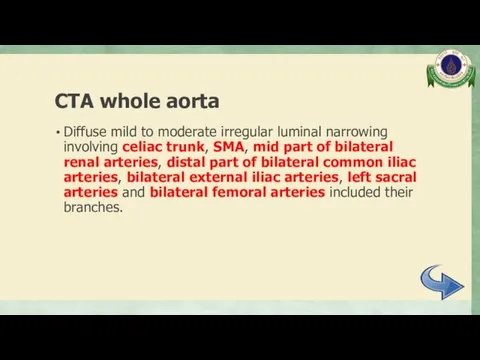
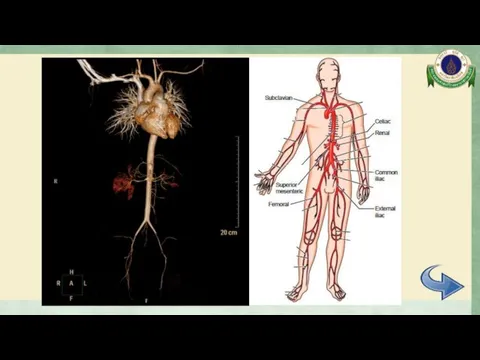
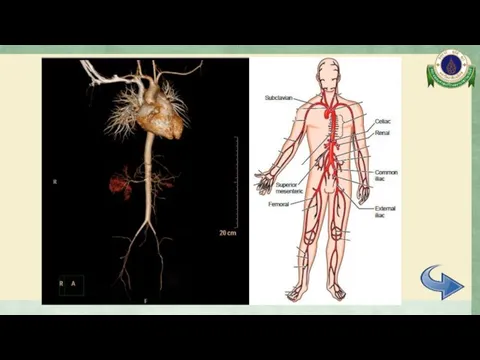
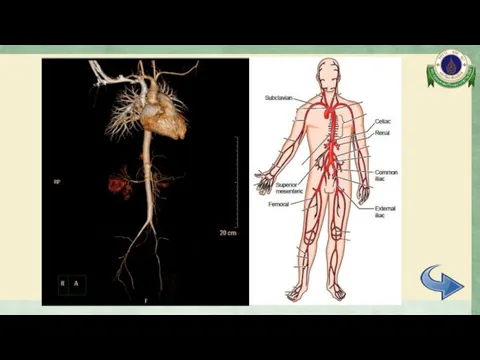
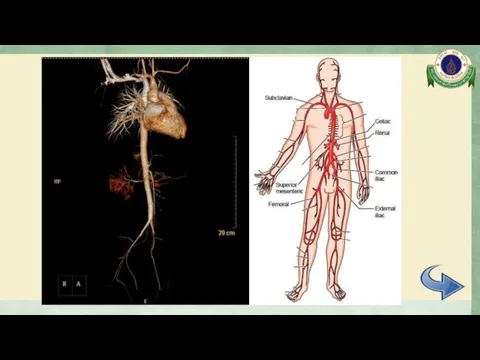
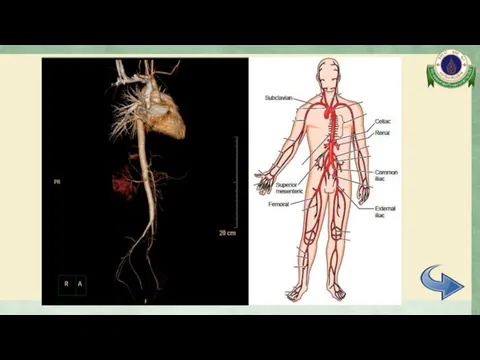
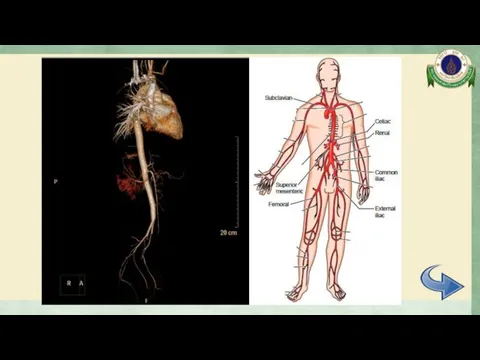
- 23. CTA whole aorta Diffuse mild to moderate irregular luminal narrowing involving celiac trunk, SMA, mid part
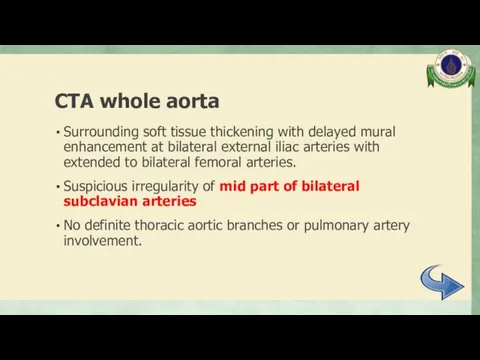
- 24. CTA whole aorta Surrounding soft tissue thickening with delayed mural enhancement at bilateral external iliac arteries
- 25. CTA whole aorta
- 26. CTA whole aorta
- 27. CTA whole aorta
- 28. CTA whole aorta
- 29. CTA whole aorta
- 30. CTA whole aorta
- 31. CTA whole aorta
- 32. Electrocardiogram Normal sinus rhythm, rate 110/min, normal axis No chamber enlargement
- 33. Echocardiogram Normal cardiac function Trivial to mild MR and AR No coarctation of aorta or aortic
- 34. Eye examination VA: Rt 20/80, 20/50 with PH Lt 20/50, 20/40 with PH IOP Rt 15,
- 35. Audiogram Moderately severe sensorineural hearing loss both ears
- 36. A 12-year-old girl Differential diagnosis
- 37. Differential diagnosis Takayasu arteritis Cogan’s syndrome Vogt-Koyanagi-Harada syndrome
- 38. Differential diagnosis
- 39. Takayasu arteritis (TA) Arteritis, often granulomatous Predominantly affecting the aorta and/or its major branches Arthritis Rheum
- 40. EULAR/PRINTO/PRES classification criteria of childhood TA Angiographic abnormalities plus 1 of 5 following criteria (sens 100%,
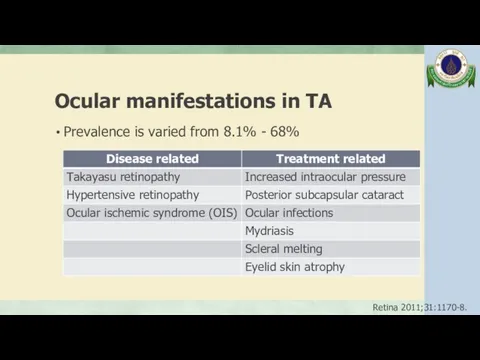
- 41. Ocular manifestations in TA Prevalence is varied from 8.1% - 68% Retina 2011;31:1170-8.
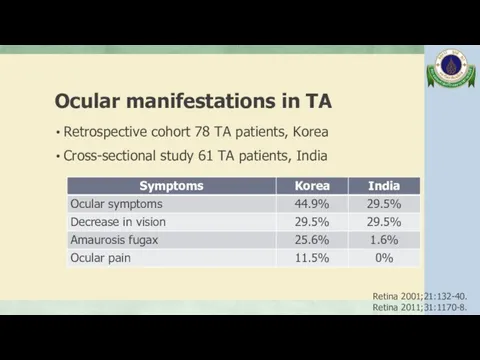
- 42. Ocular manifestations in TA Retrospective cohort 78 TA patients, Korea Cross-sectional study 61 TA patients, India
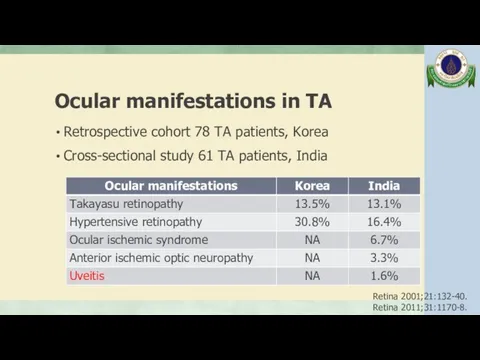
- 43. Ocular manifestations in TA Retrospective cohort 78 TA patients, Korea Cross-sectional study 61 TA patients, India
- 44. SNHL in TA Few case reports of SNHL associated with TA Many reports showed the beneficial
- 45. SNHL in TA The cause of the hearing impairment associated with TA is unknown, may be
- 46. SNHL in TA The mechanisms of the hearing loss in TA are reversible circulatory disturbances due
- 47. TA without involvement of aorta Retrospective review 85 CT angiography in TA patient, 1994-2003, Korea 95%
- 48. Cogan’s syndrome (CS) Characterized by ocular inflammatory lesions, including interstitial keratitis, uveitis, and episcleritis, and inner
- 49. Typical CS Defined by following 3 conditions: (1) Ocular symptoms typically an isolated non-syphilitic interstitial keratitis
- 50. Atypical CS Any of following conditions: (1) Inflammatory ocular manifestations including episcleritis, scleritis, retinal artery occlusion,
- 51. Ocular manifestations in CS 80% Interstitial keratitis, mostly bilateral involvement; inflamed small blood vessels invade the
- 52. Audiovestibular manifestations in CS Sudden onset of hearing loss, vertigo, tinnitus, nausea, vomiting Often resolving after
- 53. Vasculitic manifestations in CS May include arteritis (affecting small, medium, or large arteries), aortitis, aortic aneurysms,
- 54. Vogt-Koyanagi-Harada syndrome (VKH) Systemic autoimmune disease; main target is melanin-containing-cells present in the eye, meninges, ear
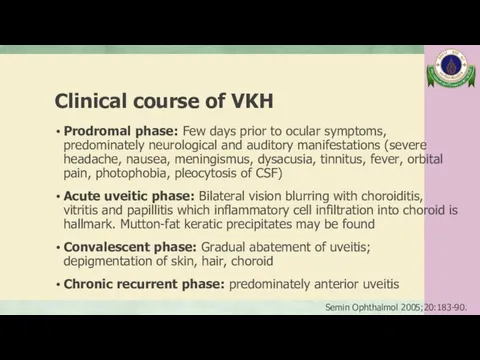
- 55. Clinical course of VKH Prodromal phase: Few days prior to ocular symptoms, predominately neurological and auditory
- 56. Revise diagnostic criteria of VKH Complete disease; criteria 1 to 5 must be present Incomplete disease;
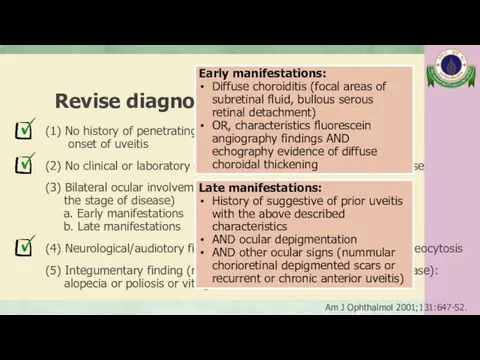
- 57. Revise diagnostic criteria of VKH (1) No history of penetrating ocular trauma or surgery preceding onset
- 58. Ocular manifestations in VKH The posterior manifestation is the hallmark, demonstrating vitreous cells with bilateral exudative
- 59. Ocular manifestations in VKH Signs of depigmentation: - Sunset glow: changes of fundus represent choroidal depigmentation
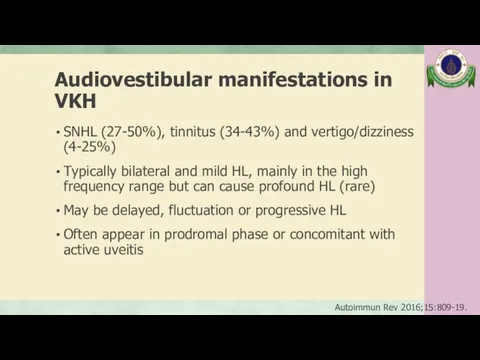
- 60. Audiovestibular manifestations in VKH SNHL (27-50%), tinnitus (34-43%) and vertigo/dizziness (4-25%) Typically bilateral and mild HL,
- 61. Vasculitis in VKH Case report of a 44-year-old female in Japan, developed VKH after diagnosed aortitis
- 62. A 12-year-old girl Management
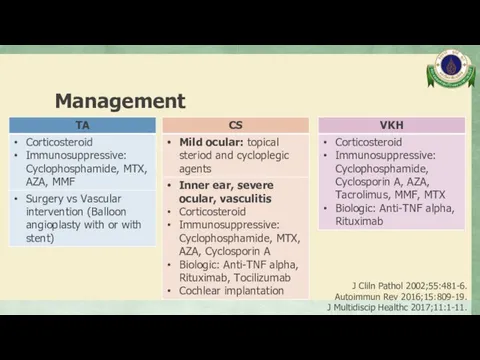
- 63. Management J Cliln Pathol 2002;55:481-6. Autoimmun Rev 2016;15:809-19. J Multidiscip Healthc 2017;11:1-11.
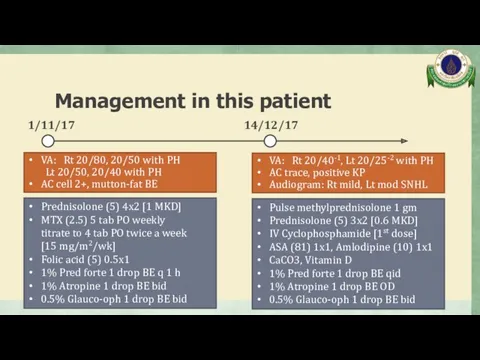
- 64. Management in this patient 1/11/17 14/12/17 Prednisolone (5) 4x2 [1 MKD] MTX (2.5) 5 tab PO
- 65. Management in this patient 11/1/18 IV Cyclophosphamide [2nd dose] Prednisolone (5) 2x2 [0.4 MKD] ASA (81)
- 66. Take home message Takayasu arteritis: Uveitis is uncommon ocular manifestation Isolated branch vessel involvement is possible
- 67. Thank you
- 68. Rheumatic diseases with reported aortic involvement Clin Exp Rheumatol 2006;24:S41-7.
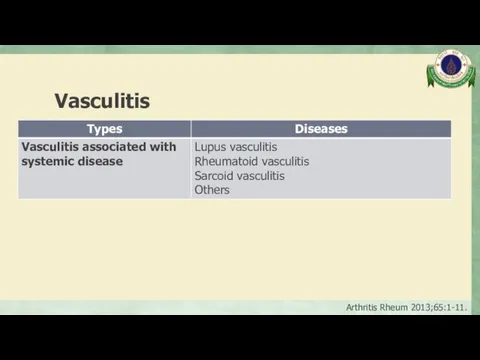
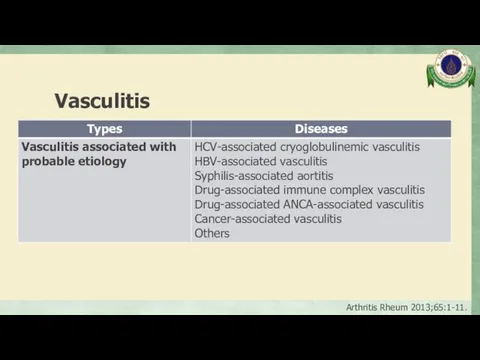
- 69. Vasculitis Inflammation of blood vessel walls The inflammatory infiltrate may be one that is predominantly neutrophilic,
- 70. Vasculitis Arthritis Rheum 2013;65:1-11.
- 71. Vasculitis Arthritis Rheum 2013;65:1-11.
- 72. Vasculitis Arthritis Rheum 2013;65:1-11.
- 73. Vasculitis Arthritis Rheum 2013;65:1-11.
- 74. Vasculitis Arthritis Rheum 2013;65:1-11.
- 75. Aortitis Pathological term for inflammation of the aortic wall The classification of aortitis broadly includes underlying
- 76. Clinical presentation Asymptomatic General syndrome: fever, malaise, weight loss, high ESR Pain (chest, back, abdominal): acute
- 77. Causes of aortitis Inflammatory: Large vessel vasculitis: TAK, GCA Rheumatoid arthritis Systemic lupus erythematosus HLA-B27 associated
- 78. Causes of aortitis Isolated aortitis: Isolated idiopathic (thoracic aortitis) Chronic periaortitis: Idiopathic retroperitoneal fibrosis, Inflammatory abdominal
- 79. Causes of aortitis Infectious: Bacteria: Salmonella spp., Staphylococcus spp., Streptococcus pneumoniae, other Syphilis Mycobacterium Other Circulation
- 80. Laboratory testing Markers of inflammation: ESR, CRP Complete blood count Kidney and liver function Additional laboratory
- 81. Imaging modalities Korean J Radiol 2017;18:786-98.
- 82. ACR classification criteria of TA ≥ 3 of 6 criteria (sens 90.5%, spec 97.8%) Age at
- 83. Takayasu arteritis (TA) Incidence 0.4-1 case/1,000,000/year Onset usually occurs before the age of 50 years, which
- 84. Angiographic classification of TA from the Takayasu conference 1994 Int J Cardiol 2012;159:14-20.
- 86. Скачать презентацию
A 12-year-old girl
CC: Blurred vision 1 day
History taking
A 12-year-old girl
CC: Blurred vision 1 day
History taking
A 12-year-old girl
Fever 3 days with headache and vomit >> Admit
A 12-year-old girl
Fever 3 days with headache and vomit >> Admit
A 12-year-old girl
Severe headache, night awakening pain
23/9/17
25/9/17
Fever subsite but still had
A 12-year-old girl
Severe headache, night awakening pain
23/9/17
25/9/17
Fever subsite but still had
A 12-year-old girl
Headache
Dizziness and tinnitus both ears Left > Right side
Blurred
A 12-year-old girl
Headache
Dizziness and tinnitus both ears Left > Right side
Blurred
A 12-year-old girl
Dx: Incomplete Vogt-Koyanagi- Harada syndrome
28/9/17
Rx: Pulse methylprednisolone
1 gm
A 12-year-old girl
Dx: Incomplete Vogt-Koyanagi- Harada syndrome
28/9/17
Rx: Pulse methylprednisolone 1 gm
Past history
No history of eye trauma
No history of anorexia/weight loss
No history
Past history
No history of eye trauma
No history of anorexia/weight loss
No history
A 12-year-old girl
Physical examination
A 12-year-old girl
Physical examination
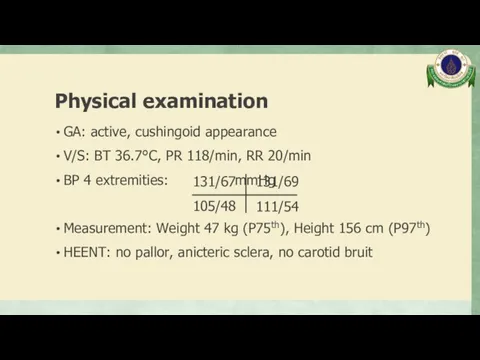
Physical examination
GA: active, cushingoid appearance
V/S: BT 36.7°C, PR 118/min, RR 20/min
BP
Physical examination
GA: active, cushingoid appearance
V/S: BT 36.7°C, PR 118/min, RR 20/min
BP
Physical examination
LNs: negative
Heart: no heave/thrill, normal S1S2, no murmur
Lungs: clear
Physical examination
LNs: negative
Heart: no heave/thrill, normal S1S2, no murmur
Lungs: clear
Physical examination
Neuro signs:
Good consciousness
Intact CN functions
Normal tone, Motor
Physical examination
Neuro signs: Good consciousness Intact CN functions Normal tone, Motor
A 12-year-old girl
Problem list
A 12-year-old girl
Problem list
Problem list
Hypertension with arterial insufficiency: Lower limb claudication with different BP
Problem list
Hypertension with arterial insufficiency: Lower limb claudication with different BP
A 12-year-old girl
Differential diagnosis
A 12-year-old girl
Differential diagnosis
Differential diagnosis
Takayasu arteritis
Cogan’s syndrome
Vogt-Koyanagi-Harada syndrome
Differential diagnosis
Takayasu arteritis
Cogan’s syndrome
Vogt-Koyanagi-Harada syndrome
A 12-year-old girl
Investigation
A 12-year-old girl
Investigation

Investigation
Investigation
Complete blood count
Hb 13.6 g/dL, Hct 43.3%
WBC 13,300/µL, N 75%, L
Complete blood count
Hb 13.6 g/dL, Hct 43.3%
WBC 13,300/µL, N 75%, L
Blood chemistry
BUN 19, Cr 0.35 mg/dL
Na 142, K 3.93, Cl 107,
Blood chemistry
BUN 19, Cr 0.35 mg/dL
Na 142, K 3.93, Cl 107,
Inflammatory markers
ESR 8 mm/hr
CRP < 1 mg/L
Inflammatory markers
ESR 8 mm/hr
CRP < 1 mg/L
Urinalysis
Sp. gr. 1.019, pH 5, protein negative, blood negative
WBC 0-1, RBC
Urinalysis
Sp. gr. 1.019, pH 5, protein negative, blood negative
WBC 0-1, RBC
Immunology
ANA negative
Immunology
ANA negative
CTA whole aorta
Diffuse mild to moderate irregular luminal narrowing involving celiac
CTA whole aorta
Diffuse mild to moderate irregular luminal narrowing involving celiac
CTA whole aorta
Surrounding soft tissue thickening with delayed mural enhancement at
CTA whole aorta
Surrounding soft tissue thickening with delayed mural enhancement at
CTA whole aorta
CTA whole aorta
CTA whole aorta
CTA whole aorta
CTA whole aorta
CTA whole aorta
CTA whole aorta
CTA whole aorta
CTA whole aorta
CTA whole aorta
CTA whole aorta
CTA whole aorta

CTA whole aorta
CTA whole aorta
Electrocardiogram
Normal sinus rhythm, rate 110/min, normal axis
No chamber enlargement
Electrocardiogram
Normal sinus rhythm, rate 110/min, normal axis
No chamber enlargement
Echocardiogram
Normal cardiac function
Trivial to mild MR and AR
No coarctation of aorta
Echocardiogram
Normal cardiac function
Trivial to mild MR and AR
No coarctation of aorta
Eye examination
VA: Rt 20/80, 20/50 with PH
Lt 20/50, 20/40 with
Eye examination
VA: Rt 20/80, 20/50 with PH Lt 20/50, 20/40 with
Audiogram
Moderately severe sensorineural hearing loss both ears
Audiogram
Moderately severe sensorineural hearing loss both ears
A 12-year-old girl
Differential diagnosis
A 12-year-old girl
Differential diagnosis
Differential diagnosis
Takayasu arteritis
Cogan’s syndrome
Vogt-Koyanagi-Harada syndrome
Differential diagnosis
Takayasu arteritis
Cogan’s syndrome
Vogt-Koyanagi-Harada syndrome
Differential diagnosis
Differential diagnosis
Takayasu arteritis (TA)
Arteritis, often granulomatous
Predominantly affecting the aorta and/or its major
Takayasu arteritis (TA)
Arteritis, often granulomatous
Predominantly affecting the aorta and/or its major
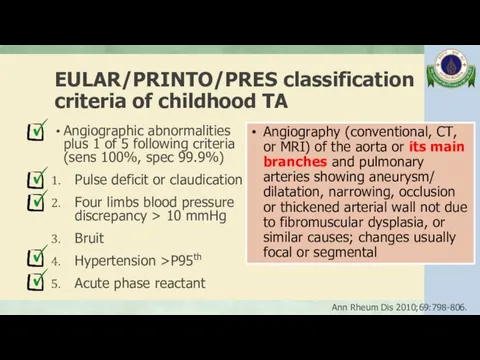
EULAR/PRINTO/PRES classification criteria of childhood TA
Angiographic abnormalities
plus 1 of 5
EULAR/PRINTO/PRES classification criteria of childhood TA
Angiographic abnormalities plus 1 of 5
Ocular manifestations in TA
Prevalence is varied from 8.1% - 68%
Retina 2011;31:1170-8.
Ocular manifestations in TA
Prevalence is varied from 8.1% - 68%
Retina 2011;31:1170-8.
Ocular manifestations in TA
Retrospective cohort 78 TA patients, Korea
Cross-sectional study
Ocular manifestations in TA
Retrospective cohort 78 TA patients, Korea
Cross-sectional study
Ocular manifestations in TA
Retrospective cohort 78 TA patients, Korea
Cross-sectional study
Ocular manifestations in TA
Retrospective cohort 78 TA patients, Korea
Cross-sectional study
SNHL in TA
Few case reports of SNHL associated with TA
Many reports
SNHL in TA
Few case reports of SNHL associated with TA
Many reports
SNHL in TA
The cause of the hearing impairment associated with TA
SNHL in TA
The cause of the hearing impairment associated with TA
SNHL in TA
The mechanisms of the hearing loss in TA are
SNHL in TA
The mechanisms of the hearing loss in TA are
TA without involvement of aorta
Retrospective review 85 CT angiography in TA
TA without involvement of aorta
Retrospective review 85 CT angiography in TA
Cogan’s syndrome (CS)
Characterized by ocular inflammatory lesions, including interstitial keratitis, uveitis,
Cogan’s syndrome (CS)
Characterized by ocular inflammatory lesions, including interstitial keratitis, uveitis,
Typical CS
Defined by following 3 conditions:
(1) Ocular symptoms typically
Typical CS
Defined by following 3 conditions:
(1) Ocular symptoms typically
Atypical CS
Any of following conditions:
(1) Inflammatory ocular manifestations including
Atypical CS
Any of following conditions:
(1) Inflammatory ocular manifestations including
Ocular manifestations in CS
80% Interstitial keratitis, mostly bilateral involvement; inflamed small
Ocular manifestations in CS
80% Interstitial keratitis, mostly bilateral involvement; inflamed small
Audiovestibular manifestations in CS
Sudden onset of hearing loss, vertigo, tinnitus, nausea,
Audiovestibular manifestations in CS
Sudden onset of hearing loss, vertigo, tinnitus, nausea,
Vasculitic manifestations in CS
May include arteritis (affecting small, medium, or large
Vasculitic manifestations in CS
May include arteritis (affecting small, medium, or large
Vogt-Koyanagi-Harada syndrome (VKH)
Systemic autoimmune disease; main target is melanin-containing-cells present in
Vogt-Koyanagi-Harada syndrome (VKH)
Systemic autoimmune disease; main target is melanin-containing-cells present in
Clinical course of VKH
Prodromal phase: Few days prior to ocular symptoms,
Clinical course of VKH
Prodromal phase: Few days prior to ocular symptoms,
Revise diagnostic criteria of VKH
Complete disease; criteria 1 to 5 must
Revise diagnostic criteria of VKH
Complete disease; criteria 1 to 5 must
Revise diagnostic criteria of VKH
(1) No history of penetrating ocular trauma
Revise diagnostic criteria of VKH
(1) No history of penetrating ocular trauma
Ocular manifestations in VKH
The posterior manifestation is the hallmark, demonstrating vitreous
Ocular manifestations in VKH
The posterior manifestation is the hallmark, demonstrating vitreous
Ocular manifestations in VKH
Signs of depigmentation:
- Sunset glow: changes of
Ocular manifestations in VKH
Signs of depigmentation: - Sunset glow: changes of
Audiovestibular manifestations in VKH
SNHL (27-50%), tinnitus (34-43%) and vertigo/dizziness (4-25%)
Typically
Audiovestibular manifestations in VKH
SNHL (27-50%), tinnitus (34-43%) and vertigo/dizziness (4-25%)
Typically
Vasculitis in VKH
Case report of a 44-year-old female in Japan, developed
Vasculitis in VKH
Case report of a 44-year-old female in Japan, developed
A 12-year-old girl
Management
A 12-year-old girl
Management
Management
J Cliln Pathol 2002;55:481-6.
Autoimmun Rev 2016;15:809-19.
J Multidiscip Healthc 2017;11:1-11.
Management
J Cliln Pathol 2002;55:481-6.
Autoimmun Rev 2016;15:809-19.
J Multidiscip Healthc 2017;11:1-11.
Management in this patient
1/11/17
14/12/17
Prednisolone (5) 4x2 [1 MKD]
MTX (2.5) 5 tab
Management in this patient
1/11/17
14/12/17
Prednisolone (5) 4x2 [1 MKD]
MTX (2.5) 5 tab
![Management in this patient 11/1/18 IV Cyclophosphamide [2nd dose] Prednisolone](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/423837/slide-64.jpg)
Management in this patient
11/1/18
IV Cyclophosphamide [2nd dose]
Prednisolone (5) 2x2 [0.4 MKD]
ASA
Management in this patient
11/1/18
IV Cyclophosphamide [2nd dose]
Prednisolone (5) 2x2 [0.4 MKD]
ASA
Take home message
Takayasu arteritis:
Uveitis is uncommon ocular manifestation
Isolated branch vessel
Take home message
Takayasu arteritis:
Uveitis is uncommon ocular manifestation
Isolated branch vessel
Thank you
Thank you
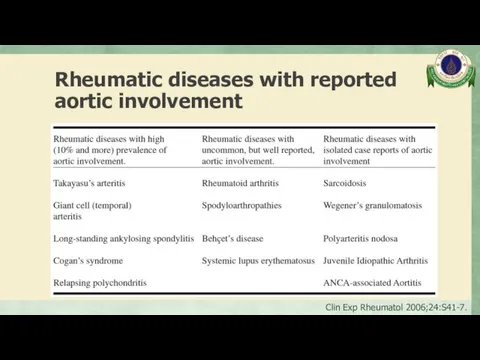
Rheumatic diseases with reported aortic involvement
Clin Exp Rheumatol 2006;24:S41-7.
Rheumatic diseases with reported aortic involvement
Clin Exp Rheumatol 2006;24:S41-7.
Vasculitis
Inflammation of blood vessel walls
The inflammatory infiltrate may be one
Vasculitis
Inflammation of blood vessel walls
The inflammatory infiltrate may be one
Vasculitis
Arthritis Rheum 2013;65:1-11.
Vasculitis
Arthritis Rheum 2013;65:1-11.
Vasculitis
Arthritis Rheum 2013;65:1-11.
Vasculitis
Arthritis Rheum 2013;65:1-11.
Vasculitis
Arthritis Rheum 2013;65:1-11.
Vasculitis
Arthritis Rheum 2013;65:1-11.
Vasculitis
Arthritis Rheum 2013;65:1-11.
Vasculitis
Arthritis Rheum 2013;65:1-11.
Vasculitis
Arthritis Rheum 2013;65:1-11.
Vasculitis
Arthritis Rheum 2013;65:1-11.
Aortitis
Pathological term for inflammation of the aortic wall
The classification of aortitis
Aortitis
Pathological term for inflammation of the aortic wall
The classification of aortitis
Clinical presentation
Asymptomatic
General syndrome: fever, malaise, weight loss, high ESR
Pain (chest, back,
Clinical presentation
Asymptomatic
General syndrome: fever, malaise, weight loss, high ESR
Pain (chest, back,
Causes of aortitis
Inflammatory:
Large vessel vasculitis: TAK, GCA
Rheumatoid arthritis
Systemic lupus erythematosus
HLA-B27
Causes of aortitis
Inflammatory:
Large vessel vasculitis: TAK, GCA
Rheumatoid arthritis
Systemic lupus erythematosus
HLA-B27
Causes of aortitis
Isolated aortitis:
Isolated idiopathic (thoracic aortitis)
Chronic periaortitis: Idiopathic retroperitoneal
Causes of aortitis
Isolated aortitis:
Isolated idiopathic (thoracic aortitis)
Chronic periaortitis: Idiopathic retroperitoneal
Causes of aortitis
Infectious:
Bacteria: Salmonella spp., Staphylococcus spp., Streptococcus pneumoniae, other
Syphilis
Mycobacterium
Other
Circulation
Causes of aortitis
Infectious:
Bacteria: Salmonella spp., Staphylococcus spp., Streptococcus pneumoniae, other
Syphilis
Mycobacterium
Other
Circulation
Laboratory testing
Markers of inflammation: ESR, CRP
Complete blood count
Kidney and liver function
Additional
Laboratory testing
Markers of inflammation: ESR, CRP
Complete blood count
Kidney and liver function
Additional
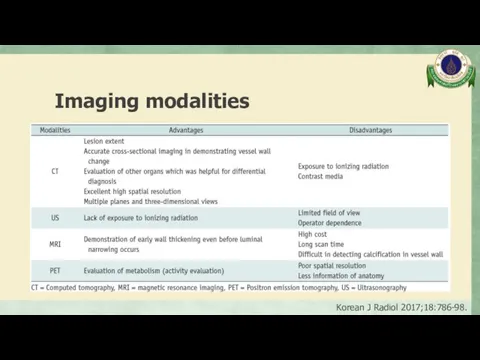
Imaging modalities
Korean J Radiol 2017;18:786-98.
Imaging modalities
Korean J Radiol 2017;18:786-98.
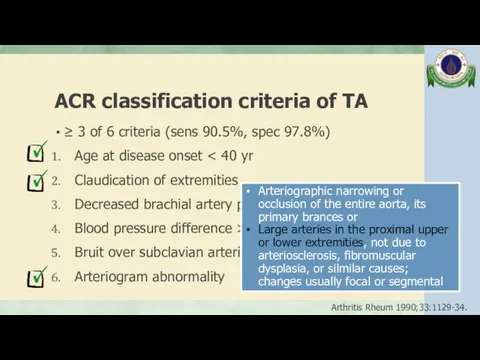
ACR classification criteria of TA
≥ 3 of 6 criteria (sens 90.5%,
ACR classification criteria of TA
≥ 3 of 6 criteria (sens 90.5%,
Takayasu arteritis (TA)
Incidence 0.4-1 case/1,000,000/year
Onset usually occurs before the age of
Takayasu arteritis (TA)
Incidence 0.4-1 case/1,000,000/year
Onset usually occurs before the age of
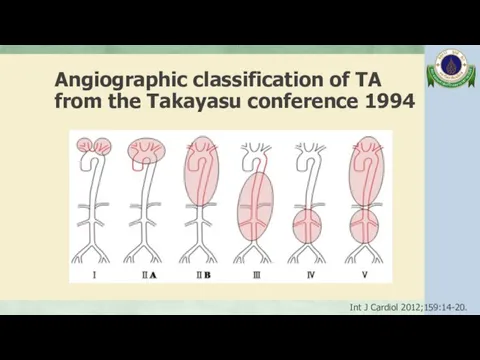
Angiographic classification of TA from the Takayasu conference 1994
Int J Cardiol
Angiographic classification of TA from the Takayasu conference 1994
Int J Cardiol
 Немедикаментозное лечение и профилактика кардиоваскулярных заболеваний
Немедикаментозное лечение и профилактика кардиоваскулярных заболеваний Медико-генетикалық кеңестің нәрестенің туа біткен ақаулықтарын алдын-алудағы рөлі және диагностикасы
Медико-генетикалық кеңестің нәрестенің туа біткен ақаулықтарын алдын-алудағы рөлі және диагностикасы Респираторные формы аллергии у детей
Респираторные формы аллергии у детей Медицинская арахноэнтомология
Медицинская арахноэнтомология Лечебно-охранительный режим ЛПУ. Безопасная больничная среда
Лечебно-охранительный режим ЛПУ. Безопасная больничная среда Психологические аспекты тандема врач-ассистент-пациент
Психологические аспекты тандема врач-ассистент-пациент Желчегонные средства
Желчегонные средства Консультирование больных с метаболическим синдромом
Консультирование больных с метаболическим синдромом Дүниежүзілік денсаулық сақтау ұйымы (ДДҰ) Қазақстанда
Дүниежүзілік денсаулық сақтау ұйымы (ДДҰ) Қазақстанда Факторы здоровья
Факторы здоровья Заполнение данных о работе скорой, в том числе скорой специализированной, медицинской помощи
Заполнение данных о работе скорой, в том числе скорой специализированной, медицинской помощи История нейрохирургии
История нейрохирургии Традиционная гигиена в античную эпоху древней Греции и Римской империи
Традиционная гигиена в античную эпоху древней Греции и Римской империи Лечебное воздействие звука на человека. Человек - отражение вселенной
Лечебное воздействие звука на человека. Человек - отражение вселенной Болезнь Виллебранда
Болезнь Виллебранда Переливание крови
Переливание крови Нейропластичность и нейродегенерация
Нейропластичность и нейродегенерация Искусственная вентиляция легких
Искусственная вентиляция легких Строение и работа мышц
Строение и работа мышц Дивертикул толстой кишки
Дивертикул толстой кишки Закрытая травма живота у детей
Закрытая травма живота у детей Заикание у детей и взрослых
Заикание у детей и взрослых Медико-этические и социально-правовые аспекты современной трансплантологии
Медико-этические и социально-правовые аспекты современной трансплантологии Стационардағы медбикенің қол жуу маңыздылығы
Стационардағы медбикенің қол жуу маңыздылығы Профилактика туберкулеза. Диспансерное наблюдение, группы учета. Вакцинация БЦЖ и ее осложнения
Профилактика туберкулеза. Диспансерное наблюдение, группы учета. Вакцинация БЦЖ и ее осложнения Первая помощь при отравлениях
Первая помощь при отравлениях ECA solutions for poultry farming
ECA solutions for poultry farming Патология многоплодной беременности
Патология многоплодной беременности