- Investigation of the urinary system

Содержание
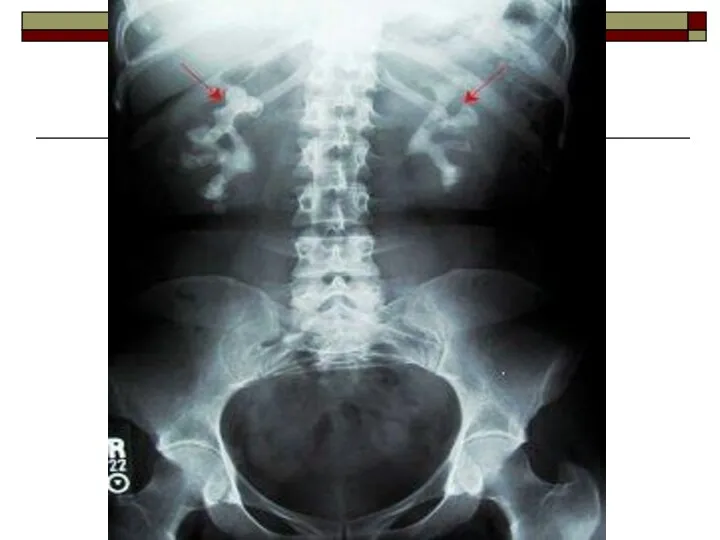
- 2. Plain Film: Plain film is taken in supine position. The radiograph should include the upper poles
- 3. This may show renal calculi in the pelvicalyceal system renal parenchymal calcification ureteric calculi bladder calcification
- 4. Caution should be used in interpreting renal-tract calcification as overlying calcified mesenteric glands and pelvic vein
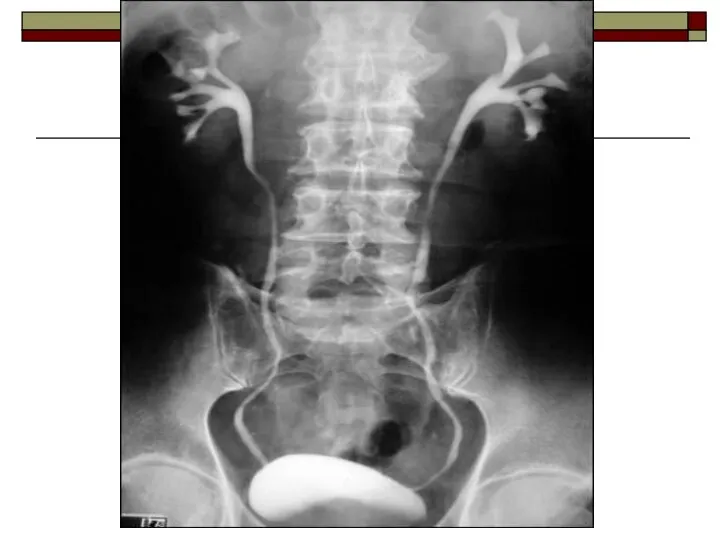
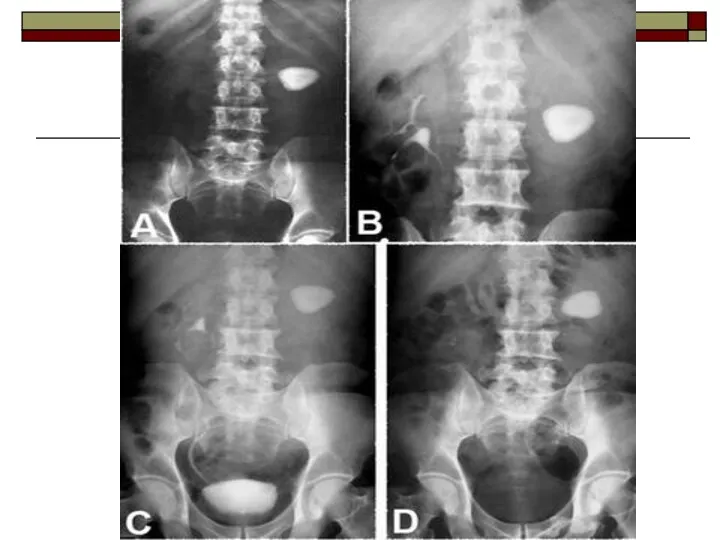
- 8. Intravenous Urography (IVU): IVU is frequently performed in the evaluation of hematuria. Urography may also be
- 9. Indications obstructive calculi hematuria or pyuria diseases of renal collecting system and renal pelvis abnormalities of
- 10. Patient preparation blood urea and serum creatinine level should be within normal limits if patient is
- 11. patient should be well hydrated (dehydrated patients are prone for renal damage) bowel preparation is necessary,
- 12. Bowel wash is given till bowel is clear of faecal matter on previous night. Laxatives (ducolax,
- 13. Procedure Patient is placed in supine position. The patient is asked to void the bladder before
- 14. Contrast media is injected intravenously into a prominent vein in the arm. Test injection of 1ml
- 15. Contrast media Contrast materials currently in use are excreted almost exclusively by glomerular filtration, with subsequent
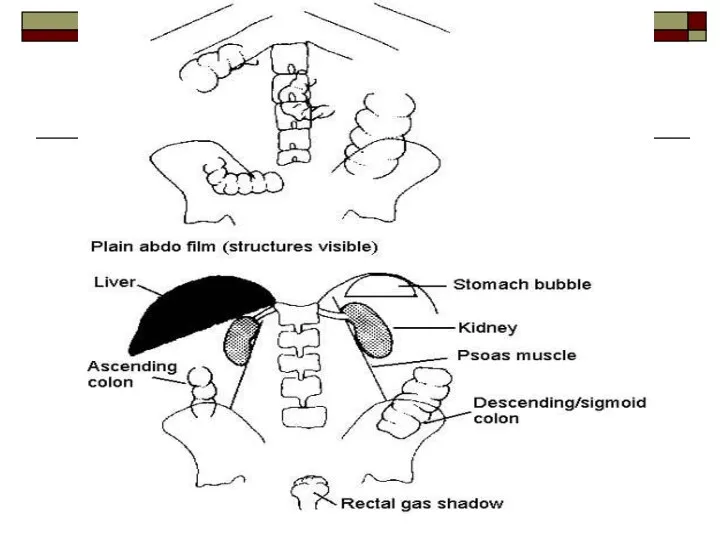
- 16. Filming technique and interpretation Plain x-ray (scout film) It gives information about: renal outlines psoas muscles
- 17. 5-10 min film Shows nephrogram, renal pelvis 15-20 min film A complete visualization of the pelvicalyceal
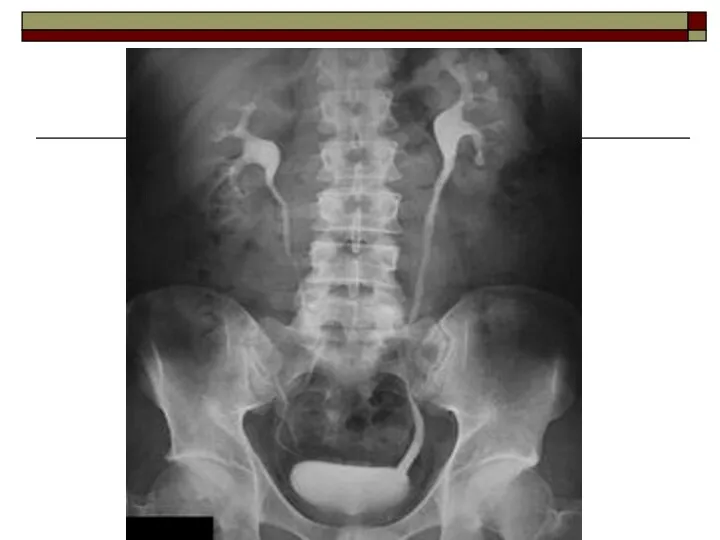
- 18. 30-35 min film A complete visualization of the urinary tract: kidney, ureter, bladder can be done
- 19. Post void film It taken immediately after voiding. To assess for: residual urine bladder mucosal lesions
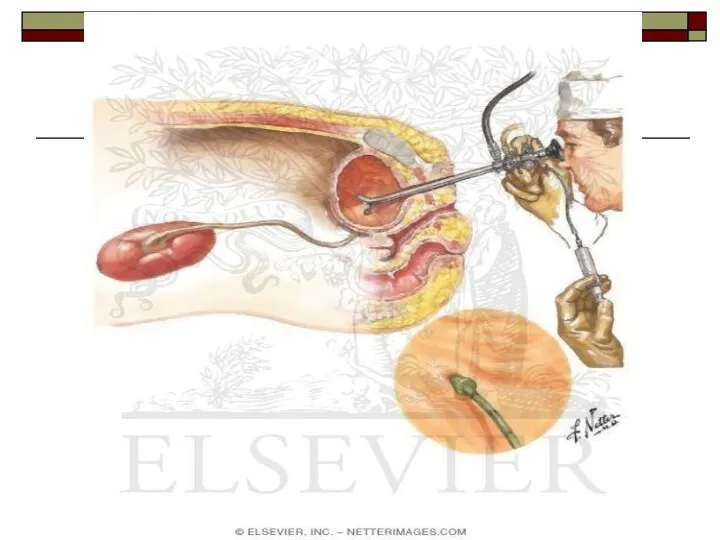
- 26. Retrograde pyelography A retrograde pyelography is occasionally necessary when detail of the pelvicalyceal system and ureter
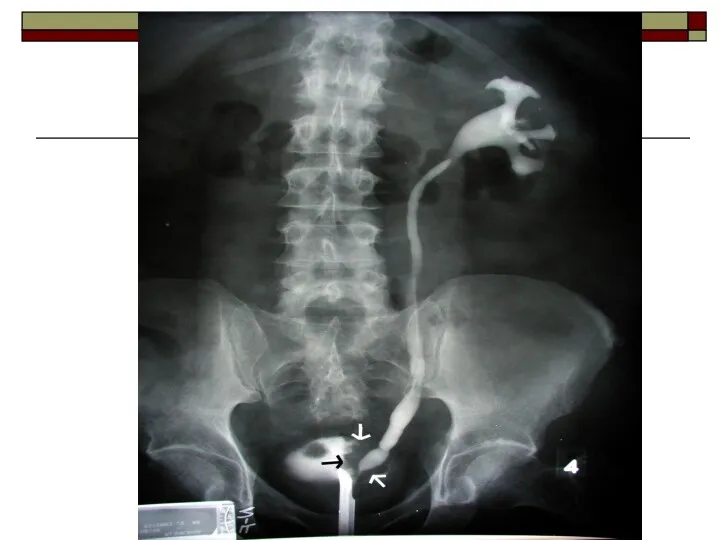
- 30. Antegrade pyelography A fine-gauge needle, under local anesthetic, can be inserted directly into the pelvicalyceal system
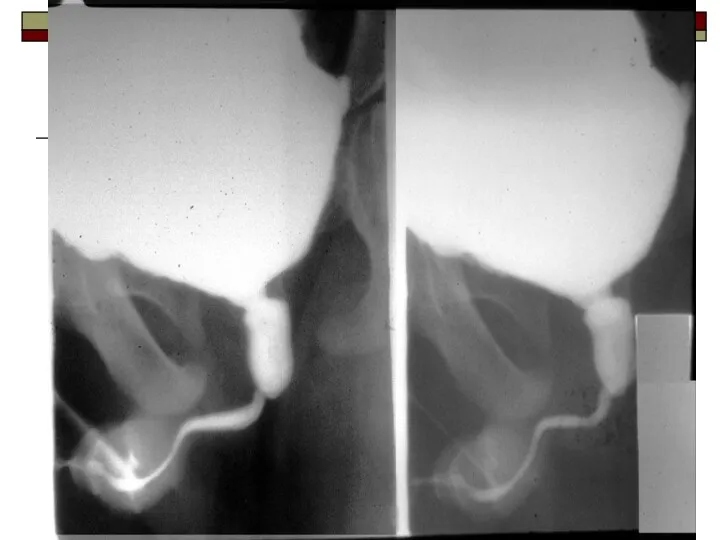
- 32. Micturating cystogram A catheter is inserted in the bladder which is filled to capacity with contrast.
- 33. Indications Children: vesico-ureteric reflux post urinary tract infection trauma hematuria posterior urethral valve voiding difficulties like
- 34. Adults: trauma to urethra urethral stricture urethral diverticula vesico-ureteric reflux
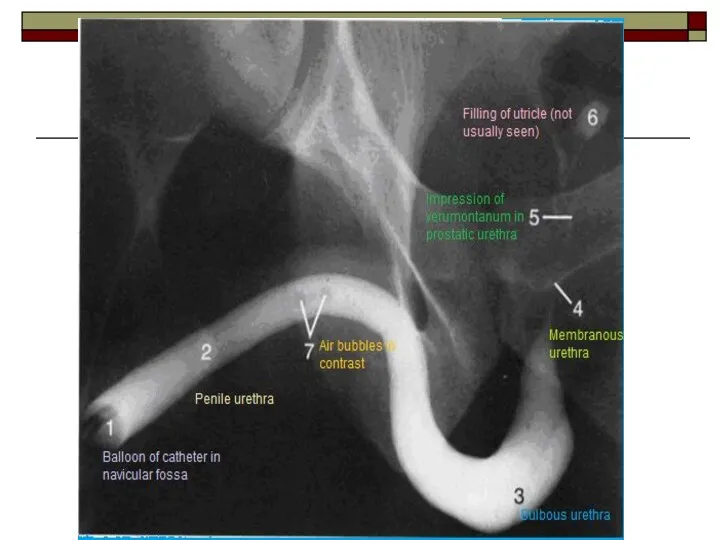
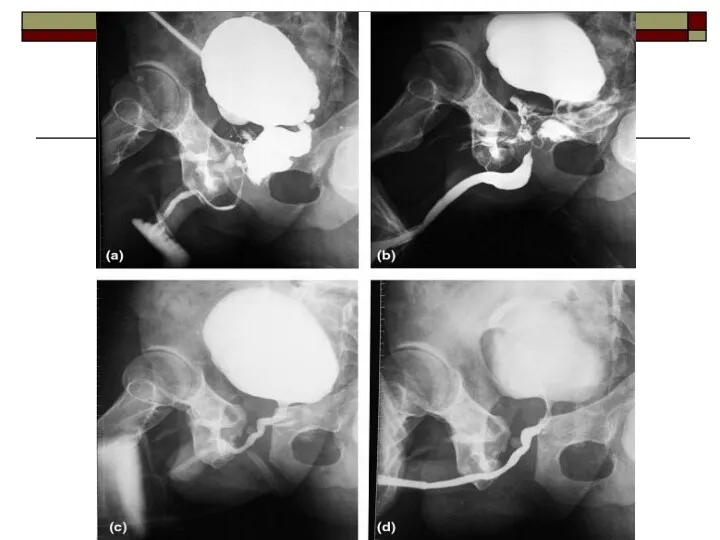
- 36. Urethrography The adult male urethra can be visualized by: ascending urethrography: contrast is injected into the
- 40. Ultrasound Ultrasound is one of the most valuable investigations of the urinary tract and the investigation
- 41. renal obstruction urinary tract infection hematuria congenital abnormalities renal failure transplants bladder residual volumes prostatic size
- 42. Urinary bladder
- 43. Isotope Scanning: Static Scanning: Technetium-99m DMSA: Selective uptake by the renal cells with stagnation in the
- 44. Dynamic scanning: Technetium-99m DTPA: Isotope clearance by glomerular filtration produces a dynamic scan, providing information on
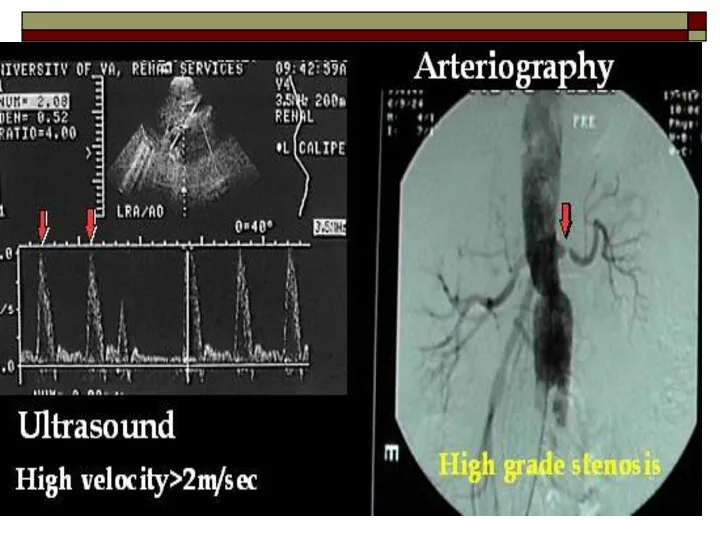
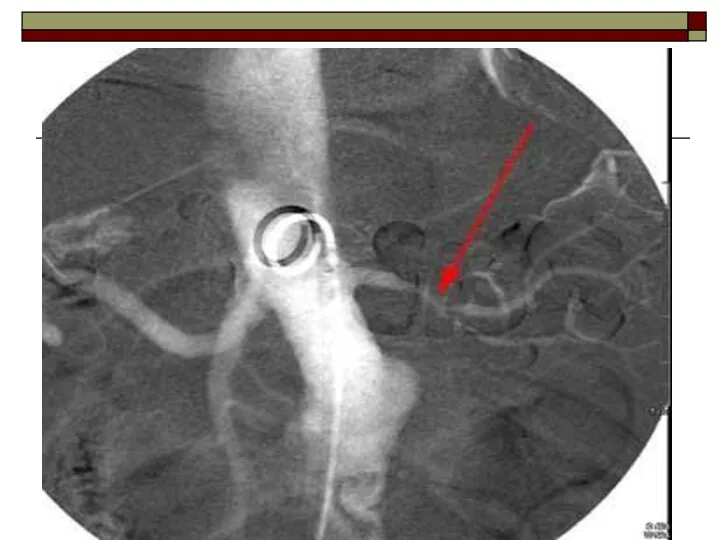
- 47. . Arteriography: Evaluation of the renal arterial circulation may be necessary for: further investigation of equivocal
- 50. Computed tomography This aids assessment of: renal masses – especially differentiation of solid and cystic lesions
- 54. Congenital anomalies Ectopic kidney Normally the kidneys are located in the abdomen adjacent to the upper
- 56. Crossed fused ectopia The two renal masses fuse with each other however the ureters draining the
- 57. Horse shoe kidney Is a fusion of lower poles of both the kidneys occurs by either
- 58. IVU: may demonstrate the isthmus which connects the two kidneys. There is some degree of malrotation
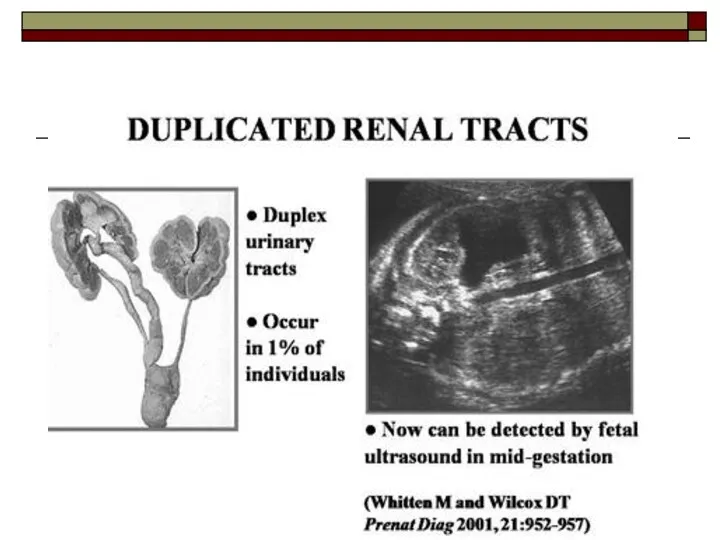
- 63. Duplex Kidney: the commonest renal anomaly with a variable degree of duplication ranging from minor changes
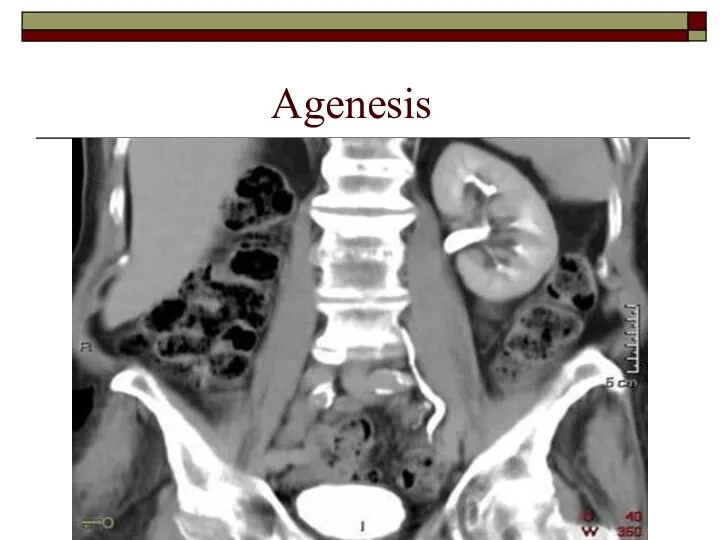
- 68. Agenesis
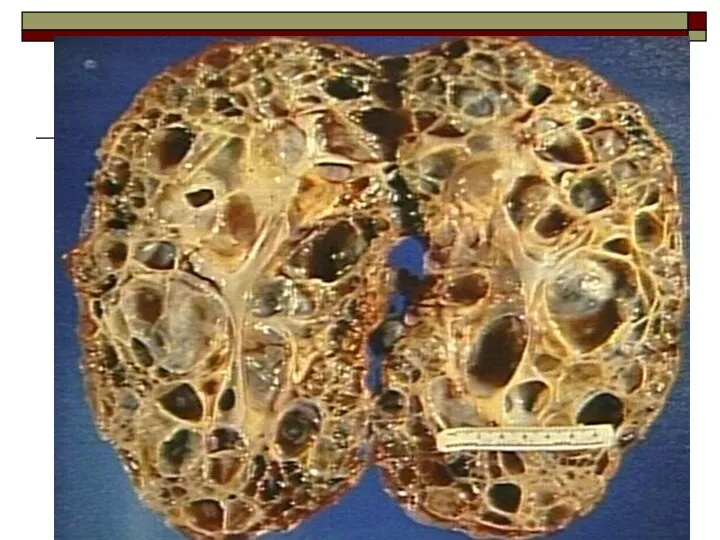
- 69. Polycystic kidney disease Clinical features hypertension bilaterally enlargement kidneys as masses per abdomen loin pain rarely
- 70. IVU major calyces may be displaced, narrowed and elongated by adjacent cyst in advanced cases there
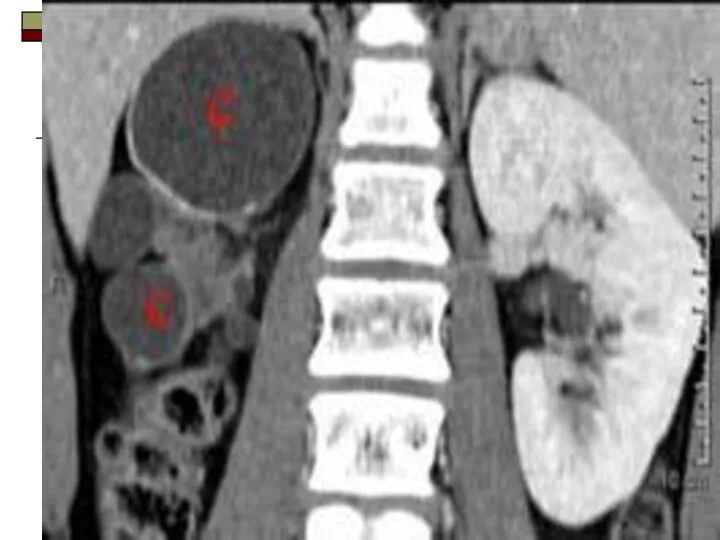
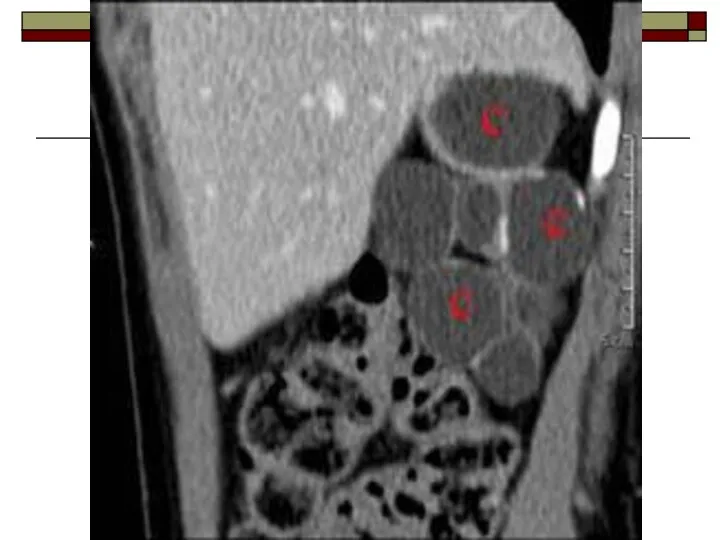
- 71. Ultrasound enlarged kidneys cysts are seen as anechoic lesions (black) with distal acoustic enhancement CT cysts
- 78. Retrocaval ureter Normally the right ureter lies anterolateral to the inferior vena cava. Occasionally the right
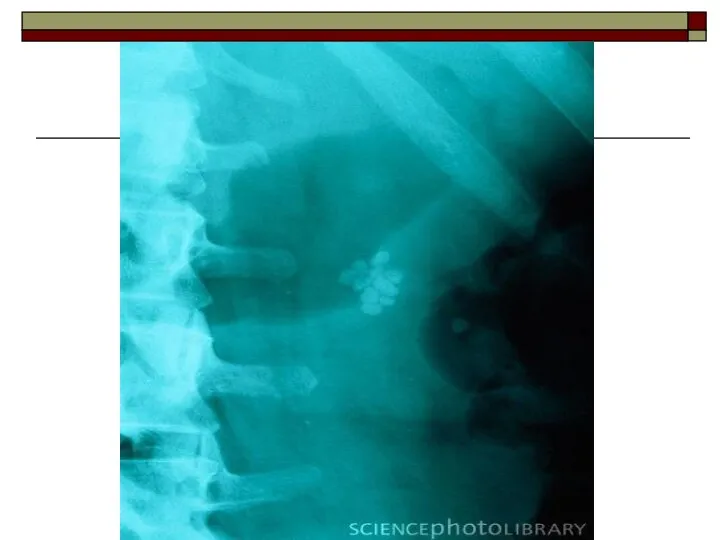
- 81. Urinary tract stones Urinary tract stones are the stones within the collecting system which are due
- 82. Radio lucent stones: uric acid stones xanthine stones Radiolucent stones are not visualized on x-ray, however,
- 83. Ultrasound Stones will be seen as hyperechoic (bright) focus within the collecting system with distal shadowing.
- 88. Hydronephrosis Hydronephrosis is a dilatation of PCS secondary to distal obstruction. Causes ureteric stones ureteric stricture
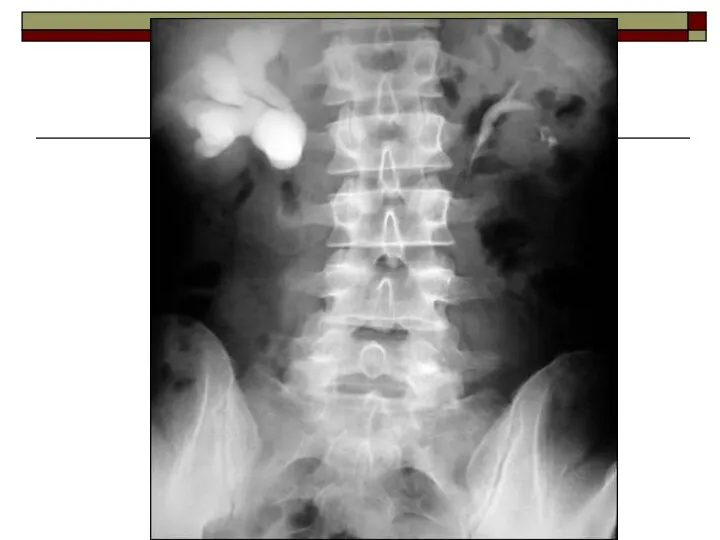
- 89. IVU Findings may vary with the duration and degree of the obstruction. Renal outline may be
- 90. Ultrasound dilatation of the collecting system will be seen as hypoechogenicity (dark) within the (bright) renal
- 94. Hydroureter Hydroureter is ureteric dilatation due to either obstructive or non obstructive causes. An absolute ureteral
- 95. Causes Ureteric calculus Ureteric stricture Ureterocele Congenital megaureter Retroperitoneal tumor/Retroperitoneal fibrosis Pelvic malignancies
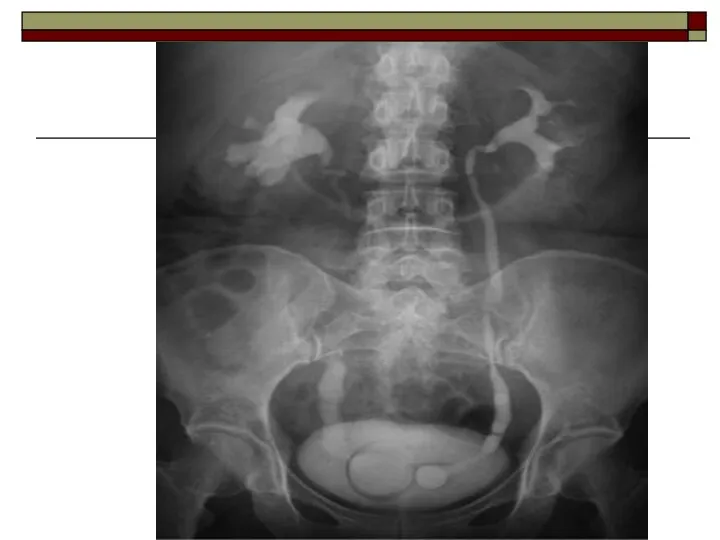
- 98. Ureterocele Submucosal dilatation of the intramural distal ureter which often protrudes into the bladder lumen is
- 103. Primary megaureter Primary megaureter is congenital abnormal musculature of the distal ureter, leading to focal failure
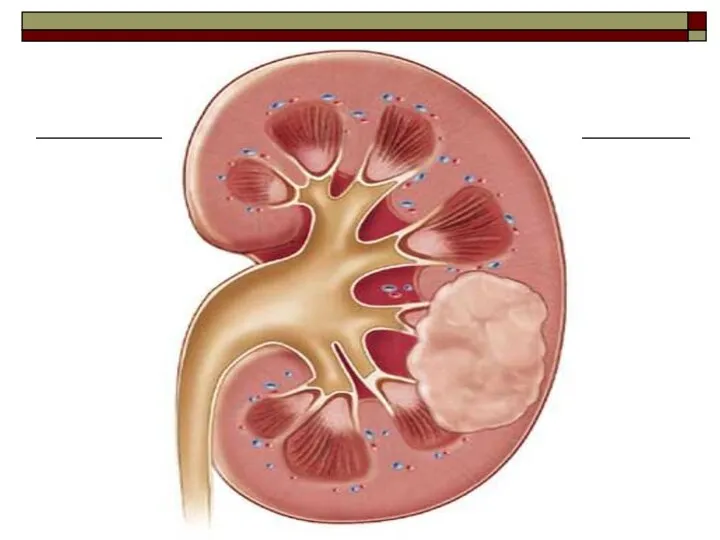
- 104. Renal cell carcinoma Common age of presentation between 50 to 70 years. Common urological malignancy in
- 105. IVU displacement, compression and cut off of calyces, change of axis of the kidney enlargement of
- 106. Ultrasound heterogenous echotexture lesion within the renal parenchyma CT scan highly vascular mass lesion which is
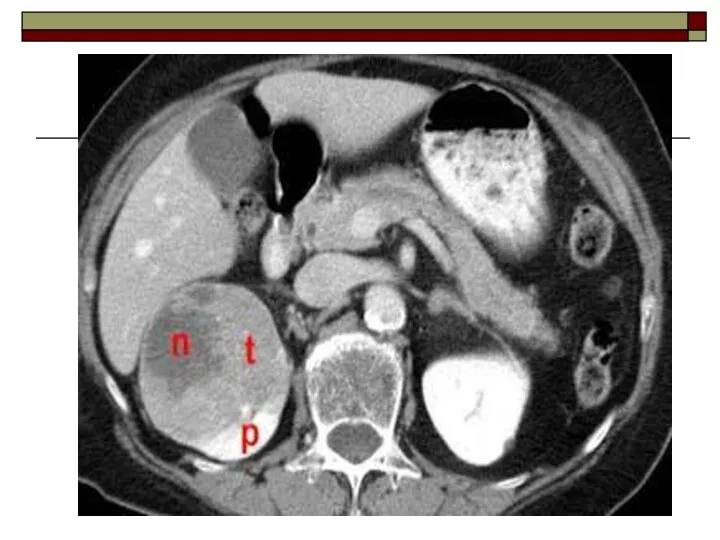
- 110. Wilms tumor commonest renal malignancy in children presents mainly between 1 to 5 years of age
- 111. IVU enlargement of affected part of the kidney distortion of the PCS by a tumor Ultrasound
- 114. Diverticulum of bladder It is outpouching of mucosa trough the walls of the bladder. Types: congenital
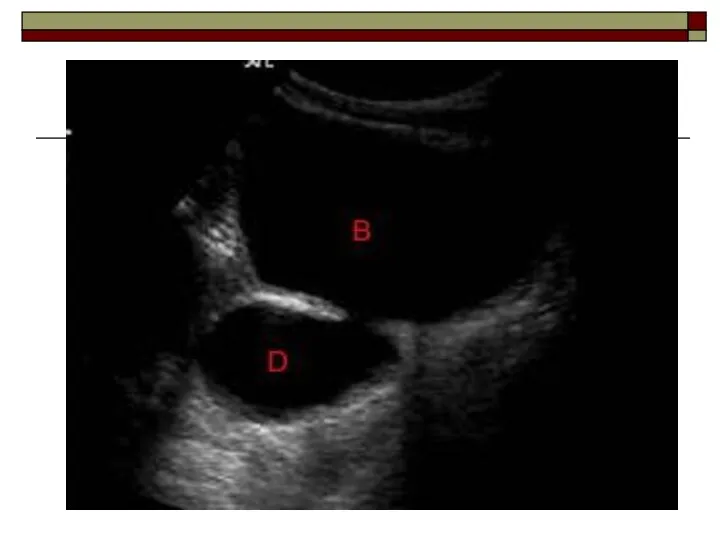
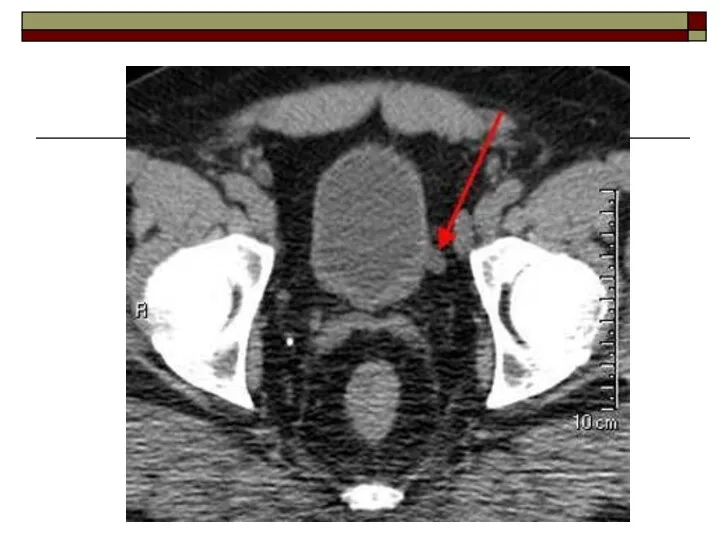
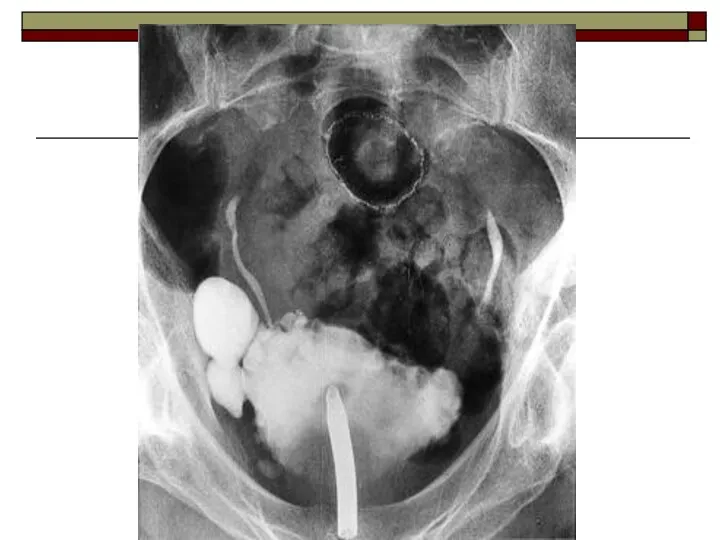
- 115. Imaging appearances the diverticulum may have wide neck or narrow neck in the diverticulum with wide
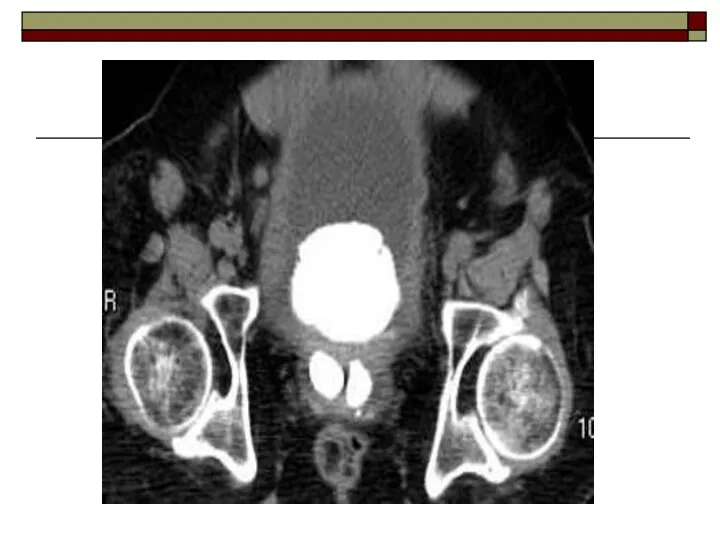
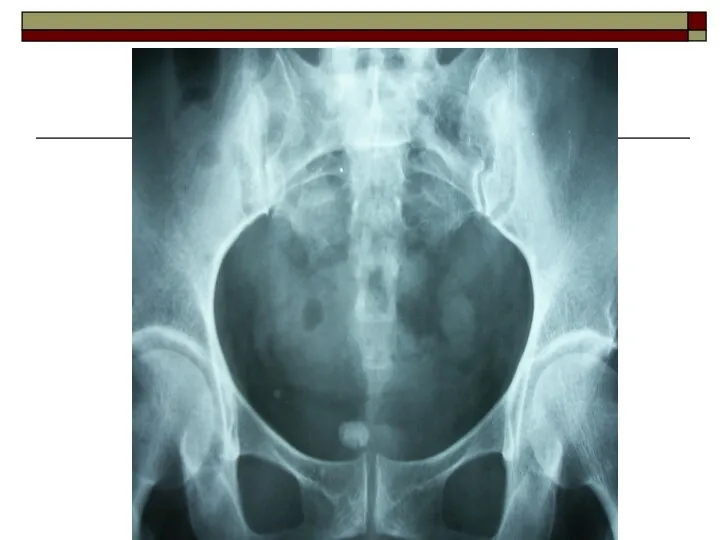
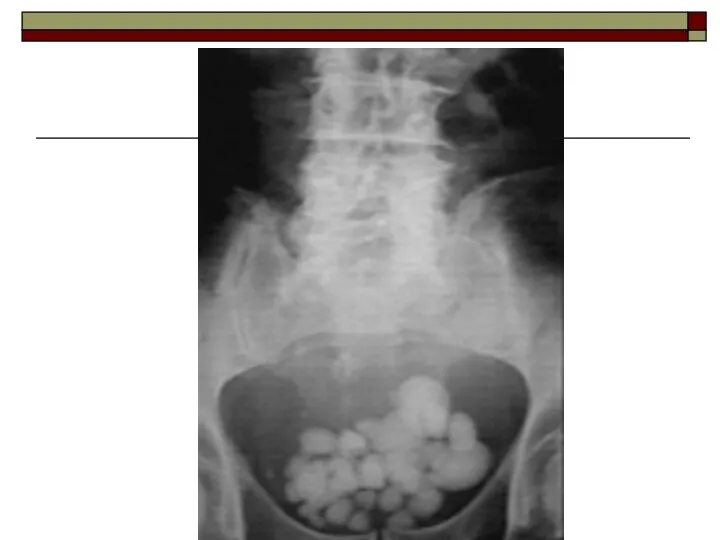
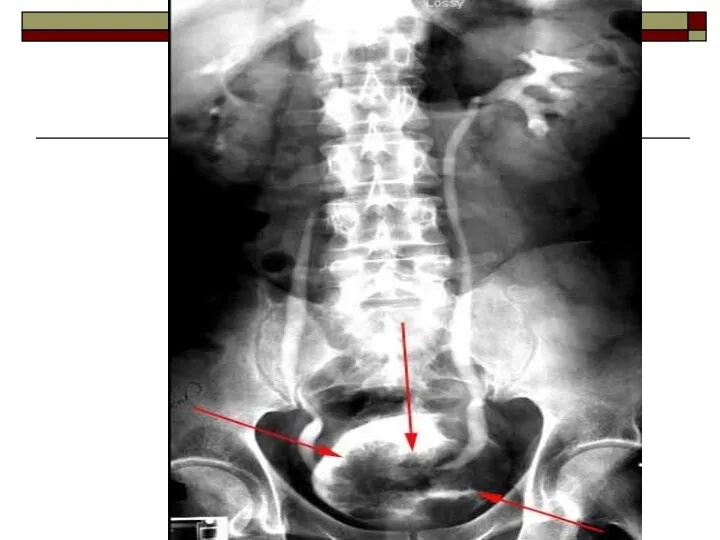
- 120. Bladder calculi usually secondary to outflow obstruction/bladder diverticula or urinary tract infections it may occur in
- 121. urinary bladder stones mimics phlebolith (stones in the venous wall) and should be differentiated from it:
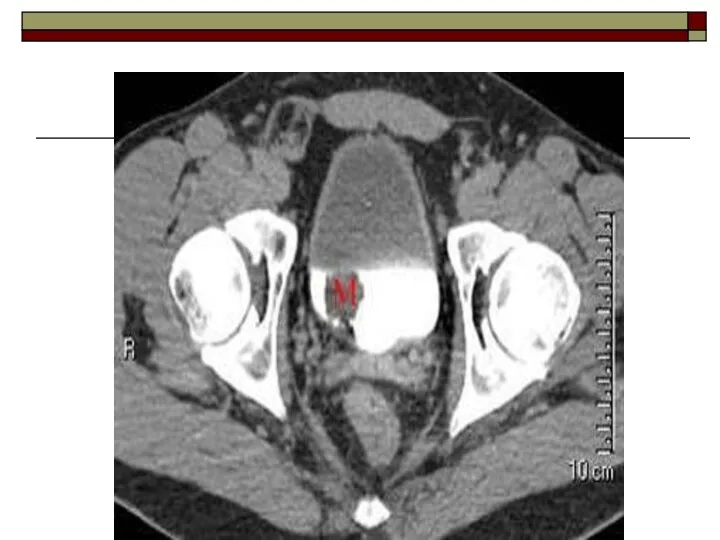
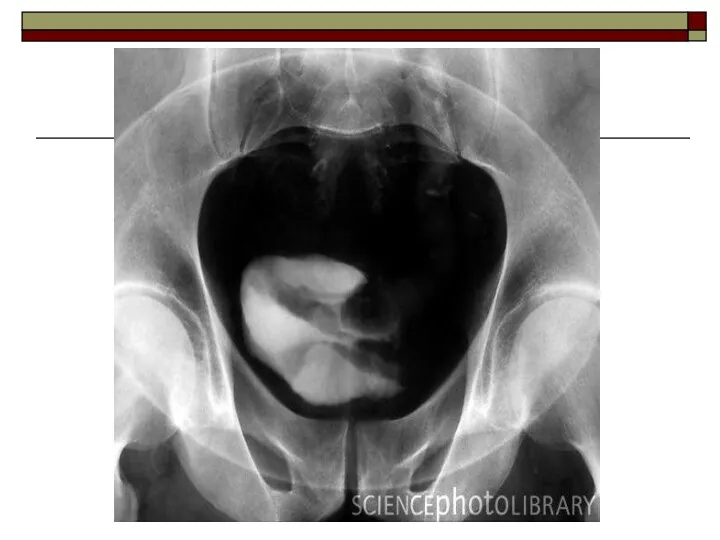
- 128. Bladder tumors It commonly occurs in posterior and lateral walls near vesico-ureteric junction. Types epithelial tumors:
- 129. Epithelial tumors: 90%-transitional cell ca 1-10%-squamous cell ca Clinical features painless hematuria Imaging
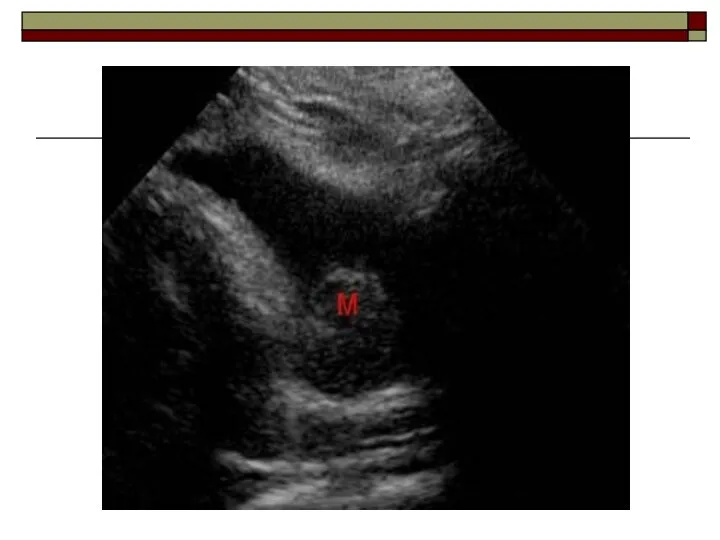
- 130. IVU filling defect in the bladder decreased capacity of bladder may not detect small tumors Ultrasound
- 136. Small smooth kidney Unilateral ischaemia due to renal artery stenosis post obstructive atrophy Bilateral arterial hypertension
- 138. Скачать презентацию
Plain Film:
Plain film is taken in supine position. The radiograph
Plain Film:
Plain film is taken in supine position. The radiograph
This may show
renal calculi in the pelvicalyceal system
renal parenchymal
This may show
renal calculi in the pelvicalyceal system
renal parenchymal
Caution should be used in interpreting renal-tract calcification as overlying
Caution should be used in interpreting renal-tract calcification as overlying

Intravenous Urography (IVU):
IVU is frequently performed in the evaluation of
Intravenous Urography (IVU):
IVU is frequently performed in the evaluation of
Indications
obstructive calculi
hematuria or pyuria
diseases of renal collecting system and renal pelvis
abnormalities
Indications
obstructive calculi
hematuria or pyuria
diseases of renal collecting system and renal pelvis
abnormalities
Patient preparation
blood urea and serum creatinine level should be within normal
Patient preparation
blood urea and serum creatinine level should be within normal
patient should be well hydrated (dehydrated patients are prone for renal
patient should be well hydrated (dehydrated patients are prone for renal
Bowel wash is given till bowel is clear of faecal matter
Bowel wash is given till bowel is clear of faecal matter
Procedure
Patient is placed in supine position. The patient is asked
Procedure
Patient is placed in supine position. The patient is asked
Contrast media is injected intravenously into a prominent vein in the
Contrast media is injected intravenously into a prominent vein in the
Contrast media
Contrast materials currently in use are excreted almost exclusively
Contrast media
Contrast materials currently in use are excreted almost exclusively
Filming technique and interpretation
Plain x-ray (scout film)
It gives information about:
renal
Filming technique and interpretation
Plain x-ray (scout film)
It gives information about:
renal
5-10 min film
Shows nephrogram, renal pelvis
15-20 min film
A complete visualization of
5-10 min film
Shows nephrogram, renal pelvis
15-20 min film
A complete visualization of
30-35 min film
A complete visualization of the urinary tract: kidney, ureter,
30-35 min film
A complete visualization of the urinary tract: kidney, ureter,
Post void film
It taken immediately after voiding.
To assess for:
residual
Post void film
It taken immediately after voiding.
To assess for:
residual

Retrograde pyelography
A retrograde pyelography is occasionally necessary when detail of
Retrograde pyelography
A retrograde pyelography is occasionally necessary when detail of

Antegrade pyelography
A fine-gauge needle, under local anesthetic, can be inserted
Antegrade pyelography
A fine-gauge needle, under local anesthetic, can be inserted

Micturating cystogram
A catheter is inserted in the bladder which is
Micturating cystogram
A catheter is inserted in the bladder which is
Indications
Children:
vesico-ureteric reflux
post urinary tract infection
trauma
hematuria
posterior urethral valve
voiding difficulties like dysuria,
Indications
Children:
vesico-ureteric reflux
post urinary tract infection
trauma
hematuria
posterior urethral valve
voiding difficulties like dysuria,
Adults:
trauma to urethra
urethral stricture
urethral diverticula
vesico-ureteric reflux
Adults:
trauma to urethra
urethral stricture
urethral diverticula
vesico-ureteric reflux
Urethrography
The adult male urethra can be visualized by:
ascending urethrography: contrast
Urethrography
The adult male urethra can be visualized by:
ascending urethrography: contrast

Ultrasound
Ultrasound is one of the most valuable investigations of the
Ultrasound
Ultrasound is one of the most valuable investigations of the
renal obstruction
urinary tract infection
hematuria
congenital abnormalities
renal failure
transplants
bladder residual volumes
prostatic size
it is non-invasive
renal obstruction
urinary tract infection
hematuria
congenital abnormalities
renal failure
transplants
bladder residual volumes
prostatic size
it is non-invasive
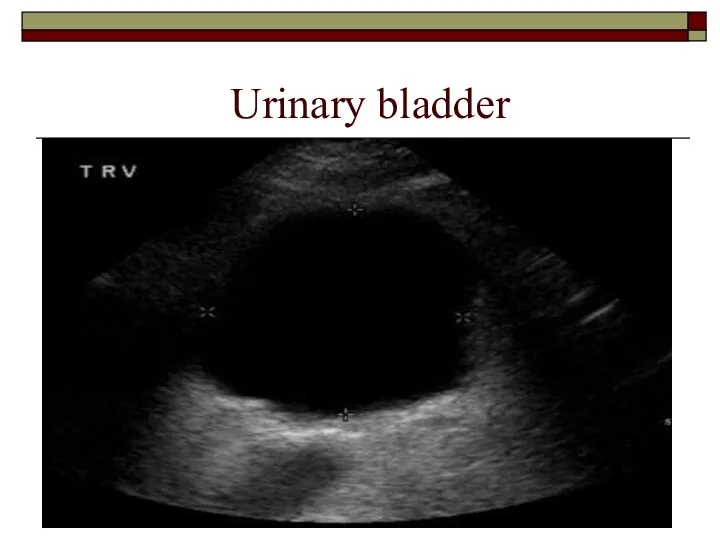
Urinary bladder
Urinary bladder
Isotope Scanning:
Static Scanning: Technetium-99m DMSA:
Selective uptake by the
Isotope Scanning:
Static Scanning: Technetium-99m DMSA:
Selective uptake by the
Dynamic scanning: Technetium-99m DTPA:
Isotope clearance by glomerular filtration produces a
Dynamic scanning: Technetium-99m DTPA:
Isotope clearance by glomerular filtration produces a
.
Arteriography:
Evaluation of the renal arterial circulation may be necessary for:
.
Arteriography:
Evaluation of the renal arterial circulation may be necessary for:
Computed tomography
This aids assessment of:
renal masses – especially differentiation of
Computed tomography
This aids assessment of:
renal masses – especially differentiation of



Congenital anomalies
Ectopic kidney
Normally the kidneys are located in the abdomen
Congenital anomalies
Ectopic kidney
Normally the kidneys are located in the abdomen

Crossed fused ectopia
The two renal masses fuse with each other
Crossed fused ectopia
The two renal masses fuse with each other
Horse shoe kidney
Is a fusion of lower poles of both
Horse shoe kidney
Is a fusion of lower poles of both
IVU: may demonstrate the isthmus which connects the two kidneys. There
IVU: may demonstrate the isthmus which connects the two kidneys. There
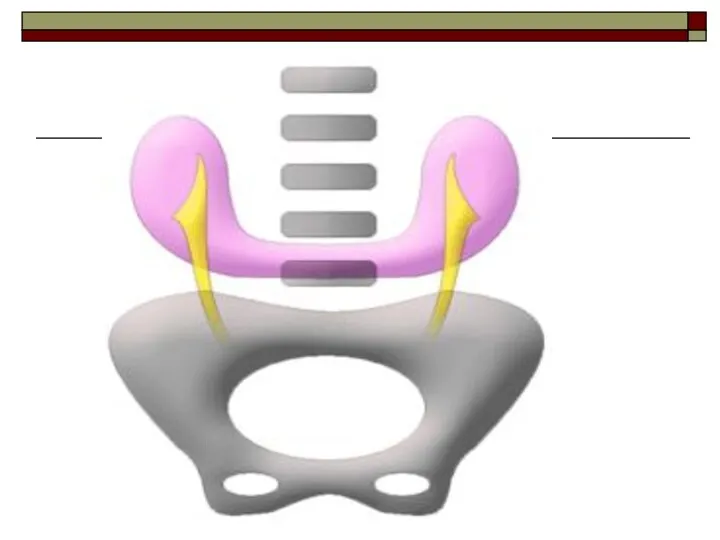
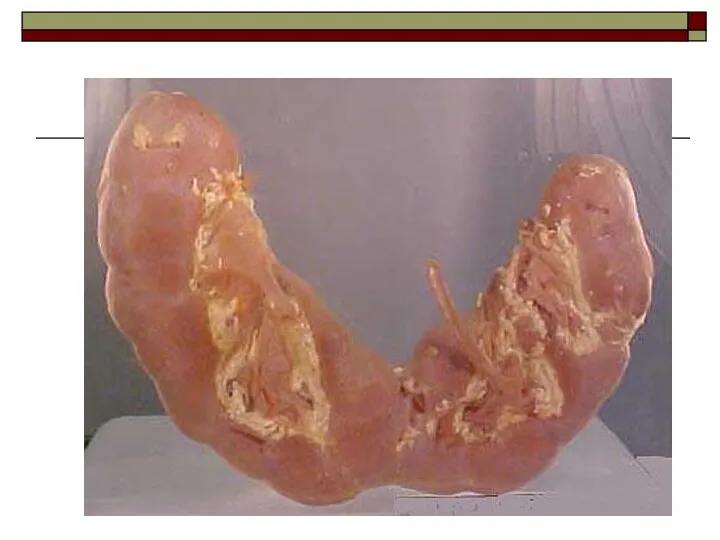
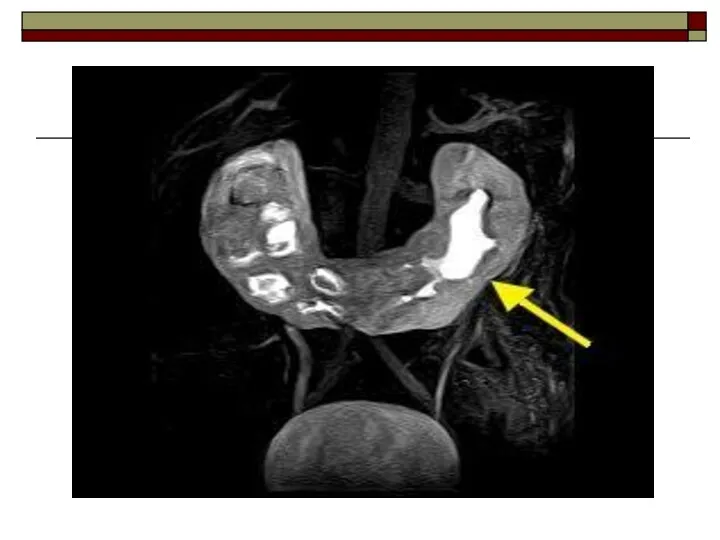

Duplex Kidney:
the commonest renal anomaly with a variable degree of
Duplex Kidney:
the commonest renal anomaly with a variable degree of



Agenesis
Agenesis
Polycystic kidney disease
Clinical features
hypertension
bilaterally enlargement kidneys as masses per abdomen
loin
Polycystic kidney disease
Clinical features
hypertension
bilaterally enlargement kidneys as masses per abdomen
loin
IVU
major calyces may be displaced, narrowed and elongated by adjacent cyst
in
IVU
major calyces may be displaced, narrowed and elongated by adjacent cyst
in
Ultrasound
enlarged kidneys
cysts are seen as anechoic lesions (black) with distal acoustic
Ultrasound
enlarged kidneys
cysts are seen as anechoic lesions (black) with distal acoustic


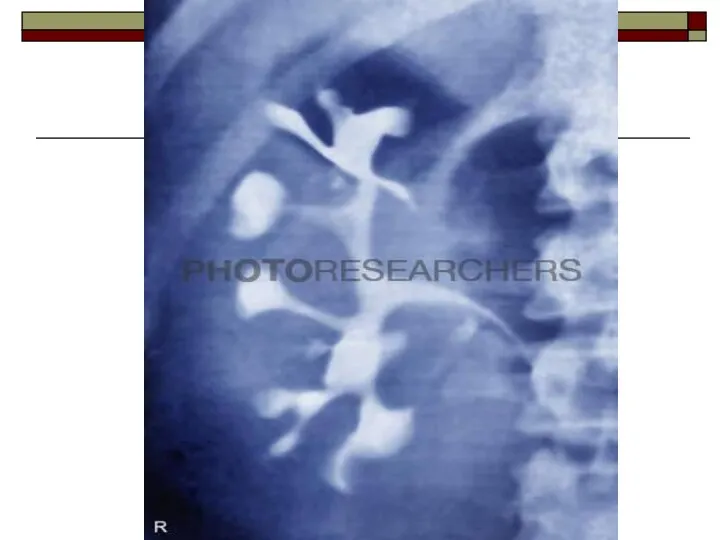
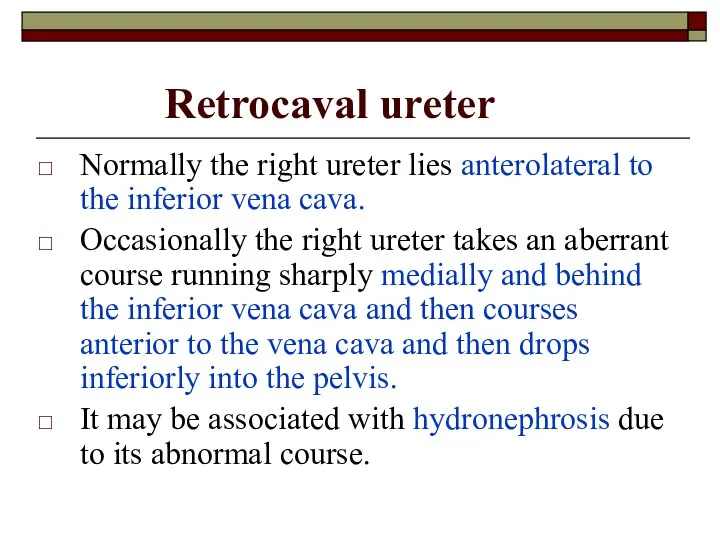
Retrocaval ureter
Normally the right ureter lies anterolateral to the inferior
Retrocaval ureter
Normally the right ureter lies anterolateral to the inferior

Urinary tract stones
Urinary tract stones are the stones within the
Urinary tract stones
Urinary tract stones are the stones within the
Radio lucent stones:
uric acid stones
xanthine stones
Radiolucent stones are not visualized on
Radio lucent stones:
uric acid stones
xanthine stones
Radiolucent stones are not visualized on
Ultrasound
Stones will be seen as hyperechoic (bright) focus within the collecting
Ultrasound
Stones will be seen as hyperechoic (bright) focus within the collecting



Hydronephrosis
Hydronephrosis is a dilatation of PCS secondary to distal obstruction.
Causes
ureteric
Hydronephrosis
Hydronephrosis is a dilatation of PCS secondary to distal obstruction.
Causes
ureteric
IVU
Findings may vary with the duration and degree of the obstruction.
IVU
Findings may vary with the duration and degree of the obstruction.
Ultrasound
dilatation of the collecting system will be seen as hypoechogenicity (dark)
Ultrasound
dilatation of the collecting system will be seen as hypoechogenicity (dark)


Hydroureter
Hydroureter is ureteric dilatation due to either obstructive or non
Hydroureter
Hydroureter is ureteric dilatation due to either obstructive or non
Causes
Ureteric calculus
Ureteric stricture
Ureterocele
Congenital megaureter
Retroperitoneal tumor/Retroperitoneal fibrosis
Pelvic malignancies
Causes
Ureteric calculus
Ureteric stricture
Ureterocele
Congenital megaureter
Retroperitoneal tumor/Retroperitoneal fibrosis
Pelvic malignancies

Ureterocele
Submucosal dilatation of the intramural distal ureter which often protrudes
Ureterocele
Submucosal dilatation of the intramural distal ureter which often protrudes
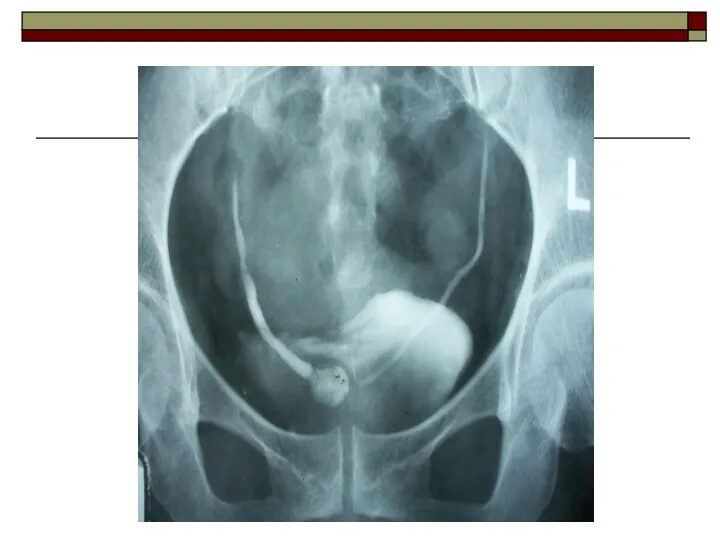
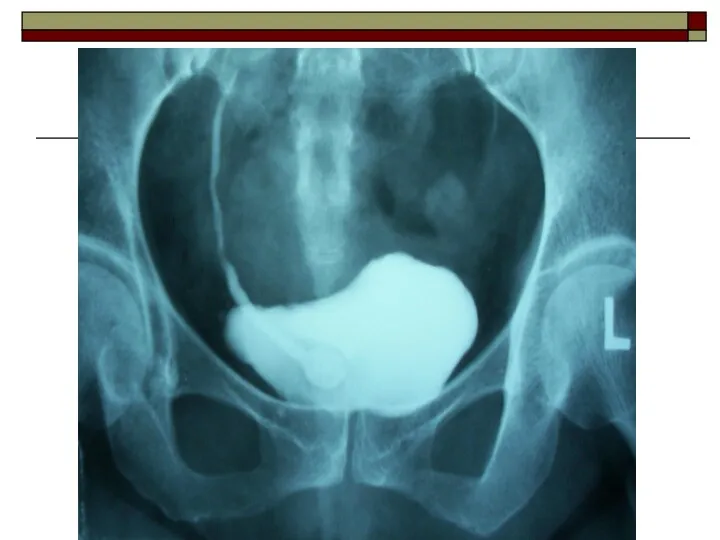
Primary megaureter
Primary megaureter is congenital abnormal musculature of the distal
Primary megaureter
Primary megaureter is congenital abnormal musculature of the distal
Renal cell carcinoma
Common age of presentation between 50 to 70
Renal cell carcinoma
Common age of presentation between 50 to 70
IVU
displacement, compression and cut off of calyces, change of axis of
IVU
displacement, compression and cut off of calyces, change of axis of
Ultrasound
heterogenous echotexture lesion within the renal parenchyma
CT scan
highly vascular mass lesion
Ultrasound
heterogenous echotexture lesion within the renal parenchyma
CT scan
highly vascular mass lesion

Wilms tumor
commonest renal malignancy in children
presents mainly between 1
Wilms tumor
commonest renal malignancy in children
presents mainly between 1
IVU
enlargement of affected part of the kidney
distortion of the PCS by
IVU
enlargement of affected part of the kidney
distortion of the PCS by


Diverticulum of bladder
It is outpouching of mucosa trough the walls
Diverticulum of bladder
It is outpouching of mucosa trough the walls
Imaging appearances
the diverticulum may have wide neck or narrow neck
in the
Imaging appearances
the diverticulum may have wide neck or narrow neck
in the

Bladder calculi
usually secondary to outflow obstruction/bladder diverticula or urinary tract
Bladder calculi
usually secondary to outflow obstruction/bladder diverticula or urinary tract
urinary bladder stones mimics phlebolith (stones in the venous wall) and
urinary bladder stones mimics phlebolith (stones in the venous wall) and



Bladder tumors
It commonly occurs in posterior and lateral walls near
Bladder tumors
It commonly occurs in posterior and lateral walls near
Epithelial tumors:
90%-transitional cell ca
1-10%-squamous cell ca
Clinical features
painless hematuria
Imaging
Epithelial tumors:
90%-transitional cell ca
1-10%-squamous cell ca
Clinical features
painless hematuria
Imaging
IVU
filling defect in the bladder
decreased capacity of bladder
may not detect small
IVU
filling defect in the bladder
decreased capacity of bladder
may not detect small

Small smooth kidney
Unilateral
ischaemia due to renal artery stenosis
post obstructive atrophy
Bilateral
arterial
Small smooth kidney
Unilateral
ischaemia due to renal artery stenosis
post obstructive atrophy
Bilateral
arterial
 Еркін қозғалыс жүйесі. Қозғалыс анализаторының анатомо-физиологиялық ерекшеліктері. Орталық және шеткі салдану белгілері
Еркін қозғалыс жүйесі. Қозғалыс анализаторының анатомо-физиологиялық ерекшеліктері. Орталық және шеткі салдану белгілері Принципы рационального питания. Лечебно-профилактическое питание, болезни связанные с характером питания
Принципы рационального питания. Лечебно-профилактическое питание, болезни связанные с характером питания Экстракорпоральные методы детоксикации
Экстракорпоральные методы детоксикации Балаларда Helicobacter pylori – инфекциясымен шақырылған асқорыту жолының жоғары бөлігін емдеу схемасы
Балаларда Helicobacter pylori – инфекциясымен шақырылған асқорыту жолының жоғары бөлігін емдеу схемасы Безсмертник
Безсмертник Онкология сегодня
Онкология сегодня Пороки развития головного мозга. Синдром Веста
Пороки развития головного мозга. Синдром Веста Дистрофии. Механизмы развития дистрофий
Дистрофии. Механизмы развития дистрофий Filling’s material: permanent & temporary
Filling’s material: permanent & temporary Гигиена зрения. Предупреждение глазных болезней
Гигиена зрения. Предупреждение глазных болезней Жүктіліктің УД зерттеу әдісі
Жүктіліктің УД зерттеу әдісі Сифилис. Лепра. Склерома. Сап. Карантинные инфекции
Сифилис. Лепра. Склерома. Сап. Карантинные инфекции Педикулез: симптомы, клиника, диагностика, лечение
Педикулез: симптомы, клиника, диагностика, лечение Описание локального статуса хирургического больного
Описание локального статуса хирургического больного Венерические заболевания
Венерические заболевания Первая медицинская помощь при неотложных состояниях
Первая медицинская помощь при неотложных состояниях Мукополисахаридоз типа I-Н (синдром Гурлер)
Мукополисахаридоз типа I-Н (синдром Гурлер) Организация акушерско-гинекологической помощи
Организация акушерско-гинекологической помощи Электромагниттердің адам өміріне зияны
Электромагниттердің адам өміріне зияны Транквилизаторы. Болеутоляющие средства. Седативные средства
Транквилизаторы. Болеутоляющие средства. Седативные средства Медикаментозная терапия при лихорадке
Медикаментозная терапия при лихорадке Понятия о ВИЧ-инфекции и СПИДе
Понятия о ВИЧ-инфекции и СПИДе Общественное здоровье и здравоохранение. Введение. (Лекция 1)
Общественное здоровье и здравоохранение. Введение. (Лекция 1) Семейства Гречишные (Polygonaceae), Буковые (Fagaceae), Берёзовые (Betulaceae)
Семейства Гречишные (Polygonaceae), Буковые (Fagaceae), Берёзовые (Betulaceae) Кардиопротективные свойства магния в комплексной терапии ишемической болезни сердца
Кардиопротективные свойства магния в комплексной терапии ишемической болезни сердца Государственное учреждение здравоохранения Севастополя Городская больница №5 – Центр охраны здоровья матери и ребенка
Государственное учреждение здравоохранения Севастополя Городская больница №5 – Центр охраны здоровья матери и ребенка Нарушение осанки и плоскостопие
Нарушение осанки и плоскостопие Дистоция плечиков
Дистоция плечиков