- Laryngeal edema and stenosis

Содержание
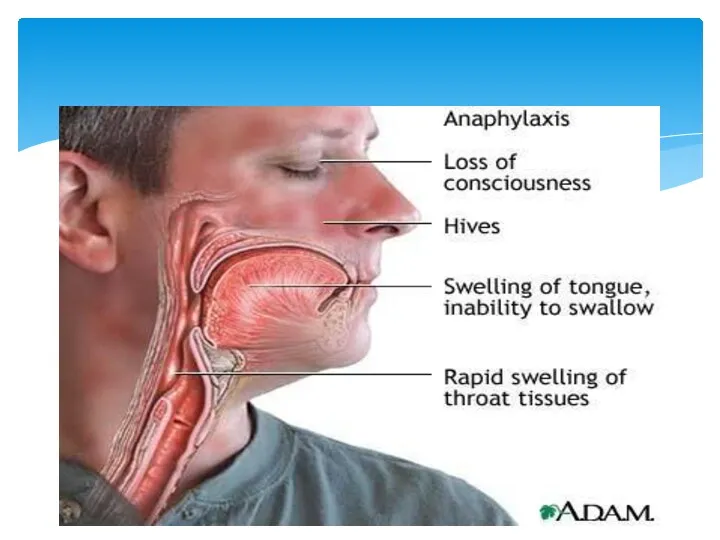
- 2. Laryngeal edema Laryngeal edema is a common cause of airway obstruction in the recently extubated intensive
- 4. Infections: epiglottitis, laryngo trachea bronchitis, tuberculosis or syphylisnof larynx Infections in neighbourhood peritonsillar abscess, retropharyngeal abscess,
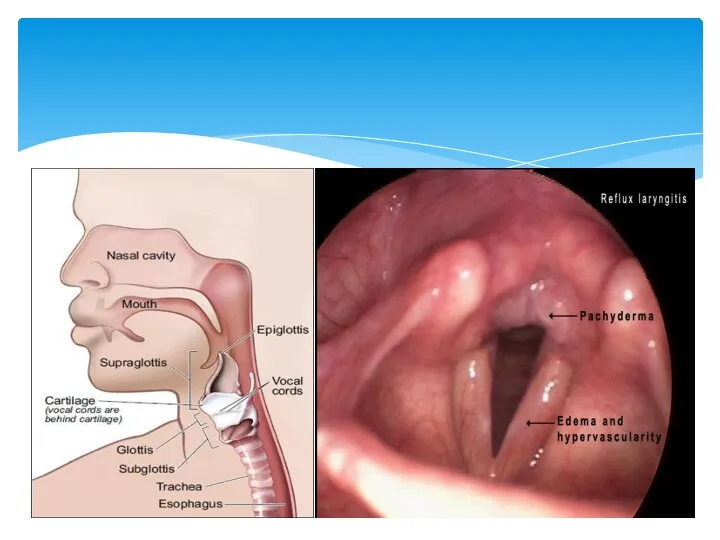
- 5. Airway obstruction Inspiratory stridor Diagnostics Indirect laryngoscopy shows oedema of supraglottic or subglottic region. Children may
- 7. Intubation/ tracheostomy Steroids (thermal, chemical) Adrenaline (1:1000) i/m 0,3-0,5ml repeated every 15 minutes Steroids are useful
- 8. Level 1: Steroid therapy decreases post-extubation stridor and need for reintubation in patients at increased risk
- 9. Laryngeal stenosis is a congenital or acquired narrowing of the airway that may affect the supraglottis,
- 10. ETIOLOGY 1.Trauma: External blunt penetrating Internal intubation post tracheostomy post surgery post radiotherapy thermal/ chemical burns
- 11. ETIOLOGY 2. Chronic inflammatory disease tuberculosis/ leprosy sacoidosis scleroma histoplasmosis diphtheria syphilis 3. Benign disorders intrinsic
- 12. ETIOLOGY 4. Malignant disorders Intrinsic SCC/ minor salivary gland tumor sarcoma/ lymphomas Extrinsic Thyroid malignancy 5.
- 13. PATHOPHYSIOLOGY Knowledge of pathophysiologyy is essential that it gives idea regarding time/ frequency of intervention, surgical
- 14. PATHOPHYSIOLOGY External trauma disruption of cartilagenous framework hematoma/ mucosal disruption hematoma: cartilage loss heals by fibrosis
- 15. CLASSIFICATION COTTONS system of grading
- 16. CLASSIFICATION Post glottic stenosis (bogdasarin & olson) TYPE 1 vocal process adhesion TYPE 2 post commissure
- 17. CLASSIFICATION Mc Caffery ( clinical status ) GRADE 1-subglottic / tracheal stenosis long. GRADE 2- subglottic
- 20. Stridor is a common presenting sign in laryngeal obstruction. Supraglottic or glottic obstruction generally presents as
- 21. The main symptoms of laryngeal stenosis relate to airway, voice, and feeding. Progressive respiratory difficulty is
- 22. ASSESSMENT OF LTS History : trauma, mode of onset, effect on airway, voice etc… Indirect/ Direct
- 23. Radiologic evaluation Radiologic evaluation is performed after stabilization of the airway. Radiography helps assess the exact
- 24. New Technology Trans-nasal “Esophagoscope” Expanded diagnostic endoscopy Laryngoscopy Bronchoscopy Esophagoscopy 2.0 mm Working Channel Biopsies Injections
- 25. SURGICAL MANAGEMENT SUPRA GLOTTIC STENOSIS ; injury can be epiglottis adherent to post / lateral hypopharyngeal
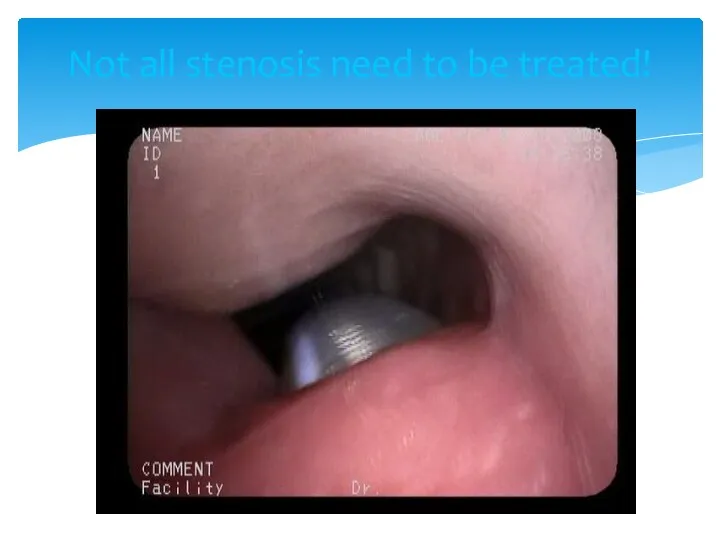
- 27. Not all stenosis need to be treated!
- 28. Treatment of Laryngotracheal Stenosis Endoscopic Laser Dilation ± Steroid injection, Mitomycin-C application Open Surgical Primary resection
- 29. Supra glottic stenosis treatment trans hyoid pharyngotomy; horizontal skin incision( hyoid bone ) if hyoid #
- 30. Supra glottic stenosis treatment In case of extensive mucosal defect – skin graft. Full thickness loss
- 31. Glottic stenosis Ant glottic stenosis; external trauma/ post intubation. thyroid cartilage #/ mucosal disruption two opposing
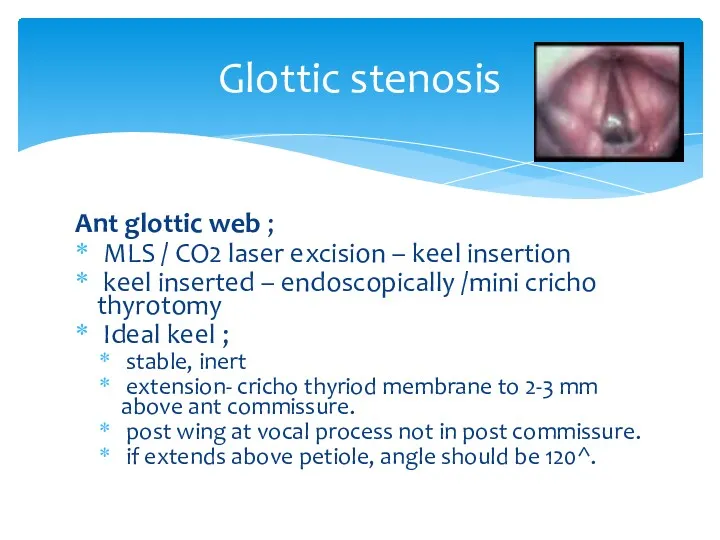
- 32. Glottic stenosis Ant glottic web ; MLS / CO2 laser excision – keel insertion keel inserted
- 33. Glottic stenosis Ant glottic stenosis; external laryngo fissure indications; sub glottic extension >5 mm inlet stenosis.
- 34. Glottic stenosis Post glottic stenosis; cause – post intubation (most common) _ cricho arytenoid joint arthritis.
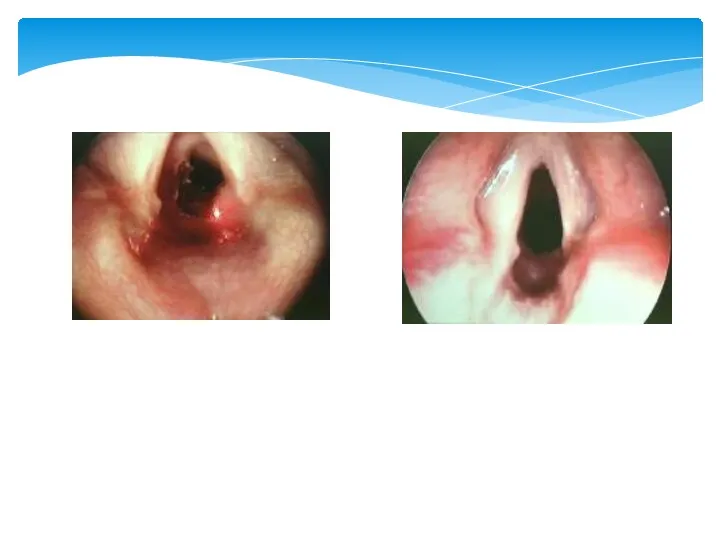
- 36. Glottic stenosis complete glottic stenosis; laryngofissure ( main stay of treatment ) Stenosis divided at midline.
- 37. Glottic stenosis Alternative approach; Epiglottic flap indication severe glottic stenosis with 50% reduction in A-P diameter
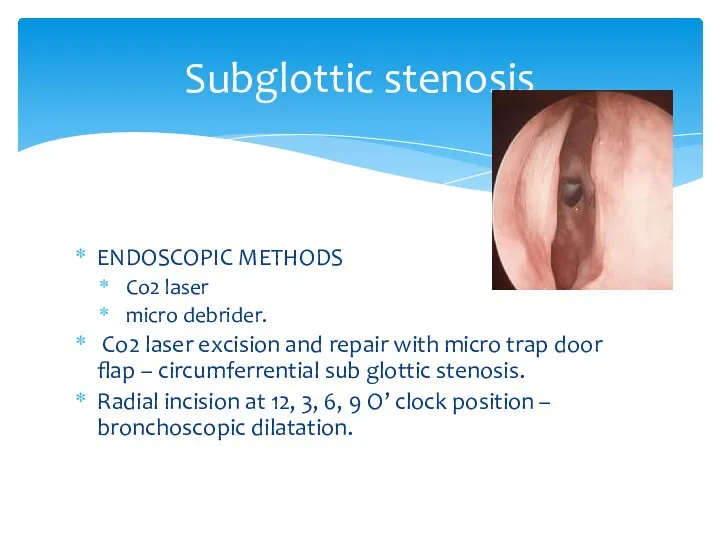
- 38. Subglottic stenosis ENDOSCOPIC METHODS Co2 laser micro debrider. Co2 laser excision and repair with micro trap
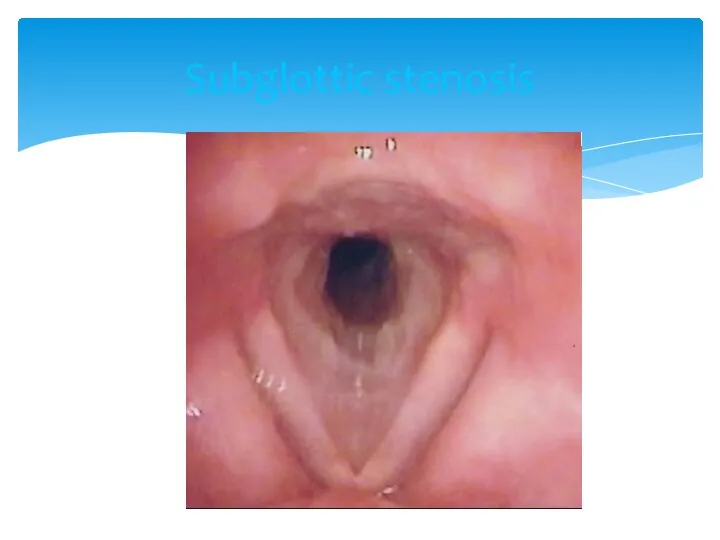
- 39. Subglottic stenosis
- 40. Subglottic stenosis EXTERNAL APPROACH; scar resection and SSG grafting. hyoid sterno hyoid muscle interposition graft .
- 42. LTS IN PEDIATRIC AGE GROUP ANATOMY; situated at a higher level funnel shape; midcricoid area 2-3
- 43. LTS IN PEDIATRIC AGE GROUP ETIOLOGY; congenital cong sub glottic stenosis vocal cord paralysis sub glottic
- 44. LTS IN PEDIATRIC AGE GROUP MANAGEMENT; endoscopic open techniques ant cricoid split laryngo tracheoplasty laryngo tracheal
- 45. LTS IN PEDIATRIC AGE GROUP POST OP MANAGEMENT; antibiotic cover anti reflux medication 6 wk endoscopy-
- 46. RESTENOSIS PREVENTION; steroids,mitomycin-c anti reflux/ antibiotics tissue engineering techniques fetal fibroblasts transposition( IL6,8) tissue engineered scaffolds
- 48. Скачать презентацию
Laryngeal edema
Laryngeal edema is a common cause of airway obstruction in
Laryngeal edema
Laryngeal edema is a common cause of airway obstruction in
Infections:
epiglottitis, laryngo trachea bronchitis, tuberculosis or syphylisnof larynx
Infections
Infections:
epiglottitis, laryngo trachea bronchitis, tuberculosis or syphylisnof larynx
Infections
Airway obstruction
Inspiratory stridor
Diagnostics
Indirect laryngoscopy shows oedema of supraglottic
or subglottic region.
Airway obstruction
Inspiratory stridor
Diagnostics
Indirect laryngoscopy shows oedema of supraglottic
or subglottic region.
Intubation/ tracheostomy
Steroids (thermal, chemical)
Adrenaline (1:1000) i/m 0,3-0,5ml repeated every 15 minutes
Steroids
Intubation/ tracheostomy
Steroids (thermal, chemical)
Adrenaline (1:1000) i/m 0,3-0,5ml repeated every 15 minutes
Steroids
Level 1: Steroid therapy decreases post-extubation stridor and need for reintubation
Level 1: Steroid therapy decreases post-extubation stridor and need for reintubation
Laryngeal stenosis is a congenital or acquired narrowing of the airway
Laryngeal stenosis is a congenital or acquired narrowing of the airway
ETIOLOGY
1.Trauma:
External
blunt
penetrating
Internal
intubation
post tracheostomy
post surgery
post
ETIOLOGY
1.Trauma:
External
blunt
penetrating
Internal
intubation
post tracheostomy
post surgery
post
ETIOLOGY
2. Chronic inflammatory disease
tuberculosis/ leprosy
sacoidosis
scleroma
histoplasmosis
diphtheria
syphilis
3.
ETIOLOGY
2. Chronic inflammatory disease
tuberculosis/ leprosy
sacoidosis
scleroma
histoplasmosis
diphtheria
syphilis
3.
ETIOLOGY
4. Malignant disorders
Intrinsic
SCC/ minor salivary gland tumor
sarcoma/ lymphomas
ETIOLOGY
4. Malignant disorders
Intrinsic
SCC/ minor salivary gland tumor
sarcoma/ lymphomas
PATHOPHYSIOLOGY
Knowledge of pathophysiologyy is essential that it gives idea regarding
PATHOPHYSIOLOGY
Knowledge of pathophysiologyy is essential that it gives idea regarding
PATHOPHYSIOLOGY
External trauma
disruption of cartilagenous framework
hematoma/ mucosal disruption
hematoma:
PATHOPHYSIOLOGY
External trauma
disruption of cartilagenous framework
hematoma/ mucosal disruption
hematoma:
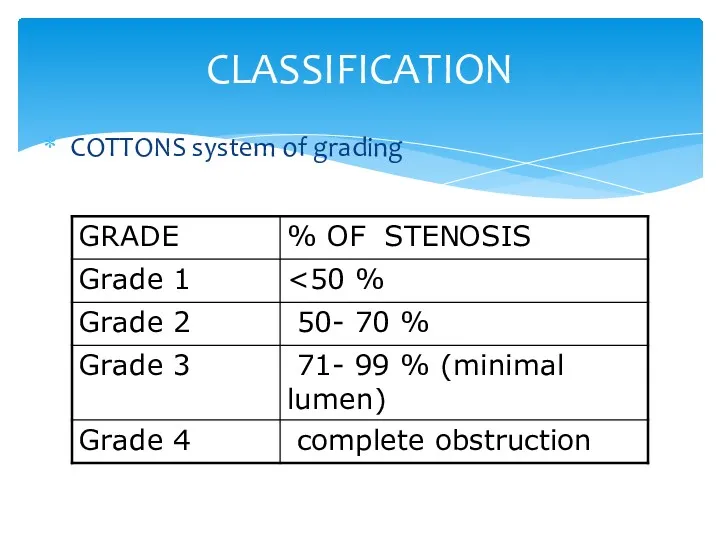
CLASSIFICATION
COTTONS system of grading
CLASSIFICATION
COTTONS system of grading
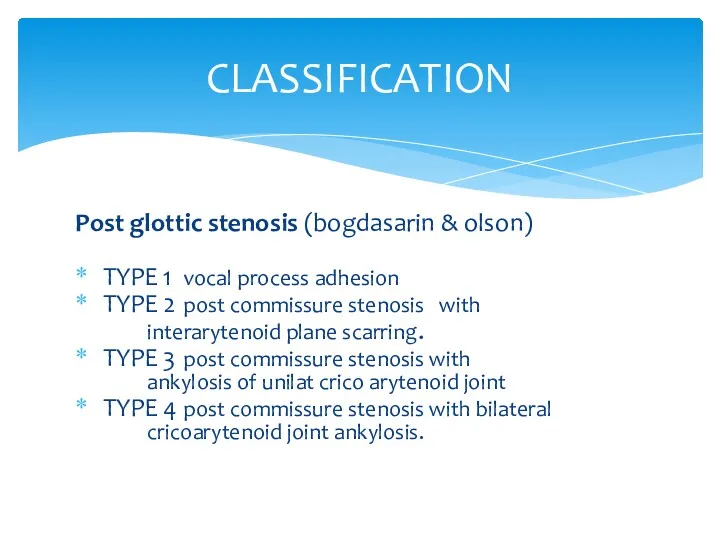
CLASSIFICATION
Post glottic stenosis (bogdasarin & olson)
TYPE 1 vocal process adhesion
TYPE
CLASSIFICATION
Post glottic stenosis (bogdasarin & olson)
TYPE 1 vocal process adhesion
TYPE
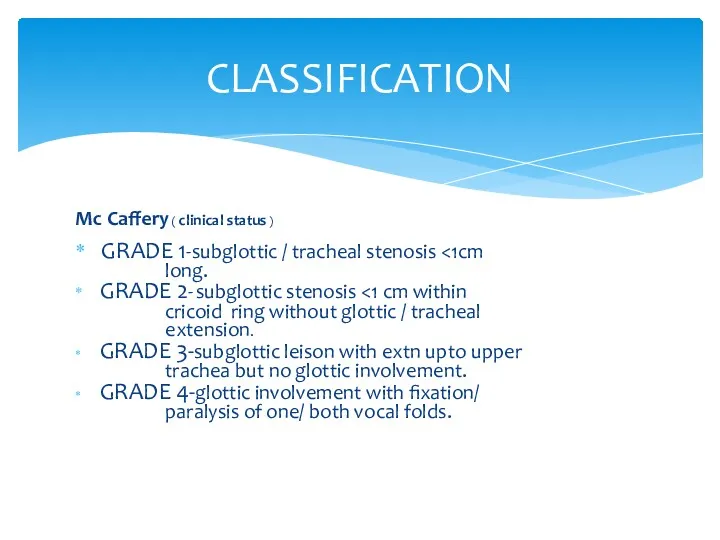
CLASSIFICATION
Mc Caffery ( clinical status )
GRADE 1-subglottic / tracheal stenosis <1cm
CLASSIFICATION
Mc Caffery ( clinical status )
GRADE 1-subglottic / tracheal stenosis <1cm

Stridor is a common presenting sign in laryngeal obstruction. Supraglottic or
Stridor is a common presenting sign in laryngeal obstruction. Supraglottic or
The main symptoms of laryngeal stenosis relate to airway, voice, and
The main symptoms of laryngeal stenosis relate to airway, voice, and
ASSESSMENT OF LTS
History : trauma, mode of onset, effect on
ASSESSMENT OF LTS
History : trauma, mode of onset, effect on
Radiologic evaluation Radiologic evaluation is performed after stabilization of the airway.
Radiologic evaluation Radiologic evaluation is performed after stabilization of the airway.
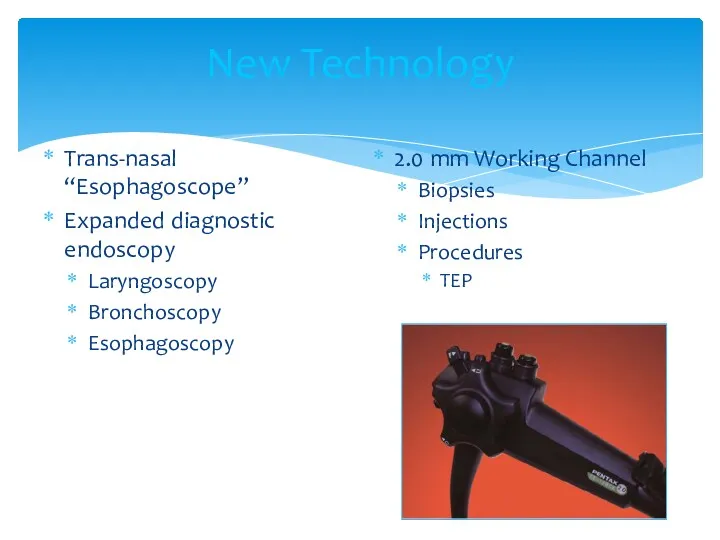
New Technology
Trans-nasal “Esophagoscope”
Expanded diagnostic endoscopy
Laryngoscopy
Bronchoscopy
Esophagoscopy
2.0 mm Working Channel
Biopsies
Injections
Procedures
TEP
New Technology
Trans-nasal “Esophagoscope”
Expanded diagnostic endoscopy
Laryngoscopy
Bronchoscopy
Esophagoscopy
2.0 mm Working Channel
Biopsies
Injections
Procedures
TEP
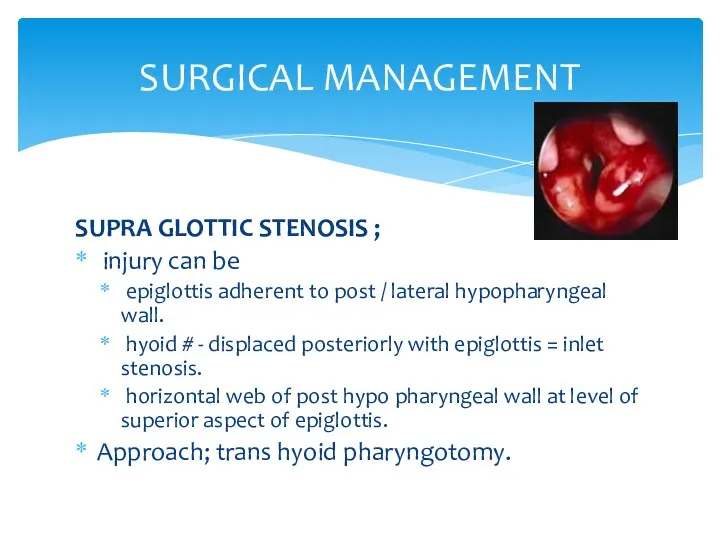
SURGICAL MANAGEMENT
SUPRA GLOTTIC STENOSIS ;
injury can be
epiglottis adherent
SURGICAL MANAGEMENT
SUPRA GLOTTIC STENOSIS ;
injury can be
epiglottis adherent
Not all stenosis need to be treated!
Not all stenosis need to be treated!
Treatment of Laryngotracheal Stenosis
Endoscopic
Laser
Dilation
± Steroid injection, Mitomycin-C application
Open Surgical
Primary resection and
Treatment of Laryngotracheal Stenosis
Endoscopic
Laser
Dilation
± Steroid injection, Mitomycin-C application
Open Surgical
Primary resection and
Supra glottic stenosis treatment
trans hyoid pharyngotomy;
horizontal skin incision( hyoid
Supra glottic stenosis treatment
trans hyoid pharyngotomy;
horizontal skin incision( hyoid
Supra glottic stenosis treatment
In case of extensive mucosal defect –
Supra glottic stenosis treatment
In case of extensive mucosal defect –
Glottic stenosis
Ant glottic stenosis;
external trauma/ post intubation.
thyroid cartilage #/
Glottic stenosis
Ant glottic stenosis;
external trauma/ post intubation.
thyroid cartilage #/
Glottic stenosis
Ant glottic web ;
MLS / CO2 laser excision
Glottic stenosis
Ant glottic web ;
MLS / CO2 laser excision
Glottic stenosis
Ant glottic stenosis;
external laryngo fissure
indications;
sub
Glottic stenosis
Ant glottic stenosis;
external laryngo fissure
indications;
sub
Glottic stenosis
Post glottic stenosis;
cause – post intubation (most common)
Glottic stenosis
Post glottic stenosis;
cause – post intubation (most common)
Glottic stenosis
complete glottic stenosis;
laryngofissure ( main stay of treatment
Glottic stenosis
complete glottic stenosis;
laryngofissure ( main stay of treatment
Glottic stenosis
Alternative approach;
Epiglottic flap
indication
severe glottic stenosis with 50%
Glottic stenosis
Alternative approach;
Epiglottic flap
indication
severe glottic stenosis with 50%
Subglottic stenosis
ENDOSCOPIC METHODS
Co2 laser
micro debrider.
Co2 laser excision and
Subglottic stenosis
ENDOSCOPIC METHODS
Co2 laser
micro debrider.
Co2 laser excision and
Subglottic stenosis
Subglottic stenosis
Subglottic stenosis
EXTERNAL APPROACH;
scar resection and SSG grafting.
hyoid sterno hyoid
Subglottic stenosis
EXTERNAL APPROACH;
scar resection and SSG grafting.
hyoid sterno hyoid

LTS IN PEDIATRIC AGE GROUP
ANATOMY;
situated at a higher level
LTS IN PEDIATRIC AGE GROUP
ANATOMY;
situated at a higher level
LTS IN PEDIATRIC AGE GROUP
ETIOLOGY;
congenital
cong sub glottic stenosis
LTS IN PEDIATRIC AGE GROUP
ETIOLOGY;
congenital
cong sub glottic stenosis
LTS IN PEDIATRIC AGE GROUP
MANAGEMENT;
endoscopic
open techniques
ant cricoid
LTS IN PEDIATRIC AGE GROUP
MANAGEMENT;
endoscopic
open techniques
ant cricoid
LTS IN PEDIATRIC AGE GROUP
POST OP MANAGEMENT;
antibiotic cover
anti
LTS IN PEDIATRIC AGE GROUP
POST OP MANAGEMENT;
antibiotic cover
anti
RESTENOSIS
PREVENTION;
steroids,mitomycin-c
anti reflux/ antibiotics
tissue engineering techniques
fetal fibroblasts transposition(
RESTENOSIS
PREVENTION;
steroids,mitomycin-c
anti reflux/ antibiotics
tissue engineering techniques
fetal fibroblasts transposition(
 Периоды жизнедеятельности человека. Роль сестринского персонала в сохранении и укреплении здоровья
Периоды жизнедеятельности человека. Роль сестринского персонала в сохранении и укреплении здоровья Влияние ВИЧ на репродуктивную функцию подростка
Влияние ВИЧ на репродуктивную функцию подростка Заболевания передающиеся половым путем
Заболевания передающиеся половым путем Федеральный проект Демография
Федеральный проект Демография Хронический пульпит
Хронический пульпит Синдромы Дауна и Патау
Синдромы Дауна и Патау Деформирующий артроз коленного сустава. Лечение
Деформирующий артроз коленного сустава. Лечение Основы иммунологии. Иммунитет. Иммунная система человека
Основы иммунологии. Иммунитет. Иммунная система человека Дыхательная недостаточность
Дыхательная недостаточность Инфекция или инфекционный процесс
Инфекция или инфекционный процесс Пародонт аурулары. Анықтамасы, жіктелуі, этиологиясы, потогенезі. Пародонт ауруларымен науқастары комплексті тексеру
Пародонт аурулары. Анықтамасы, жіктелуі, этиологиясы, потогенезі. Пародонт ауруларымен науқастары комплексті тексеру Скелет верхней и нижней конечности
Скелет верхней и нижней конечности Организация медико-генетической службы
Организация медико-генетической службы Дом для мамы: я выбираю жизнь
Дом для мамы: я выбираю жизнь Нервно-психическое развитие ребёнка раннего возраста
Нервно-психическое развитие ребёнка раннего возраста Хронический панкреатит и внешнесекреторная недостаточность поджелудочной железы у детей
Хронический панкреатит и внешнесекреторная недостаточность поджелудочной железы у детей Фармацевтическая терминология. Основные понятия фармацевтической терминологии
Фармацевтическая терминология. Основные понятия фармацевтической терминологии Острая почечная и острая печеночная недостаточность
Острая почечная и острая печеночная недостаточность Хроническая обструктивная болезнь легких
Хроническая обструктивная болезнь легких Организация оказания медицинской помощи в амбулаторно - поликлинических учреждениях
Организация оказания медицинской помощи в амбулаторно - поликлинических учреждениях Атипичные нейролептики нового поколения (антипсихотики)
Атипичные нейролептики нового поколения (антипсихотики) Роль медицинской сестры в профилактике и лечении пролежней
Роль медицинской сестры в профилактике и лечении пролежней Прием пациента в стационар. Ведение сестринской документации
Прием пациента в стационар. Ведение сестринской документации Ес және назар аудару бұзылыстарының клиникалық мінездемесі.Сана- сезімнің бұзылыстары
Ес және назар аудару бұзылыстарының клиникалық мінездемесі.Сана- сезімнің бұзылыстары Медико-соціальна експертиза при захворюваннях органів системи кровообігу
Медико-соціальна експертиза при захворюваннях органів системи кровообігу Шина Вебера. Шина Порта
Шина Вебера. Шина Порта Профилактики стоматологических заболеваний у беременных женщин. Содержание стоматологического просвещения для беременных женщин
Профилактики стоматологических заболеваний у беременных женщин. Содержание стоматологического просвещения для беременных женщин Дамудың туа біткен ақауларының түрлері
Дамудың туа біткен ақауларының түрлері