- Liver, Biliary, and Exocrine Pancreas Diseases

Содержание
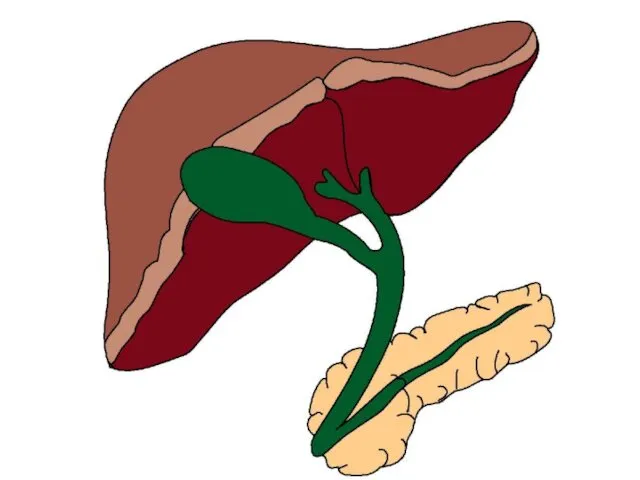
- 2. Liver “The liver ranks first in size, number and complexity of functions. It is involved in
- 4. Cystic duct Common bile duct
- 5. Functions A. Metabolism of CHO, Prot, Fat, and EtOH 1. CHO: glycogenesis, glycogenolysis, gluconeogenesis, synthesis of
- 6. B. Detoxification of drugs and other toxic substances C. Vitamin and Mineral-related functions 1. Vitamin A:
- 7. D. Blood Reservoir: Acts as a flood chamber between intestinal and general circulation. Can expand/contract. 1.
- 8. “True tests of liver function” Indicators of liver injury Biochemical Markers of Liver Disease
- 9. Disorders of the Liver A. Fatty liver– (hepatic steatosis) Accumulation of fat in hepatocytes Early stage
- 10. 1. Alcohol – induced fatty liver: a. Liver cells preferentially use FAs for energy b. Also
- 11. B. Hepatitis – Inflammation of hepatocytes 2° virus, obstruction, parasite, drug or other toxin (including EtOH),
- 12. 3. Nutrition Therapy a. Abstinence from alcohol b. Good nutrition status: c. Malnourished: d. Persistent anorexia/nausea:
- 13. C. Cirrhosis – advanced stage of liver disease scar tissue replaces hepatocytes
- 14. Consequences of Cirrhosis: 1. Portal Hypertension: elevated BP in the portal vein 2°obstructed blood flow through
- 15. 3. Ascites – edema characterized by the accumulation of fluid, electrolytes and serum proteins in the
- 16. 4. Hepatic Encephalopathy/Hepatic Coma a. Hyperammonemia – Healthy liver converts ammonia ? urea Other nitrogenous compounds
- 17. b. Psychomotor abnormalities: c. Fetor hepaticus – sign of impending coma d. Chronic disturbance in consciousness
- 18. Nutrition Therapy in Liver Disease Energy ESLD without ascites: Ascites, infection, malabsorption or malnutrition: CHO
- 19. Lipids Protein Hepatitis/cirrhosis: Repletion: Stress/decompensation/sepsis: Encephalopathy: restriction is controversial
- 20. Vitamins and Minerals Steatorrhea: fat-sol vitamins (water-miscible form) B vitamins: EtOH liver ds. (Wernicke’s Encephalopathy) Ca++,
- 21. Monitor Wt, abdominal girth, BUN/creat, Na+, albumin, and lytes.
- 23. Diseases of the Gallbladder Cholelithiasis (gallstones) US: Choledocholithiasis Cholecystitis
- 24. Acute cholecystitis: Chronic cholecystitis Cholecystectomy ADAT to regular diet Liver drains directly into duodenum Over time:
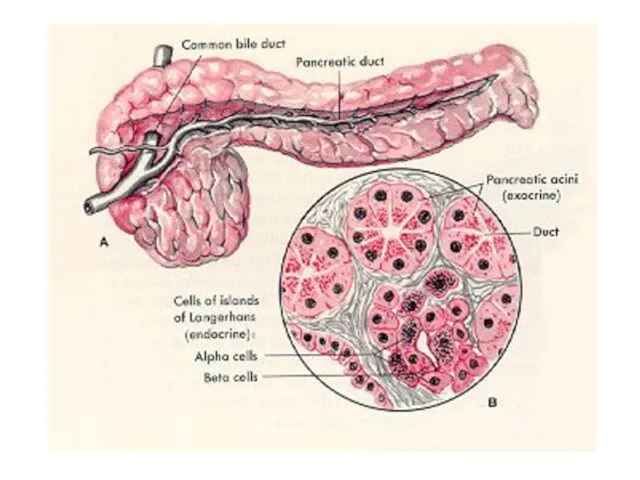
- 26. Ds. of the Exocrine Pancreas Pancreatitis Exocrine pancreatic secretions: digestive enzymes bicarbonate-rich “juices.” Disorders of the
- 27. Acute Pancreatitis Causes: Also hypertriglyceridemia, hypercalcemia, infections. Pancreatic digestive enzymes are activated within the pancreas ?
- 28. Hallmark symptoms: Severe cases: Complications:
- 29. MNT for Acute Pancreatitis NPO w/IV hydration Poss. N/G suction Mild-to-Moderate cases:
- 30. Severe cases: enteral/TPN: __________ TF to ↓ pancreatic stimulation TPN if: edema intestinal fistula Drugs: somatostatin
- 31. Chronic Pancreatitis Most commonly 2° Persistent or recurrent episodes ? Serum amylase & lipase: Pancreatic calcification
- 33. Скачать презентацию
Liver
“The liver ranks first in size, number and complexity
Liver
“The liver ranks first in size, number and complexity
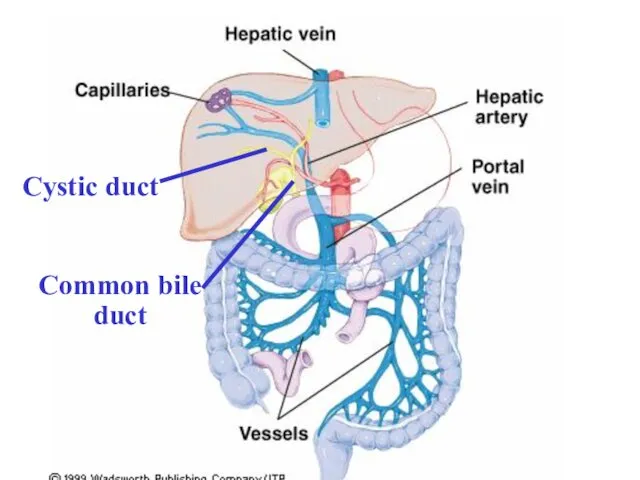
Cystic duct
Common bile duct
Cystic duct
Common bile duct
Functions
A. Metabolism of CHO, Prot, Fat, and EtOH
1. CHO: glycogenesis, glycogenolysis,
Functions
A. Metabolism of CHO, Prot, Fat, and EtOH
1. CHO: glycogenesis, glycogenolysis,
B. Detoxification of drugs and other toxic substances
C. Vitamin and Mineral-related
B. Detoxification of drugs and other toxic substances
C. Vitamin and Mineral-related
D. Blood Reservoir: Acts as a flood chamber between intestinal and
D. Blood Reservoir: Acts as a flood chamber between intestinal and
“True tests of liver function”
Indicators of liver injury
Biochemical Markers of Liver
“True tests of liver function”
Indicators of liver injury
Biochemical Markers of Liver
Disorders of the Liver
A. Fatty liver– (hepatic steatosis)
Accumulation of fat
Disorders of the Liver
A. Fatty liver– (hepatic steatosis)
Accumulation of fat
1. Alcohol – induced fatty liver:
a. Liver cells preferentially use FAs
1. Alcohol – induced fatty liver:
a. Liver cells preferentially use FAs
B. Hepatitis – Inflammation of hepatocytes 2° virus, obstruction, parasite, drug
B. Hepatitis – Inflammation of hepatocytes 2° virus, obstruction, parasite, drug
3. Nutrition Therapy
a. Abstinence from alcohol
b. Good nutrition status:
c. Malnourished:
3. Nutrition Therapy
a. Abstinence from alcohol
b. Good nutrition status:
c. Malnourished:
C. Cirrhosis – advanced stage of liver disease
scar tissue replaces hepatocytes
C. Cirrhosis – advanced stage of liver disease
scar tissue replaces hepatocytes
Consequences of Cirrhosis:
1. Portal Hypertension: elevated BP in the portal
Consequences of Cirrhosis:
1. Portal Hypertension: elevated BP in the portal
3. Ascites – edema characterized by the accumulation of fluid, electrolytes
3. Ascites – edema characterized by the accumulation of fluid, electrolytes
4. Hepatic Encephalopathy/Hepatic Coma
a. Hyperammonemia –
Healthy liver converts
4. Hepatic Encephalopathy/Hepatic Coma
a. Hyperammonemia –
Healthy liver converts
b. Psychomotor abnormalities:
c. Fetor hepaticus
– sign of impending
c. Fetor hepaticus
– sign of impending
Nutrition Therapy in Liver Disease
Energy
ESLD without ascites:
Ascites, infection, malabsorption or
Nutrition Therapy in Liver Disease
Energy
ESLD without ascites:
Ascites, infection, malabsorption or
Lipids
Protein
Hepatitis/cirrhosis:
Repletion:
Stress/decompensation/sepsis:
Encephalopathy: restriction is controversial
Lipids
Protein
Hepatitis/cirrhosis:
Repletion:
Stress/decompensation/sepsis:
Encephalopathy: restriction is controversial
Vitamins and Minerals
Steatorrhea: fat-sol vitamins (water-miscible form)
B vitamins: EtOH liver ds.
Vitamins and Minerals
Steatorrhea: fat-sol vitamins (water-miscible form)
B vitamins: EtOH liver ds.
Monitor
Wt, abdominal girth, BUN/creat, Na+, albumin, and lytes.
Monitor
Wt, abdominal girth, BUN/creat, Na+, albumin, and lytes.
Diseases of the Gallbladder
Cholelithiasis (gallstones)
US:
Choledocholithiasis
Cholecystitis
Diseases of the Gallbladder
Cholelithiasis (gallstones)
US:
Choledocholithiasis
Cholecystitis
Acute cholecystitis:
Chronic cholecystitis
Cholecystectomy
ADAT to regular diet
Liver drains directly into duodenum
Over time:
Acute cholecystitis:
Chronic cholecystitis
Cholecystectomy
ADAT to regular diet
Liver drains directly into duodenum
Over time:
Ds. of the Exocrine Pancreas
Pancreatitis
Exocrine pancreatic secretions:
digestive enzymes
bicarbonate-rich “juices.”
Ds. of the Exocrine Pancreas
Pancreatitis
Exocrine pancreatic secretions:
digestive enzymes
bicarbonate-rich “juices.”
Acute Pancreatitis
Causes:
Also hypertriglyceridemia, hypercalcemia, infections.
Pancreatic digestive enzymes are activated
Acute Pancreatitis
Causes:
Also hypertriglyceridemia, hypercalcemia, infections.
Pancreatic digestive enzymes are activated
Hallmark symptoms:
Severe cases:
Complications:
Hallmark symptoms:
Severe cases:
Complications:
MNT for Acute Pancreatitis
NPO w/IV hydration
Poss. N/G suction
Mild-to-Moderate cases:
MNT for Acute Pancreatitis
NPO w/IV hydration
Poss. N/G suction
Mild-to-Moderate cases:
Severe cases: enteral/TPN:
__________ TF to ↓ pancreatic stimulation
TPN if:
edema
intestinal fistula
Drugs:
Severe cases: enteral/TPN:
__________ TF to ↓ pancreatic stimulation
TPN if:
edema
intestinal fistula
Drugs:
Chronic Pancreatitis
Most commonly 2°
Persistent or recurrent episodes ?
Serum amylase
Chronic Pancreatitis
Most commonly 2°
Persistent or recurrent episodes ?
Serum amylase
 Прикосновение ради здоровья. Программа по сохранению и улучшению здоровья
Прикосновение ради здоровья. Программа по сохранению и улучшению здоровья Сүйек кемігі
Сүйек кемігі Основные инфекционные заболевания
Основные инфекционные заболевания Геморрагический васкулит
Геморрагический васкулит Медицинская служба мотострелковой (танковой, механизированной) бригады. Тема № 19-3
Медицинская служба мотострелковой (танковой, механизированной) бригады. Тема № 19-3 Лечение гипертонических кризов
Лечение гипертонических кризов МРТ злокачественных опухолей головного мозга (часть 2)
МРТ злокачественных опухолей головного мозга (часть 2) Артикуляция и окклюзия. Биомеханика нижней челюсти
Артикуляция и окклюзия. Биомеханика нижней челюсти Опухоли нервной системы
Опухоли нервной системы План ортодонтического лечения
План ортодонтического лечения Полиомиелит, энтеровирусные инфекции
Полиомиелит, энтеровирусные инфекции Физиотерапия, кинезитерапия при травматических повреждениях
Физиотерапия, кинезитерапия при травматических повреждениях Профессионально значимые качества медсестры
Профессионально значимые качества медсестры Аменорея. Лечение
Аменорея. Лечение Способы использования лекарственных растений и приготовление лекарственных форм из растений
Способы использования лекарственных растений и приготовление лекарственных форм из растений Технология изготовления зубных протезов
Технология изготовления зубных протезов Синдром Лайелла (токсический эпидермальный некролиз)
Синдром Лайелла (токсический эпидермальный некролиз) Мануальная медицина
Мануальная медицина Кровотечение. Первая медицинская помощь при кровотечениях
Кровотечение. Первая медицинская помощь при кровотечениях Тоқ ішек
Тоқ ішек Вирусные заболевания слизистой полости рта у детей. Лечение и профилактика
Вирусные заболевания слизистой полости рта у детей. Лечение и профилактика Средства, влияющие на систему крови Лекция для студентов стоматологического факультета
Средства, влияющие на систему крови Лекция для студентов стоматологического факультета Медико-биологиялық ақпаратты алу, тіркеу және жеткізудің құрылымдық сызба кестесі
Медико-биологиялық ақпаратты алу, тіркеу және жеткізудің құрылымдық сызба кестесі Туберкулез костей и суставов
Туберкулез костей и суставов Облитерирующий атеросклероз артерий нижних конечностей
Облитерирующий атеросклероз артерий нижних конечностей Корь. Таксономия
Корь. Таксономия Метод лечения фитотерапия
Метод лечения фитотерапия Регуляция менструального цикла
Регуляция менструального цикла