- Malignant Melanoma

Содержание
- 2. RISK FACTORS Fair skinned. Hair color other than black. Excessive sun exposure . Melanoma in first-degree
- 3. Familial Atypical Mole Melanoma Syndrome Autosomal dominant Neoplastic risk "atypical melanocytic nevus“ 25-40% with CDKN2A mutation
- 4. Xeroderma Pigmentosum Rare Autosomal recessive disease DNA repair enzyme defect Photosensitivity Photodamage Cutaneous malignancies Severe ophthalmological
- 5. Ultraviolet light
- 6. UVC ( Completely absorbed by the atmosphere and is non-relevant for UV induced skin carcinogenesis. UVB
- 8. The ABCDEs of Melanoma Diagnosis Asymmetry One half of the lesion is shaped differently than the
- 9. TYPES OF MELANOMA
- 10. NODULAR Commoner in males Trunk is a common site Poor prognosis Black/brown nodule Ulceration and bleeding
- 11. SUPERFICIAL SPREADING The most common type of MM in the white-skinned population – 70% of cases
- 12. ACRAL LENTIGINOUS MELANOMA Commonest MM in nonwhite-skinned nations Usually comprises a flat lentiginous area with an
- 13. SUBUNGAL MELANOMA Rare Often diagnosed late – confusion with benign subungal naevus, paronychial infections, trauma. Hutchinson’s
- 14. LENTIGO MALIGNA MELANOMA Occurs as a late development in a lentigo maligna. Mainly on the face
- 15. AMELANOTIC MELANOMA Diagnosis is often missed clinically. The lack of pigmentation is due to the rapid
- 16. Mucosal melanoma Muc M approximately 1 % of all melanomas . Arise primarily in the head
- 17. Ocular melanoma OM is the most common type of cancer to affect the eye, although it's
- 18. Skin biopsy Excisional Bx. Location Breslow thickness Ulceration Peripheral and deep margins.
- 19. Breslow Thickness: 1-2 mm (T2) 2-4 mm (T3) > 4.0 mm (T4) thick Intermediate
- 20. Clark Level
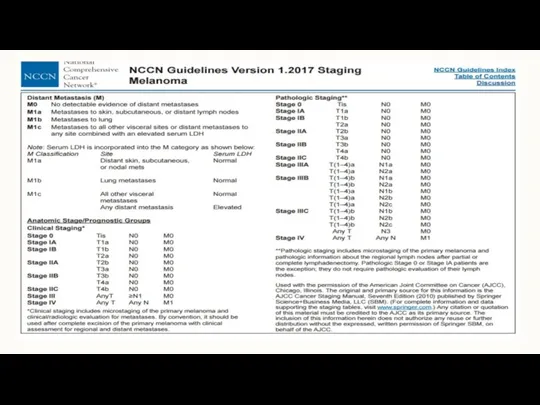
- 21. Stage 0: (TisN0M0). melanoma in situ
- 22. Stage I: Local disease - superficial
- 23. Stage II: Local disease - deep invasion.
- 24. Stage III: Regional disease
- 25. Stage IV: Metastatic disease
- 26. Prognostic factors Depth of Invasion Ulceration Lymph Node Mitotic Rate (TNM staging system 2010) LDH level
- 31. Sentinel lymph node biopsy SLN = First node(s) draining the area of primary lesion. Sentinel node
- 32. Sentinel lymph node mapping and biopsy
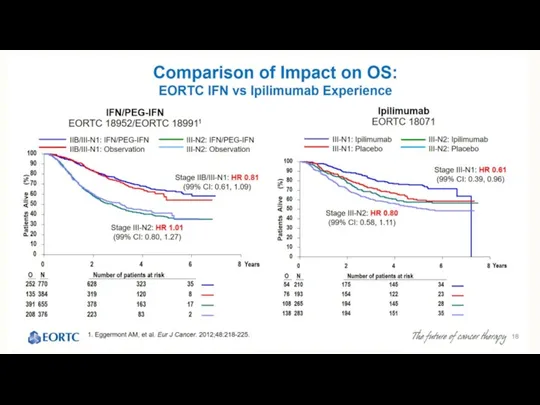
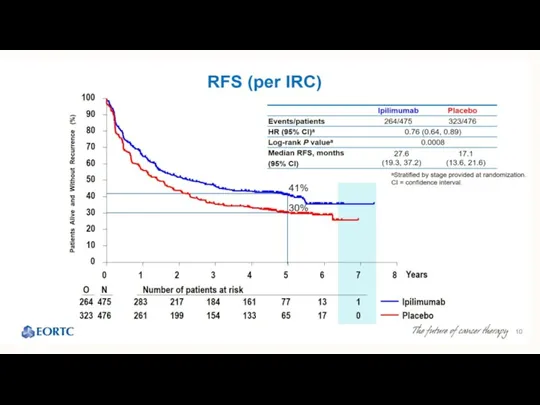
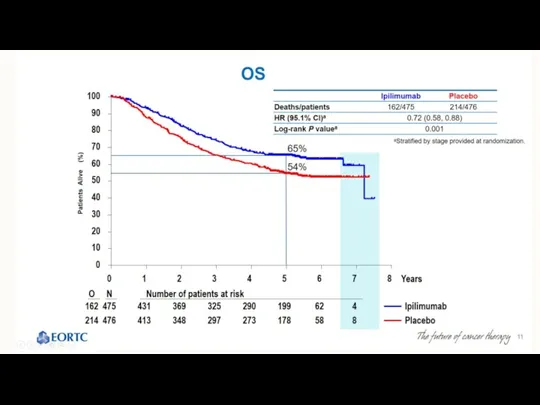
- 34. Adjuvant therapy Potential candidates Stage IIB Stage III Chemotherapy - not effective (DTIC). Immunotherapy - IFN
- 36. IPILIMUMAB Yervoy Anti CTLA4 Antibody
- 42. IFN α - Side effects Acute toxicity : (Due to PGE2 synthesis and/or other cytokines) Flue
- 43. Treatment Options for advanced Melanoma
- 44. BRAF\MEK Inhibitors Dabrafenib (TAFINLAR) Trametinib ( MEKINIST) Vemurafenib ( ZELBORAF) Cobimetinib (COTELIC)
- 50. Imunotherapy
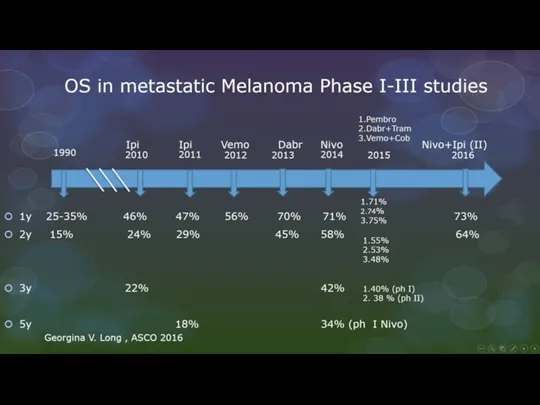
- 52. Ipillimumab (Yervoy) In pooled analysis of 12 studies, a plateau in the survival curve begins at
- 54. Anti PD1 therapy : Opdivo (Nivolumab) Keytruda (Pembrolizumab)
- 55. Opdivo Monotherapy Phase 3 Trial: Improved OS Versus Dacarbazine in BRAF Wild-type, Untreated Patients 1. Atkinson
- 56. Best Overall Response Based on 5 August 2014 database lock.
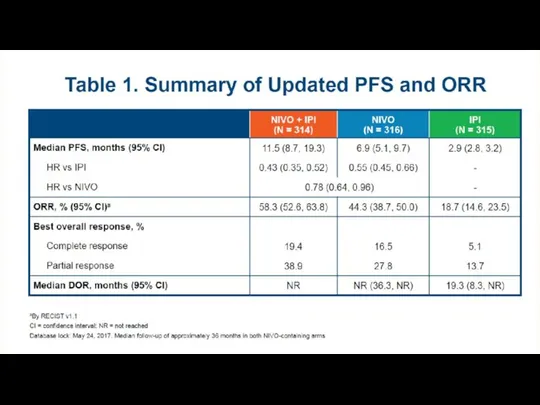
- 59. Updated Results From a Phase III Trial of Nivolumab Combined With Ipilimumab in Treatment-naïve Patients With
- 60. OS at 2 Years of Follow-up (All Randomized Patients) Checkmate 069 30/47 (64%) of patients randomized
- 61. Response To Treatment
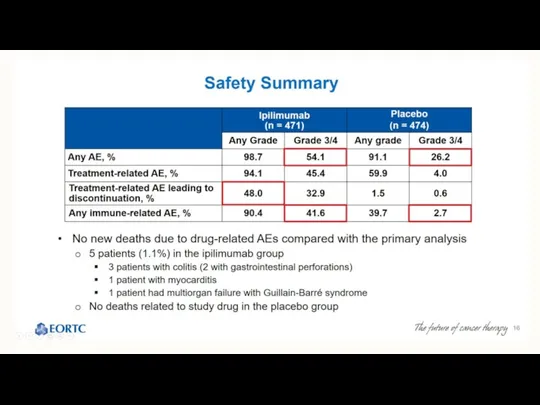
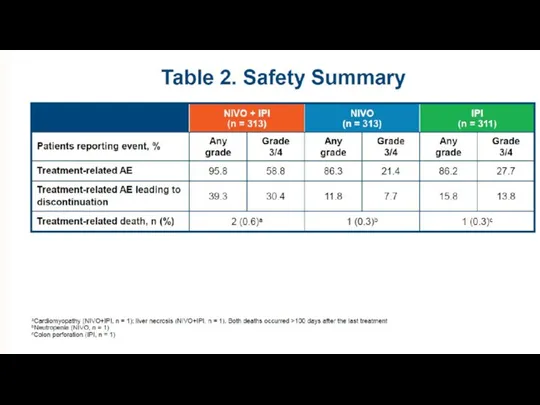
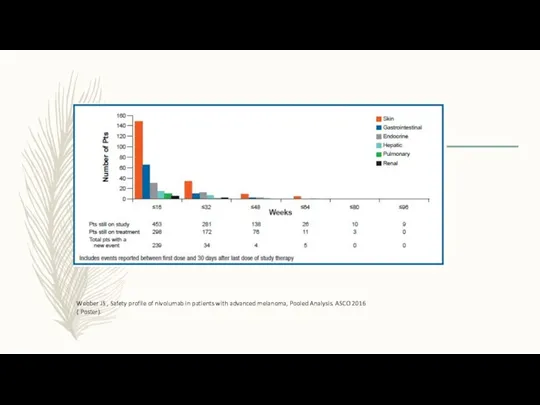
- 62. Safety Summary Updated safety information with 9 additional months of follow-up were consistent with the initial
- 65. Overall Survival at 2 Years of Follow-up 83% 71% 73% 64% 65% 54% Database lock February
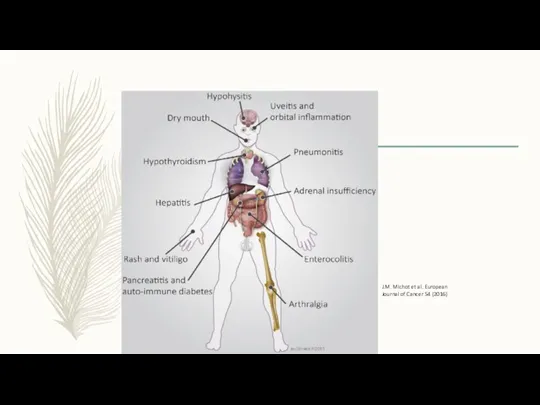
- 66. J.M. Michot et al. European Journal of Cancer 54 (2016)
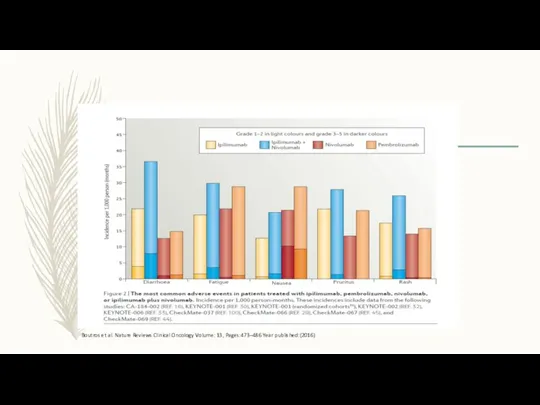
- 67. Boutros et al. Nature Reviews Clinical Oncology Volume: 13, Pages:473–486 Year published:(2016)
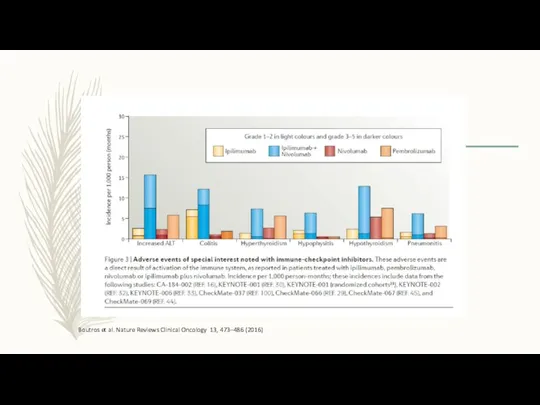
- 68. Nature Reviews Clinical Oncology Volume: 13, Pages: 473–486 Year published: (2016) DOI: doi:10.1038/nrclinonc.2016.58 Published online 04
- 69. Webber JS , Safety profile of nivolumab in patients with advanced melanoma, Pooled Analysis. ASCO 2016
- 72. Скачать презентацию
RISK FACTORS
Fair skinned.
Hair color other than black.
Excessive sun exposure .
Melanoma
RISK FACTORS
Fair skinned.
Hair color other than black.
Excessive sun exposure .
Melanoma
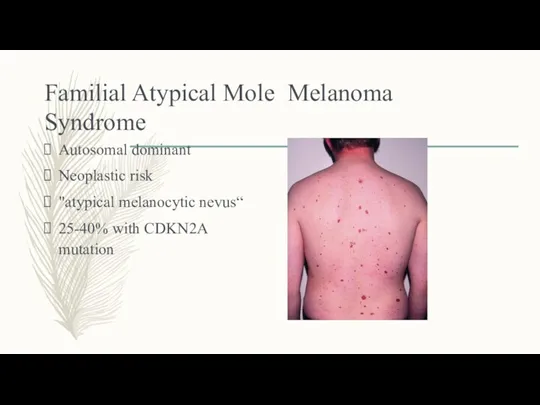
Familial Atypical Mole Melanoma Syndrome
Autosomal dominant
Neoplastic risk
"atypical melanocytic nevus“
25-40% with
Familial Atypical Mole Melanoma Syndrome
Autosomal dominant
Neoplastic risk
"atypical melanocytic nevus“
25-40% with
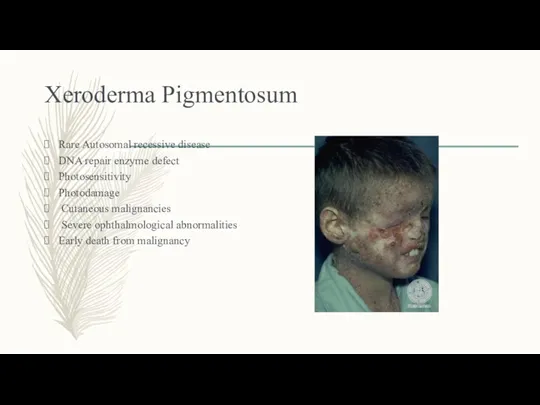
Xeroderma Pigmentosum
Rare Autosomal recessive disease
DNA repair enzyme defect
Photosensitivity
Photodamage
Cutaneous
Xeroderma Pigmentosum
Rare Autosomal recessive disease
DNA repair enzyme defect
Photosensitivity
Photodamage
Cutaneous
Ultraviolet light
Ultraviolet light
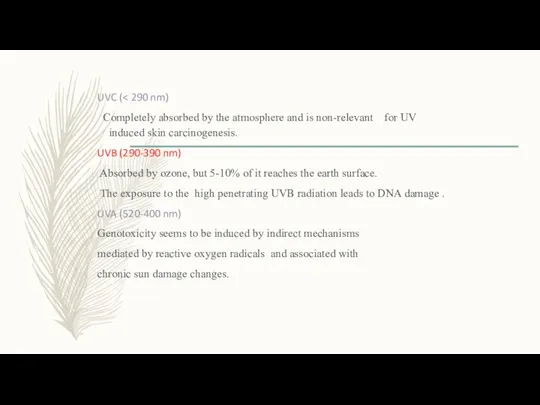
UVC (< 290 nm)
Completely absorbed by the atmosphere
UVC (< 290 nm)
Completely absorbed by the atmosphere
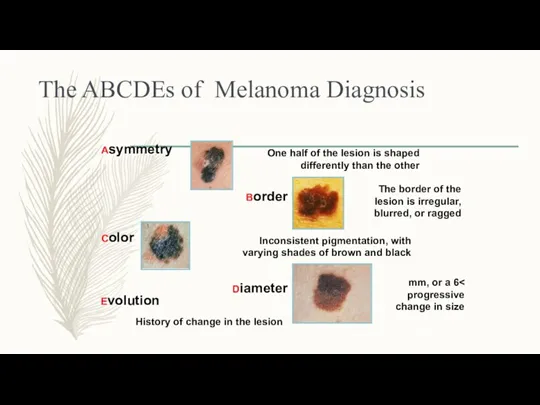
The ABCDEs of Melanoma Diagnosis
Asymmetry
One half of the lesion is shaped
The ABCDEs of Melanoma Diagnosis
Asymmetry
One half of the lesion is shaped
TYPES OF MELANOMA
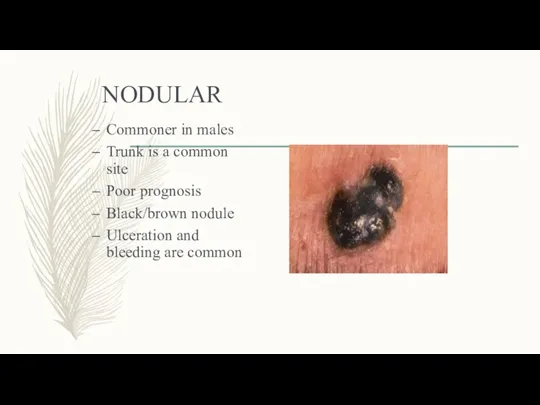
NODULAR
Commoner in males
Trunk is a common site
Poor prognosis
Black/brown nodule
Ulceration and bleeding
NODULAR
Commoner in males
Trunk is a common site
Poor prognosis
Black/brown nodule
Ulceration and bleeding
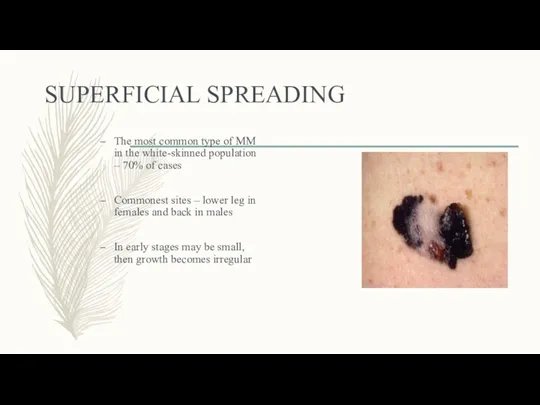
SUPERFICIAL SPREADING
The most common type of MM in the white-skinned population
SUPERFICIAL SPREADING
The most common type of MM in the white-skinned population
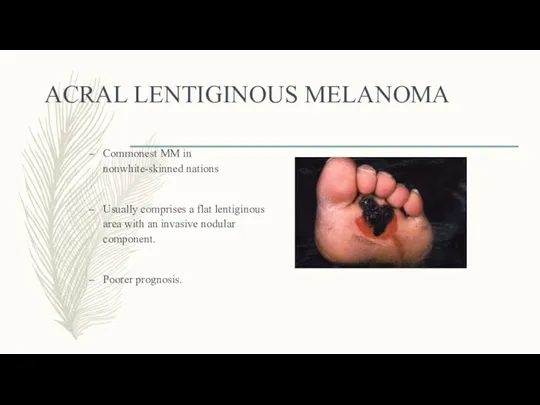
ACRAL LENTIGINOUS MELANOMA
Commonest MM in nonwhite-skinned nations
Usually comprises a flat lentiginous
ACRAL LENTIGINOUS MELANOMA
Commonest MM in nonwhite-skinned nations
Usually comprises a flat lentiginous
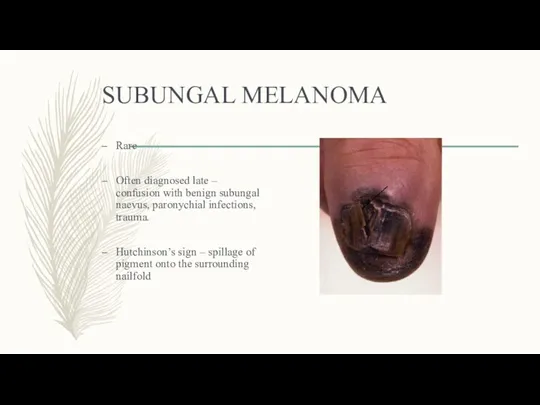
SUBUNGAL MELANOMA
Rare
Often diagnosed late – confusion with benign subungal naevus, paronychial
SUBUNGAL MELANOMA
Rare
Often diagnosed late – confusion with benign subungal naevus, paronychial
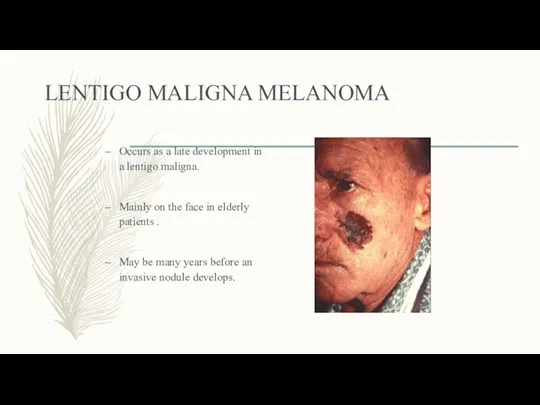
LENTIGO MALIGNA MELANOMA
Occurs as a late development in a lentigo maligna.
Mainly
LENTIGO MALIGNA MELANOMA
Occurs as a late development in a lentigo maligna.
Mainly
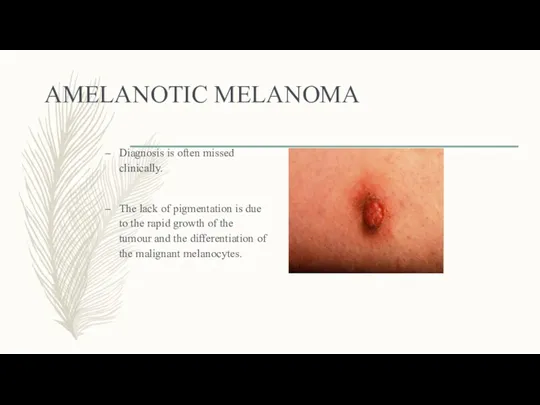
AMELANOTIC MELANOMA
Diagnosis is often missed clinically.
The lack of pigmentation is due
AMELANOTIC MELANOMA
Diagnosis is often missed clinically.
The lack of pigmentation is due
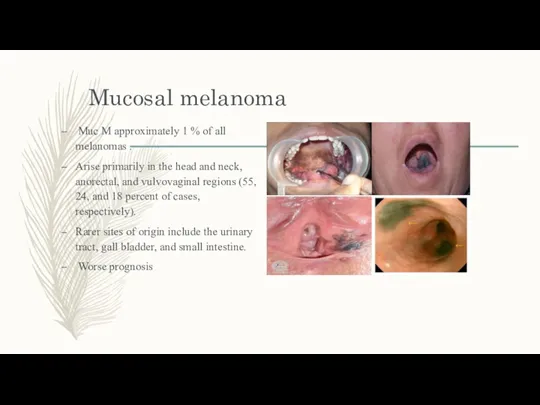
Mucosal melanoma
Muc M approximately 1 % of all melanomas .
Arise
Mucosal melanoma
Muc M approximately 1 % of all melanomas .
Arise
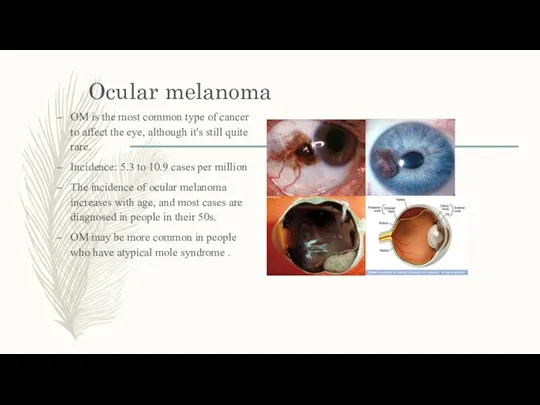
Ocular melanoma
OM is the most common type of cancer to affect
Ocular melanoma
OM is the most common type of cancer to affect
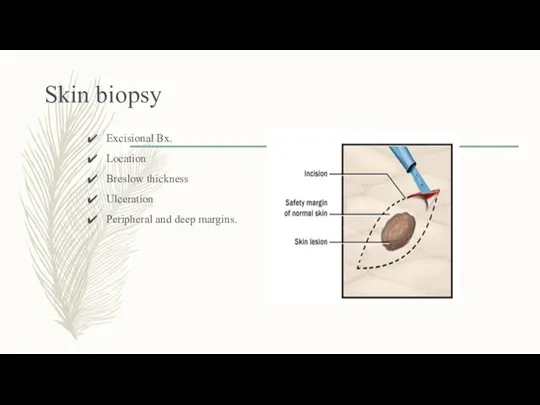
Skin biopsy
Excisional Bx.
Location
Breslow thickness
Ulceration
Peripheral and deep margins.
Skin biopsy
Excisional Bx.
Location
Breslow thickness
Ulceration
Peripheral and deep margins.
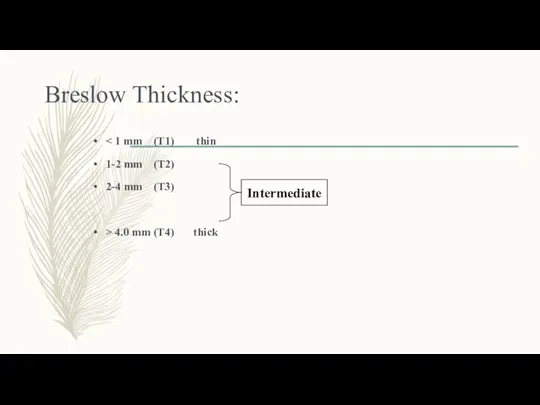
Breslow Thickness:
< 1 mm (T1) thin
1-2 mm (T2)
2-4 mm (T3)
>
Breslow Thickness:
< 1 mm (T1) thin
1-2 mm (T2)
2-4 mm (T3)
>
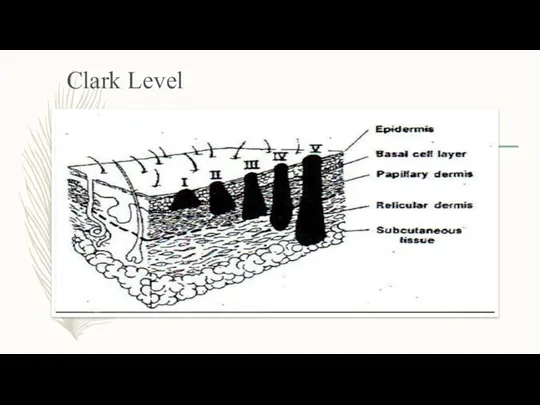
Clark Level
Clark Level
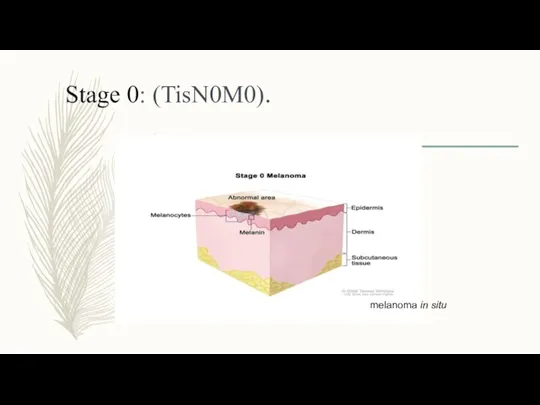
Stage 0: (TisN0M0).
melanoma in situ
Stage 0: (TisN0M0).
melanoma in situ
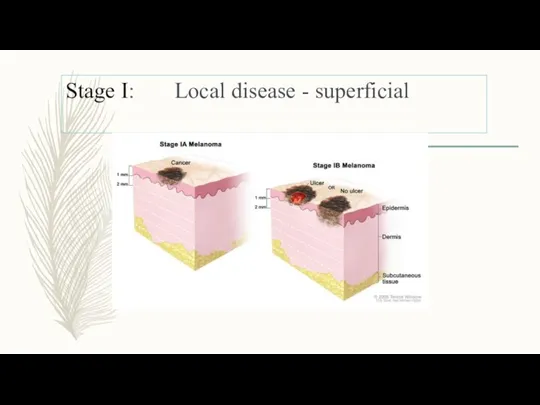
Stage I: Local disease - superficial
Stage I: Local disease - superficial
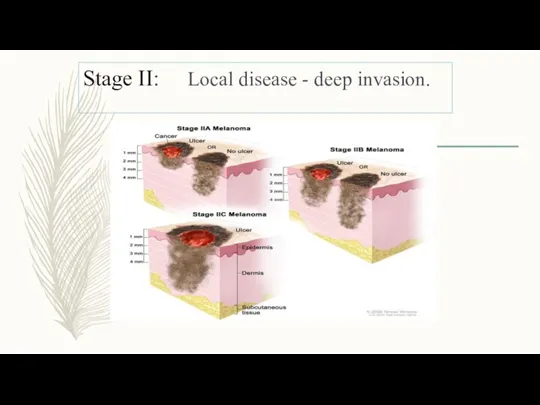
Stage II: Local disease - deep invasion.
Stage II: Local disease - deep invasion.
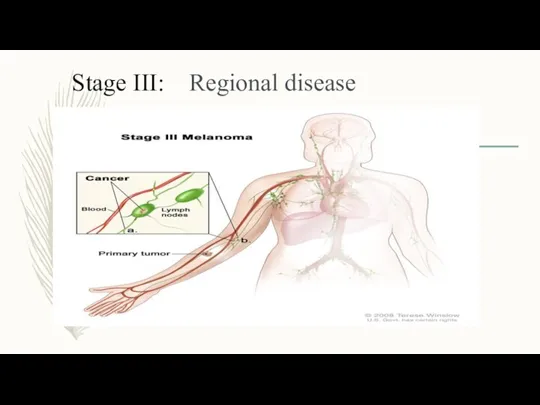
Stage III: Regional disease
Stage III: Regional disease
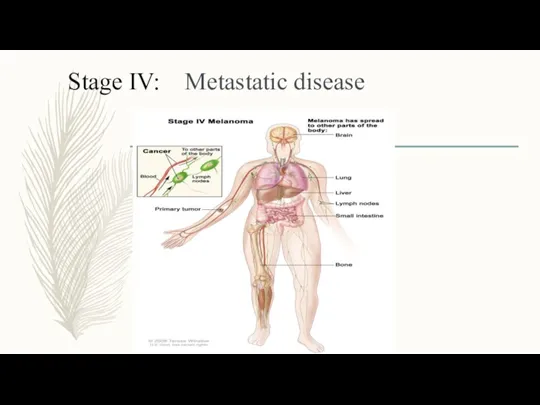
Stage IV: Metastatic disease
Stage IV: Metastatic disease
Prognostic factors
Depth of Invasion
Ulceration
Lymph Node
Mitotic Rate (TNM staging system 2010)
LDH level
Patient
Prognostic factors
Depth of Invasion
Ulceration
Lymph Node
Mitotic Rate (TNM staging system 2010)
LDH level
Patient
Sentinel lymph node biopsy
SLN = First node(s) draining the area
Sentinel lymph node biopsy
SLN = First node(s) draining the area
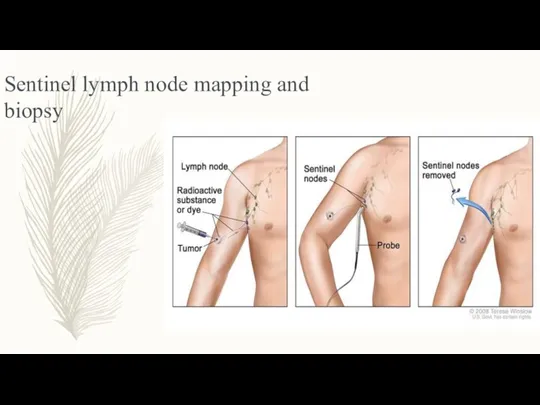
Sentinel lymph node mapping and biopsy
Sentinel lymph node mapping and biopsy
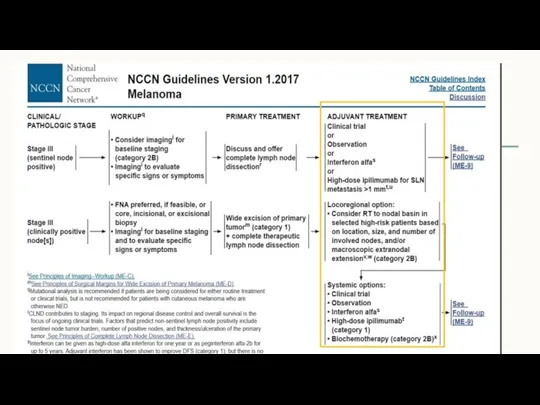
Adjuvant therapy
Potential candidates
Stage IIB
Stage III
Chemotherapy - not effective (DTIC).
Immunotherapy
Adjuvant therapy
Potential candidates
Stage IIB
Stage III
Chemotherapy - not effective (DTIC).
Immunotherapy
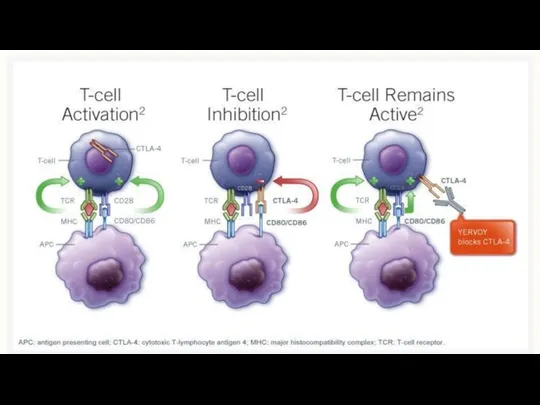
IPILIMUMAB
Yervoy
Anti CTLA4 Antibody
IPILIMUMAB
Yervoy
Anti CTLA4 Antibody
IFN α - Side effects
Acute toxicity :
(Due to PGE2 synthesis
IFN α - Side effects
Acute toxicity :
(Due to PGE2 synthesis

Treatment Options for advanced Melanoma
Treatment Options for advanced Melanoma
BRAF\MEK
Inhibitors
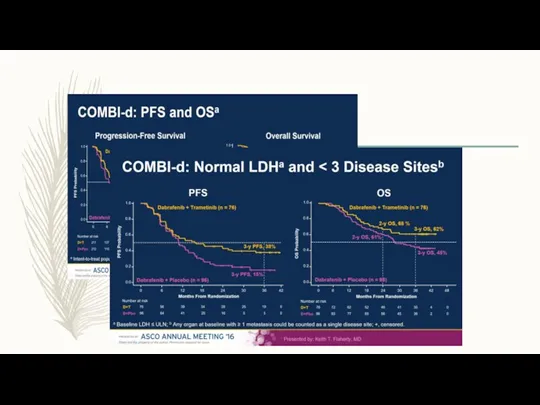
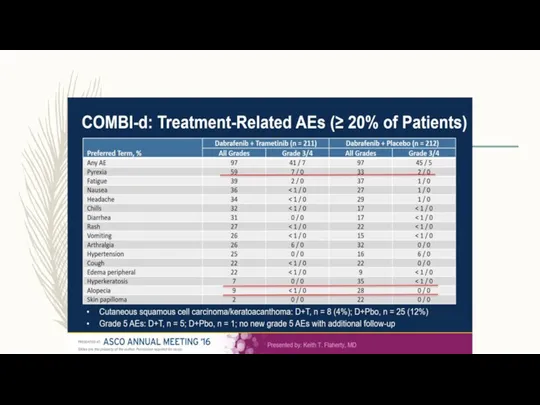
Dabrafenib (TAFINLAR) Trametinib ( MEKINIST)
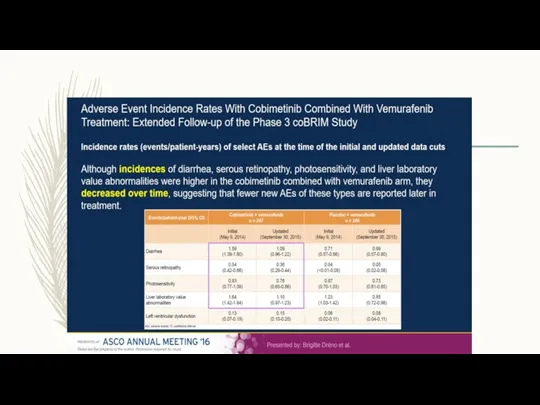
Vemurafenib ( ZELBORAF) Cobimetinib (COTELIC)
BRAF\MEK
Inhibitors
Dabrafenib (TAFINLAR) Trametinib ( MEKINIST)
Vemurafenib ( ZELBORAF) Cobimetinib (COTELIC)

Imunotherapy
Imunotherapy
Ipillimumab (Yervoy)
In pooled analysis of 12 studies, a plateau in the
Ipillimumab (Yervoy)
In pooled analysis of 12 studies, a plateau in the

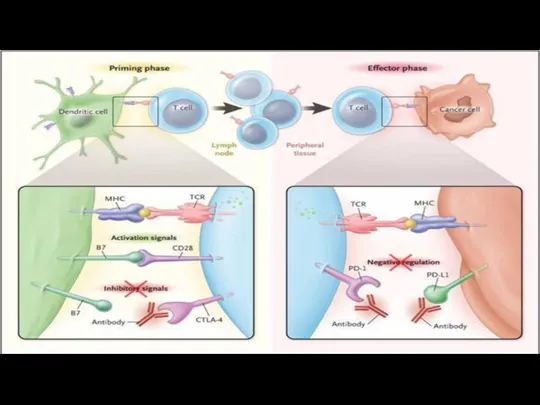
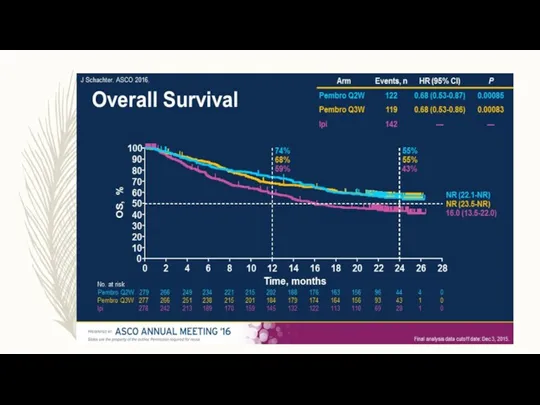
Anti PD1 therapy :
Opdivo (Nivolumab)
Keytruda
(Pembrolizumab)
Anti PD1 therapy :
Opdivo (Nivolumab)
Keytruda
(Pembrolizumab)
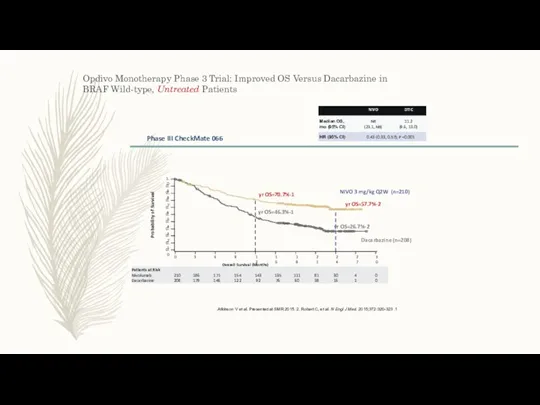
Opdivo Monotherapy Phase 3 Trial: Improved OS Versus Dacarbazine in BRAF
Opdivo Monotherapy Phase 3 Trial: Improved OS Versus Dacarbazine in BRAF
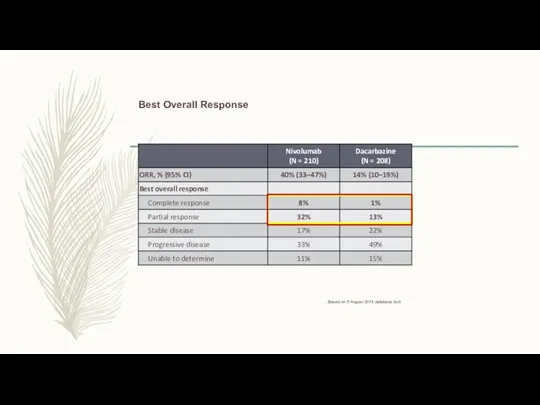
Best Overall Response
Based on 5 August 2014 database lock.
Best Overall Response
Based on 5 August 2014 database lock.
Updated Results From a Phase III Trial of Nivolumab Combined With
Updated Results From a Phase III Trial of Nivolumab Combined With
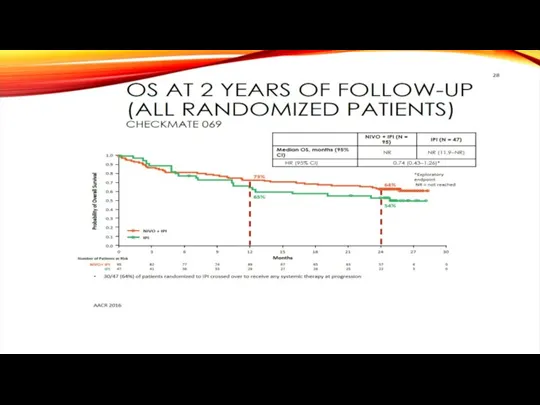
OS at 2 Years of Follow-up
(All Randomized Patients)
Checkmate 069
30/47 (64%) of
OS at 2 Years of Follow-up
(All Randomized Patients)
Checkmate 069
30/47 (64%) of
Response To Treatment
Response To Treatment
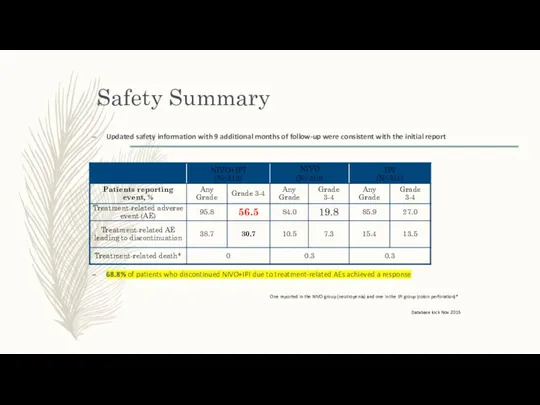
Safety Summary
Updated safety information with 9 additional months of follow-up were
Safety Summary
Updated safety information with 9 additional months of follow-up were
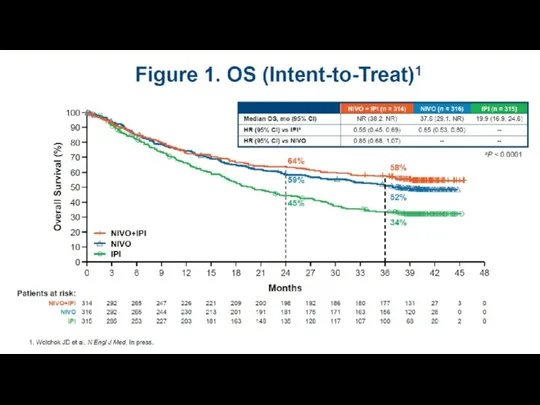
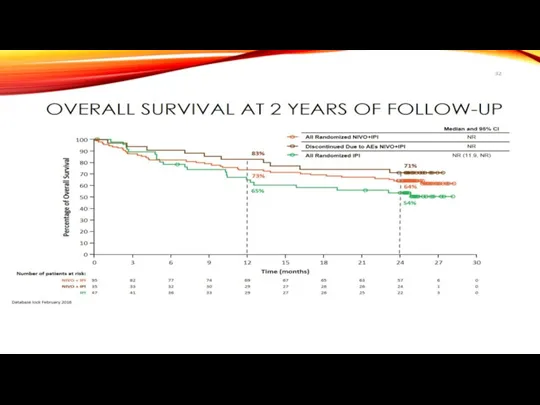
Overall Survival at 2 Years of Follow-up
83%
71%
73%
64%
65%
54%
Database lock February 2016
Number of
Overall Survival at 2 Years of Follow-up
83%
71%
73%
64%
65%
54%
Database lock February 2016
Number of
J.M. Michot et al. European Journal of Cancer 54 (2016)
J.M. Michot et al. European Journal of Cancer 54 (2016)
Boutros et al. Nature Reviews Clinical Oncology Volume: 13, Pages:473–486 Year
Boutros et al. Nature Reviews Clinical Oncology Volume: 13, Pages:473–486 Year
Nature Reviews Clinical Oncology
Volume:
13,
Pages:
473–486
Year published:
(2016)
DOI:
doi:10.1038/nrclinonc.2016.58
Published online
04 May 2016
Boutros et al.
Volume:
13,
Pages:
473–486
Year published:
(2016)
DOI:
doi:10.1038/nrclinonc.2016.58
Published online
04 May 2016
Boutros et al.
Webber JS , Safety profile of nivolumab in patients with advanced
Webber JS , Safety profile of nivolumab in patients with advanced
 Тіс, тіс қатарлары ақауын емдеу
Тіс, тіс қатарлары ақауын емдеу Десмургія. Техніка накладення пов'язок і шин
Десмургія. Техніка накладення пов'язок і шин Роль медицинской сестры палатной при соблюдении лечебно-охранительного режима в стационаре
Роль медицинской сестры палатной при соблюдении лечебно-охранительного режима в стационаре проект
проект Обезболивание. Наркоз
Обезболивание. Наркоз Науқастың күтімі және оның маңызы
Науқастың күтімі және оның маңызы Ботулизм. Возбудители ботулизма
Ботулизм. Возбудители ботулизма Сердце, аорта, кровь, вены, капилляры
Сердце, аорта, кровь, вены, капилляры Расстройства личности и поведения в зрелом возрасте (психопатии)
Расстройства личности и поведения в зрелом возрасте (психопатии) Гепатит B. Молекулярная биология
Гепатит B. Молекулярная биология Лечение артериальной гипертензии
Лечение артериальной гипертензии Мозжечок, синдромы поражения. Экстрапирамидная система, синдромы поражения
Мозжечок, синдромы поражения. Экстрапирамидная система, синдромы поражения Острые лимфобластные лейкозы
Острые лимфобластные лейкозы Первая помощь при травмах
Первая помощь при травмах Методы изучения генетики. Медико-генетическое консультирование
Методы изучения генетики. Медико-генетическое консультирование Таным туралы ілім. Медициналық, ғылыми танымның ерекшелігі
Таным туралы ілім. Медициналық, ғылыми танымның ерекшелігі Ethics and Human Rights in Medicine and Medical Research
Ethics and Human Rights in Medicine and Medical Research Меланома кожи. Диагностика, клиника и лечение
Меланома кожи. Диагностика, клиника и лечение Легионеллез
Легионеллез Отек и выпот
Отек и выпот Прогнозирование потребности в лекарственных средствах
Прогнозирование потребности в лекарственных средствах Актуализация формулярной системы в гериатрическом стационаре
Актуализация формулярной системы в гериатрическом стационаре Грыжи. Составные элементы грыжи
Грыжи. Составные элементы грыжи Частная анатомия зубов
Частная анатомия зубов Ранняя диагностика острого лейкоза у детей
Ранняя диагностика острого лейкоза у детей Наследственные болезни человека
Наследственные болезни человека Модели взаимоотношения врач-пациент. Моральные принципы и правила проведения исследований на человеке и животных
Модели взаимоотношения врач-пациент. Моральные принципы и правила проведения исследований на человеке и животных Климактерический синдром
Климактерический синдром