- Medical history pediatric diagnosis in progress

Содержание
- 2. Medicine medicine is the science of diagnosing, treating, or preventing disease and damage to the body,
- 4. Sickness
- 5. Sickness Patient - doctor
- 6. Medical aid
- 7. Medical aid Routine prophylactic investigations (screening) before job offering, study, military service etc.
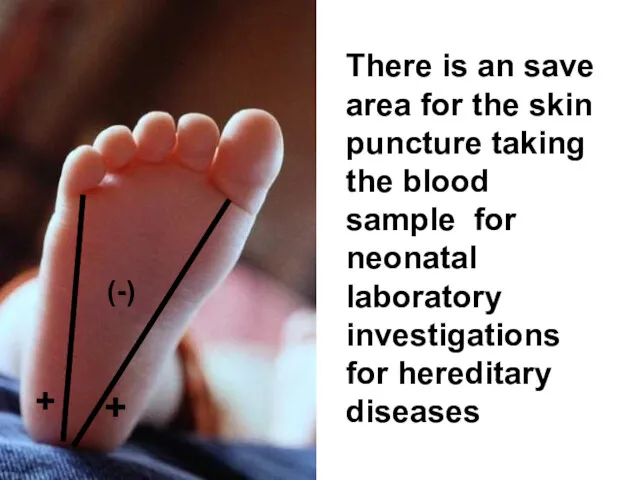
- 8. The medical neonatal screening is one of the most efficient ways of innate and hereditary diseases
- 9. (-) + + There is an save area for the skin puncture taking the blood sample
- 11. Medical aid Accidents
- 12. Medical aid patient`s visits
- 13. What is the medicine? А. The Art В. The Science С. The Service D. The Source
- 14. What is the medicine? А. The Art В. The Science С. The Service D. The Source
- 15. Medical service Physician Patient
- 16. Competency, qualification Communication Marketing Service Physician Management
- 17. Competency, qualification Competency (from Latin – competere, correspond to, approach) ability to use the knowledge, skills,
- 18. The Medical textbooks, reference books, periodic journals, lectures. Practical training
- 20. ICD-10
- 21. Zaporozhye State Medical University Propedeutics of Pediatrics Department STUDENT’S CASE HISTORY (SCH) The patient’s name, surname___________________
- 22. Management Management or administration are skills to organize an efficient control over the social relationships (for
- 23. А
- 24. В
- 25. С
- 26. D
- 27. Medical marketing Medical marketing (MARKETING as a sale, trade on the market) is a process of
- 28. In healthcare practice Compliance is a patient's and doctor's adherence to a chosen course ( eg,
- 29. Before visit Knock and carefully open the door Greet everyone with cordial manner Confirm personality of
- 30. Hand`s washing Наказ №149
- 31. Modesty & temperance
- 32. The Communication The Communication (in psychology) is an exchange by information between alive organisms. In common
- 33. Communication with the patient`s relatives and directly with the child (…the roses and their thorns)
- 34. The principals of efficient communication During interview follow all time to look at the mother. It
- 35. pacifist potentate, boss Conservative trailblazer, innovator + + + + (-) PTPC
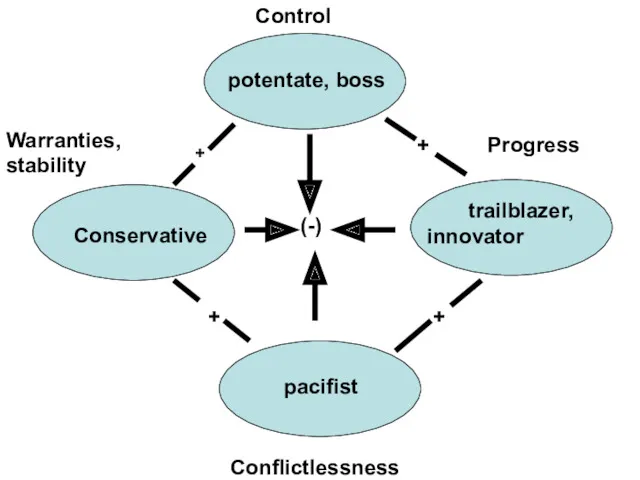
- 36. pacifist potentate, boss Conservative trailblazer, innovator + + + + (-) Control Progress Warranties, stability Conflictlessness
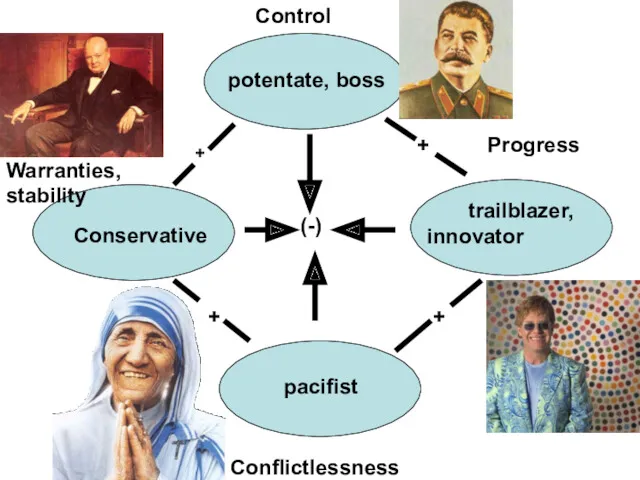
- 37. pacifist potentate, boss Conservative trailblazer, innovator + + + + (-) Control Progress Warranties, stability Conflictlessness
- 38. Medical history The Correct medical history is only one way to reach the correct diagnosis. The
- 39. The main goal of the medical history is the gathering of symptoms
- 40. Symptom (from greece σύμπτομα as event, coincidence, sign) is one separate sign, frequent manifestation of some
- 41. I. Passport data 1. Patient’s surname, first and second name. 2. Age, date of birth (age
- 42. Куру
- 43. Complaints
- 44. Ask the parents or the child about the causes of their visit. First, enumerate complaints, second
- 45. It is Important to take into account not only complaints of relatives, but also complaints of
- 46. III. History of the disease, Present illness (Anamnesis morbi) (According the mother's information) Development of the
- 47. IV. Past history, Anamnesis vitae (for child from birth to 3 yrs old) The child was
- 48. The newborn’s condition Specific data include (1) weight and length, head and chest circumferences at birth;
- 49. Weight loss in first few days: 5-10% of BWt (birth weight). Return to BWt: 7 –
- 50. Characteristic of physical development Weight, height, head, chest circumference gain. The most important previous growth patterns
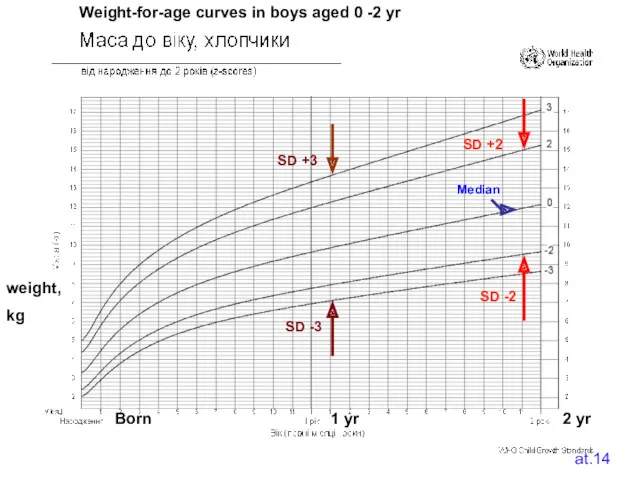
- 51. If to build a graph having the child age postponed on horizontal axis and the anthropometric
- 52. at.14 Median SD +2 SD -2 SD -3 SD +3 Weight-for-age curves in boys aged 0
- 53. What do the SD lines mean? The line 0 on every graph is being the median
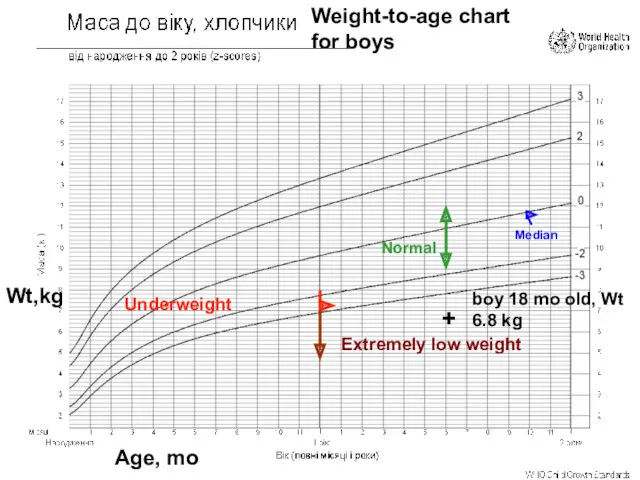
- 55. Median Underweight Normal Extremely low weight + boy 18 mo old, Wt 6.8 kg Weight-to-age chart
- 57. Median Growth delay Normalrange Extremely short stature + + Stature cm Age, mo Stature-to-age chart in
- 59. Median Underfeeding Normal Alimentary marasmus Risk of overweight Overweight Obesity Wt,kg Stature, cm Weight-to-height correlation
- 60. Body-Weight index (BWi or Ketle`s index). Obesity in young children – BWi > 20 kg/m² Obesity
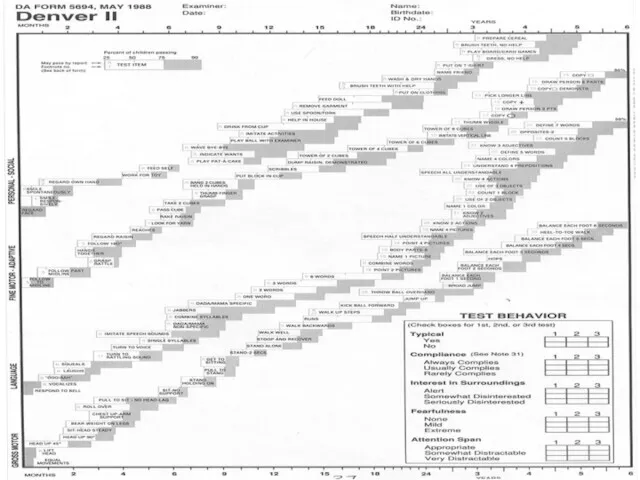
- 61. Developmental milestones include (1) age of holding up head steadily, (2) age of sitting alone without
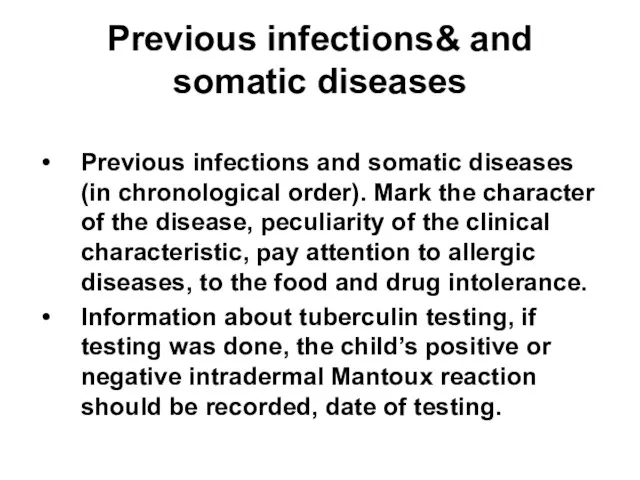
- 63. Previous infections& and somatic diseases Previous infections and somatic diseases (in chronological order). Mark the character
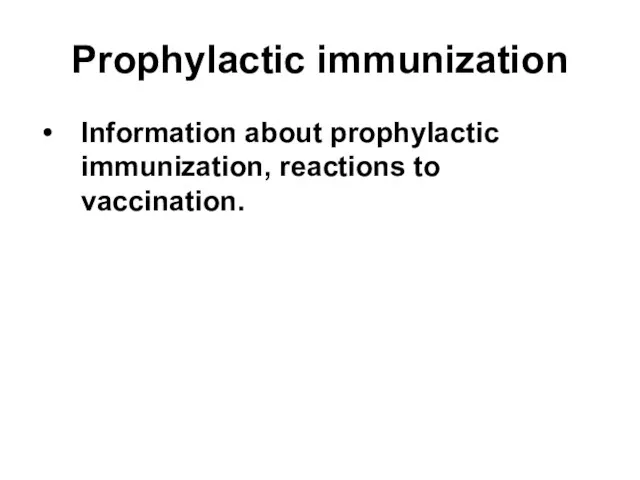
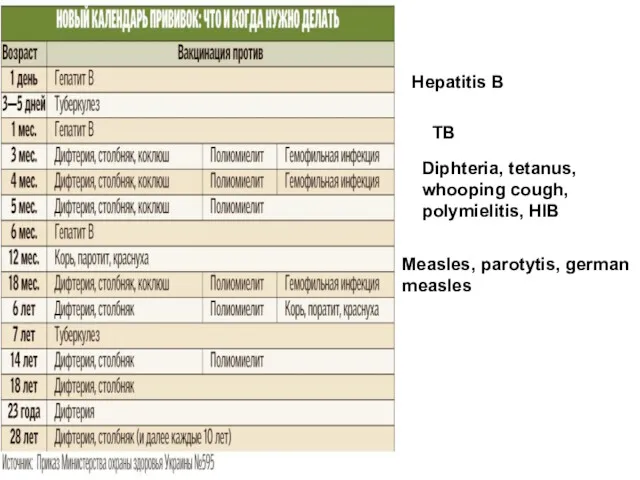
- 64. Prophylactic immunization Information about prophylactic immunization, reactions to vaccination.
- 65. Hepatitis B TB Diphteria, tetanus, whooping cough, polymielitis, HIB Measles, parotytis, german measles
- 66. The child's hygienic regime, who takes care for the child, the term of being out-doors, sleep
- 67. V. Family history (to identify the presence of genetic traits or diseases that have familial tendencies
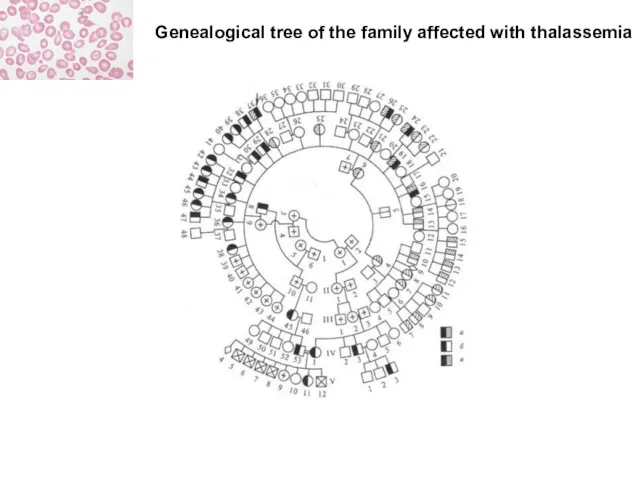
- 68. Genealogical tree of the family affected with thalassemia
- 69. Пробанд
- 70. Status praesens objectivus
- 71. The child looks well
- 72. 1. General condition of the patient is mild, moderate, severe , and life-threatening. conscious, unconscious Patient's
- 73. 2. Physical development and its assessment. Weight (P) in kg, height (L) in cm, circumference of
- 74. Conclusion: underweight (underfeeding), low weight, extremely low weight (marasmus) etc.
- 75. Objective examination is a complex medical diagnostic approach executed by physician to reveal the diagnosis. All
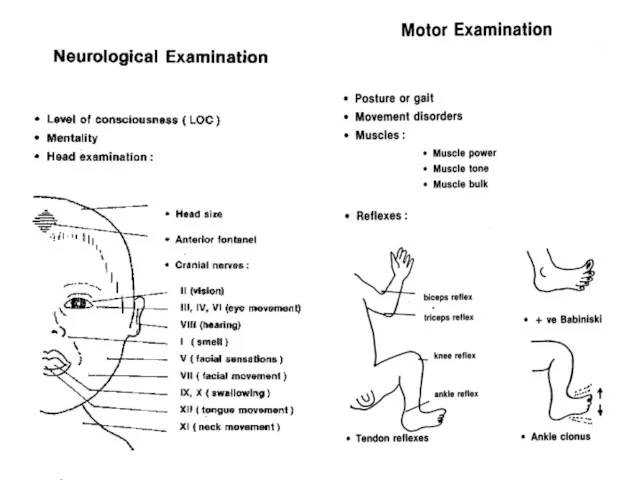
- 76. 3. Nervous system Level of consciousness (LOC): alert and oriented to person, place, and time; loss
- 78. 4. Skin: color (usual for proper race, pale, cyanotic, hyperemic, icteric etc.), abnormal pigmentation (depigmentation, hypopigmentation,
- 79. 5. Visible mucous membranes and conjunctivae: color, clear or not. 6. Subcutaneous tissue: its development (normal,
- 80. 7. Lymph nodes: palpation of lymph nodes (their size in cm if enlarged, their consistence, mobility,
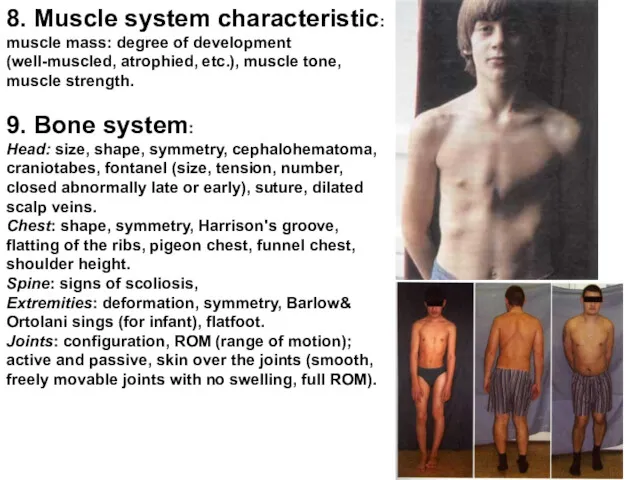
- 81. 8. Muscle system characteristic: muscle mass: degree of development (well-muscled, atrophied, etc.), muscle tone, muscle strength.
- 82. Dysplastic / dislocative hip (DDH) tests
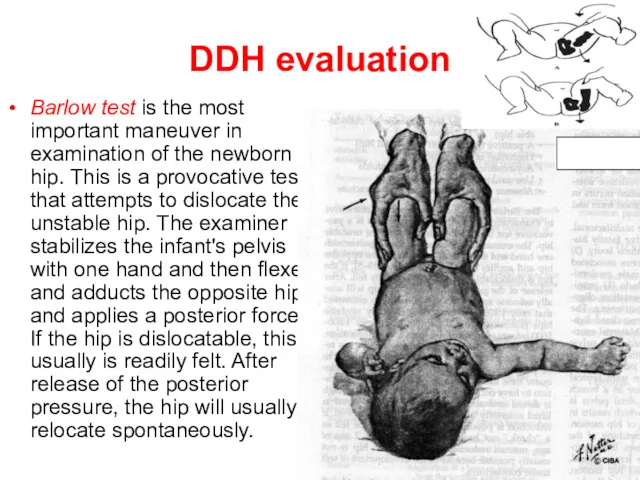
- 83. DDH evaluation Barlow test is the most important maneuver in examination of the newborn hip. This
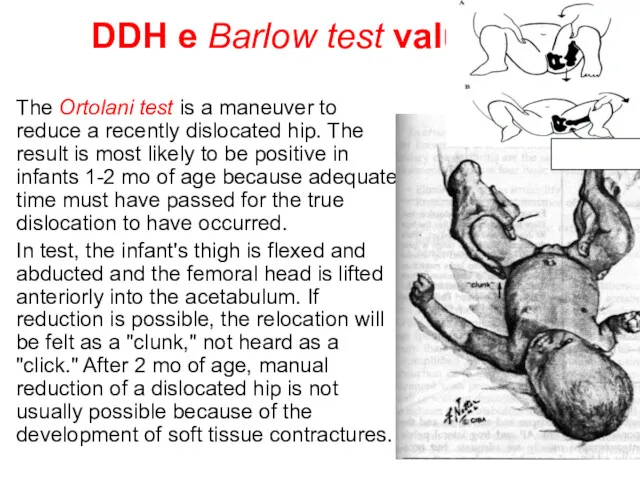
- 84. DDH e Barlow test valuation The Ortolani test is a maneuver to reduce a recently dislocated
- 85. 10. Respiratory system Inspection: cyanosis, finger clubbing, nasal flaring, the type of respiration (thoracic, abdominal, mixed;
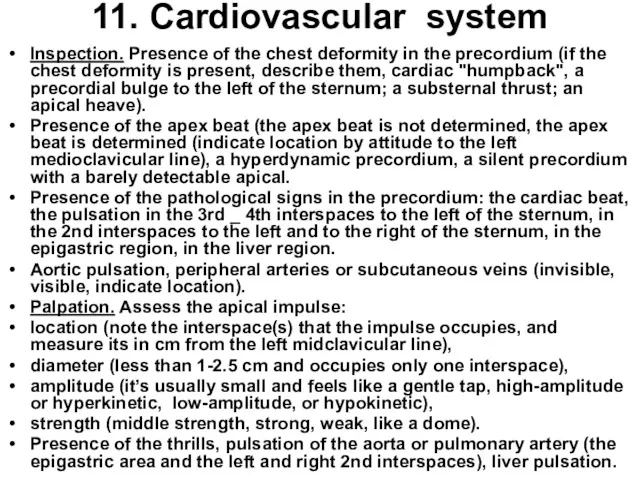
- 87. 11. Cardiovascular system Inspection. Presence of the chest deformity in the precordium (if the chest deformity
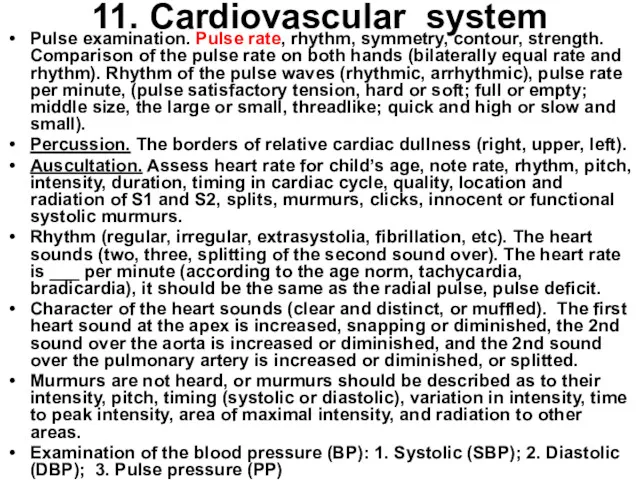
- 88. 11. Cardiovascular system Pulse examination. Pulse rate, rhythm, symmetry, contour, strength. Comparison of the pulse rate
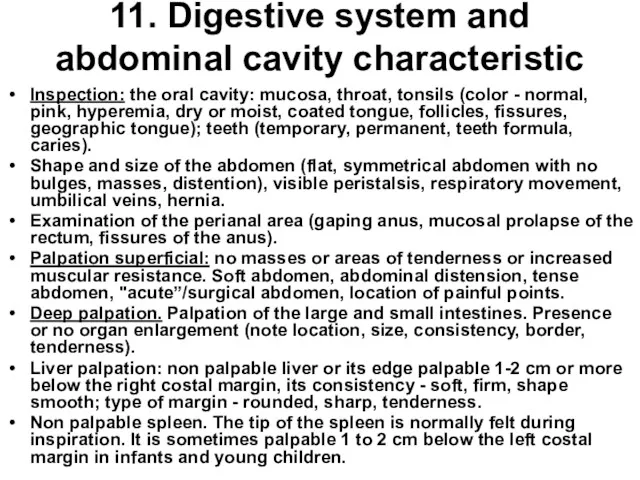
- 89. 11. Digestive system and abdominal cavity characteristic Inspection: the oral cavity: mucosa, throat, tonsils (color -
- 90. 11. Digestive system and abdominal cavity characteristic Percussion of the abdomen: tympany in all four quadrants,
- 91. 6EDCB BCDE6 6EDCB1 1BCDE6 6 seal
- 92. 12. Urinary system Inspection of lumbal region, bimanual palpation of kidneys (nonpalpable kidneys or solid, firm,
- 93. 13. Endocrine system characteristic. Disorders of growth (gigantism, nanism), and body weight (malnutrition, obesity), allocation of
- 94. Preliminary (provisional) diagnosis In medicineIn medicine a syndrome is the association of several clinically recognizable features,
- 95. Syndrome For instance, the headache, malaise, fever correspond to acute infectious or flu like syndrome in
- 96. Laboratory investigations
- 97. CBC RBC Plattellet cells count WBC Differential count • ESR • Pathological bleeding
- 98. Методы визуализации The methods of visualization
- 99. Instrumental methods of diagnostics
- 100. Medical diagnosis Medical diagnosis (often simply termed diagnosis) refers to the process of attempting to determine
- 101. Diagnosis (from greece διάγνωσις - recognition) is conclusion about essence of the disease in a patient
- 102. ICD-10 ICD-10 is the 10th revision of the International Statistical Classification of Diseases and Related Health
- 103. 15. Summary diagnostic conclusion Summary diagnostic conclusion should be done according to the patient’s complaints, illness
- 104. Consilium (Latin - counsel, discussion) is counsel of several scientists of one or different professions. The
- 105. Diagnosis is right if it can be confirmed (for instance, ex juvantibus – Latin – by
- 107. Скачать презентацию
Medicine
medicine is the science of diagnosing, treating, or preventing disease and
Medicine
medicine is the science of diagnosing, treating, or preventing disease and


Sickness
Sickness
Sickness
Patient - doctor
Sickness
Patient - doctor

Medical aid
Medical aid
Medical aid
Routine prophylactic investigations (screening) before job offering, study, military
Medical aid
Routine prophylactic investigations (screening) before job offering, study, military
The medical neonatal screening is one of the most efficient
The medical neonatal screening is one of the most efficient
(-)
+
+
There is an save area for the skin puncture
(-)
+
+
There is an save area for the skin puncture


Medical aid
Accidents
Medical aid
Accidents
Medical aid
patient`s visits
Medical aid
patient`s visits
What is the medicine?
А. The Art
В. The Science
С. The
What is the medicine?
А. The Art
В. The Science
С. The
What is the medicine?
А. The Art
В. The Science
С. The
What is the medicine?
А. The Art
В. The Science
С. The
Medical service
Physician
Patient
Medical service
Physician
Patient
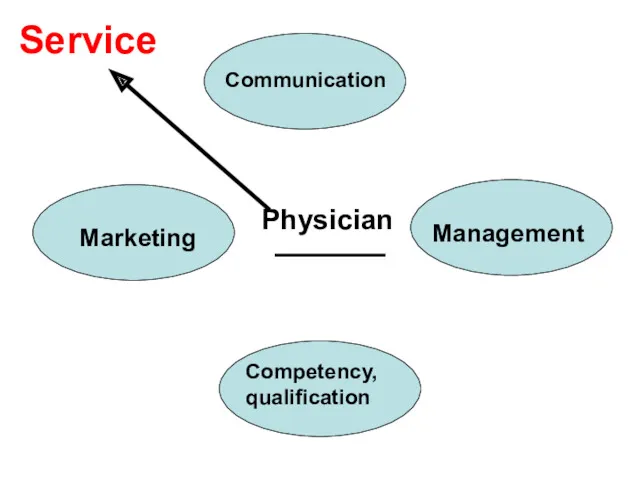
Competency, qualification
Communication
Marketing
Service
Physician
Management
Competency, qualification
Communication
Marketing
Service
Physician
Management
Competency, qualification
Competency (from Latin – competere, correspond to, approach) ability to
Competency, qualification
Competency (from Latin – competere, correspond to, approach) ability to
The Medical textbooks, reference books, periodic journals, lectures.
Practical training
The Medical textbooks, reference books, periodic journals, lectures.
Practical training

ICD-10
ICD-10
Zaporozhye State Medical University
Propedeutics of Pediatrics Department
STUDENT’S CASE HISTORY
(SCH)
The patient’s
Zaporozhye State Medical University
Propedeutics of Pediatrics Department
STUDENT’S CASE HISTORY
(SCH)
The patient’s
Management
Management or administration are skills to organize an efficient control over
Management
Management or administration are skills to organize an efficient control over
А
А

В
В
С
С

D
D
Medical marketing
Medical marketing (MARKETING as a sale, trade on the market)
Medical marketing
Medical marketing (MARKETING as a sale, trade on the market)
In healthcare practice Compliance is a patient's and doctor's adherence to
In healthcare practice Compliance is a patient's and doctor's adherence to
Before visit
Knock and carefully open the door
Greet everyone with cordial
Before visit
Knock and carefully open the door
Greet everyone with cordial
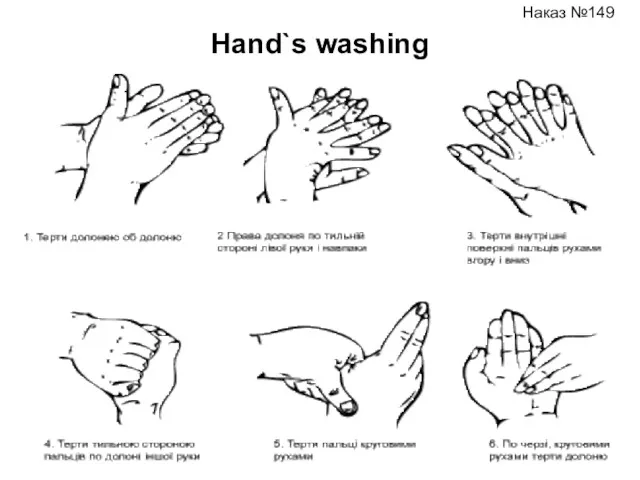
Hand`s washing
Наказ №149
Hand`s washing
Наказ №149

Modesty & temperance
The Communication
The Communication (in psychology) is an exchange by information between
The Communication
The Communication (in psychology) is an exchange by information between
Communication with the patient`s relatives and directly with the child
(…the
Communication with the patient`s relatives and directly with the child
(…the
The principals of efficient communication
During interview follow all time to
The principals of efficient communication
During interview follow all time to
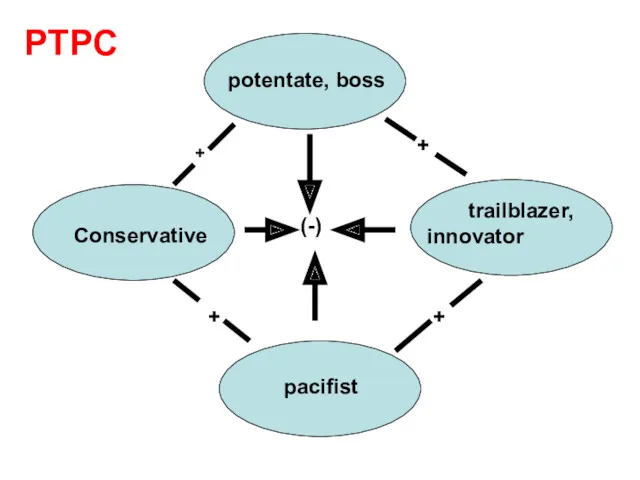
pacifist
potentate, boss
Conservative
trailblazer, innovator
+
+
+
+
(-)
PTPC
pacifist
potentate, boss
Conservative
trailblazer, innovator
+
+
+
+
(-)
PTPC
pacifist
potentate, boss
Conservative
trailblazer, innovator
+
+
+
+
(-)
pacifist
potentate, boss
Conservative
trailblazer, innovator
+
+
+
+
(-)
pacifist
potentate, boss
Conservative
trailblazer, innovator
+
+
+
+
(-)
pacifist
potentate, boss
Conservative
trailblazer, innovator
+
+
+
+
(-)
Medical history
The Correct medical history is only one way to reach
Medical history
The Correct medical history is only one way to reach
The main goal of the medical history is the gathering of
The main goal of the medical history is the gathering of
Symptom (from greece σύμπτομα as event, coincidence, sign) is one separate
Symptom (from greece σύμπτομα as event, coincidence, sign) is one separate
I. Passport data
1. Patient’s surname, first and second name.
2. Age, date
I. Passport data
1. Patient’s surname, first and second name.
2. Age, date
Куру
Куру

Complaints
Complaints
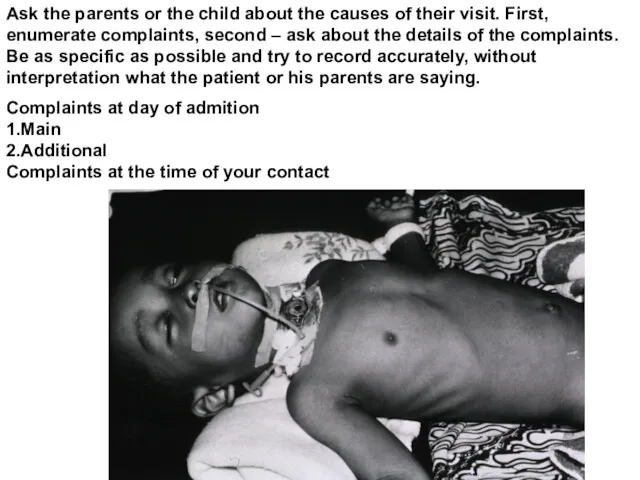
Ask the parents or the child about the causes of their
Ask the parents or the child about the causes of their
It is Important to take into account not only complaints of
It is Important to take into account not only complaints of
III. History of the disease, Present illness (Anamnesis morbi)
(According the mother's
III. History of the disease, Present illness (Anamnesis morbi)
(According the mother's
IV. Past history, Anamnesis vitae
(for child from birth to 3 yrs
IV. Past history, Anamnesis vitae (for child from birth to 3 yrs
The newborn’s condition
Specific data include
(1) weight and length, head
The newborn’s condition
Specific data include
(1) weight and length, head
Weight loss in first few days: 5-10% of BWt (birth weight).
Weight loss in first few days: 5-10% of BWt (birth weight).
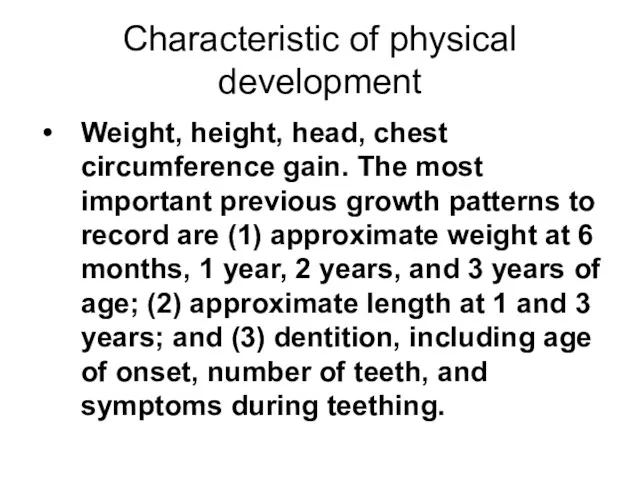
Characteristic of physical development
Weight, height, head, chest circumference gain. The most
Characteristic of physical development
Weight, height, head, chest circumference gain. The most
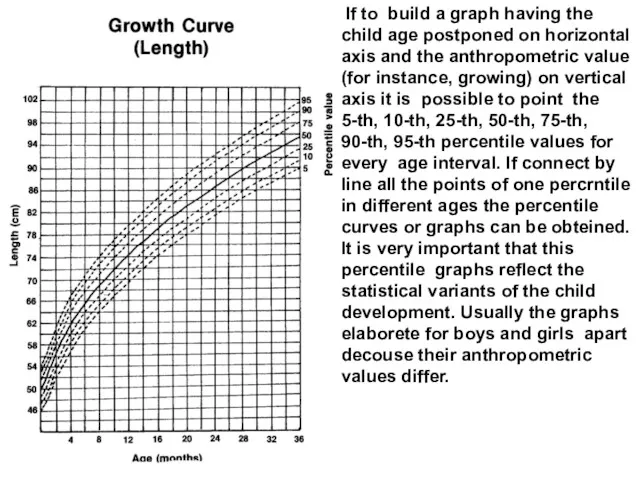
If to build a graph having the child age postponed
If to build a graph having the child age postponed
at.14
Median
SD +2
SD -2
SD -3
SD +3
Weight-for-age curves
at.14
Median
SD +2
SD -2
SD -3
SD +3
Weight-for-age curves
What do the SD lines mean?
The line 0 on every
What do the SD lines mean?
The line 0 on every
Median
Underweight
Normal
Extremely low weight
+
boy 18 mo old, Wt 6.8
Median
Underweight
Normal
Extremely low weight
+
boy 18 mo old, Wt 6.8
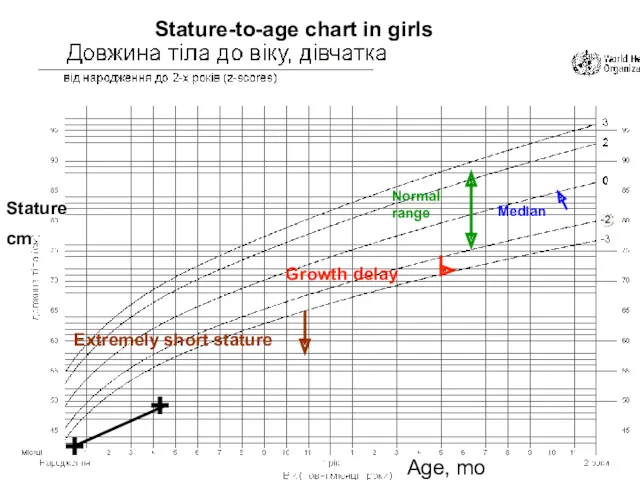
Median
Growth delay
Normalrange
Extremely short stature
+
+
Stature
cm
Age, mo
Stature-to-age chart in girls
Median
Growth delay
Normalrange
Extremely short stature
+
+
Stature
cm
Age, mo
Stature-to-age chart in girls

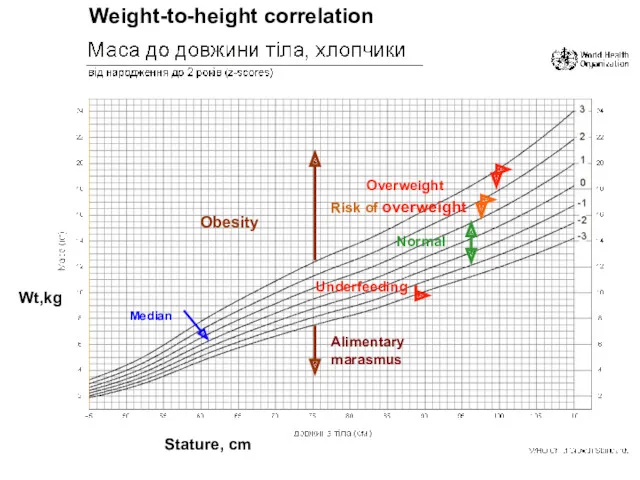
Median
Underfeeding
Normal
Alimentary marasmus
Risk of overweight
Overweight
Obesity
Wt,kg
Stature, cm
Weight-to-height correlation
Median
Underfeeding
Normal
Alimentary marasmus
Risk of overweight
Overweight
Obesity
Wt,kg
Stature, cm
Weight-to-height correlation
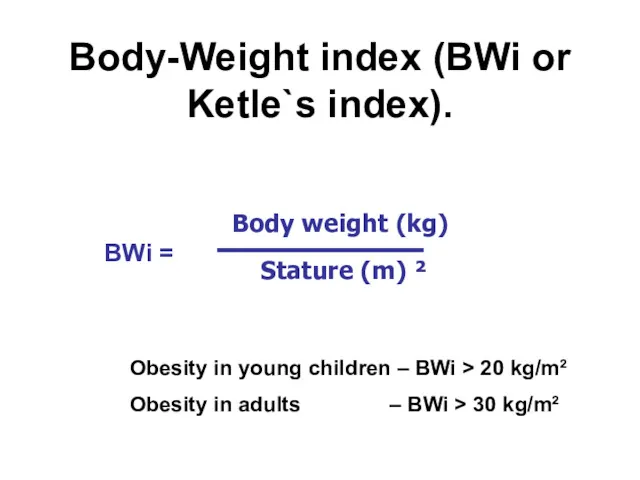
Body-Weight index (BWi or Ketle`s index).
Obesity in young children – BWi
Body-Weight index (BWi or Ketle`s index).
Obesity in young children – BWi
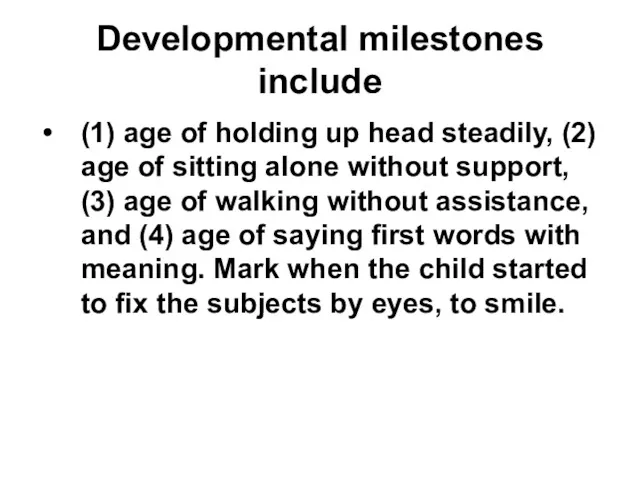
Developmental milestones include
(1) age of holding up head steadily, (2) age
Developmental milestones include
(1) age of holding up head steadily, (2) age
Previous infections& and somatic diseases
Previous infections and somatic diseases (in
Previous infections& and somatic diseases
Previous infections and somatic diseases (in
Prophylactic immunization
Information about prophylactic immunization, reactions to vaccination.
Prophylactic immunization
Information about prophylactic immunization, reactions to vaccination.
Hepatitis B
TB
Diphteria, tetanus, whooping cough, polymielitis, HIB
Measles, parotytis, german measles
Hepatitis B
TB
Diphteria, tetanus, whooping cough, polymielitis, HIB
Measles, parotytis, german measles
The child's hygienic regime, who takes care for the child, the
The child's hygienic regime, who takes care for the child, the
V. Family history
(to identify the presence of genetic traits or diseases
V. Family history
(to identify the presence of genetic traits or diseases
Genealogical tree of the family affected with thalassemia
Genealogical tree of the family affected with thalassemia
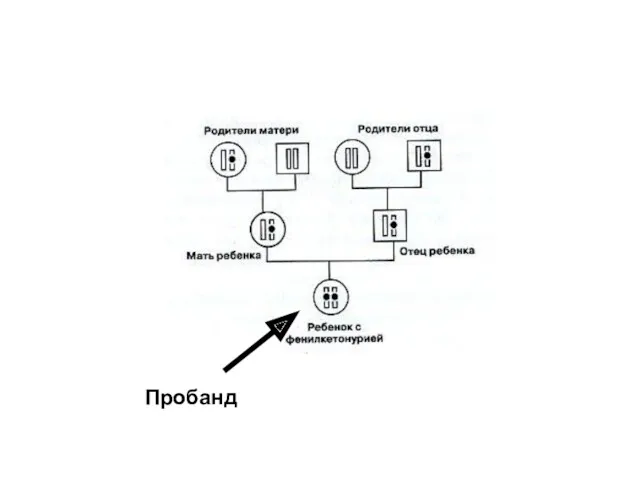
Пробанд
Пробанд
Status praesens objectivus
The child looks well
The child looks well
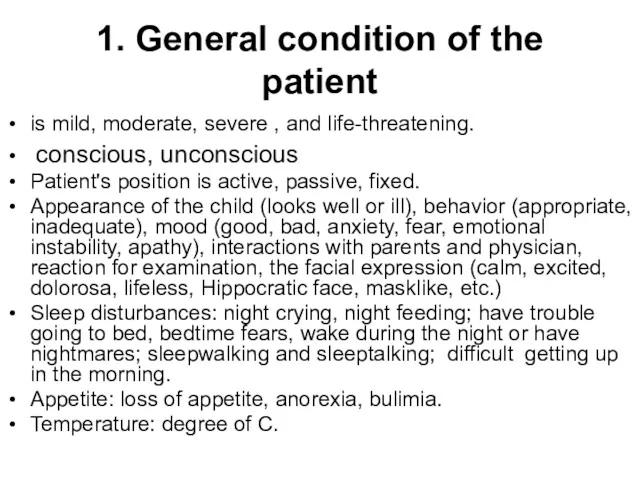
1. General condition of the patient
is mild, moderate, severe , and
1. General condition of the patient
is mild, moderate, severe , and
2. Physical development and its assessment.
Weight (P) in kg, height (L)
2. Physical development and its assessment.
Weight (P) in kg, height (L)
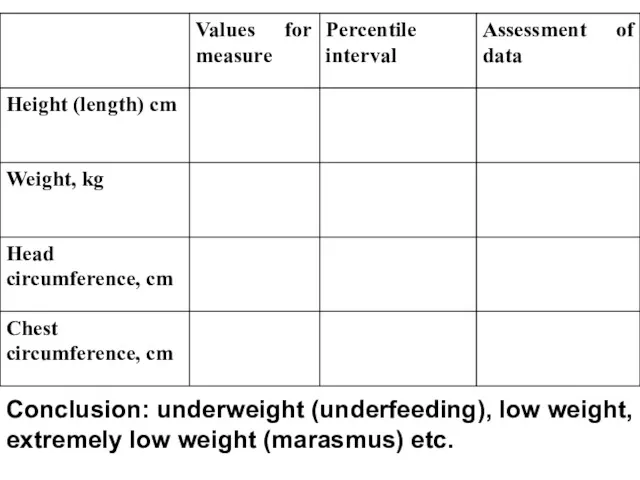
Conclusion: underweight (underfeeding), low weight, extremely low weight (marasmus) etc.
Conclusion: underweight (underfeeding), low weight, extremely low weight (marasmus) etc.
Objective examination is a complex medical diagnostic approach executed by physician
Objective examination is a complex medical diagnostic approach executed by physician
3. Nervous system
Level of consciousness (LOC): alert and oriented to person,
3. Nervous system
Level of consciousness (LOC): alert and oriented to person,
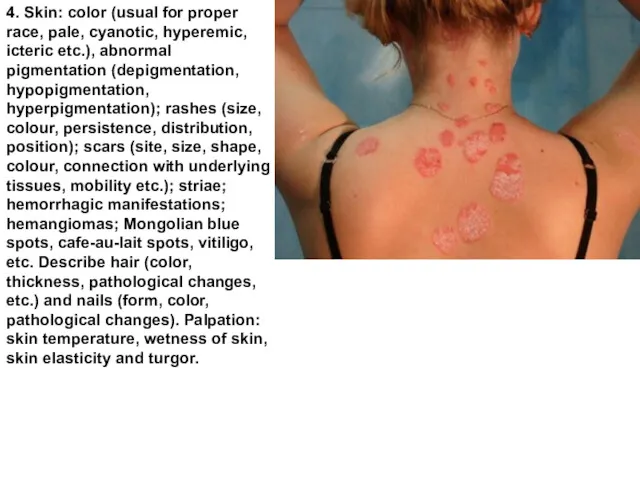
4. Skin: color (usual for proper race, pale, cyanotic, hyperemic, icteric
4. Skin: color (usual for proper race, pale, cyanotic, hyperemic, icteric
5. Visible mucous membranes and conjunctivae: color, clear or not.
6. Subcutaneous
5. Visible mucous membranes and conjunctivae: color, clear or not.
6. Subcutaneous
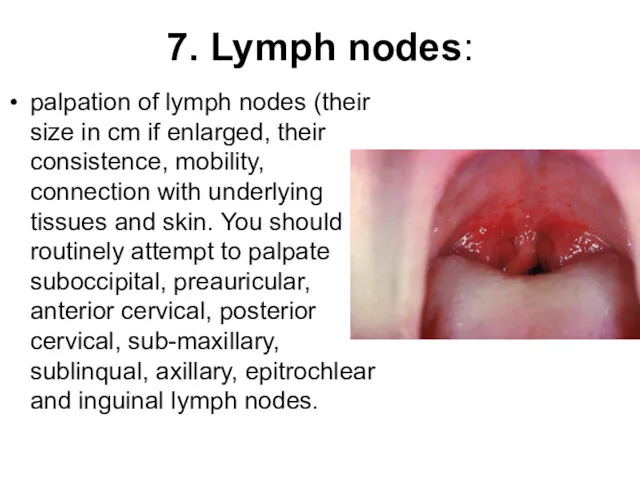
7. Lymph nodes:
palpation of lymph nodes (their size in cm if
7. Lymph nodes:
palpation of lymph nodes (their size in cm if
8. Muscle system characteristic: muscle mass: degree of development (well-muscled, atrophied,
8. Muscle system characteristic: muscle mass: degree of development (well-muscled, atrophied,

Dysplastic / dislocative hip (DDH) tests
Dysplastic / dislocative hip (DDH) tests
DDH evaluation
Barlow test is the most important maneuver in examination of
DDH evaluation
Barlow test is the most important maneuver in examination of
DDH e Barlow test valuation
The Ortolani test is a maneuver
DDH e Barlow test valuation
The Ortolani test is a maneuver
10. Respiratory system
Inspection: cyanosis, finger clubbing, nasal flaring, the type of
10. Respiratory system
Inspection: cyanosis, finger clubbing, nasal flaring, the type of
11. Cardiovascular system
Inspection. Presence of the chest deformity in the precordium
11. Cardiovascular system
Inspection. Presence of the chest deformity in the precordium
11. Cardiovascular system
Pulse examination. Pulse rate, rhythm, symmetry, contour, strength. Comparison
11. Cardiovascular system
Pulse examination. Pulse rate, rhythm, symmetry, contour, strength. Comparison
11. Digestive system and abdominal cavity characteristic
Inspection: the oral cavity: mucosa,
11. Digestive system and abdominal cavity characteristic
Inspection: the oral cavity: mucosa,
11. Digestive system and abdominal cavity characteristic
Percussion of the abdomen: tympany
11. Digestive system and abdominal cavity characteristic
Percussion of the abdomen: tympany

6EDCB BCDE6
6EDCB1 1BCDE6
6
seal
6EDCB BCDE6
6EDCB1 1BCDE6
6
seal
12. Urinary system
Inspection of lumbal region, bimanual palpation of kidneys (nonpalpable
12. Urinary system
Inspection of lumbal region, bimanual palpation of kidneys (nonpalpable
13. Endocrine system characteristic.
Disorders of growth (gigantism, nanism), and body weight
13. Endocrine system characteristic.
Disorders of growth (gigantism, nanism), and body weight
Preliminary (provisional) diagnosis
In medicineIn medicine a syndrome is the association of
Preliminary (provisional) diagnosis
In medicineIn medicine a syndrome is the association of
Syndrome
For instance, the headache, malaise, fever correspond to acute infectious
Syndrome
For instance, the headache, malaise, fever correspond to acute infectious

Laboratory investigations
Laboratory investigations
CBC
RBC
Plattellet cells count
WBC
Differential count
• ESR
• Pathological bleeding
CBC
RBC
Plattellet cells count
WBC
Differential count
• ESR
• Pathological bleeding
Методы визуализации
The methods of visualization
Методы визуализации
The methods of visualization
Instrumental methods of diagnostics
Instrumental methods of diagnostics
Medical diagnosis
Medical diagnosis (often simply termed diagnosis) refers to the process
Medical diagnosis
Medical diagnosis (often simply termed diagnosis) refers to the process
Diagnosis (from greece διάγνωσις - recognition) is conclusion about essence of
Diagnosis (from greece διάγνωσις - recognition) is conclusion about essence of
ICD-10
ICD-10 is the 10th revision of the International Statistical Classification of
ICD-10
ICD-10 is the 10th revision of the International Statistical Classification of
15. Summary diagnostic conclusion
Summary diagnostic conclusion should be done according to
15. Summary diagnostic conclusion
Summary diagnostic conclusion should be done according to

Consilium (Latin - counsel, discussion) is counsel of several scientists of
Consilium (Latin - counsel, discussion) is counsel of several scientists of
Diagnosis is right if it can be confirmed (for instance,
Diagnosis is right if it can be confirmed (for instance,
 Лекарственные растения успокаивающего действия
Лекарственные растения успокаивающего действия Невідкладні стани. Анафілактична та алергічна реакція
Невідкладні стани. Анафілактична та алергічна реакція Органы чувств. Чувствительность
Органы чувств. Чувствительность Борьба с допингом на современном этапе
Борьба с допингом на современном этапе Рак мочевого пузыря
Рак мочевого пузыря Дыхательная гимнастика А. Н. Стрельниковой
Дыхательная гимнастика А. Н. Стрельниковой Рак шейки матки. Факторы риска, диагностика, стадирование, лечение и прогноз
Рак шейки матки. Факторы риска, диагностика, стадирование, лечение и прогноз Оптимизация обучения студентов медицинского университета
Оптимизация обучения студентов медицинского университета Медицина катастроф. Крупнейшие чрезвычайные ситуации в России в конце 80-х годов
Медицина катастроф. Крупнейшие чрезвычайные ситуации в России в конце 80-х годов Аномалии рефракции
Аномалии рефракции Связь телосложения и заболеваний человека
Связь телосложения и заболеваний человека Основы педиатрии. Введение. Педиатрия и гигиена - основные понятия и принципы
Основы педиатрии. Введение. Педиатрия и гигиена - основные понятия и принципы Ветеринарно-санитарная экспертиза яиц
Ветеринарно-санитарная экспертиза яиц Неврологические проявления острых порфирий
Неврологические проявления острых порфирий Клинические формы первичного туберкулеза. Дифференциальная диагностика туберкулеза с другими заболеваниями. Лекция 4
Клинические формы первичного туберкулеза. Дифференциальная диагностика туберкулеза с другими заболеваниями. Лекция 4 Всесвітній день боротьби зі СНІДом
Всесвітній день боротьби зі СНІДом Методы исследования сердечно-сосудистой системы
Методы исследования сердечно-сосудистой системы Денсаулық сақтау саласының кез-келген қаржыландыру және басқару нысанында. Модернизациясы
Денсаулық сақтау саласының кез-келген қаржыландыру және басқару нысанында. Модернизациясы Стрес. Гостра стресова реакція. Посттравматична стресова реакція
Стрес. Гостра стресова реакція. Посттравматична стресова реакція Профилактика заболеваний. СПИД
Профилактика заболеваний. СПИД Расстройства эмоциональной, двигательно-волевой сферы
Расстройства эмоциональной, двигательно-волевой сферы Акушерия гинекологиядағы шуғыл жағдайлар. Ауруханадан тыс босану
Акушерия гинекологиядағы шуғыл жағдайлар. Ауруханадан тыс босану Пузырчатка (Pemphigus acantholyticus)
Пузырчатка (Pemphigus acantholyticus) Септический шок
Септический шок Clinical manifestation of HIV-infection
Clinical manifestation of HIV-infection Введение в дисциплину. Общие основы физической реабилитации в травматологии и ортопедии
Введение в дисциплину. Общие основы физической реабилитации в травматологии и ортопедии Поздние осложнения сахарного диабета
Поздние осложнения сахарного диабета Наркомании, токсикомании. Выявление болезней зависимости в общесоматической сети
Наркомании, токсикомании. Выявление болезней зависимости в общесоматической сети