- Menstrual cycle and it's disorders

Содержание
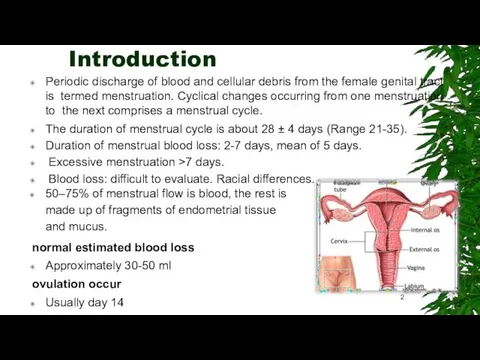
- 2. Introduction Periodic discharge of blood and cellular debris from the female genital tract is termed menstruation.
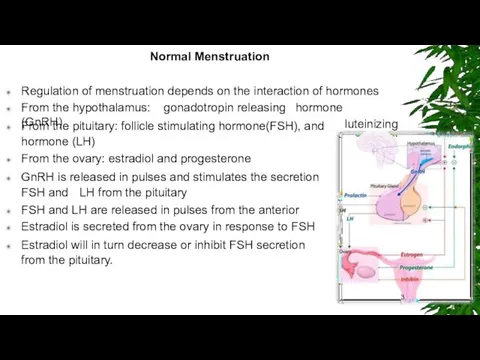
- 3. Normal Menstruation Regulation of menstruation depends on the interaction of hormones From the hypothalamus: gonadotropin releasing
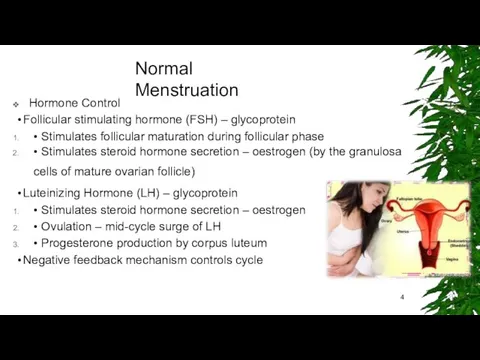
- 4. Normal Menstruation Hormone Control Follicular stimulating hormone (FSH) – glycoprotein • Stimulates follicular maturation during follicular
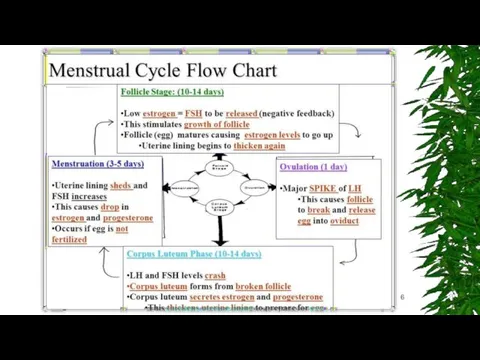
- 5. Menstrual cycle Phases The menstrual cycle is divided into three phases: Follicular (Preovulatory) Phase Ovulatory Phase
- 7. Menstrual Disorders There are a number of different menstrual disorders. Problems can range from heavy, painful
- 8. Dysmenorrhea (Painful Cramps) Dysmenorrhea is severe, frequent cramping during menstruation. Pain occurs in the lower abdomen
- 9. Causes of Dysmenorrhea (Painful Periods) Primary dysmenorrhea is caused by prostaglandins, hormone-like substances that are produced
- 10. Menorrhagia Menorrhagia is menstrual flow that lasts longer and is heavier than normal. The bleeding occurs
- 11. Metrorrhagia, also called breakthrough bleeding, refers to bleeding that occurs at irregular intervals and with variable
- 12. Causes of Menorrhagia (Heavy Bleeding) There are many possible causes for heavy bleeding: Hormonal Imbalances. Imbalances
- 13. Amenorrhea (Absence of Menstruation) Amenorrhea is the absence of menstruation. There are two categories: primary amenorrhea
- 14. Oligomenorrhea (Light or Infrequent Menstruation) Oligomenorrhea is a condition in which menstrual cycles are infrequent, greater
- 15. Causes of Amenorrhea and Oligomenorrhea (Absent or Light Periods) Consistently absent periods may be due to
- 16. Premenstrual Syndrome (PMS) Premenstrual syndrome (PMS) is a set of physical, emotional, and behavioural symptoms that
- 17. Risk Factors Age plays a key role in menstrual disorders. Girls who start menstruating at age
- 18. Complications Anaemia Menorrhagia is the most common cause of anaemia (reduction in red blood cells) in
- 19. Diagnosis Your doctor may ask questions concerning: Menstrual cycle patterns -- length of time between periods,
- 20. Blood, Hormonal Tests and ultrasound 1. Blood tests can help rule out other conditions that cause
- 21. Other Diagnostic Procedures Hysteroscopy. Hysteroscopy is a procedure that can detect the presence of fibroids, polyps,
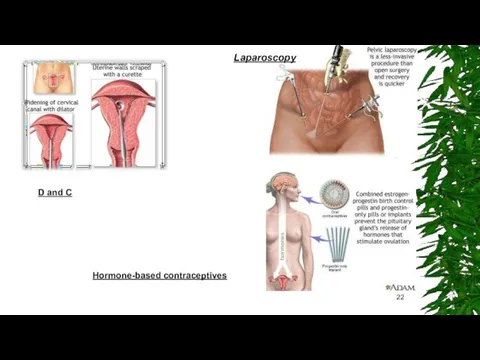
- 22. D and C Hormone-based contraceptives Laparoscopy
- 23. Lifestyle Changes Dietary Factors Making dietary adjustments starting about 14 days before a period may help
- 24. Other Lifestyle Measures Exercise. Exercise may help reduce menstrual pain. Sexual Activity. There have been reports
- 25. Alternative Remedies Acupuncture and Acupressure. Some studies have reported relief from pelvic pain after acupuncture or
- 26. Medications There are a number of different medicines prescribed for menstrual disorders. Common Pain Relievers for
- 27. Medications Oral Contraceptives Oral contraceptives (OCs), commonly called birth control pills or "the Pill," contain combinations
- 28. Medications Standard OCs usually come in a 28-pill pack with 21 days of “active” (hormone) pills
- 29. Medications Progestins Progestins (synthetic progesterone) are used by women with irregular or skipped periods to restore
- 30. Medications GnRH Agonists Gonadotropin releasing hormone (GnRH) agonists are sometimes used to treat severe menorrhagia. GnRH
- 31. Medications Non-Hormonal Drugs (Lysteda) Tranexamic acid (Lysteda) is a recently approved medication for treating heavy menstrual
- 32. Endometrial Ablation In endometrial ablation, the entire lining of the uterus (the endometrium) is removed or
- 34. Скачать презентацию
Introduction
Periodic discharge of blood and cellular debris from the female genital
Introduction
Periodic discharge of blood and cellular debris from the female genital
Normal Menstruation
Regulation of menstruation depends on the interaction of hormones
From the
Normal Menstruation
Regulation of menstruation depends on the interaction of hormones
From the
Normal Menstruation
Hormone Control
Follicular stimulating hormone (FSH) – glycoprotein
• Stimulates follicular maturation
Normal Menstruation
Hormone Control
Follicular stimulating hormone (FSH) – glycoprotein
• Stimulates follicular maturation
Menstrual cycle Phases
The menstrual cycle is divided into three phases:
Follicular (Preovulatory)
Menstrual cycle Phases
The menstrual cycle is divided into three phases:
Follicular (Preovulatory)
Menstrual Disorders
There are a number of different menstrual disorders. Problems can
Menstrual Disorders
There are a number of different menstrual disorders. Problems can
Dysmenorrhea (Painful Cramps)
Dysmenorrhea is severe, frequent cramping during menstruation. Pain occurs
Dysmenorrhea (Painful Cramps)
Dysmenorrhea is severe, frequent cramping during menstruation. Pain occurs
Causes of Dysmenorrhea (Painful Periods)
Primary dysmenorrhea is caused by prostaglandins, hormone-like
Causes of Dysmenorrhea (Painful Periods)
Primary dysmenorrhea is caused by prostaglandins, hormone-like
Menorrhagia
Menorrhagia is menstrual flow that lasts longer and is heavier than
Menorrhagia
Menorrhagia is menstrual flow that lasts longer and is heavier than
Metrorrhagia, also called breakthrough bleeding, refers to bleeding that occurs at
Metrorrhagia, also called breakthrough bleeding, refers to bleeding that occurs at
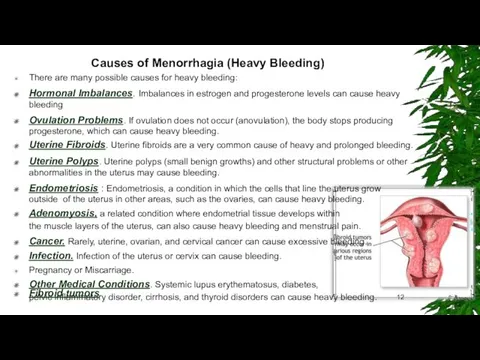
Causes of Menorrhagia (Heavy Bleeding)
There are many possible causes for heavy
Causes of Menorrhagia (Heavy Bleeding)
There are many possible causes for heavy
Amenorrhea (Absence of Menstruation)
Amenorrhea is the absence of menstruation. There are
Amenorrhea (Absence of Menstruation)
Amenorrhea is the absence of menstruation. There are
Oligomenorrhea (Light or Infrequent Menstruation)
Oligomenorrhea is a condition in which menstrual
Oligomenorrhea (Light or Infrequent Menstruation)
Oligomenorrhea is a condition in which menstrual
Causes of Amenorrhea and Oligomenorrhea (Absent or Light Periods)
Consistently absent periods
Causes of Amenorrhea and Oligomenorrhea (Absent or Light Periods)
Consistently absent periods
Premenstrual Syndrome (PMS)
Premenstrual syndrome (PMS) is a set of physical, emotional,
Premenstrual Syndrome (PMS)
Premenstrual syndrome (PMS) is a set of physical, emotional,
Risk Factors
Age plays a key role in menstrual disorders. Girls who
Risk Factors
Age plays a key role in menstrual disorders. Girls who
Complications
Anaemia
Menorrhagia is the most common cause of anaemia (reduction in red
Complications
Anaemia
Menorrhagia is the most common cause of anaemia (reduction in red
Diagnosis
Your doctor may ask questions concerning:
Menstrual cycle patterns -- length of
Diagnosis
Your doctor may ask questions concerning:
Menstrual cycle patterns -- length of
Blood, Hormonal Tests and ultrasound
1. Blood tests can help rule out other
Blood, Hormonal Tests and ultrasound
1. Blood tests can help rule out other
Other Diagnostic Procedures
Hysteroscopy. Hysteroscopy is a procedure that can detect the
Other Diagnostic Procedures
Hysteroscopy. Hysteroscopy is a procedure that can detect the
D and C
Hormone-based contraceptives
Laparoscopy
D and C
Hormone-based contraceptives
Laparoscopy
Lifestyle Changes
Dietary Factors
Making dietary adjustments starting about 14 days before a
Lifestyle Changes
Dietary Factors
Making dietary adjustments starting about 14 days before a
Other Lifestyle Measures
Exercise. Exercise may help reduce menstrual pain.
Sexual Activity. There
Other Lifestyle Measures
Exercise. Exercise may help reduce menstrual pain.
Sexual Activity. There
Alternative Remedies
Acupuncture and Acupressure. Some studies have reported relief from pelvic
Alternative Remedies
Acupuncture and Acupressure. Some studies have reported relief from pelvic
Medications
There are a number of different medicines prescribed for menstrual disorders.
Common
Medications
There are a number of different medicines prescribed for menstrual disorders.
Common
Medications
Oral Contraceptives
Oral contraceptives (OCs), commonly called birth control pills or "the
Medications
Oral Contraceptives
Oral contraceptives (OCs), commonly called birth control pills or "the
Medications
Standard OCs usually come in a 28-pill pack with 21 days
Medications
Standard OCs usually come in a 28-pill pack with 21 days
Medications
Progestins
Progestins (synthetic progesterone) are used by women with irregular or skipped
Medications
Progestins
Progestins (synthetic progesterone) are used by women with irregular or skipped
Medications
GnRH Agonists
Gonadotropin releasing hormone (GnRH) agonists are sometimes used to treat
Medications
GnRH Agonists
Gonadotropin releasing hormone (GnRH) agonists are sometimes used to treat
Medications
Non-Hormonal Drugs (Lysteda)
Tranexamic acid (Lysteda) is a recently approved medication for
Medications
Non-Hormonal Drugs (Lysteda)
Tranexamic acid (Lysteda) is a recently approved medication for
Endometrial Ablation
In endometrial ablation, the entire lining of the uterus (the
Endometrial Ablation
In endometrial ablation, the entire lining of the uterus (the
 Патогенные грибы. Обзор микозов
Патогенные грибы. Обзор микозов Физиология пищевода. Глотание. Лекция
Физиология пищевода. Глотание. Лекция Омыртқа жотасының физиологиялық және паталогиялық иілімдері
Омыртқа жотасының физиологиялық және паталогиялық иілімдері Биоэтические аспекты производства, дистрибьюции, рекламы и фальсификации лекарственных средств
Биоэтические аспекты производства, дистрибьюции, рекламы и фальсификации лекарственных средств Трихинеллёз. Возбудитель Трихинеллёза
Трихинеллёз. Возбудитель Трихинеллёза Синдром дефицита внимания и гиперактивности
Синдром дефицита внимания и гиперактивности Фитохимическое и фармакогностическое изучение лекарственных растений
Фитохимическое и фармакогностическое изучение лекарственных растений Диагностика геморрагических лихорадок, клещевого энцефалита, лайм-боррелиоза
Диагностика геморрагических лихорадок, клещевого энцефалита, лайм-боррелиоза Внутриматочные спирали
Внутриматочные спирали Комбинированные радиационные и химические поражения
Комбинированные радиационные и химические поражения Психопатии. Патохарактерологическое развитие личности
Психопатии. Патохарактерологическое развитие личности Лечение астматического статуса
Лечение астматического статуса Мікози. Клінічна класифікація мікозів
Мікози. Клінічна класифікація мікозів Свертывающая система крови. Гемостаз
Свертывающая система крови. Гемостаз Эффективность сиалиса по сравнению с плацебо вовремя восстановления эректильной дисфункции
Эффективность сиалиса по сравнению с плацебо вовремя восстановления эректильной дисфункции Шок. Патофизиология и принципы интенсивной терапии
Шок. Патофизиология и принципы интенсивной терапии Клинический случай. Менингит
Клинический случай. Менингит Актуальные проблемы педиатрии
Актуальные проблемы педиатрии Алла Ильинична Лёвушкина
Алла Ильинична Лёвушкина Острая и хроническая почечная недостаточность
Острая и хроническая почечная недостаточность Жақтың өсуінің негізгі кезеңдері
Жақтың өсуінің негізгі кезеңдері Средства для наркоза. Снотворные средства. Спирт этиловый
Средства для наркоза. Снотворные средства. Спирт этиловый Сепсис. Определение понятия
Сепсис. Определение понятия Планирование в здравоохранении
Планирование в здравоохранении Методы обследования полости рта
Методы обследования полости рта Красный крест
Красный крест Роль медицинской сестры в обеспечении качественной медицинской помощи при выполнении инъекций
Роль медицинской сестры в обеспечении качественной медицинской помощи при выполнении инъекций Нарушение речи
Нарушение речи