- murmur

Содержание
- 2. 11/12/02 Lubna Piracha, D.O. What is a Murmur? It maybe a normal or abnormal sound that
- 3. 11/12/02 Lubna Piracha, D.O. Timing and Location Timing: Systolic Diastolic Continuous Location: RUSB LUSB LLSB apex
- 4. 11/12/02 Lubna Piracha, D.O. Intensity and Frequency High Frequency MR TR AR Low Frequency MS TS
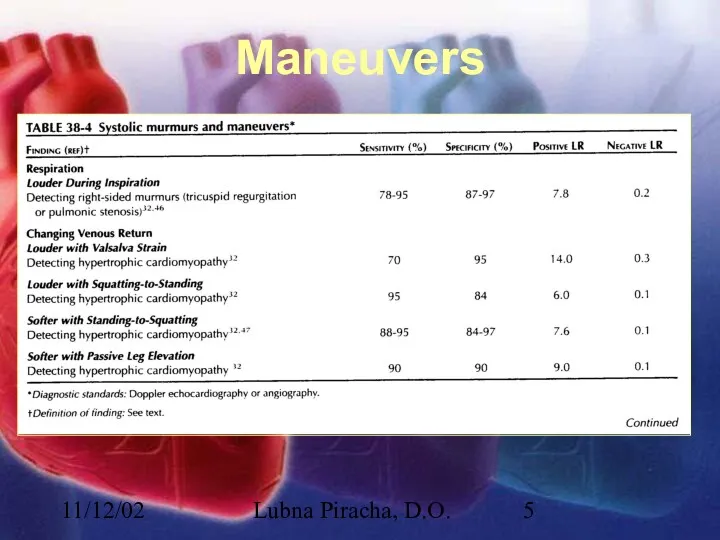
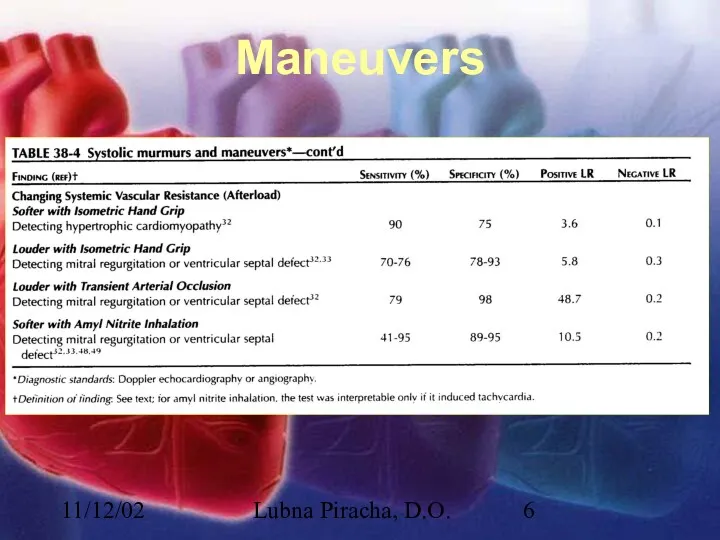
- 5. 11/12/02 Lubna Piracha, D.O. Maneuvers
- 6. 11/12/02 Lubna Piracha, D.O. Maneuvers
- 7. 11/12/02 Lubna Piracha, D.O. Case Studies A 50 year old male with a known heart murmur
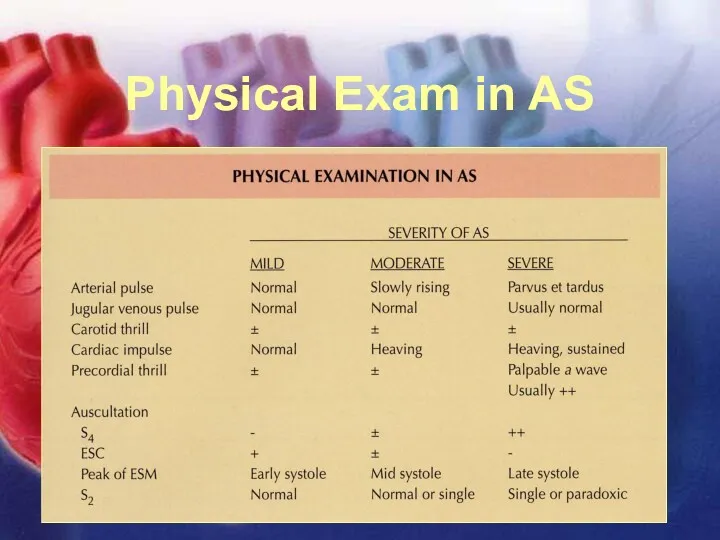
- 8. 11/12/02 Lubna Piracha, D.O. Physical Exam in AS
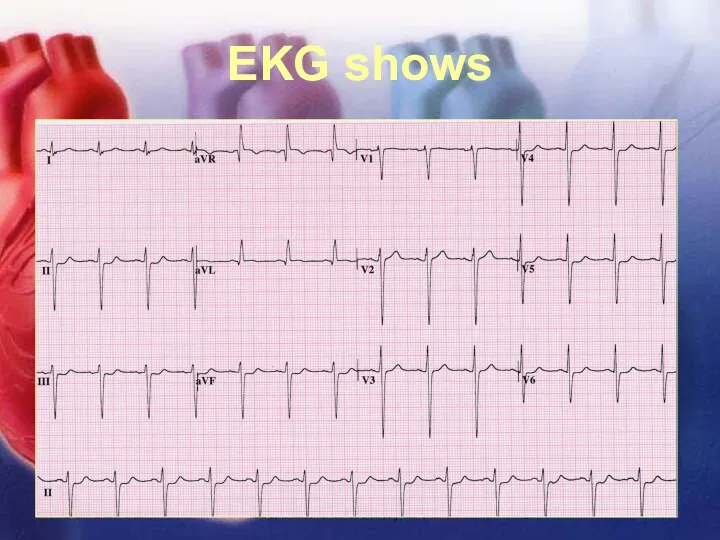
- 9. 11/12/02 Lubna Piracha, D.O. EKG shows
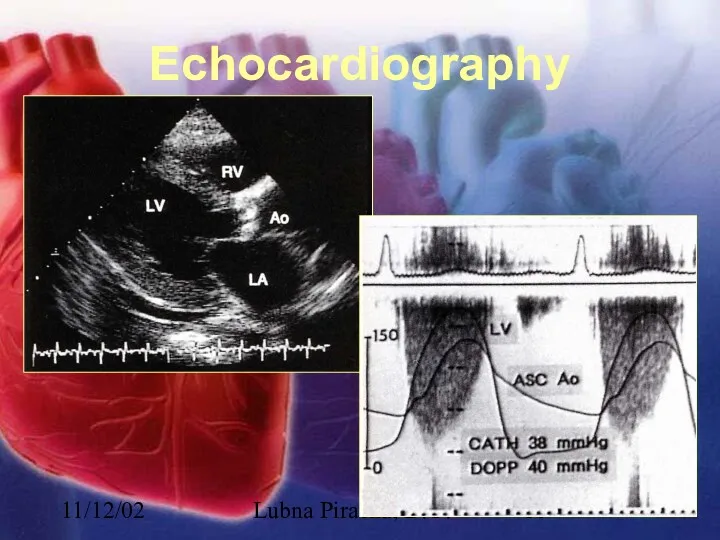
- 10. 11/12/02 Lubna Piracha, D.O. Echocardiography
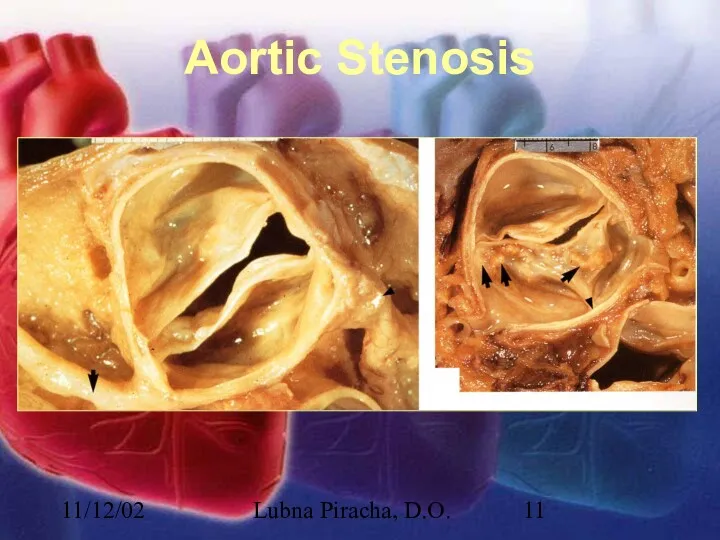
- 11. 11/12/02 Lubna Piracha, D.O. Aortic Stenosis
- 12. 11/12/02 Lubna Piracha, D.O. Aortic Stenosis There is little hemodynamic disturbance that occurs as the valve
- 13. 11/12/02 Lubna Piracha, D.O. Aortic Stenosis continued: Concentric hypertrophy develops in response to this overload. The
- 14. 11/12/02 Lubna Piracha, D.O. Case Study: A 45 year old male with a history of rheumatic
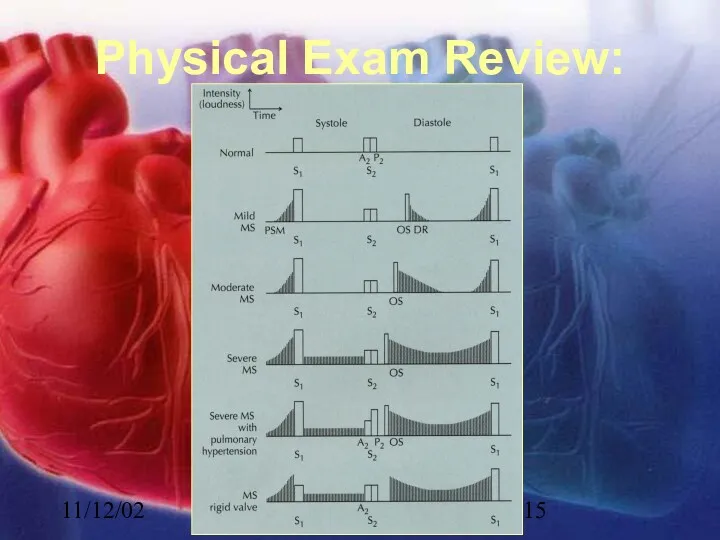
- 15. 11/12/02 Lubna Piracha, D.O. Physical Exam Review:
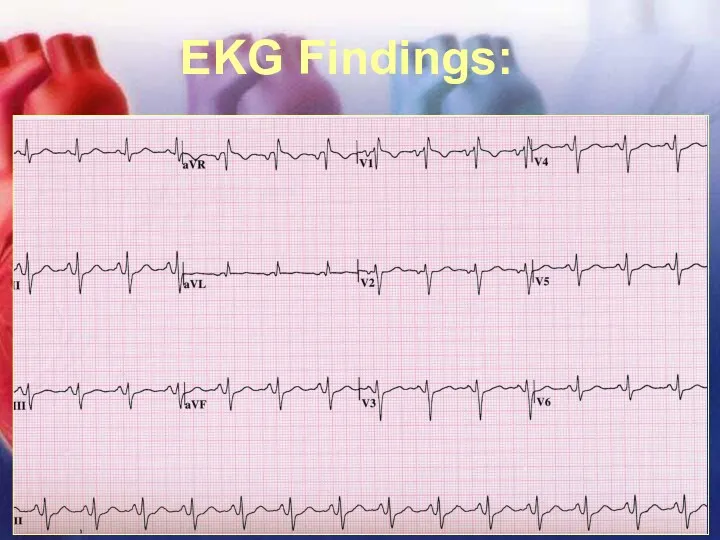
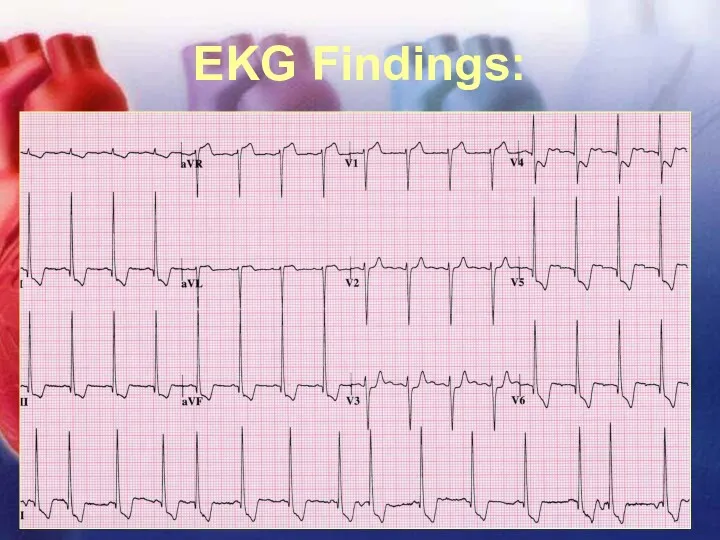
- 16. 11/12/02 Lubna Piracha, D.O. EKG Findings:
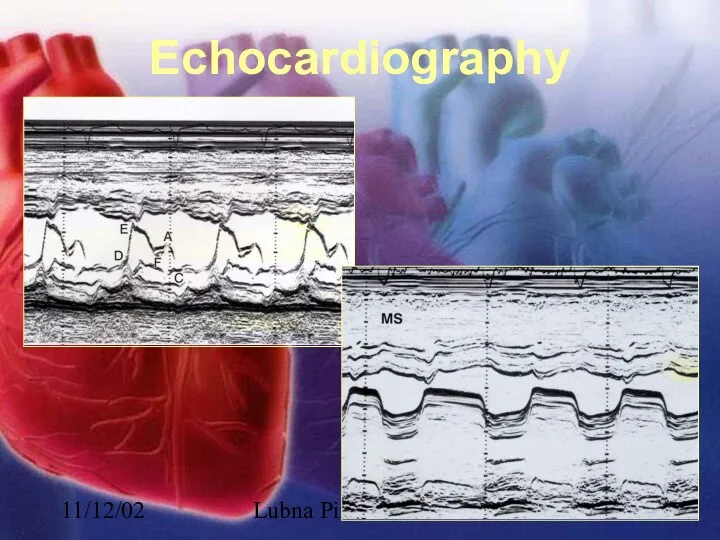
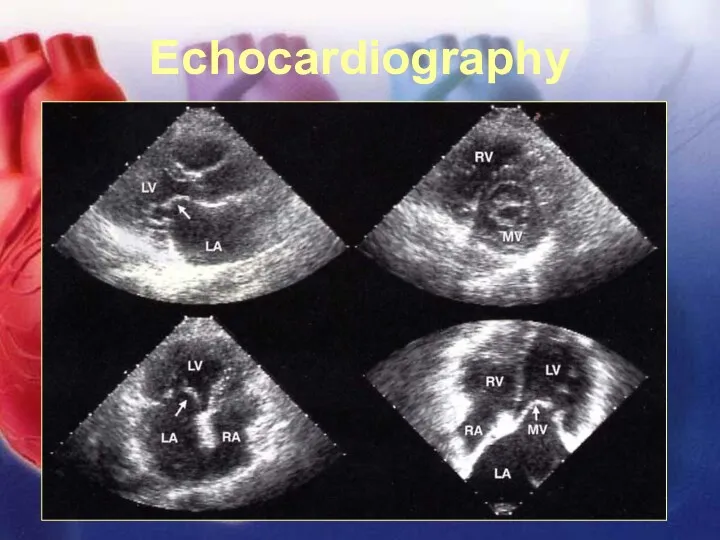
- 17. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 18. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 19. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 20. 11/12/02 Lubna Piracha, D.O. Mitral Stenosis In severe mitral stenosis the left ventricle is spared and
- 21. 11/12/02 Lubna Piracha, D.O. Case Studies: A 52 year old female presents with complaints of slowly
- 22. 11/12/02 Lubna Piracha, D.O. Physical Exam Review Early diastolic murmur of regurgitation blowing, and high frequency,
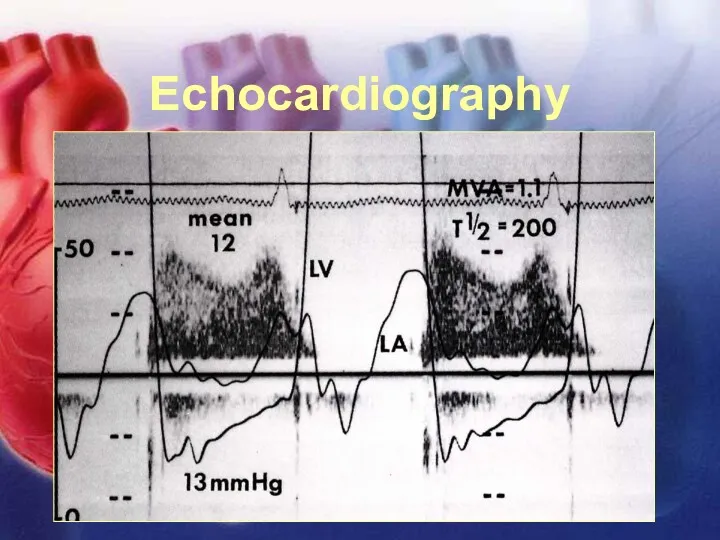
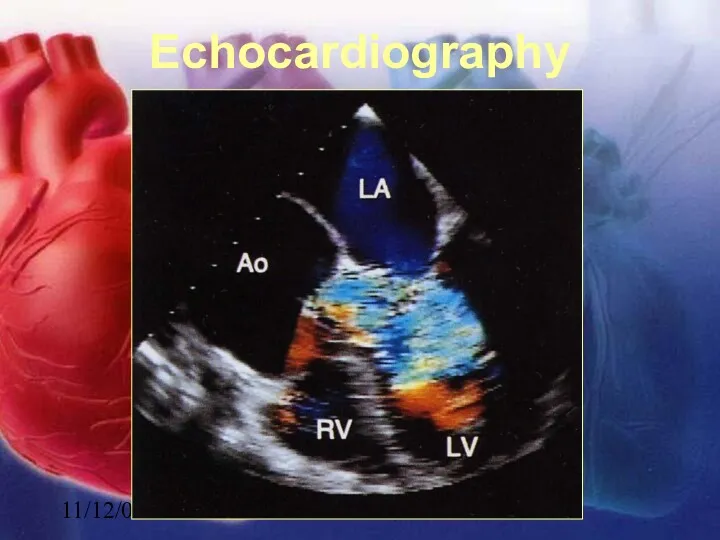
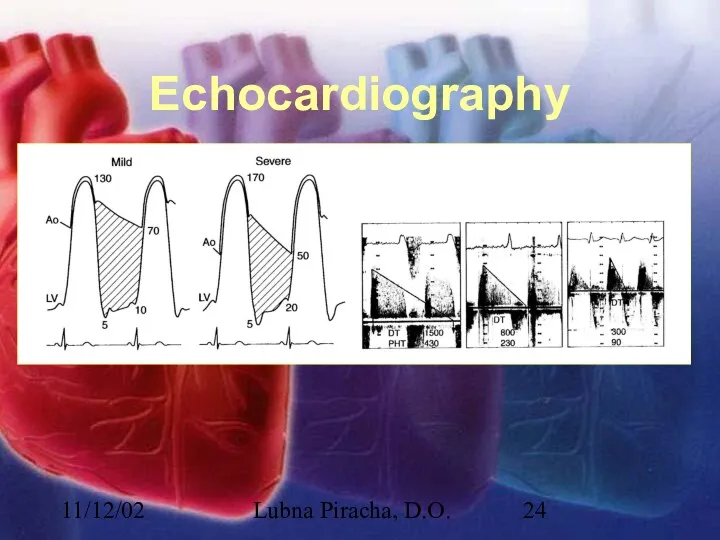
- 23. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 24. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 25. 11/12/02 Lubna Piracha, D.O. Aortic Insufficiency Acute aortic insufficiency usually due to acute aortic dissection or
- 26. 11/12/02 Lubna Piracha, D.O. Aortic Insufficiency In chronic aortic insufficiency, compensatory left ventricular changes occur over
- 27. 11/12/02 Lubna Piracha, D.O. Case Study A 75 year old male present to the emergency room
- 28. 11/12/02 Lubna Piracha, D.O. Physical Exam Review In acute MR, there is tachycardia, the murmur maybe
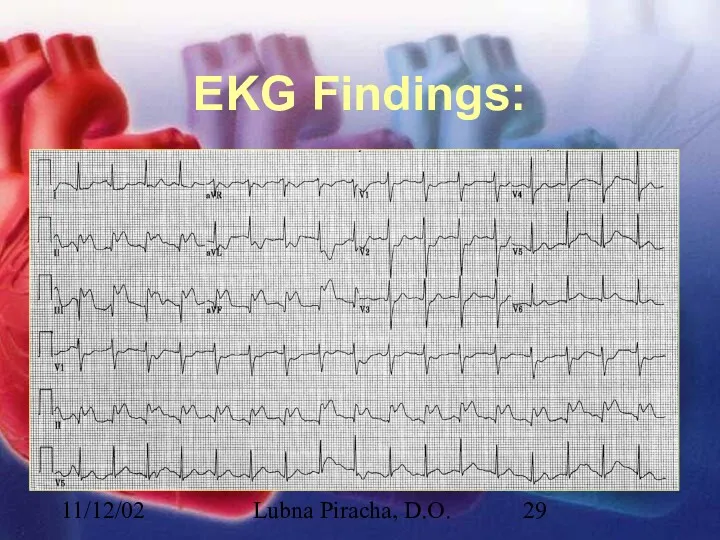
- 29. 11/12/02 Lubna Piracha, D.O. EKG Findings:
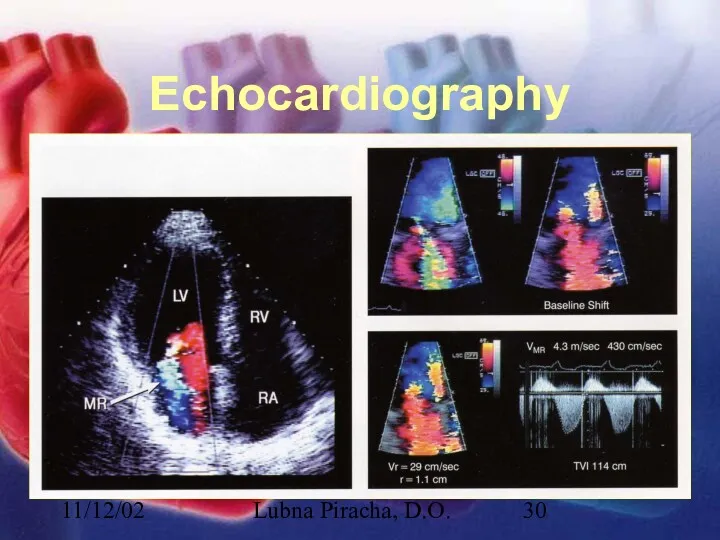
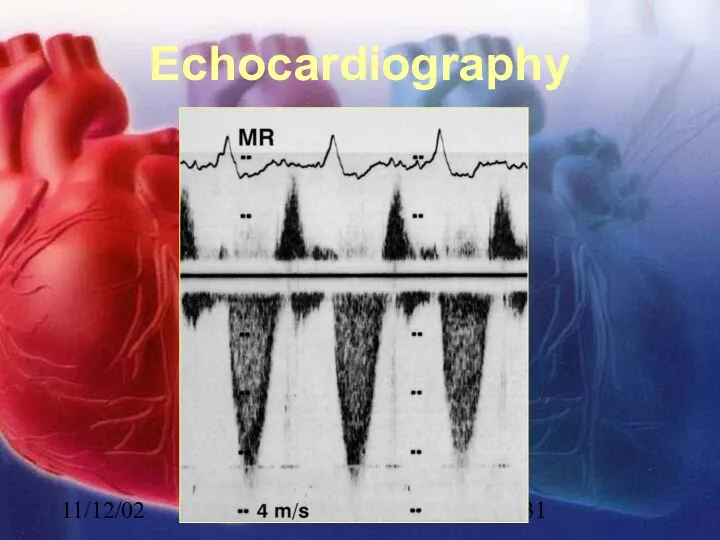
- 30. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 31. 11/12/02 Lubna Piracha, D.O. Echocardiography
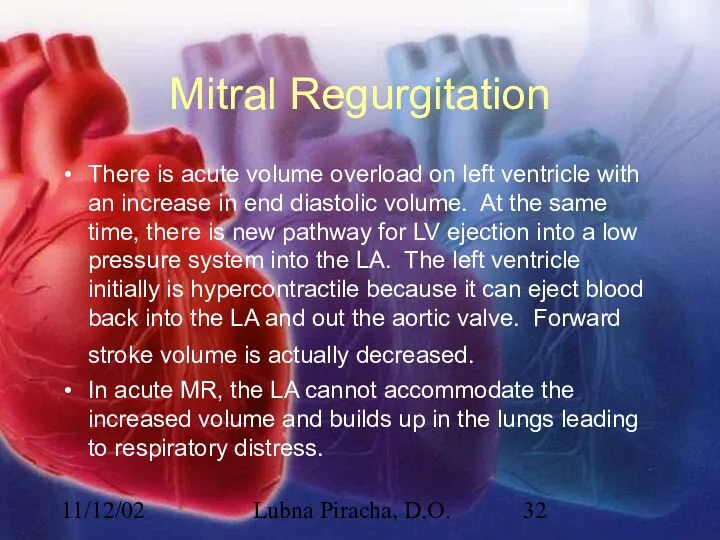
- 32. 11/12/02 Lubna Piracha, D.O. Mitral Regurgitation There is acute volume overload on left ventricle with an
- 33. 11/12/02 Lubna Piracha, D.O. Mitral Regurgitation In chronic MR, the LA will slowly dilate, the LV
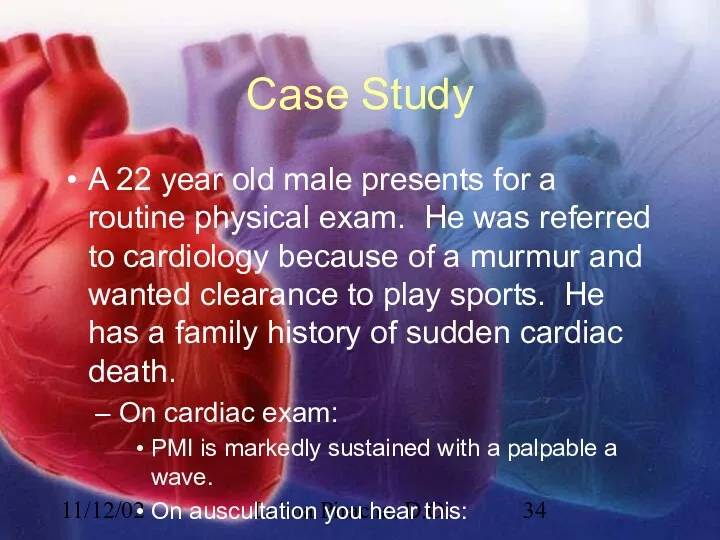
- 34. 11/12/02 Lubna Piracha, D.O. Case Study A 22 year old male presents for a routine physical
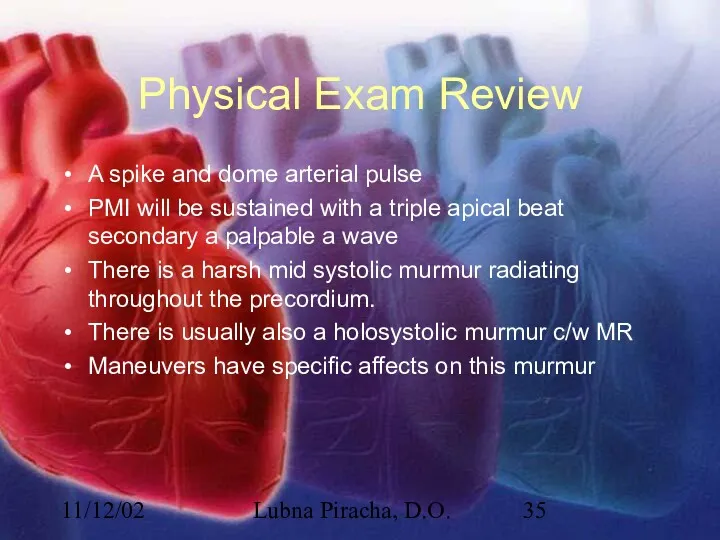
- 35. 11/12/02 Lubna Piracha, D.O. Physical Exam Review A spike and dome arterial pulse PMI will be
- 36. 11/12/02 Lubna Piracha, D.O. EKG Findings:
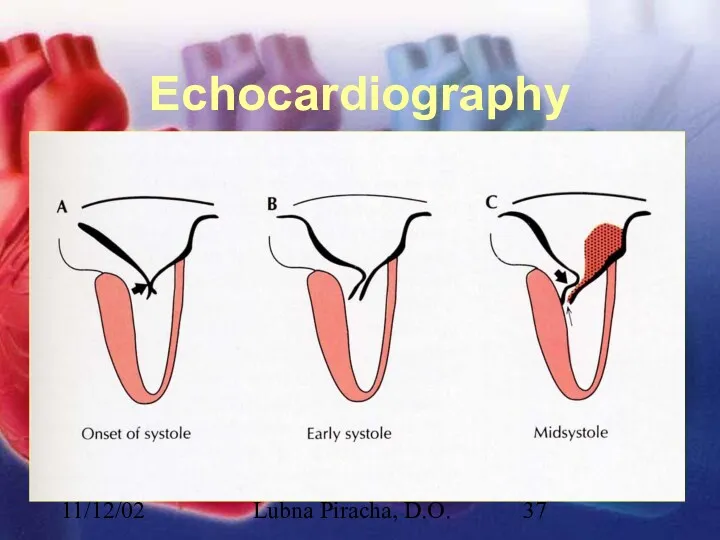
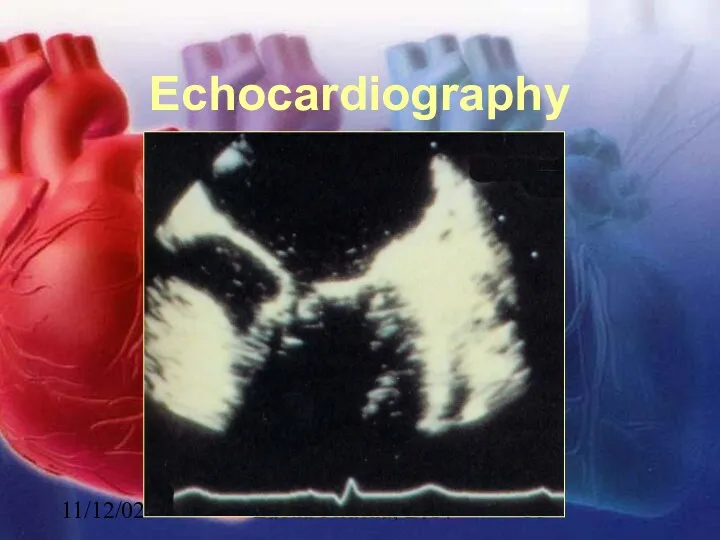
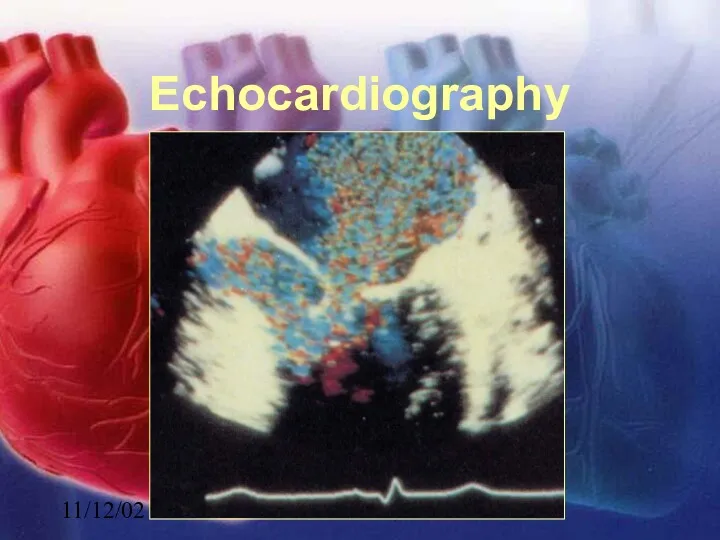
- 37. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 38. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 39. 11/12/02 Lubna Piracha, D.O. Echocardiography
- 40. 11/12/02 Lubna Piracha, D.O. Hypertrophic Cardiomyopathy HCM is frequently a hereditary disorder, with transmission to first-degree
- 42. Скачать презентацию
11/12/02
Lubna Piracha, D.O.
What is a Murmur?
It maybe a normal or abnormal
11/12/02
Lubna Piracha, D.O.
What is a Murmur?
It maybe a normal or abnormal
11/12/02
Lubna Piracha, D.O.
Timing and Location
Timing:
Systolic
Diastolic
Continuous
Location:
RUSB
LUSB
LLSB
apex
11/12/02
Lubna Piracha, D.O.
Timing and Location
Timing:
Systolic
Diastolic
Continuous
Location:
RUSB
LUSB
LLSB
apex
11/12/02
Lubna Piracha, D.O.
Intensity and Frequency
High Frequency
MR
TR
AR
Low Frequency
MS
TS
Intensity
Grade 1
Grade 2
Grade 3
Grade
11/12/02
Lubna Piracha, D.O.
Intensity and Frequency
High Frequency
MR
TR
AR
Low Frequency
MS
TS
Intensity
Grade 1
Grade 2
Grade 3
Grade
11/12/02
Lubna Piracha, D.O.
Maneuvers
11/12/02
Lubna Piracha, D.O.
Maneuvers
11/12/02
Lubna Piracha, D.O.
Maneuvers
11/12/02
Lubna Piracha, D.O.
Maneuvers
11/12/02
Lubna Piracha, D.O.
Case Studies
A 50 year old male with a known
11/12/02
Lubna Piracha, D.O.
Case Studies
A 50 year old male with a known
11/12/02
Lubna Piracha, D.O.
Physical Exam in AS
11/12/02
Lubna Piracha, D.O.
Physical Exam in AS
11/12/02
Lubna Piracha, D.O.
EKG shows
11/12/02
Lubna Piracha, D.O.
EKG shows
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Aortic Stenosis
11/12/02
Lubna Piracha, D.O.
Aortic Stenosis
11/12/02
Lubna Piracha, D.O.
Aortic Stenosis
There is little hemodynamic disturbance that occurs as
11/12/02
Lubna Piracha, D.O.
Aortic Stenosis
There is little hemodynamic disturbance that occurs as
11/12/02
Lubna Piracha, D.O.
Aortic Stenosis continued:
Concentric hypertrophy develops in response to this
11/12/02
Lubna Piracha, D.O.
Aortic Stenosis continued:
Concentric hypertrophy develops in response to this
11/12/02
Lubna Piracha, D.O.
Case Study:
A 45 year old male with a history
11/12/02
Lubna Piracha, D.O.
Case Study:
A 45 year old male with a history
11/12/02
Lubna Piracha, D.O.
Physical Exam Review:
11/12/02
Lubna Piracha, D.O.
Physical Exam Review:
11/12/02
Lubna Piracha, D.O.
EKG Findings:
11/12/02
Lubna Piracha, D.O.
EKG Findings:
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Mitral Stenosis
In severe mitral stenosis the left ventricle
11/12/02
Lubna Piracha, D.O.
Mitral Stenosis
In severe mitral stenosis the left ventricle

11/12/02
Lubna Piracha, D.O.
Case Studies:
A 52 year old female presents with complaints
11/12/02
Lubna Piracha, D.O.
Case Studies:
A 52 year old female presents with complaints
11/12/02
Lubna Piracha, D.O.
Physical Exam Review
Early diastolic murmur of regurgitation
blowing, and high
11/12/02
Lubna Piracha, D.O.
Physical Exam Review
Early diastolic murmur of regurgitation
blowing, and high
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Aortic Insufficiency
Acute aortic insufficiency usually due to acute aortic
11/12/02
Lubna Piracha, D.O.
Aortic Insufficiency
Acute aortic insufficiency usually due to acute aortic
11/12/02
Lubna Piracha, D.O.
Aortic Insufficiency
In chronic aortic insufficiency, compensatory left ventricular changes
11/12/02
Lubna Piracha, D.O.
Aortic Insufficiency
In chronic aortic insufficiency, compensatory left ventricular changes
11/12/02
Lubna Piracha, D.O.
Case Study
A 75 year old male present to the
11/12/02
Lubna Piracha, D.O.
Case Study
A 75 year old male present to the
11/12/02
Lubna Piracha, D.O.
Physical Exam Review
In acute MR, there is tachycardia, the
11/12/02
Lubna Piracha, D.O.
Physical Exam Review
In acute MR, there is tachycardia, the
11/12/02
Lubna Piracha, D.O.
EKG Findings:
11/12/02
Lubna Piracha, D.O.
EKG Findings:
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Mitral Regurgitation
There is acute volume overload on left ventricle
11/12/02
Lubna Piracha, D.O.
Mitral Regurgitation
There is acute volume overload on left ventricle

11/12/02
Lubna Piracha, D.O.
Mitral Regurgitation
In chronic MR, the LA will slowly dilate,
11/12/02
Lubna Piracha, D.O.
Mitral Regurgitation
In chronic MR, the LA will slowly dilate,
11/12/02
Lubna Piracha, D.O.
Case Study
A 22 year old male presents for a
11/12/02
Lubna Piracha, D.O.
Case Study
A 22 year old male presents for a
11/12/02
Lubna Piracha, D.O.
Physical Exam Review
A spike and dome arterial pulse
PMI will
11/12/02
Lubna Piracha, D.O.
Physical Exam Review
A spike and dome arterial pulse
PMI will
11/12/02
Lubna Piracha, D.O.
EKG Findings:
11/12/02
Lubna Piracha, D.O.
EKG Findings:
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Echocardiography
11/12/02
Lubna Piracha, D.O.
Hypertrophic Cardiomyopathy
HCM is frequently a hereditary disorder, with transmission
11/12/02
Lubna Piracha, D.O.
Hypertrophic Cardiomyopathy
HCM is frequently a hereditary disorder, with transmission
 Пульмонологиядагы микробиологиялық зерттеу әдістері
Пульмонологиядагы микробиологиялық зерттеу әдістері Средства наружной терапии в дерматологии
Средства наружной терапии в дерматологии Методика проведения массажа и обертывания с водорослями в боди - коррекция в области бедер и ягодиц
Методика проведения массажа и обертывания с водорослями в боди - коррекция в области бедер и ягодиц Эндокринная система. Механизм действия гидрофильных гормонов
Эндокринная система. Механизм действия гидрофильных гормонов История развития сестринского дела в России
История развития сестринского дела в России Воспаление. Факторы, вызывающие воспаление
Воспаление. Факторы, вызывающие воспаление Микроспория (микроспороз, стригущий лишай)
Микроспория (микроспороз, стригущий лишай) Здоровый образ жизни
Здоровый образ жизни Материалы для обтурации корневых каналов
Материалы для обтурации корневых каналов Ведение в токсикологию. Основные закономерности взаимодействия организма и химических веществ
Ведение в токсикологию. Основные закономерности взаимодействия организма и химических веществ Ешерихії, сальмонели та їх класифікація
Ешерихії, сальмонели та їх класифікація Медико–педагогическая реабилитация детей с врожденными расщелинами верхней губы и неба
Медико–педагогическая реабилитация детей с врожденными расщелинами верхней губы и неба Сестринское дело в системе первичной медико-санитарной помощи населению
Сестринское дело в системе первичной медико-санитарной помощи населению Ламбдацизм и методы его исправления
Ламбдацизм и методы его исправления Лечение кишечных инфекций. Сальмонеллёз
Лечение кишечных инфекций. Сальмонеллёз Генерализованный листериоз у новорожденного. Случай из практики
Генерализованный листериоз у новорожденного. Случай из практики День донора
День донора Интеграция в психотерапии. Использование уникальных условий океанской среды для лечения расстройств
Интеграция в психотерапии. Использование уникальных условий океанской среды для лечения расстройств Пиодермии
Пиодермии Бронхиальная астма – глобальная проблема
Бронхиальная астма – глобальная проблема Стрептомицин. Фармакотерапиялық тобы
Стрептомицин. Фармакотерапиялық тобы Заболевания прямой кишки
Заболевания прямой кишки Методы иммунодиагностики и иммунопрофилактики инфекционных болезней
Методы иммунодиагностики и иммунопрофилактики инфекционных болезней Cовременные синтетические материалы в хирургии и травматологии
Cовременные синтетические материалы в хирургии и травматологии Перинаталді медицинаның қазіргі мәселелері
Перинаталді медицинаның қазіргі мәселелері ЭКГ қалыпты жағдайдағы
ЭКГ қалыпты жағдайдағы Жедел іш синдромы кезіндегі диагностика және жедел көмек көрсету алгоритмі
Жедел іш синдромы кезіндегі диагностика және жедел көмек көрсету алгоритмі Мозжечок, синдромы поражения. Экстрапирамидная система, синдромы поражения
Мозжечок, синдромы поражения. Экстрапирамидная система, синдромы поражения