- Neonatal resuscitation fatma aletebi

Содержание
- 2. Asphyxia - The Basics Apnea The asphyxiated infant passes through a series of events: rapid breathing
- 3. Clearing Fetal Lung Fluid The first few breaths of a normal infant are usually adequate to
- 4. Pulmonary Circulation At birth, pulmonary blood flow increases rapidly as the lung arterioles open up and
- 5. Systemic Circulation and Cardiac Function Early in asphyxia, vasoconstriction in the gut, kidneys, muscles and skin
- 6. Preparation for Delivery Anticipate Need for Resuscitation Antepartum and intrapartum history may help to alert delivery-room
- 7. Antepartum Factors Age > 35 years Maternal diabetes Pregnancy-induced hypertension Chronic hypertension Other maternal illness (e.g.
- 8. Intrapartum Factors Abnormal presentation Operative delivery Premature labour Premature rupture of membranes Precipitous labour Prolonged labour
- 9. Personnel At every delivery, at least one individual should be capable of performing a complete resuscitation
- 10. When neonatal asphyxia is anticipated, two individuals whose sole responsibility is to the infant, should be
- 11. Equipment Equipment and medications should be checked as a daily routine and then prior to anticipated
- 12. Resuscitation Equipment in the Delivery Room Radiant Heater Stethoscope ECG monitor Wall oxygen with flowmeter and
- 13. Initial Stabilization Prevent Heat Loss Place the infant under an overhead radiant heater to minimize radiant
- 14. Open the Airway Position the infant supine or on his or her side with the neck
- 15. Tactile Stimulation If drying and suctioning do not induce effective breathing, additional safe methods include: slapping
- 16. Evaluate the Infant Respirations: Infants who are apneic or gasping despite brief stimulation attempts should receive
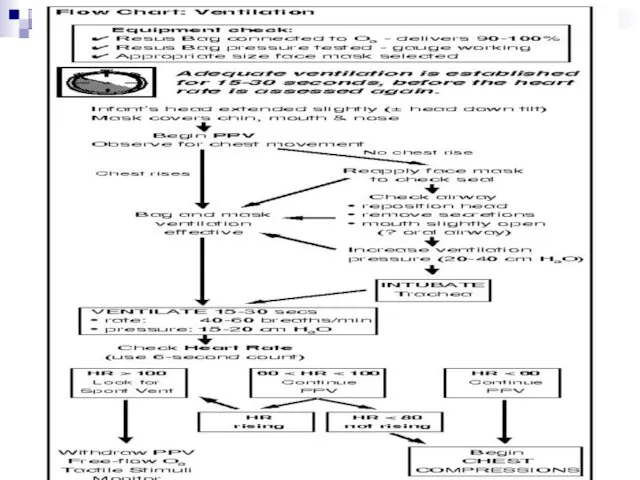
- 18. Ventilating Procedure When ventilatory support is required, most neonates can be adequately ventilated with a bag
- 19. Adequate ventilation is assessed by observing chest wall motion and hearing breath sounds bilaterally. If chest
- 20. After 15-30 seconds of effective ventilation, the heart rate of the neonate should be evaluated. To
- 21. The next step in the resuscitation depends on the heart rate which is determined HR >
- 23. Chest Compressions Rationale Asphyxia in the neonate not only slows the heart rate but also decreases
- 24. Indications When to Begin Chest Compressions: After 15-30 seconds of PPV with 100% O2 - the
- 25. Technique Location: Pressure should be applied to the middle third of sternum, just below an imaginary
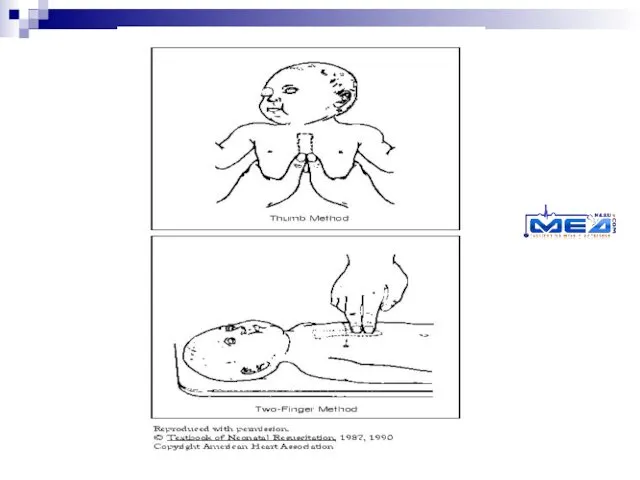
- 26. Thumb Method: Encircle the torso with both hands and compress the sternum with both thumbs side-by-side
- 28. Evaluating the Heart Rate After the first 30 seconds of chest compressions, the heart rate should
- 29. Endotracheal Intubation Indications In most cases, when positive-pressure ventilation is required, it should be initiated with
- 30. Other Equipment Laryngoscope: Attach to the handle the appropriate size straight (Miller) blade: No. 0 for
- 31. Confirmation of ET Tube Placement If the ET tube is correctly placed in the mid-tracheal region,
- 32. Complications of Intubation HypoxiaTaking too long to intubate Incorrect placement of tube Bradycardia/ApneaHypoxia Vagal response due
- 33. Tracheal Suction for Meconium Aspiration About one in eight deliveries are complicated by the presence of
- 34. If meconium is present in an infant with respiratory difficulties, then immediately after delivery the posterior
- 35. Drugs and Fluids For the majority of infants who require resuscitation, the only "medication" needed will
- 36. Epinephrine: Indications: - the heart rate stays below 80 despite effective ventilation with 100% oxygen and
- 37. Volume Expanders: Indications: Signs of hypovolemia. A 20% or greater loss in blood volume should be
- 38. Naloxone: Indications: Naloxone is indicated in the infant for reversal of respiratory depression secondary to maternal
- 39. Reserved for prolonged resuscitations only Sodium Bicarbonate (0.5 mEq�ml-1 = 4.2% soln) 2 mEq � kg-1
- 40. Postresuscitation Care Newborns who have been successfully resuscitated will require close monitoring in a neonatal intensive
- 42. Скачать презентацию
Asphyxia - The Basics
Apnea
The asphyxiated infant passes through a series of
Asphyxia - The Basics
Apnea
The asphyxiated infant passes through a series of
Clearing Fetal Lung Fluid
The first few breaths of a normal infant
Clearing Fetal Lung Fluid
The first few breaths of a normal infant
Pulmonary Circulation
At birth, pulmonary blood flow increases rapidly as the lung
Pulmonary Circulation
At birth, pulmonary blood flow increases rapidly as the lung
Systemic Circulation and Cardiac Function
Early in asphyxia, vasoconstriction in the gut,
Systemic Circulation and Cardiac Function
Early in asphyxia, vasoconstriction in the gut,
Preparation for Delivery
Anticipate Need for Resuscitation
Antepartum and intrapartum history may help
Preparation for Delivery
Anticipate Need for Resuscitation
Antepartum and intrapartum history may help
Antepartum Factors
Age > 35 years
Maternal diabetes
Pregnancy-induced hypertension
Chronic hypertension
Other maternal illness
(e.g.
Antepartum Factors
Age > 35 years Maternal diabetes Pregnancy-induced hypertension Chronic hypertension Other maternal illness (e.g.
Intrapartum Factors
Abnormal presentation
Operative delivery
Premature labour
Premature rupture of membranes
Precipitous labour
Prolonged labour
Indices
Intrapartum Factors
Abnormal presentation Operative delivery Premature labour Premature rupture of membranes Precipitous labour Prolonged labour Indices
Personnel
At every delivery, at least one individual should be capable of
Personnel
At every delivery, at least one individual should be capable of
When neonatal asphyxia is anticipated, two individuals whose sole responsibility is
When neonatal asphyxia is anticipated, two individuals whose sole responsibility is
Equipment
Equipment and medications should be checked as a daily routine and
Equipment
Equipment and medications should be checked as a daily routine and
Resuscitation Equipment in the Delivery Room
Radiant Heater
Stethoscope
ECG monitor
Wall oxygen with flowmeter
Resuscitation Equipment in the Delivery Room
Radiant Heater
Stethoscope
ECG monitor
Wall oxygen with flowmeter
Initial Stabilization
Prevent Heat Loss
Place the infant under an overhead radiant heater
Initial Stabilization
Prevent Heat Loss
Place the infant under an overhead radiant heater
Open the Airway
Position the infant supine or on his or her
Open the Airway
Position the infant supine or on his or her
Tactile Stimulation
If drying and suctioning do not induce effective breathing, additional
Tactile Stimulation
If drying and suctioning do not induce effective breathing, additional
Evaluate the Infant
Respirations: Infants who are apneic or gasping despite brief
Evaluate the Infant
Respirations: Infants who are apneic or gasping despite brief
Ventilating Procedure
When ventilatory support is required, most neonates can be adequately
Ventilating Procedure
When ventilatory support is required, most neonates can be adequately
Adequate ventilation is assessed by observing chest wall motion and hearing
Adequate ventilation is assessed by observing chest wall motion and hearing
After 15-30 seconds of effective ventilation, the heart rate of the
After 15-30 seconds of effective ventilation, the heart rate of the
The next step in the resuscitation depends on the heart rate
The next step in the resuscitation depends on the heart rate
Chest Compressions
Rationale
Asphyxia in the neonate not only slows the heart rate
Chest Compressions
Rationale
Asphyxia in the neonate not only slows the heart rate
Indications
When to Begin Chest Compressions:
After 15-30 seconds of PPV with
Indications
When to Begin Chest Compressions:
After 15-30 seconds of PPV with
Technique
Location: Pressure should be applied to the middle third of sternum,
Technique
Location: Pressure should be applied to the middle third of sternum,
Thumb Method: Encircle the torso with both hands and compress the
Thumb Method: Encircle the torso with both hands and compress the
Evaluating the Heart Rate
After the first 30 seconds of chest compressions,
Evaluating the Heart Rate
After the first 30 seconds of chest compressions,
Endotracheal Intubation
Indications
In most cases, when positive-pressure ventilation is required, it should
Endotracheal Intubation
Indications
In most cases, when positive-pressure ventilation is required, it should
Other Equipment
Laryngoscope: Attach to the handle the appropriate size straight (Miller)
Other Equipment
Laryngoscope: Attach to the handle the appropriate size straight (Miller)
Confirmation of ET Tube Placement
If the ET tube is correctly placed
Confirmation of ET Tube Placement
If the ET tube is correctly placed
Complications of Intubation
HypoxiaTaking too long to intubate Incorrect placement of tube
Complications of Intubation
HypoxiaTaking too long to intubate Incorrect placement of tube
Tracheal Suction for Meconium Aspiration
About one in eight deliveries are complicated
Tracheal Suction for Meconium Aspiration
About one in eight deliveries are complicated
If meconium is present in an infant with respiratory difficulties, then
If meconium is present in an infant with respiratory difficulties, then
Drugs and Fluids
For the majority of infants who require resuscitation, the
Drugs and Fluids
For the majority of infants who require resuscitation, the
Epinephrine:
Indications:
- the heart rate stays below 80 despite effective
Epinephrine:
Indications:
- the heart rate stays below 80 despite effective
Volume Expanders:
Indications:
Signs of hypovolemia. A 20% or greater loss
Volume Expanders:
Indications:
Signs of hypovolemia. A 20% or greater loss
Naloxone:
Indications:
Naloxone is indicated in the infant for reversal of
Naloxone:
Indications:
Naloxone is indicated in the infant for reversal of
Reserved for prolonged resuscitations only
Sodium Bicarbonate
(0.5 mEq�ml-1 = 4.2% soln)
2 mEq
Reserved for prolonged resuscitations only
Sodium Bicarbonate
(0.5 mEq�ml-1 = 4.2% soln)
2 mEq
Postresuscitation Care
Newborns who have been successfully resuscitated will require close monitoring
Postresuscitation Care
Newborns who have been successfully resuscitated will require close monitoring
 Физиология дыхания
Физиология дыхания Кожное заболевание чесотка
Кожное заболевание чесотка Воспалительные заболевания слуховой трубы
Воспалительные заболевания слуховой трубы История болезни
История болезни Антибиотики. Определение
Антибиотики. Определение Теоретическая основа здравоохранения и фармации
Теоретическая основа здравоохранения и фармации Эндокринология. Общая эндокринология. Частная эндокринология
Эндокринология. Общая эндокринология. Частная эндокринология Умирание, смерть и трупные изменения
Умирание, смерть и трупные изменения Перекрестный прикус
Перекрестный прикус Шок – собирательный термин, обозначающий критическое состояние
Шок – собирательный термин, обозначающий критическое состояние Профилактика ранней беременности
Профилактика ранней беременности Роль и место препаратов сульфонилмочевины в терапии сахарного диабета 2 типа
Роль и место препаратов сульфонилмочевины в терапии сахарного диабета 2 типа Общая реакция организма на повреждение
Общая реакция организма на повреждение Общие вопросы стоматологии. Организация работы врача - стоматолога-терапевта
Общие вопросы стоматологии. Организация работы врача - стоматолога-терапевта Канцерогены, как факторы опухолевого роста
Канцерогены, как факторы опухолевого роста Алергія. Типи алергічних реакцій
Алергія. Типи алергічних реакцій Психопатология, психопатия и акцентуация характера
Психопатология, психопатия и акцентуация характера Кешенді медициналық ақпараттық жүйе (КМИС)
Кешенді медициналық ақпараттық жүйе (КМИС) Сахарный диабет первого типа. Определение, распространение, социальное значение. Клиника, диагностика, лечение
Сахарный диабет первого типа. Определение, распространение, социальное значение. Клиника, диагностика, лечение Пародонттың қызметі және
Пародонттың қызметі және Бронхиальная астма, сердечная астма, астма при уремии
Бронхиальная астма, сердечная астма, астма при уремии Сит задачи по ОЖ экзаменац
Сит задачи по ОЖ экзаменац Одонтогенные верхнечелюстные синуситы
Одонтогенные верхнечелюстные синуситы Показания к оперативному лечению. Методы предоперационного обследования
Показания к оперативному лечению. Методы предоперационного обследования Острый коронарный синдром: инфаркт миокарда без подъема ST
Острый коронарный синдром: инфаркт миокарда без подъема ST Острые лейкозы
Острые лейкозы ВИЧ/СПИД
ВИЧ/СПИД Фармакология кардиотонических препаратов
Фармакология кардиотонических препаратов