- Neuroendocrine tumors overview of treatment

Содержание
- 2. NET Neuroendocrine tumors (NETs), sometimes referred to as carcinoids, are abnormal growths that begin in the
- 3. NETs = Carcinoid tumours - heterogeneous group of tumours arising from distinct neuroendocrine cells located throughout
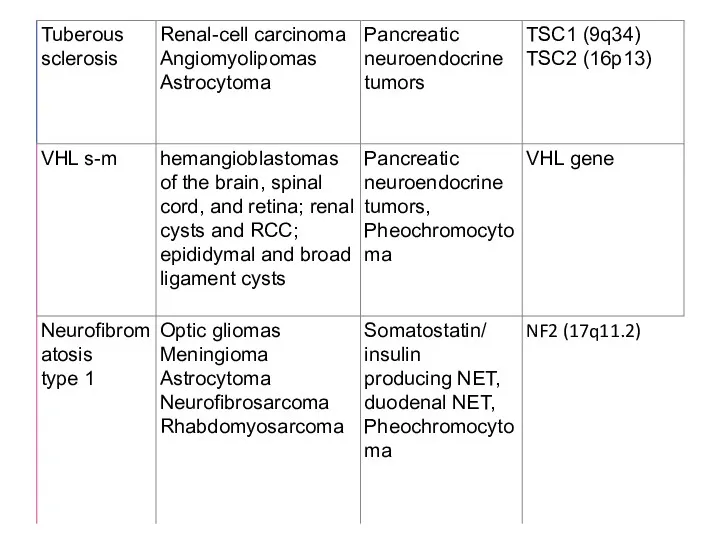
- 4. NETs: An Overview Tumours may be sporadic or hereditary (rare) When hereditary, they may be associated
- 6. Mucosal neuroma
- 8. Increase in NET Incidence Compared with All Malignant Neoplasms* NETs, neuroendocrine tumors; SEER, Surveillance, Epidemiology, and
- 9. GEP-NETs: Rare But Increasing, particularly for small intestine and rectal tumors Small intestine and pancreatic tumors
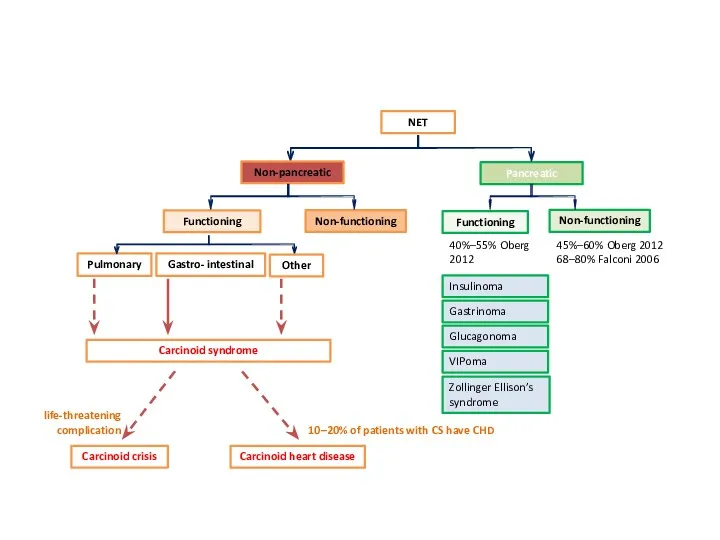
- 10. NET Pancreatic Non-pancreatic Functioning Non-functioning Functioning Non-functioning 40%–55% Oberg 2012 45%–60% Oberg 2012 68–80% Falconi 2006
- 11. Classification by embryonic origin
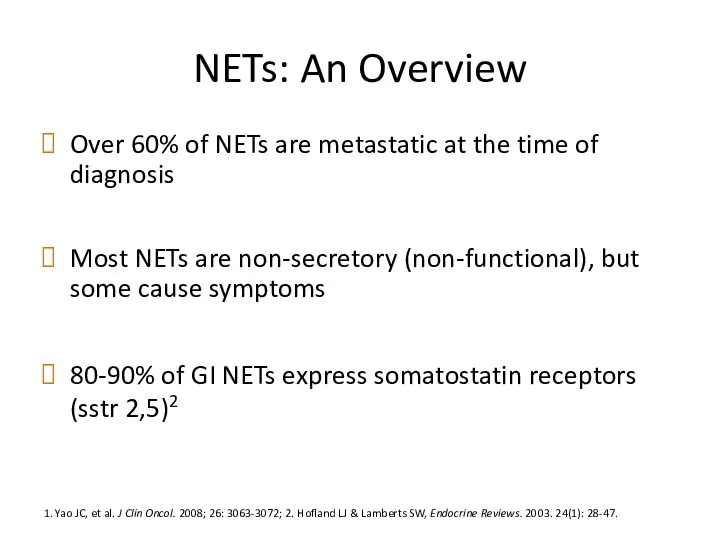
- 12. NETs: An Overview Over 60% of NETs are metastatic at the time of diagnosis Most NETs
- 13. Median Survival for Patients with Localised and Metastatic NET 1Yao J, et al. J Clin Oncol.
- 14. Observed 5-Year Survival for GEP-NET Primary Sites* Source: US SEER database. Lawrence et al. Endocrinol Metab
- 15. How Well Do They Resemble Their Normal Cell Counterpart?1,2 The proliferative rate can be assessed by:
- 16. Correlation of Tumour Grade and Cumulative Survival Pape UF, et al. Cancer. 2008; 113: 256-265. 1
- 17. Clinical Presentation Adapted from Vinik A, et al. Pancreas. 2009; 38(8): 876-89. Nausea Weight loss /
- 18. Kарциноидный синдром 10% случаев опухоли Midgut (около 70%). при метастазах в печени не характерен для легочный
- 19. Kлиника приливы (90%), поносы (80%), боли в животе (40%), поражение клапанов сердца и Сердечная недостаточность (Carcinoid
- 20. Карциноидный криз Во время операции резкий выход серотонина в кровь Бронхообструкция, гипотензия, аритмии Профилактика: аналоги соматостатина
- 21. Диагностика CT MRI Radiolabeled somatostatin receptor scintigraphy DOTATATE (better) 5HIAA (5-Hydroxyindoleacetic acid - главный метаболит серотонина)
- 22. Карциноид Тимуса 2% - 7% DS при наличии передней медиастинальной массы Кушинг 25% ассоциированы с MEN1
- 23. Легочный карциноид 25% Typical (low grade) Atypical (intermediate grade) SCLC – KI67% > 30-40 Diffuse idiopathic
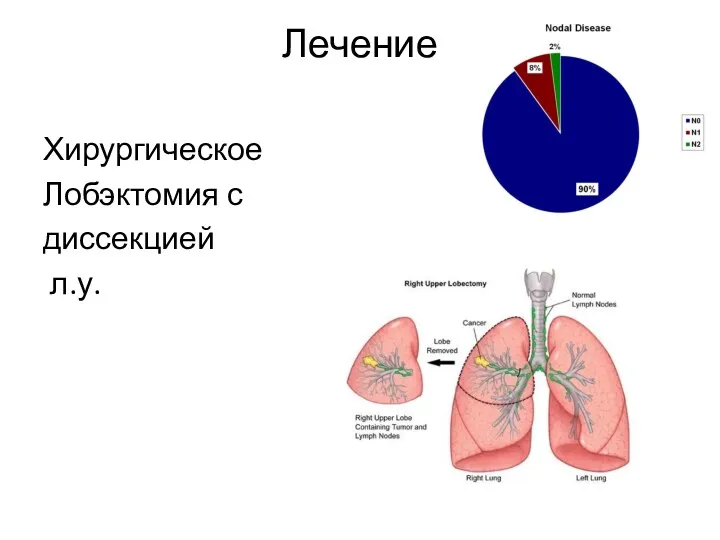
- 24. Лечение Хирургическое Лобэктомия с диссекцией л.у.
- 25. Kарциноид желудка
- 26. Лечение карциноидных опухолей желудка I тип - эндоскопическое иссечение одиночных опухолей - частичная резекция желудка при
- 27. Kарциноид кишечника лечение хирургическое Аппендикс - > 2 cm – RT hemicolectomy Rectum - > 2
- 28. Нейроэндокринные опухоли поджелудочной железы
- 29. Инсулиномы Cамые частые растет из бета клеток Только 5-10% злокачественные Основной симптом – гипогликемия, связан с
- 30. Гастриномы (синдром Золлингера – Эллисона) Bторое место среди эндокринных опухолей поджелудочной железы 70% - в двенадцатиперстной
- 31. Випомы (синдром Вернера – Моррисона) Cекреция вазоактивного интестинального пептида (VIP) MEN1 - 6% Метастазирование Поносы
- 32. Глюкагономы B α - клетках поджелудочной железы Глюкагон стимулирует распад гликогена, глюконеогенез, кетогенез, секрецию инсулина, липолиз,
- 33. Pancreatic polypeptidoma Относится к нефункционирующим опухолям ПЖЖ Как правило Дз в поздних стадиях Клиника обусловлена массой
- 34. Therapeutic Options NETs Surgery Curative, Ablative Debulking Radiofrequency ablation (RFA) Embolization/chemoembolization/radioembolization (SIRT) Debulking surgery? Irradiation External
- 35. Общие принципы лечения локальной болезни в зависимости от GRADE G1-2 – хирургическое G3 – химиотерапия (экстраполяция
- 37. Somatostatin Signalling in NETs More than 90% of NET express somatostatin receptors3-5
- 38. Somatostatin analogs
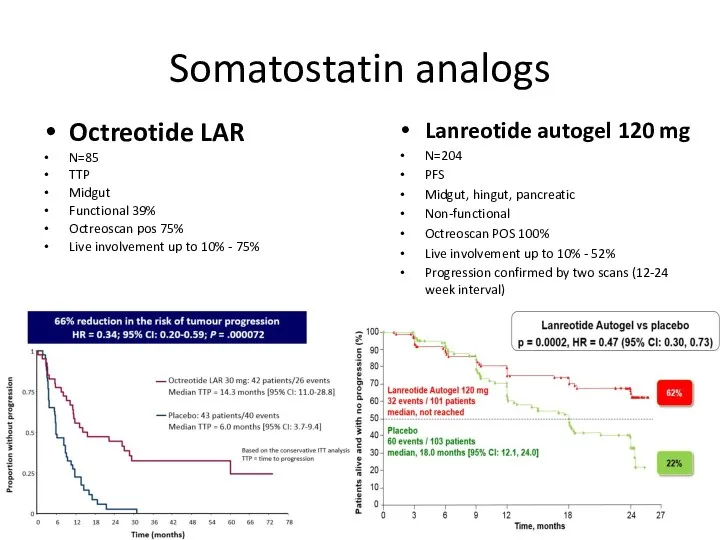
- 40. Somatostatin analogs Octreotide LAR N=85 TTP Midgut Functional 39% Octreoscan pos 75% Live involvement up to
- 41. Tolerability of Somatostatin Analogues Shah T & Caplin ME, Best Pract Res Clin Gastroenterol. 2005; 19(4):
- 42. PASPORT Carcinoid (C2303) ClinicalTrials.gov Identifier:NCT00690430 Primary endpoint: Reduction in bowel movements and/or flushing episodes at 24
- 43. Trial was terminated early based on interim analysis demonstrating futility for primary end point Overall response
- 44. High doses of SSA
- 45. SSA refractory Carcinoid Syndrome TELESTAR Telotristat etiprate is a novel oral inhibitor of Tryptophan Two early-stage
- 46. Targeting the mTOR and Pathways in NETs Everolimus (m-TOR inhibitor) Sunitinib (Inhibition of PDGF + VEGF
- 47. The RADIANT Study Programme (RAD001 In Advanced Neuroendocrine Tumors) EVEROLIMUS
- 48. Sunitinib Phase III Trial: Raymond E, et al. N Engl J Med. 2011;364:501-513. Blumenthal GM, et
- 49. Everolimus vs Sunitinib GI & Lung NET A/E: stomatitis, pneumonitis, hypeglycemia (good for functional insulinoma) pNET
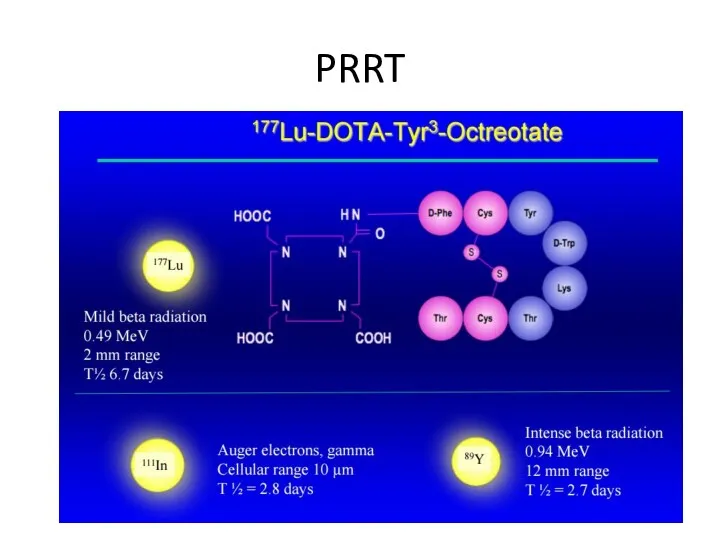
- 50. PRRT
- 51. PRRT
- 52. Studies showed efficacy in tumor shrinkage, symptoms relief, QOL and possible impact on survival However, there
- 53. Netter-1 trial Volume 376(2):125-135 January 12, 2017
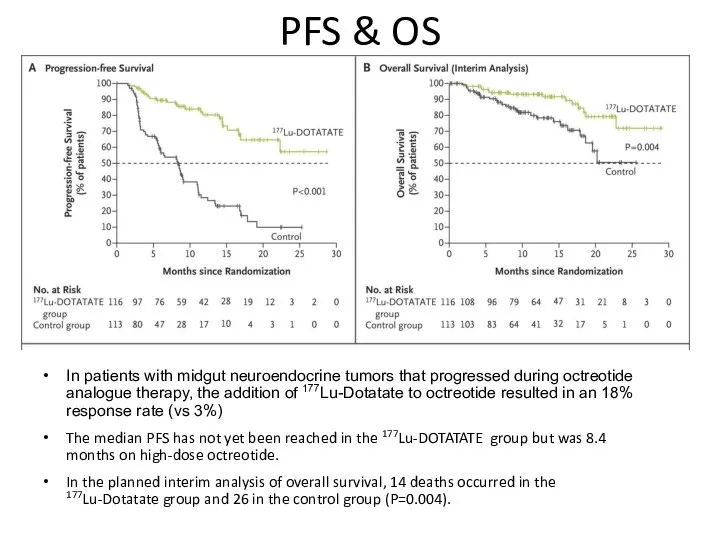
- 54. PFS & OS In patients with midgut neuroendocrine tumors that progressed during octreotide analogue therapy, the
- 55. Chemotherapy in NET Well-differentiated NET do not exhibit high sensitivity to chemotherapy because: of their low
- 56. Chemotherapy in NET (cont’d)
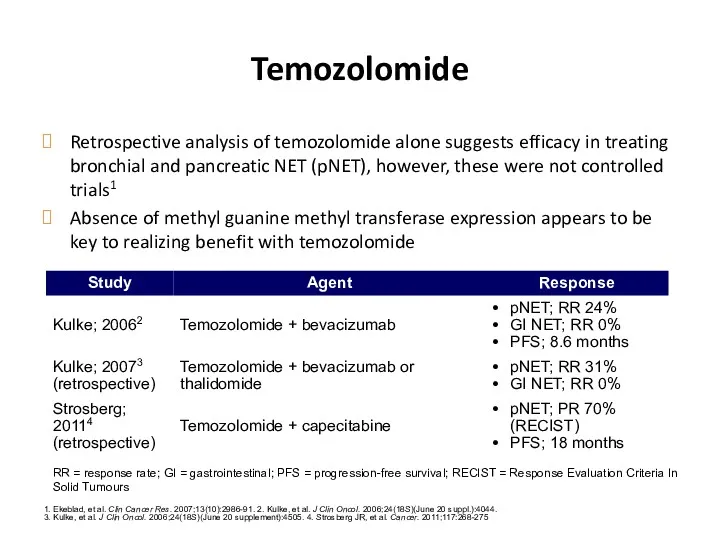
- 57. Temozolomide Retrospective analysis of temozolomide alone suggests efficacy in treating bronchial and pancreatic NET (pNET), however,
- 59. Скачать презентацию
NET
Neuroendocrine tumors (NETs), sometimes referred to as carcinoids, are abnormal growths
NET
Neuroendocrine tumors (NETs), sometimes referred to as carcinoids, are abnormal growths
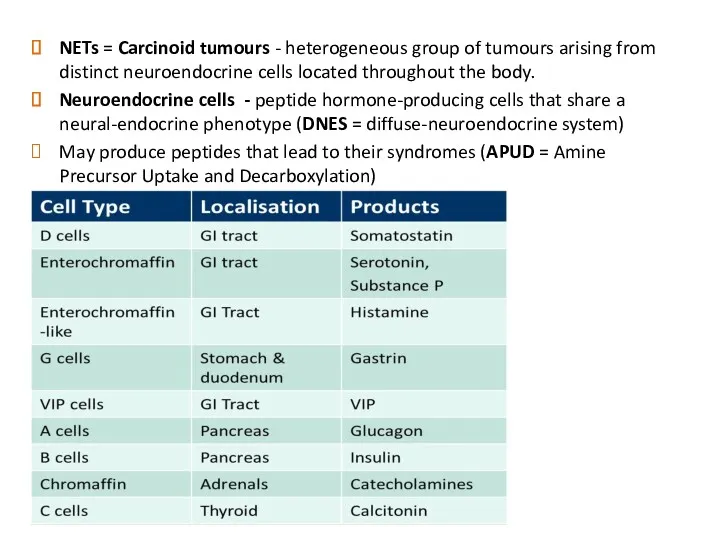
NETs = Carcinoid tumours - heterogeneous group of tumours arising from
NETs = Carcinoid tumours - heterogeneous group of tumours arising from
NETs: An Overview
Tumours may be sporadic or hereditary (rare)
When hereditary, they
NETs: An Overview
Tumours may be sporadic or hereditary (rare)
When hereditary, they
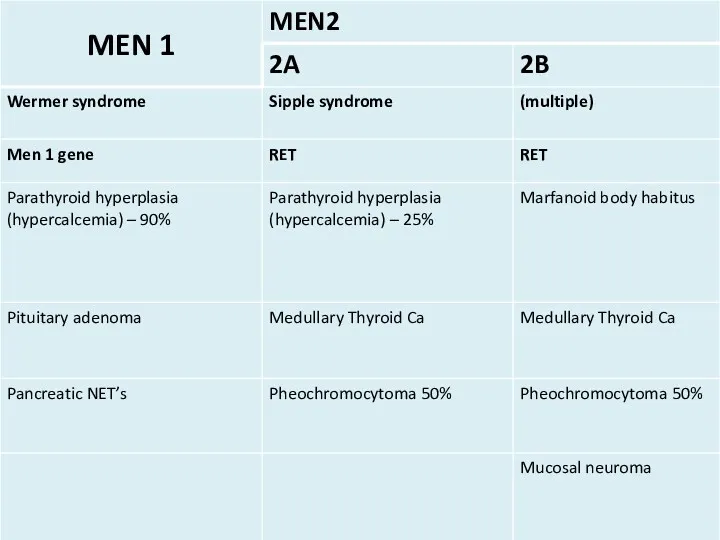
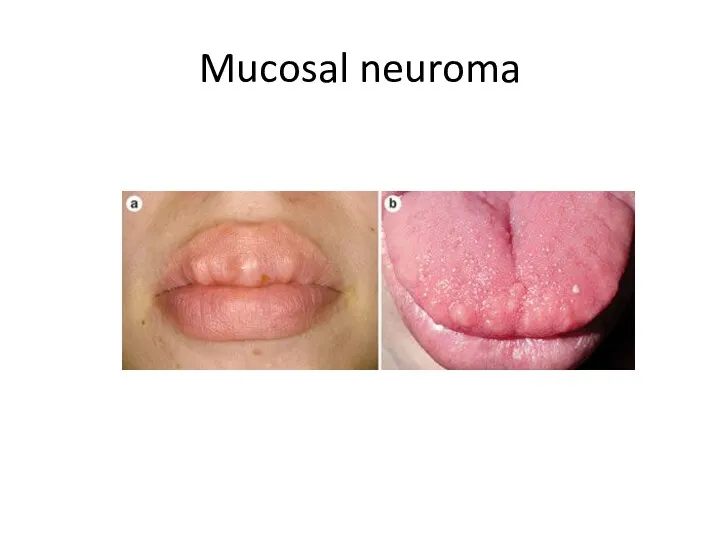
Mucosal neuroma
Mucosal neuroma
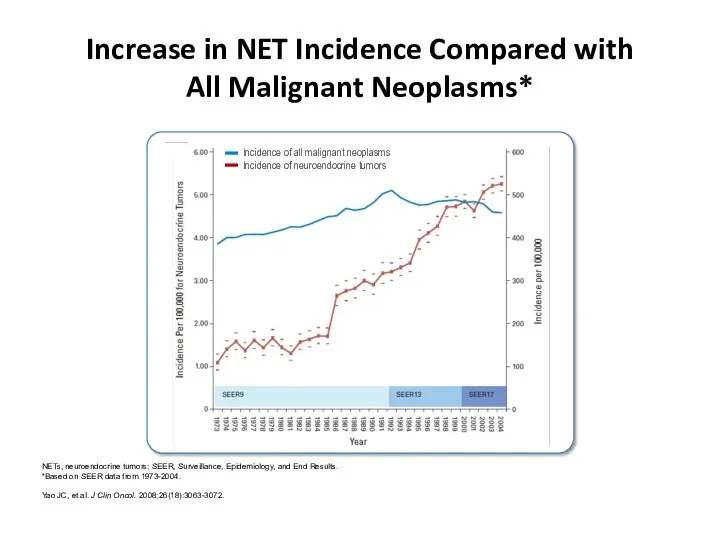
Increase in NET Incidence Compared with
All Malignant Neoplasms*
NETs, neuroendocrine tumors; SEER,
Increase in NET Incidence Compared with
All Malignant Neoplasms*
NETs, neuroendocrine tumors; SEER,
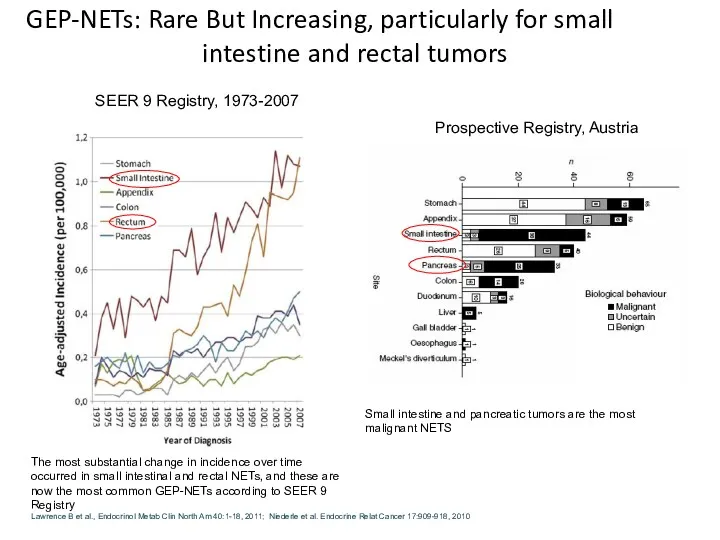
GEP-NETs: Rare But Increasing, particularly for small intestine and rectal tumors
Small
GEP-NETs: Rare But Increasing, particularly for small intestine and rectal tumors
Small
NET
Pancreatic
Non-pancreatic
Functioning
Non-functioning
Functioning
Non-functioning
40%–55% Oberg 2012
45%–60% Oberg 2012
68–80% Falconi 2006
Carcinoid syndrome
Carcinoid crisis
Carcinoid
NET
Pancreatic
Non-pancreatic
Functioning
Non-functioning
Functioning
Non-functioning
40%–55% Oberg 2012
45%–60% Oberg 2012
68–80% Falconi 2006
Carcinoid syndrome
Carcinoid crisis
Carcinoid
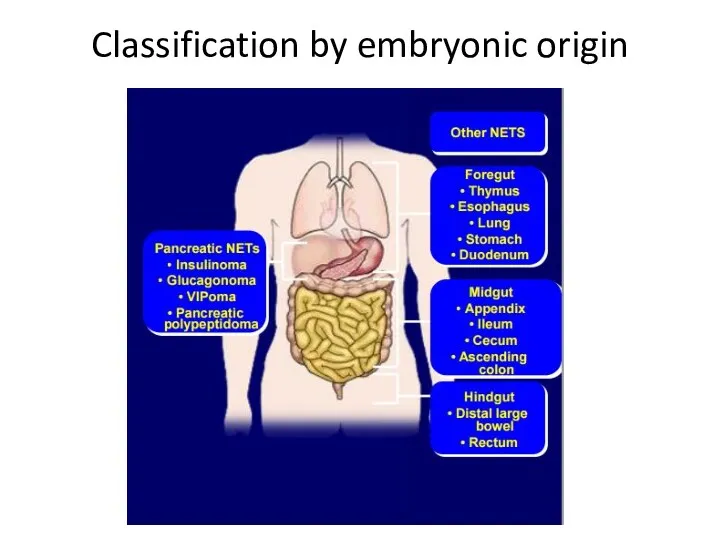
Classification by embryonic origin
Classification by embryonic origin
NETs: An Overview
Over 60% of NETs are metastatic at the time
NETs: An Overview
Over 60% of NETs are metastatic at the time
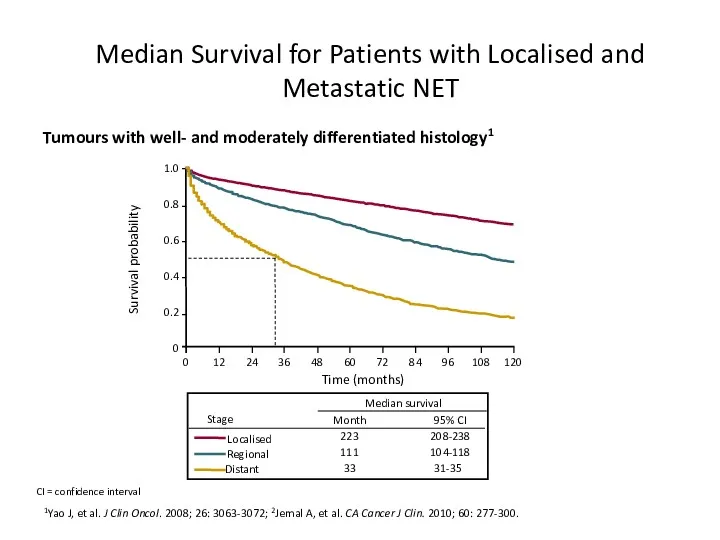
Median Survival for Patients with Localised and Metastatic NET
1Yao J, et
Median Survival for Patients with Localised and Metastatic NET
1Yao J, et
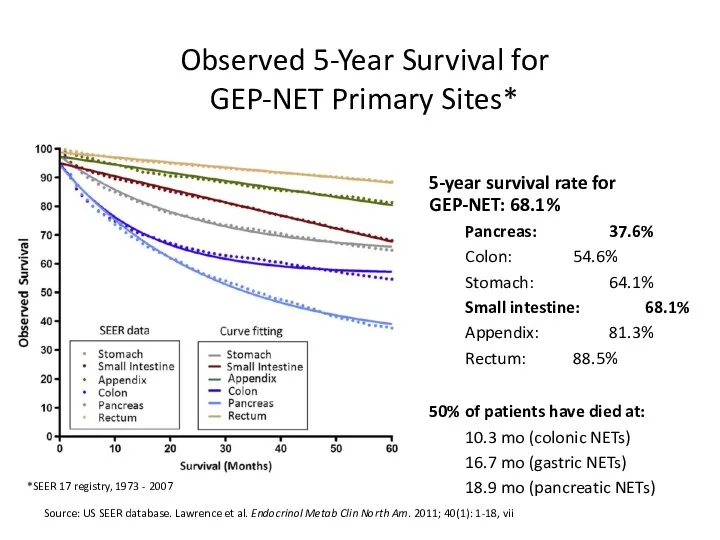
Observed 5-Year Survival for
GEP-NET Primary Sites*
Source: US SEER database. Lawrence
Observed 5-Year Survival for
GEP-NET Primary Sites*
Source: US SEER database. Lawrence
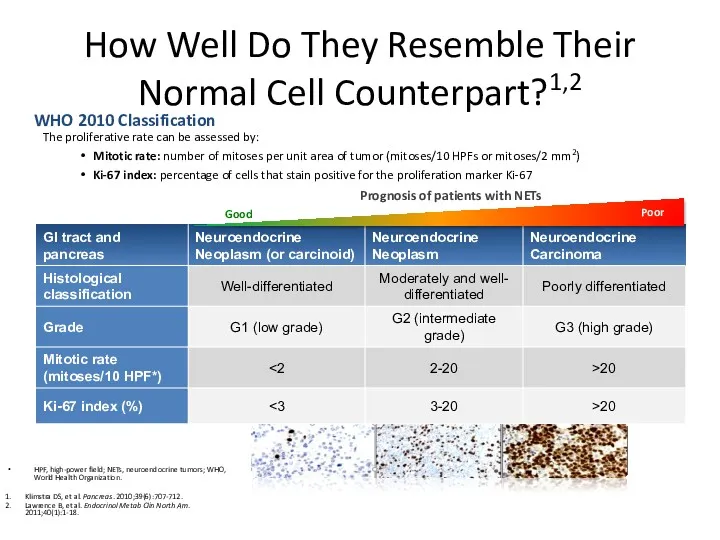
How Well Do They Resemble Their Normal Cell Counterpart?1,2
The proliferative
How Well Do They Resemble Their Normal Cell Counterpart?1,2
The proliferative
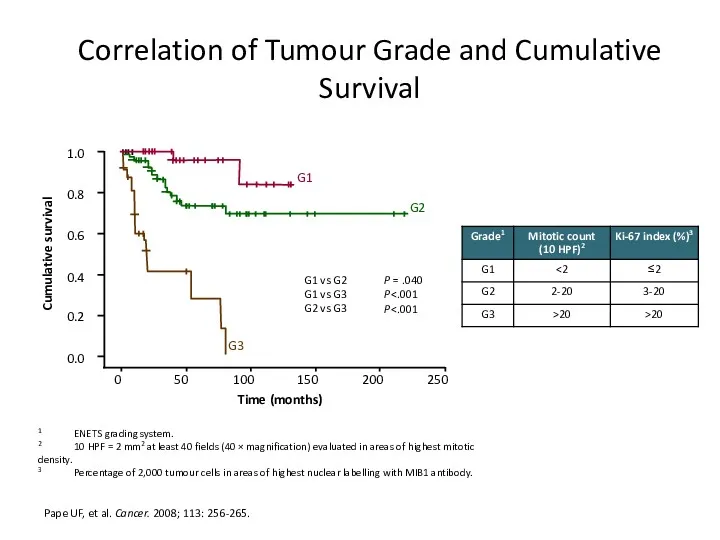
Correlation of Tumour Grade and Cumulative Survival
Pape UF, et al. Cancer.
Correlation of Tumour Grade and Cumulative Survival
Pape UF, et al. Cancer.
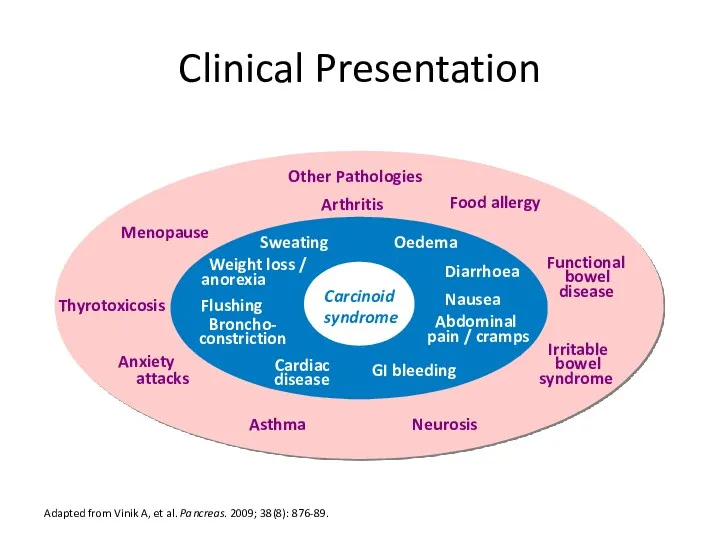
Clinical Presentation
Adapted from Vinik A, et al. Pancreas. 2009; 38(8): 876-89.
Nausea
Weight
Clinical Presentation
Adapted from Vinik A, et al. Pancreas. 2009; 38(8): 876-89.
Nausea
Weight
Kарциноидный синдром
10% случаев
опухоли Midgut (около 70%).
при метастазах в
Kарциноидный синдром
10% случаев
опухоли Midgut (около 70%).
при метастазах в
Kлиника
приливы (90%),
поносы (80%),
боли в животе (40%),
поражение клапанов сердца
Kлиника
приливы (90%),
поносы (80%),
боли в животе (40%),
поражение клапанов сердца
Карциноидный криз
Во время операции резкий выход серотонина в кровь
Бронхообструкция, гипотензия, аритмии
Профилактика:
Карциноидный криз
Во время операции резкий выход серотонина в кровь
Бронхообструкция, гипотензия, аритмии
Профилактика:
Диагностика
CT
MRI
Radiolabeled somatostatin receptor scintigraphy
DOTATATE (better)
5HIAA (5-Hydroxyindoleacetic acid - главный метаболит
Диагностика
CT
MRI
Radiolabeled somatostatin receptor scintigraphy
DOTATATE (better)
5HIAA (5-Hydroxyindoleacetic acid - главный метаболит
Карциноид Тимуса
2% - 7% DS при наличии передней медиастинальной массы
Кушинг
25% ассоциированы с
Карциноид Тимуса
2% - 7% DS при наличии передней медиастинальной массы
Кушинг
25% ассоциированы с
Легочный карциноид
25%
Typical (low grade)
Atypical (intermediate grade)
SCLC – KI67% > 30-40
Diffuse idiopathic
Легочный карциноид
25%
Typical (low grade)
Atypical (intermediate grade)
SCLC – KI67% > 30-40
Diffuse idiopathic
Лечение
Хирургическое
Лобэктомия с
диссекцией
л.у.
Лечение
Хирургическое
Лобэктомия с
диссекцией
л.у.
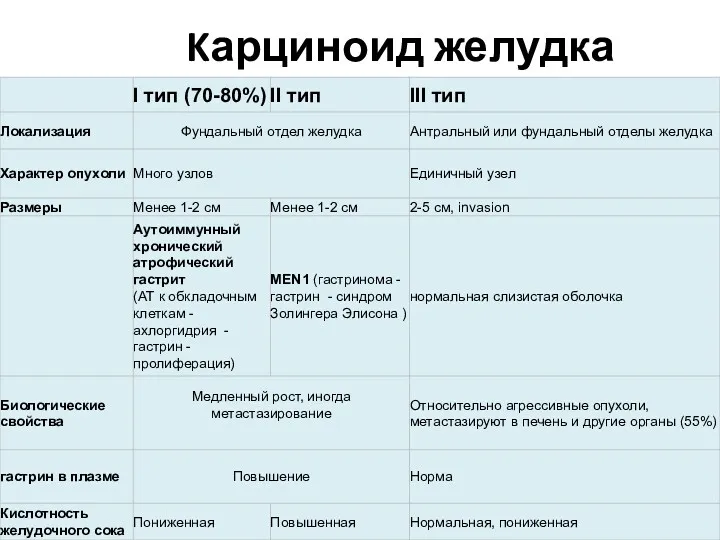
Kарциноид желудка
Kарциноид желудка
Лечение карциноидных опухолей желудка
I тип
- эндоскопическое иссечение одиночных опухолей
Лечение карциноидных опухолей желудка
I тип
- эндоскопическое иссечение одиночных опухолей
Kарциноид кишечника
лечение хирургическое
Аппендикс - <2 cm – simple apedectomy
> 2
Kарциноид кишечника
лечение хирургическое
Аппендикс - <2 cm – simple apedectomy
> 2
Нейроэндокринные опухоли поджелудочной железы
Нейроэндокринные опухоли поджелудочной железы
Инсулиномы
Cамые частые
растет из бета клеток
Только 5-10% злокачественные
Основной симптом – гипогликемия, связан
Инсулиномы
Cамые частые
растет из бета клеток
Только 5-10% злокачественные
Основной симптом – гипогликемия, связан
Гастриномы (синдром Золлингера – Эллисона)
Bторое место среди эндокринных опухолей поджелудочной железы
70%
Гастриномы (синдром Золлингера – Эллисона)
Bторое место среди эндокринных опухолей поджелудочной железы
70%
Випомы (синдром Вернера –
Моррисона)
Cекреция вазоактивного интестинального пептида (VIP)
MEN1 - 6%
Метастазирование
Поносы
Випомы (синдром Вернера –
Моррисона)
Cекреция вазоактивного интестинального пептида (VIP)
MEN1 - 6%
Метастазирование
Поносы
Глюкагономы
B α - клетках поджелудочной железы
Глюкагон стимулирует распад гликогена, глюконеогенез, кетогенез,
Глюкагономы
B α - клетках поджелудочной железы
Глюкагон стимулирует распад гликогена, глюконеогенез, кетогенез,
Pancreatic polypeptidoma
Относится к нефункционирующим опухолям ПЖЖ
Как правило Дз в поздних стадиях
Клиника
Pancreatic polypeptidoma
Относится к нефункционирующим опухолям ПЖЖ
Как правило Дз в поздних стадиях
Клиника
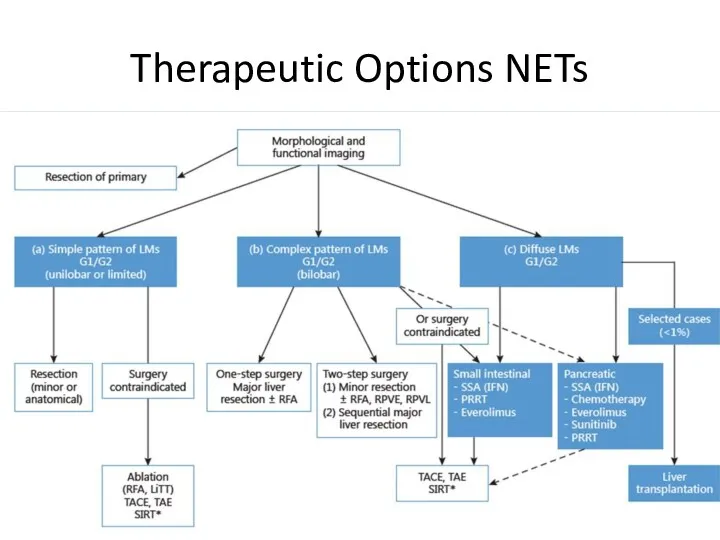
Therapeutic Options NETs
Surgery
Curative, Ablative
Debulking
Radiofrequency ablation (RFA)
Embolization/chemoembolization/radioembolization (SIRT)
Debulking surgery?
Irradiation
External
Therapeutic Options NETs
Surgery
Curative, Ablative
Debulking
Radiofrequency ablation (RFA)
Embolization/chemoembolization/radioembolization (SIRT)
Debulking surgery?
Irradiation
External
Общие принципы лечения локальной болезни в зависимости от GRADE
G1-2 – хирургическое
G3
Общие принципы лечения локальной болезни в зависимости от GRADE
G1-2 – хирургическое
G3
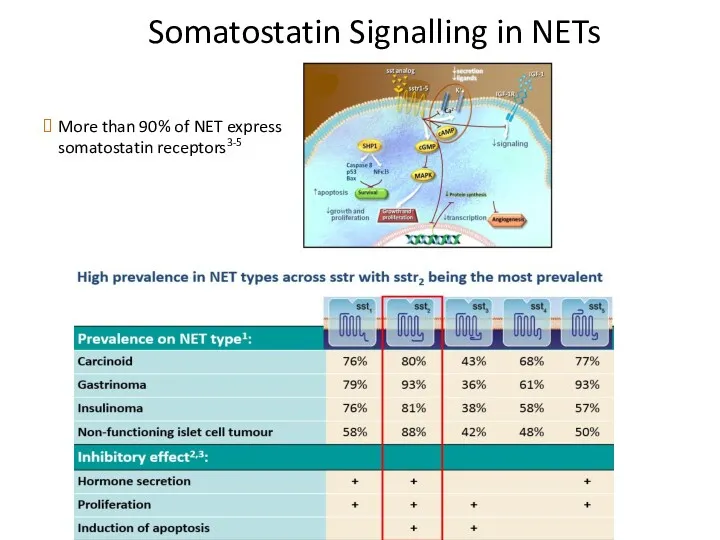
Somatostatin Signalling in NETs
More than 90% of NET express somatostatin receptors3-5
Somatostatin Signalling in NETs
More than 90% of NET express somatostatin receptors3-5
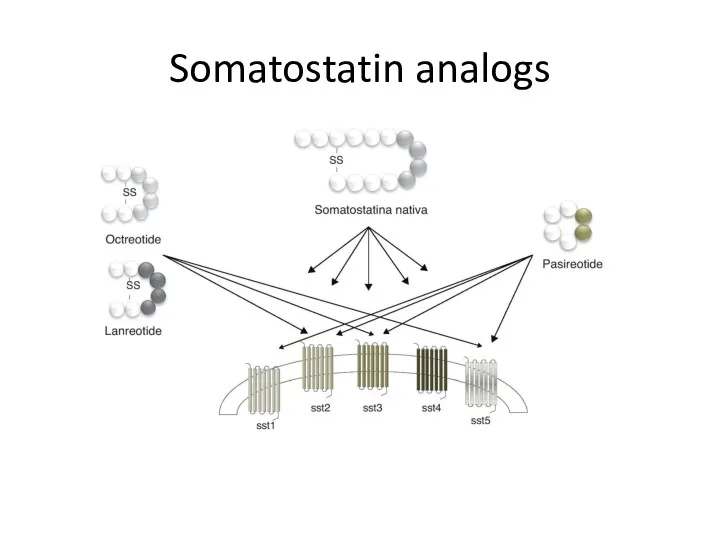
Somatostatin analogs
Somatostatin analogs
Somatostatin analogs
Octreotide LAR
N=85
TTP
Midgut
Functional 39%
Octreoscan pos 75%
Live involvement up to 10%
Somatostatin analogs
Octreotide LAR
N=85
TTP
Midgut
Functional 39%
Octreoscan pos 75%
Live involvement up to 10%
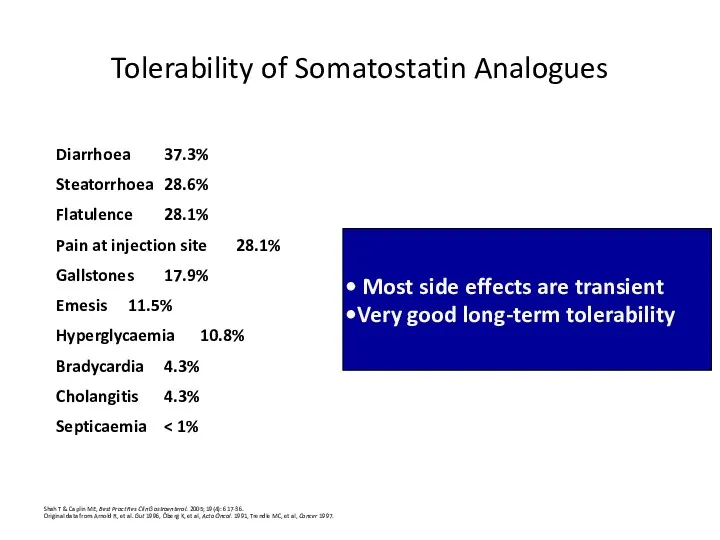
Tolerability of Somatostatin Analogues
Shah T & Caplin ME, Best Pract Res
Tolerability of Somatostatin Analogues
Shah T & Caplin ME, Best Pract Res
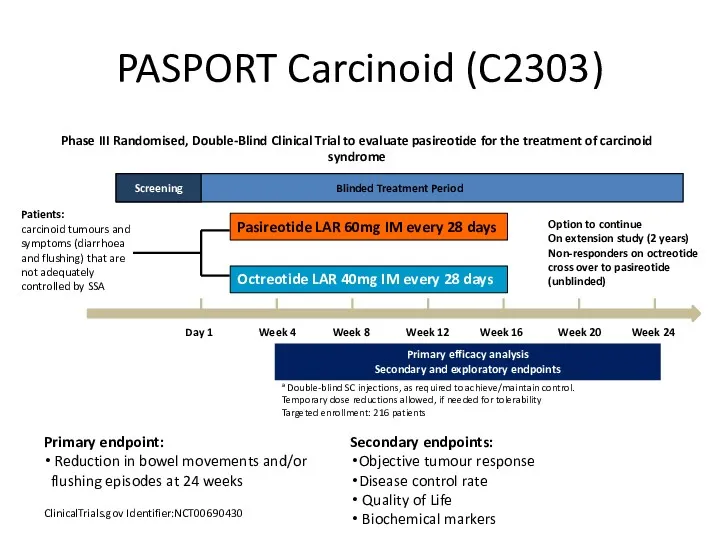
PASPORT Carcinoid (C2303)
ClinicalTrials.gov Identifier:NCT00690430
Primary endpoint:
Reduction in bowel movements and/or
PASPORT Carcinoid (C2303)
ClinicalTrials.gov Identifier:NCT00690430
Primary endpoint:
Reduction in bowel movements and/or
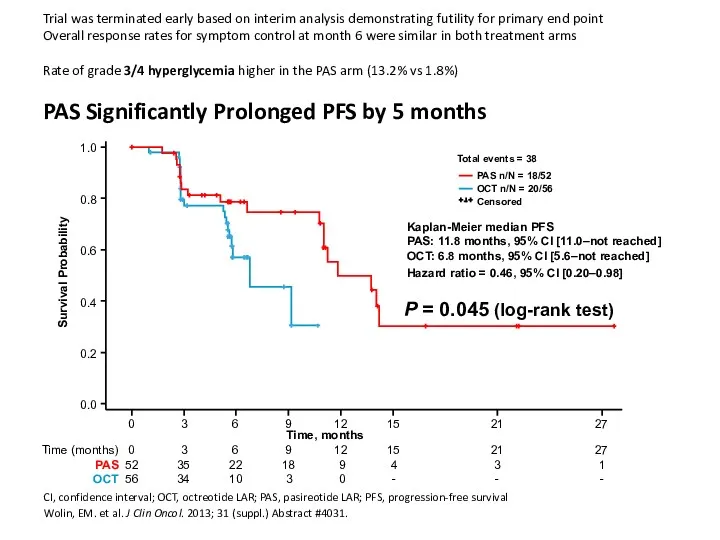
Trial was terminated early based on interim analysis demonstrating futility for
Trial was terminated early based on interim analysis demonstrating futility for
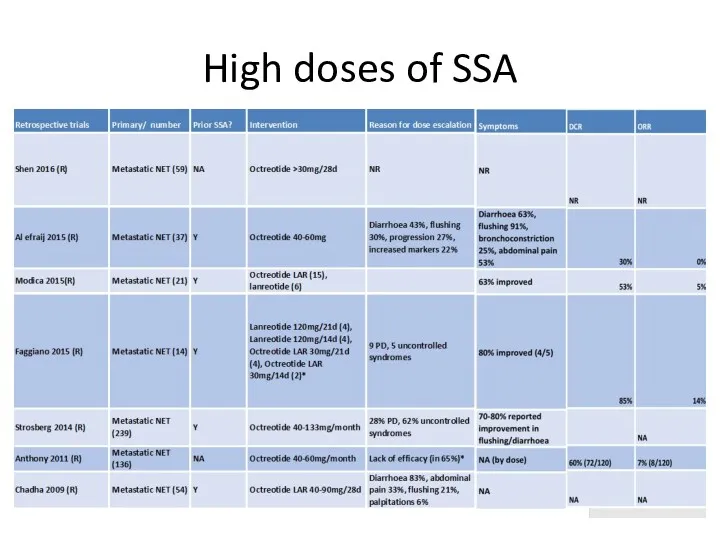
High doses of SSA
High doses of SSA
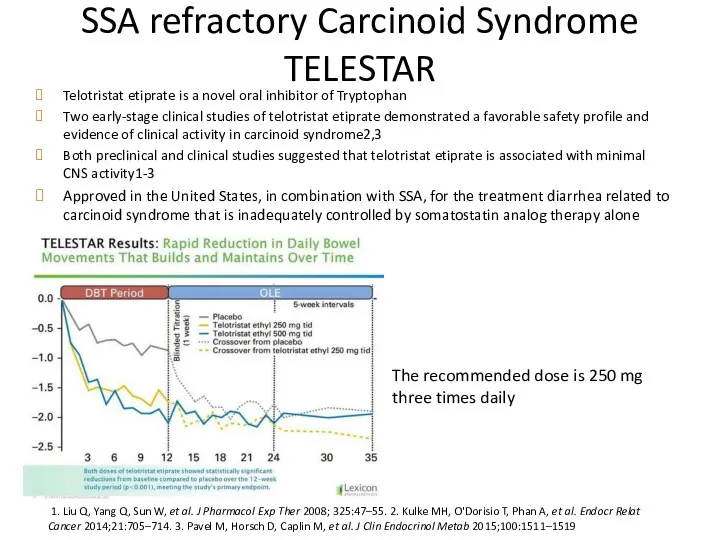
SSA refractory Carcinoid Syndrome TELESTAR
Telotristat etiprate is a novel oral inhibitor
SSA refractory Carcinoid Syndrome TELESTAR
Telotristat etiprate is a novel oral inhibitor
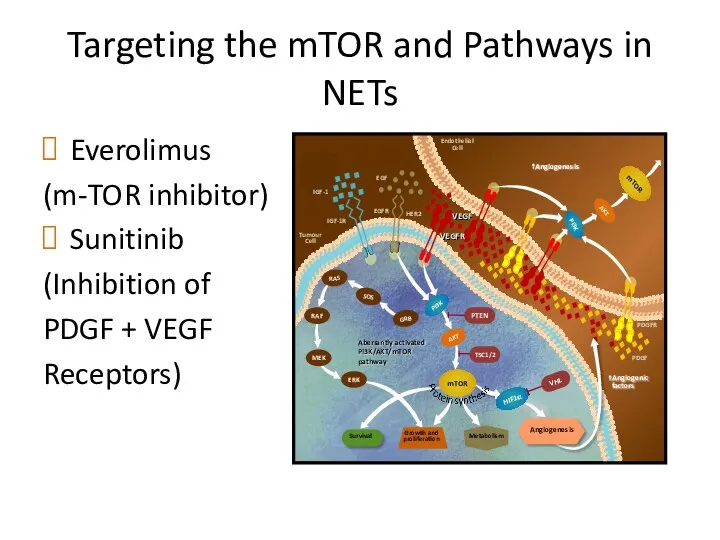
Targeting the mTOR and Pathways in NETs
Everolimus
(m-TOR inhibitor)
Sunitinib
(Inhibition of
PDGF +
Targeting the mTOR and Pathways in NETs
Everolimus
(m-TOR inhibitor)
Sunitinib
(Inhibition of
PDGF +
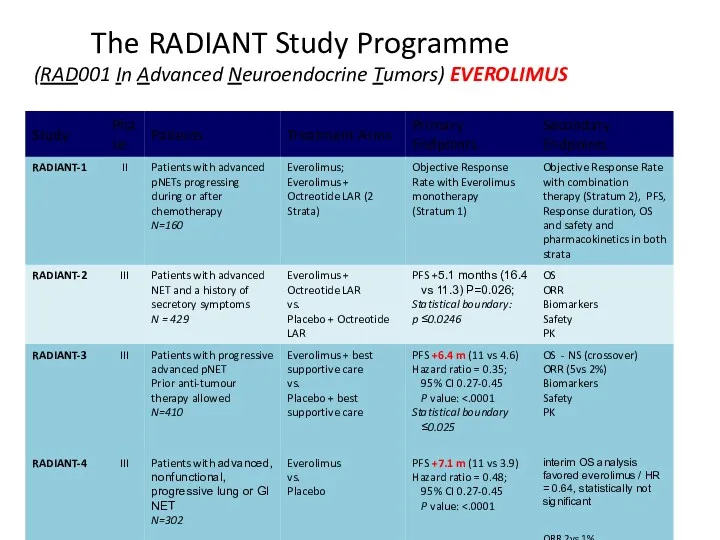
The RADIANT Study Programme
(RAD001 In Advanced Neuroendocrine Tumors) EVEROLIMUS
The RADIANT Study Programme
(RAD001 In Advanced Neuroendocrine Tumors) EVEROLIMUS
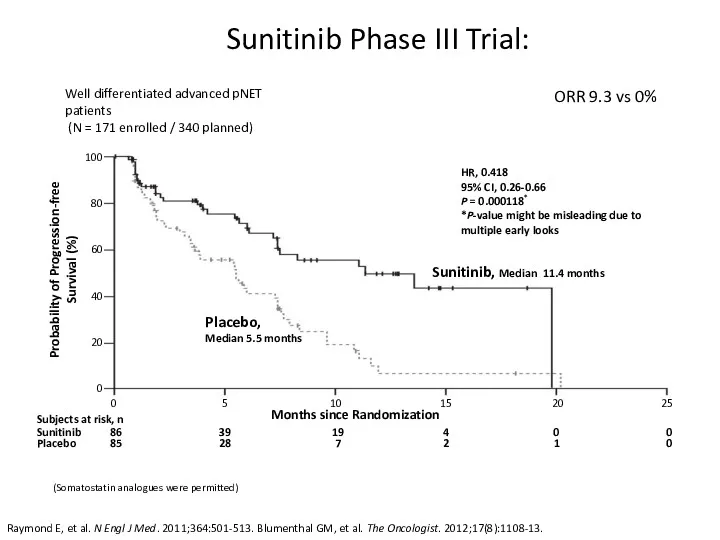
Sunitinib Phase III Trial:
Raymond E, et al. N Engl J
Sunitinib Phase III Trial:
Raymond E, et al. N Engl J
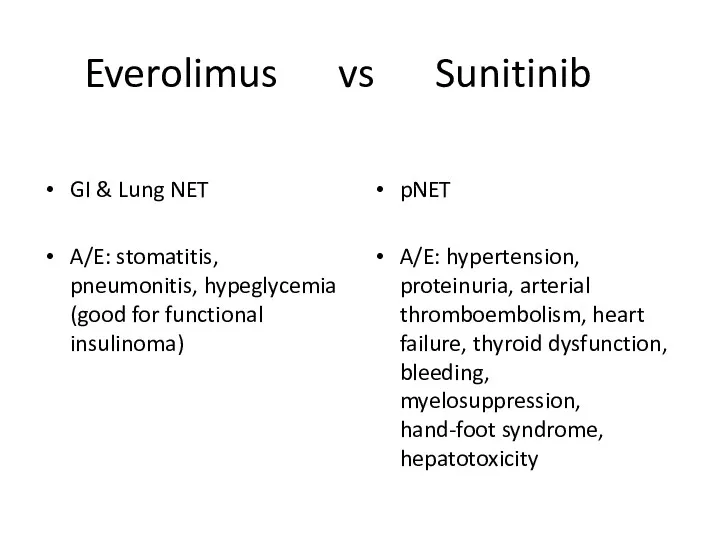
Everolimus vs Sunitinib
GI & Lung NET
A/E: stomatitis, pneumonitis, hypeglycemia (good for
Everolimus vs Sunitinib
GI & Lung NET
A/E: stomatitis, pneumonitis, hypeglycemia (good for
PRRT
PRRT
PRRT
PRRT
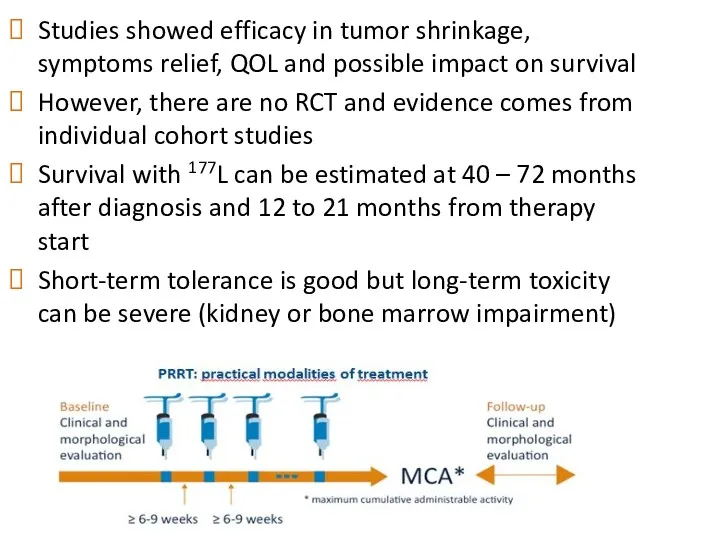
Studies showed efficacy in tumor shrinkage, symptoms relief, QOL and possible
Studies showed efficacy in tumor shrinkage, symptoms relief, QOL and possible
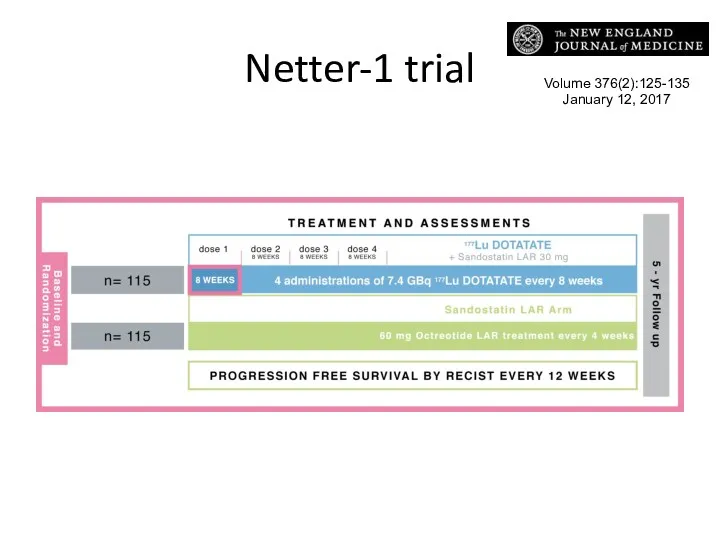
Netter-1 trial
Volume 376(2):125-135
January 12, 2017
Netter-1 trial
Volume 376(2):125-135
January 12, 2017
PFS & OS
In patients with midgut neuroendocrine tumors that progressed during
PFS & OS
In patients with midgut neuroendocrine tumors that progressed during
Chemotherapy in NET
Well-differentiated NET do not exhibit high sensitivity to chemotherapy
Chemotherapy in NET
Well-differentiated NET do not exhibit high sensitivity to chemotherapy
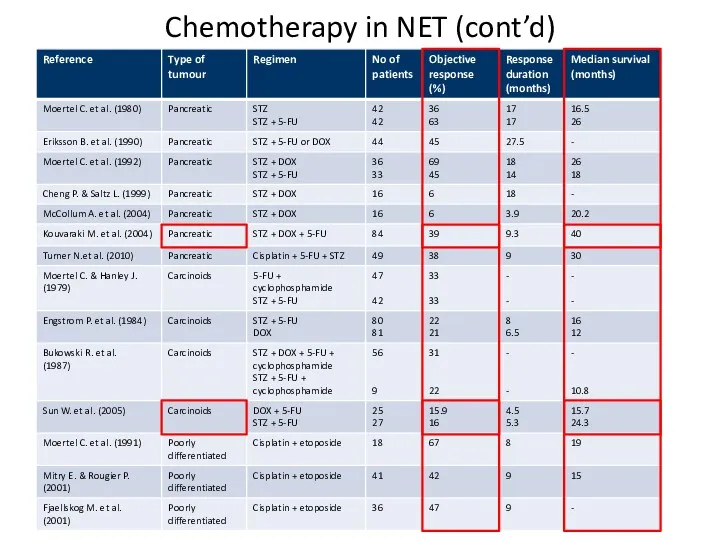
Chemotherapy in NET (cont’d)
Chemotherapy in NET (cont’d)
Temozolomide
Retrospective analysis of temozolomide alone suggests efficacy in treating bronchial and
Temozolomide
Retrospective analysis of temozolomide alone suggests efficacy in treating bronchial and
 Группы здоровья детей в детском саду
Группы здоровья детей в детском саду Растения, кровоостанавливающего действия
Растения, кровоостанавливающего действия Туа біткен иммунды жауапты қамтамасыз етуде микробиоценоздардың маңызы
Туа біткен иммунды жауапты қамтамасыз етуде микробиоценоздардың маңызы Особенности изучения эпизоотической ситуации при гельминтозах. Методы посмертной и прижизненной диагностики
Особенности изучения эпизоотической ситуации при гельминтозах. Методы посмертной и прижизненной диагностики Акушерлік операциялар. Акушерлік қысқаштар, вакуум-экстракция, кесар тілігі
Акушерлік операциялар. Акушерлік қысқаштар, вакуум-экстракция, кесар тілігі Санаторий-профилакторий Романтика в Кемеровской области
Санаторий-профилакторий Романтика в Кемеровской области Понятие о военной медицине. Организация и тактика медицинской службы как наука и предмет преподавания
Понятие о военной медицине. Организация и тактика медицинской службы как наука и предмет преподавания Клинические рекомендации Диагностика и лечение артериальной гипертонии
Клинические рекомендации Диагностика и лечение артериальной гипертонии Внемозговые опухоли мостомозжечкового угла. Вестибулярная шваннома. Менингиома
Внемозговые опухоли мостомозжечкового угла. Вестибулярная шваннома. Менингиома Дезинфекция и стерилизация
Дезинфекция и стерилизация Лечение и диета при ХСН
Лечение и диета при ХСН Общественное здравоохранение
Общественное здравоохранение Холера. Классификация. Клиника. Симптомы и течение
Холера. Классификация. Клиника. Симптомы и течение Тоны сердца
Тоны сердца Системная красная волчанка (МКБ – Х М32.09)
Системная красная волчанка (МКБ – Х М32.09) Топографическая анатомия и оперативная хирургия таза и промежности
Топографическая анатомия и оперативная хирургия таза и промежности Развитие зубов. Закладка зачатков зубов
Развитие зубов. Закладка зачатков зубов Ұйқы физиологиясы, бұзылыстары және емі
Ұйқы физиологиясы, бұзылыстары және емі Вирусные гепатиты
Вирусные гепатиты Виды травматизма
Виды травматизма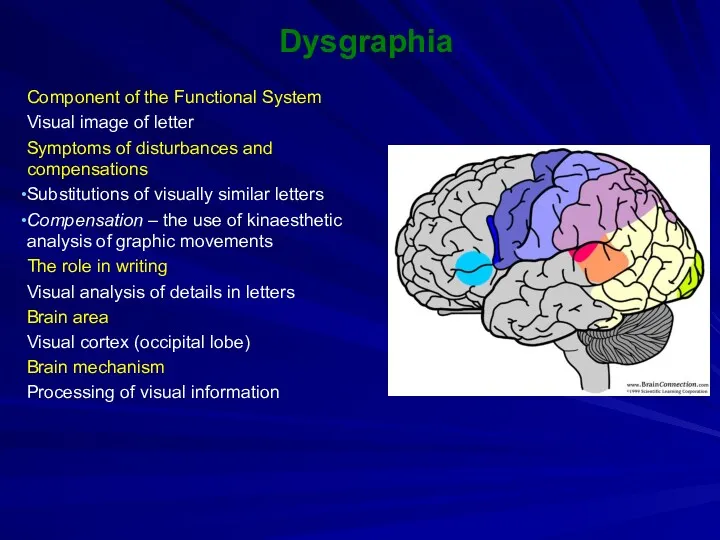 Dysgraphia
Dysgraphia Обучение пациентов. Процесс обучения
Обучение пациентов. Процесс обучения Расстройства кровообращения. Стаз, тромбоз, эмболия, инфаркт. (Занятие 5)
Расстройства кровообращения. Стаз, тромбоз, эмболия, инфаркт. (Занятие 5) Хроническая сердечная недостаточность
Хроническая сердечная недостаточность Клуб правильного питания. Часть 1
Клуб правильного питания. Часть 1 Показания к трансплантации печени
Показания к трансплантации печени Термические поражения
Термические поражения Қазіргі кездегі өнеркәсіптік қала тұрғындарының денсаулығы
Қазіргі кездегі өнеркәсіптік қала тұрғындарының денсаулығы