- Oncology. Tumor

Содержание
- 2. Tumor(s). /Lat., neoplasm, new growth/, pathological blastoma formation, spontaneously originating in the different organs, differing by
- 3. Benign tumors possess expensive growth, resulting at that surrounding tissues move apart, sometimes are compressed and
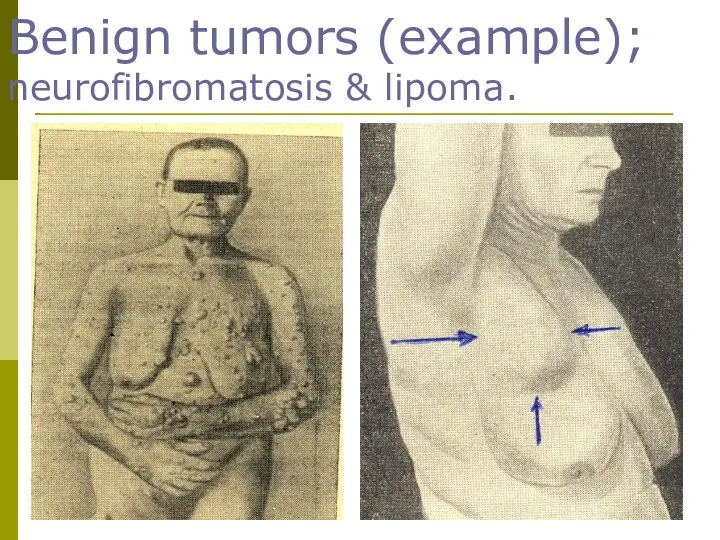
- 4. Benign tumors (example); neurofibromatosis & lipoma.
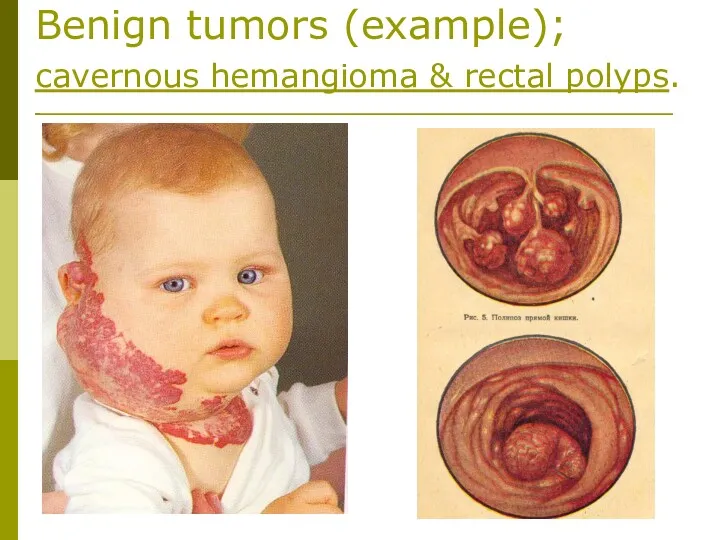
- 5. Benign tumors (example); cavernous hemangioma & rectal polyps.
- 6. Malignant tumors infiltrate and destroy surrounding tissues. Infiltrative (invasive) growth is the main criterion discriminating malignant
- 7. Malignant tumors (example); different forms of breast cancer.
- 8. Malignant tumors (example); rectal cancer & sarcoma of scapule.
- 9. Annually 6 mln people fall ill with tumors and 5 mln die from them. In the
- 10. In males the most part from all cases of malignant tumors makes cancer of the lung,
- 11. ETIOLOGY 1) Vihrov’s theory of irritation. 2) Kangeim’s theory of embryonic germs. 3) Fisher-Vazels’ regeneration-mutation theory.
- 12. At present tumors are considered to be polyetiologic diseases. In the base of their development is:
- 13. For the origin of tumor it is of necessity the presence of internal causes: genetic predisposition
- 14. Various etiological factors predominate in tumours ethiology with different localization-I. One of the main causes of
- 15. Various etiological factors predominate in tumours ethiology with different localization-II. Tumors of the body of uterus,
- 16. PATHOGENESIS-I. Arise of cancer is always separated from the moment of etiological factor action, so-called “latent
- 17. PATHOGENESIS-II. At that, the cell as a result of the genome modification gains new heritable features:
- 18. PATHOGENESIS-III. The increase of immune exertion is a result of the process mentioned above. In sufficient
- 19. PATHOGENESIS-IV. The main components, predetermining the origin of tumor are: a) local preparedness of tissues; b)
- 20. PATHOGENESIS-V. Presence of precancerous condition of the organ or tissue is the main of local factors,
- 21. PATHOGENESIS-VI. Common factors predisposing to the development of malignant process: 1) genetic predisposion; 2) changes of
- 22. Influence of benign tumors on the organism. Despite of the fact that benign tumors grow relatively
- 23. Influence of malignant tumors on the organism (in common). Two interrelated forms of systemic action on
- 24. Influence of malignant tumors on the organism-I. In carbohydrate metabolism. - In malignant tumors glucose isn’t
- 25. Influence of malignant tumors on the organism-II. In aminoacide metabolism. Tumor tissue is a peculiar trap
- 26. Influence of malignant tumors on the organism-III. In fatty /lipids/ metabolism. Growth of tumor leads to
- 27. Nomenclature, structure & classification of tumors-I. Histogenetic and histological principles are in the base of the
- 28. Nomenclature, structure & classification of tumors-II. In the name of tumor besides its histological features, there
- 29. Nomenclature, structure & classification of tumors-III. Quite often in the name of tumor its cellular content
- 30. Nomenclature, structure & classification of tumors-IV. Under the conception of possible sources of development, tumors are
- 31. Nomenclature, structure & classification of tumors-V. Malignant connective (-tissue) tumors have got the common name sarcomae.
- 32. Nomenclature, structure & classification of tumors-VI. Technologically various is indication of tumor originating from epithelium. So,
- 33. Nomenclature, structure & classification of tumors-VII. CANCER /from Lat./ - malignant tumor, developing from epithelial tissue.
- 34. Nomenclature, structure & classification of tumors-VIII. However not all mentioned features of cancer may be considered
- 35. Nomenclature, structure & classification of tumors-IX. Macroscopic view of tumor is various one. Tumor may be
- 36. Nomenclature, structure & classification of tumors-X. Relating to the lumen of the organ, tumor may be:
- 37. Different types of growth of rectal cancer (example);endophyte & exophyte.
- 38. Different types of growth of gastric cancer (example); exophyte, endophyte & mixted.
- 39. Nomenclature, structure & classification of tumors-XI. Sometimes the tumor as if infiltrates the whole organ diffuse-like.
- 40. Nomenclature, structure & classification of tumors-XII. The base for diagnosis of tumor in histological investigation is
- 41. Nomenclature, structure & classification of tumors-XIII. Microscopic investigation of tumor displays the degree of their differences
- 42. Nomenclature, structure & classification of tumors-XIV. Structural atipicity of tumor spreads over all its components –
- 43. Nomenclature, structure & classification of tumors-XV. Structure and classification of cancer. The variety of macroscopic kinds
- 44. Nomenclature, structure & classification of tumors-XVI. In benign tumors of epithelial nature the character of tumor
- 45. Nomenclature, structure & classification of tumors-XVII. For the cancer in which tumor complexes or individual tumor
- 46. Nomenclature, structure & classification of tumors-XVIII. Cancer, having endophytic growth spreads mainly in the thickness of
- 47. Nomenclature, structure & classification of tumors-XIX. In some kinds of cancer due to the lack of
- 48. Nomenclature, structure & classification of tumors-XX. Quite often the base for indication the tumor kind is
- 49. Nomenclature, structure & classification of tumors-XXI. In intracellular production of mucus cancer cells, overfull with mucoid
- 50. Nomenclature, structure & classification of tumors-XXII. Some kinds of cancer have the ability to produce specific
- 51. Nomenclature, structure & classification of tumors-XXIII. At the same time epithelium of some organs, in norm
- 52. Nomenclature, structure & classification of tumors-XXIV. Stromal component /besides epithelial component/ is the important element of
- 53. Nomenclature, structure & classification of tumors-XXV. The other forms of cancer in the low level of
- 54. Nomenclature, structure & classification of tumors-XXVI. On the ground of histological structure, by the extent of
- 55. Nomenclature, structure & classification of tumors-XXVII. It is International system of clinical classification of cancer (TNM)
- 56. Nomenclature, structure & classification of tumors-XXVIII. Spread of the primary tumor node is indicated by symbol
- 57. Nomenclature, structure & classification of tumors-XXVIX. For mammary gland tumor the gradation is fulfilled by the
- 58. Nomenclature, structure & classification of tumors-XXX. Symbol N (nodulus) is used to designate metastases into the
- 59. Nomenclature, structure & classification of tumors-XXXI. Symbol M (metastases) indicates the presence (M1 or M+) or
- 60. Nomenclature, structure & classification of tumors-XXXII. Index G (grade) – defines the degree of malignancy (degree
- 61. Nomenclature, structure & classification of tumors-XXXIII. Index P (penetration) is introduced only for tumors of the
- 62. Nomenclature, structure & classification of tumors-XXXIV. Classification by TNM system is considered to be convenient one,
- 63. Nomenclature, structure & classification of tumors-XXXV. According to clinical classification four stages of tumors are distinguished:
- 64. Nomenclature, structure & classification of tumors-XXXVI. stage III– tumor has great sizes, with resolution, grows through
- 65. Nomenclature, structure & classification of tumors-XXXVII. For every location of malignant tumor correspondence of clinical stages
- 66. Clinical picture & diagnosis of tumors-I. Diagnosis of benign tumors is based only on the local
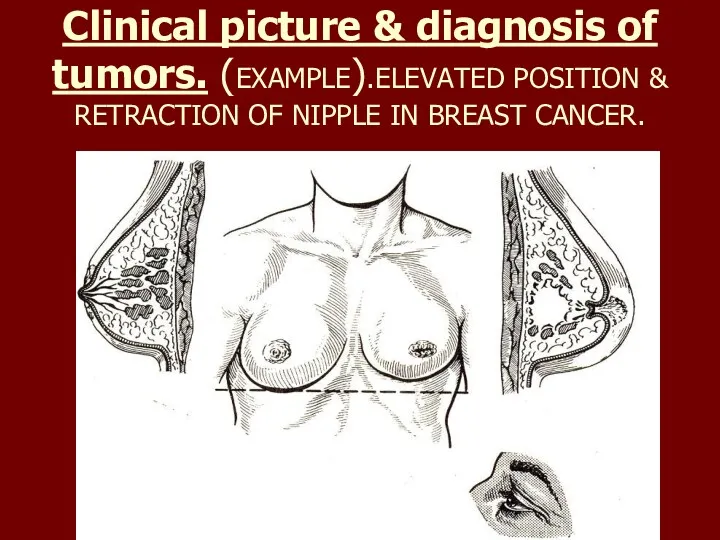
- 67. Clinical picture & diagnosis of tumors. (EXAMPLE).ELEVATED POSITION & RETRACTION OF NIPPLE IN BREAST CANCER.
- 68. Clinical picture & diagnosis of tumors-II. In clinical pictures of malignant tumors 4 principle syndromes are
- 69. Сlinical picture of malignant tumors-I Syndrome “plus-tissue”. Tumor may be founded directly in the area of
- 70. Сlinical picture of malignant tumors-II Syndrome of pathological discharge. In the presence of malignant tumor due
- 71. Сlinical picture of malignant tumors-III Syndrome of the functional disorder. Manifestations of this syndrome are various
- 72. Сlinical picture of malignant tumors-IV Syndrome of small signs. The patients with malignant new formations frequently
- 73. Diagnostics of tumors-I The base of tumor diagnosis is their timely identification at the early stages
- 74. Diagnostics of tumors-II Diagnostics of tumors are subdivided into: 1) primary diagnostics, carried out under conditions
- 75. Diagnostics of tumors-III Clarifying diagnostics in patients with already revealed malignant tumor or suspicion on it
- 76. Diagnostics of tumors-IV Local criteria include: 1) adjusted location of the primary tumor; 2) anatomical peculiarities
- 77. Diagnostics of tumors-V Along with estimation of the local and common criteria in the hospital individual
- 78. Diagnostics of tumors-VI X-ray investigation includes: 1) uncontrast & contrast methods. Uncontrast methods /roentgenoscopy/ /graphy/, tomography)
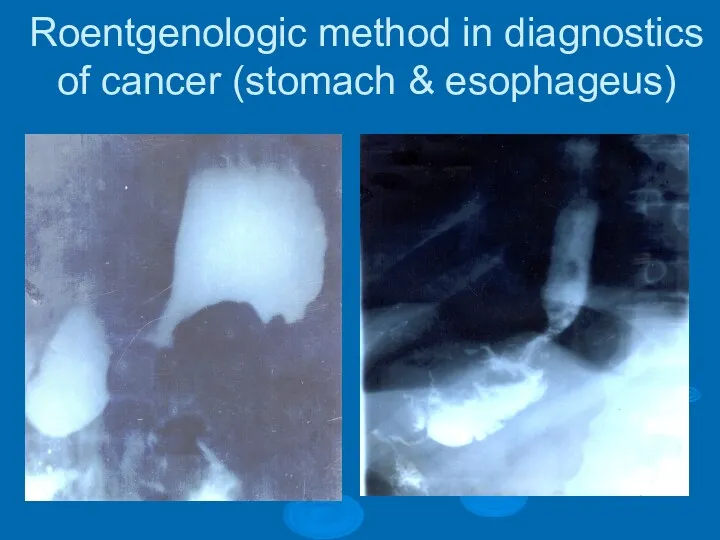
- 79. Roentgenologic method in diagnostics of cancer (stomach & esophageus)
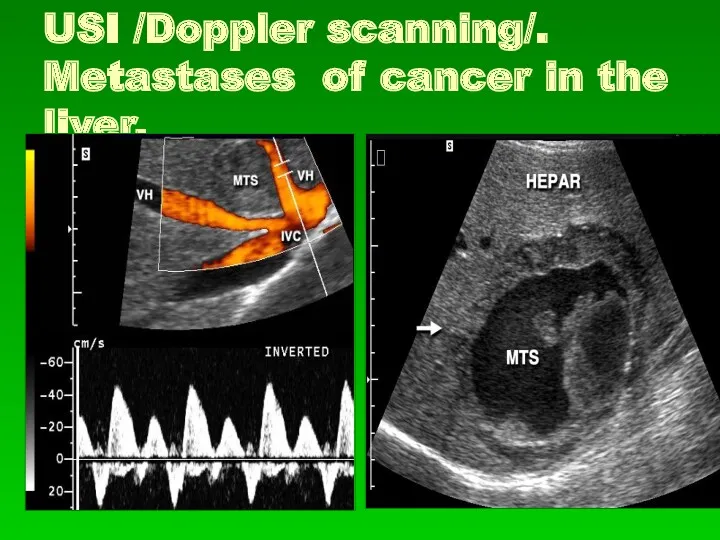
- 80. USI /Doppler scanning/. Metastases of cancer in the liver.
- 81. (CT) COMPUTER TOMOGRAPHY OF LIVER WITH CANCER (mts).
- 82. Diagnostics of tumors-VII Endoscopic methods allow to carry out investigation with the help of special instruments,
- 83. ENDOSCOPY in diagnostics of cancer of hollow organs
- 84. Diagnostics of tumors-VIII In any case of tumor or in suspicion to tumor morphological methods of
- 85. Diagnostics of tumors-IX Radioisotopic methods of investigation are based on the ability of many tumors &
- 86. Diagnostics of tumors-X Laboratory methods of diagnosis of malignant tumors are less informative, since universal laboratory
- 87. Diagnostics of tumors-XI In the cases when the complex of clarifying diagnostification methods is found to
- 88. Treatment of tumors-I Treatment of benign tumors - operative excision of tumor /in individual cases it
- 89. Treatment of tumors-II Treatment of malignant tumors is fulfilled by various means depending on: a) character
- 90. Treatment of tumors-III The main methods of treating of malignant tumors are: 1) surgical treatment; 2)
- 91. Treatment of tumors-IV Surgical treatment is the main one in the most tumors. It may be
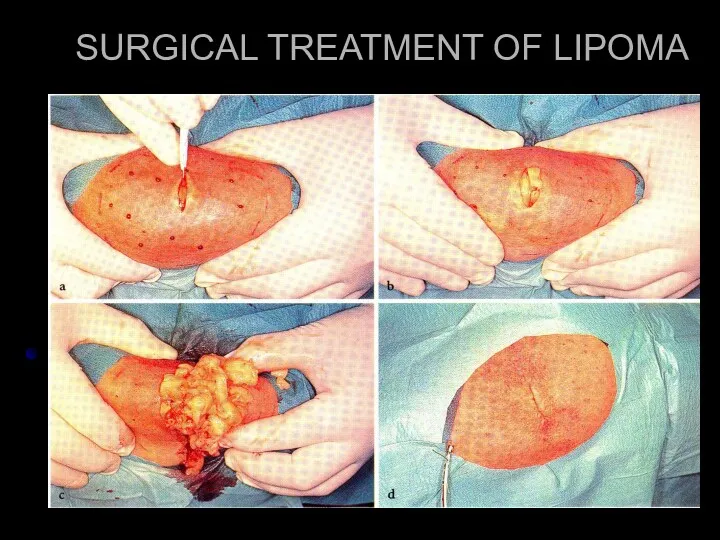
- 92. SURGICAL TREATMENT OF LIPOMA
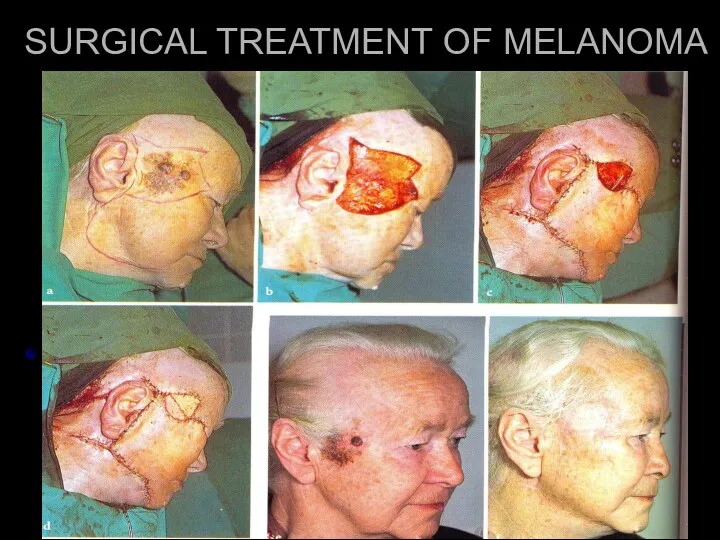
- 93. SURGICAL TREATMENT OF MELANOMA
- 94. Treatment of tumors-V During the removal of malignant new formation it is necessary to observe so-called
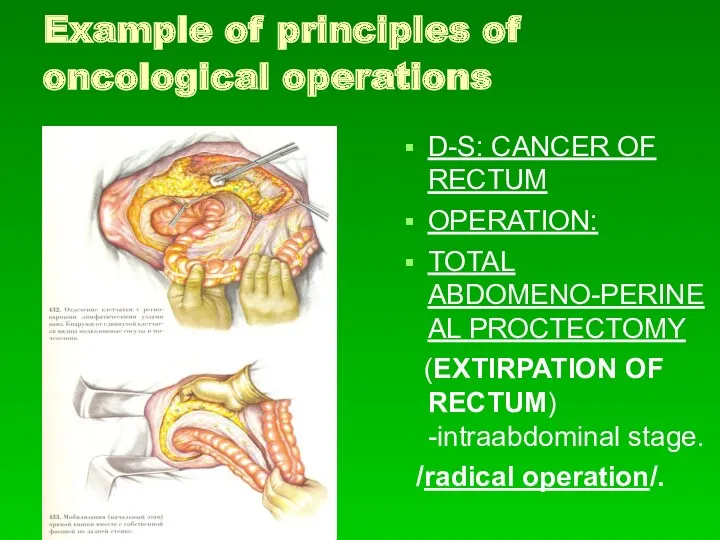
- 95. Example of principles of oncological operations D-S: CANCER OF RECTUM OPERATION: TOTAL ABDOMENO-PERINEAL PROCTECTOMY (EXTIRPATION OF
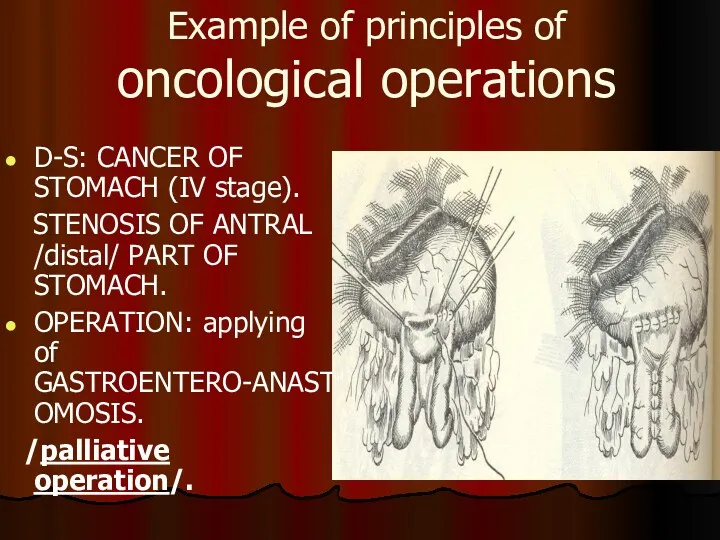
- 96. Example of principles of oncological operations D-S: CANCER OF STOMACH (IV stage). STENOSIS OF ANTRAL /distal/
- 97. Treatment of tumors-VI - Ablastics – complex of measures directed at prevention of tumor cells spread
- 98. Treatment of tumors-VII - Antiblastics – complex of measures directed at destruction at the time of
- 99. Treatment of tumors-VIII - Zoning. During the operation for malignant tumor it is necessary to remove
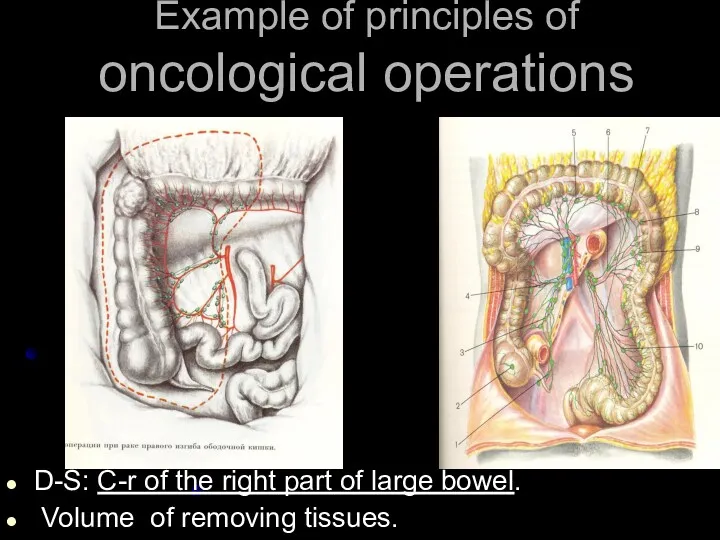
- 100. Example of principles of oncological operations D-S: C-r of the right part of large bowel. Volume
- 101. Treatment of tumors-IX In exophytic growth of tumor /when its base is relatively narrow, and the
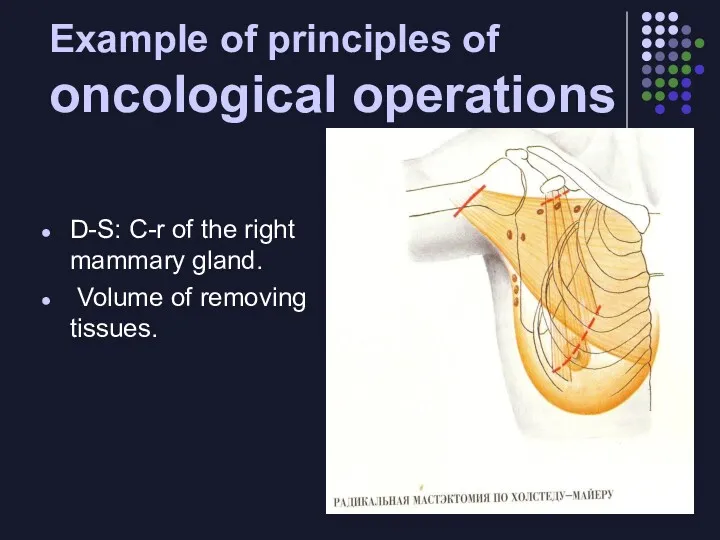
- 102. Example of principles of oncological operations D-S: С-r of the right mammary gland. Volume of removing
- 103. Treatment of tumors-X (Saving/keeping/ «case»). Lymph vessels and nodes, through wich is possible the spreading of
- 104. Treatment of tumors-XI Radical operations in cancer of any location may be one- or multistage. For
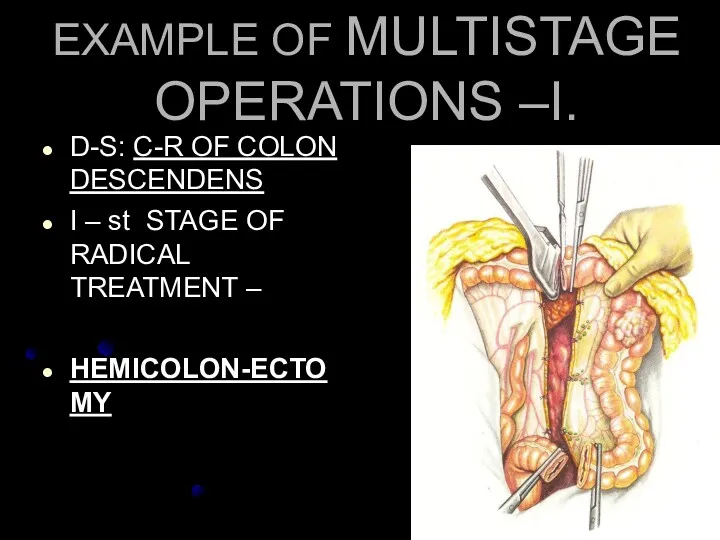
- 105. EXAMPLE OF MULTISTAGE OPERATIONS –I. D-S: С-R OF COLON DESCENDENS I – st STAGE OF RADICAL
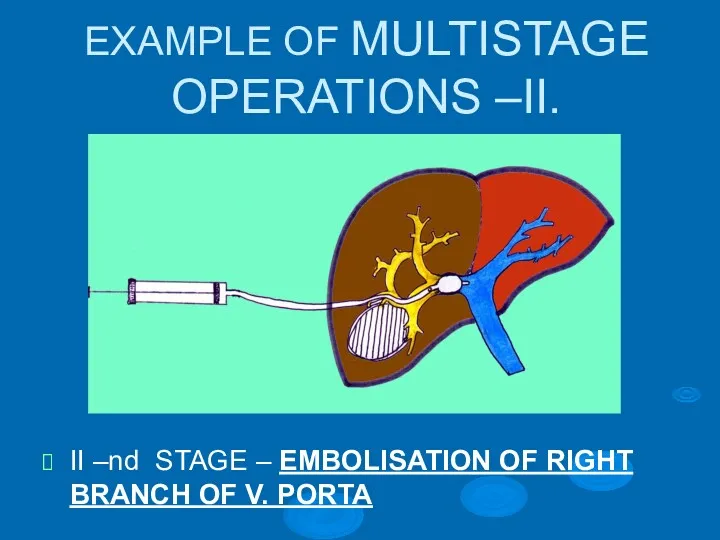
- 106. EXAMPLE OF MULTISTAGE OPERATIONS –II. II –nd STAGE – EMBOLISATION OF RIGHT BRANCH OF V. PORTA
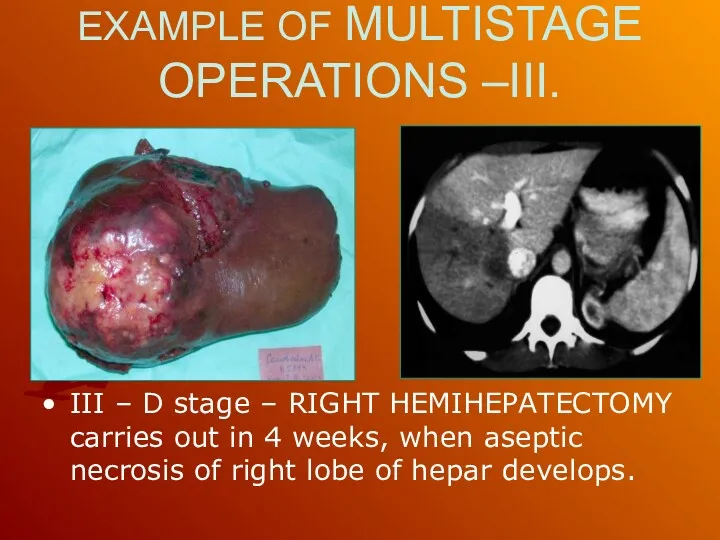
- 107. EXAMPLE OF MULTISTAGE OPERATIONS –III. III – D stage – RIGHT HEMIHEPATECTOMY carries out in 4
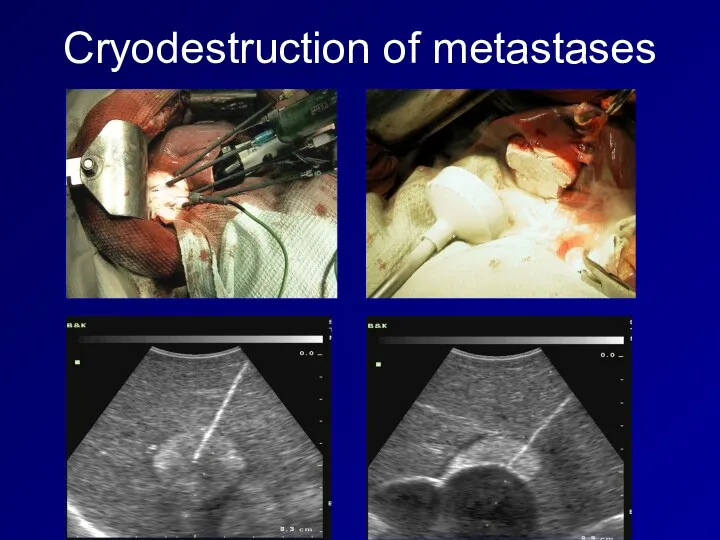
- 108. Treatment of tumors-XII Besides classical surgical treatment laser- or cryodestruction is performed. Cryodestruction is used in
- 109. Cryodestruction of metastases
- 110. Treatment of tumors-XIII Radiation therapy. Application of radiation therapy for treatment of oncological patients is based
- 111. Treatment of tumors-XIV The efficiency of the damage of tumor cells de-pend on the size of
- 112. Treatment of tumors-XV Existing difference in radio-sensitivity of tumor and normal tissue is causes the development
- 113. Treatment of tumors-XVI Different kinds of electromagnetic or cor-puscular irradiation are used for radiation therapy, namely:
- 114. Treatment of tumors-XVII In the external (distance) radiation devises for X-ray therapy and telegammatherapy (isotopes Co
- 115. Treatment of tumors-XVIII Intracaval radiation allows to move a source of radiation near the place of
- 116. Treatment of tumors-XIX Applique ’radiation is indicated in the relatively superficial tumors (of the skin, low
- 117. Treatment of tumors-XX Interstitical radiation is carried out be introducing into tumoral tissue radioac-tive needles, hollow
- 118. Treatment of tumors-XXI Depending on the purpose of radiation therapy /if it is used independently/ is
- 119. Treatment of tumors-XXII Radiation methods of treatment may be a part of combined or complex treatment
- 120. Treatment of tumors-XXIII Medicinal treatment,or chemotherapy – means the use of medicinal preparations, having a damage
- 121. Treatment of tumors-XXIV All preparations used for medicinal treatment of tumors are subdivided into two groups:
- 122. Treatment of tumors-XXV Proper chemotherapeutic preparations are subdivided into: 1) cytostatics: a) alkylating preparations; b) alkaloids;
- 123. Treatment of tumors-XXVI Cytostatics inhibit reproduction of tumor cells, oppressing their mitotic activity. At that alkylating
- 124. Treatment of tumors-XXVII Antitumoral antibiotics (doxorubicin, bleomycin, rubromycin, mitomycin) suppress DNA and RNA synthesis, strengthen activity
- 125. Treatment of tumors-XXVIII Taking into account up-to-date abilities of chemotherapy all tumors may be conditionally subdivided
- 126. Treatment of tumors-XXIX 3. tumors with low sensitivity to the action of chemotherapy (cancers of GIT,
- 128. Скачать презентацию
Tumor(s). /Lat., neoplasm, new growth/, pathological blastoma formation, spontaneously originating in
Tumor(s). /Lat., neoplasm, new growth/, pathological blastoma formation, spontaneously originating in
Benign tumors
possess expensive growth, resulting at that surrounding tissues move apart,
Benign tumors
possess expensive growth, resulting at that surrounding tissues move apart,
Benign tumors (example); neurofibromatosis & lipoma.
Benign tumors (example); neurofibromatosis & lipoma.
Benign tumors (example);
cavernous hemangioma & rectal polyps.
Benign tumors (example);
cavernous hemangioma & rectal polyps.
Malignant tumors
infiltrate and destroy surrounding tissues. Infiltrative (invasive) growth is the
Malignant tumors
infiltrate and destroy surrounding tissues. Infiltrative (invasive) growth is the
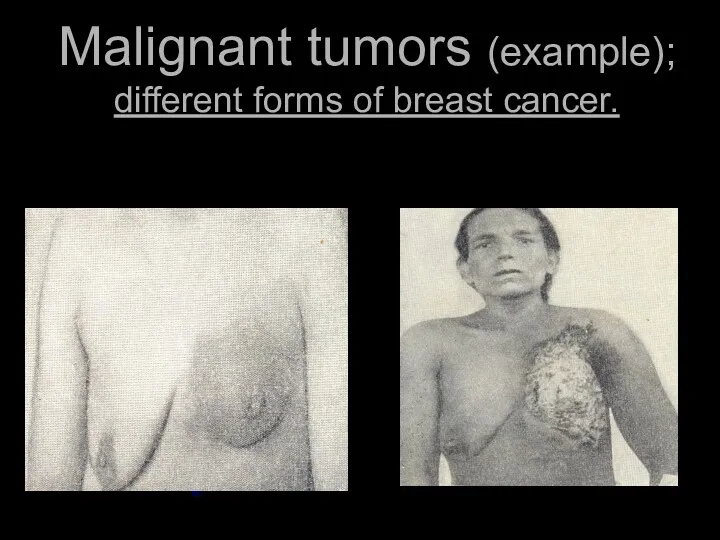
Malignant tumors (example); different forms of breast cancer.
Malignant tumors (example); different forms of breast cancer.
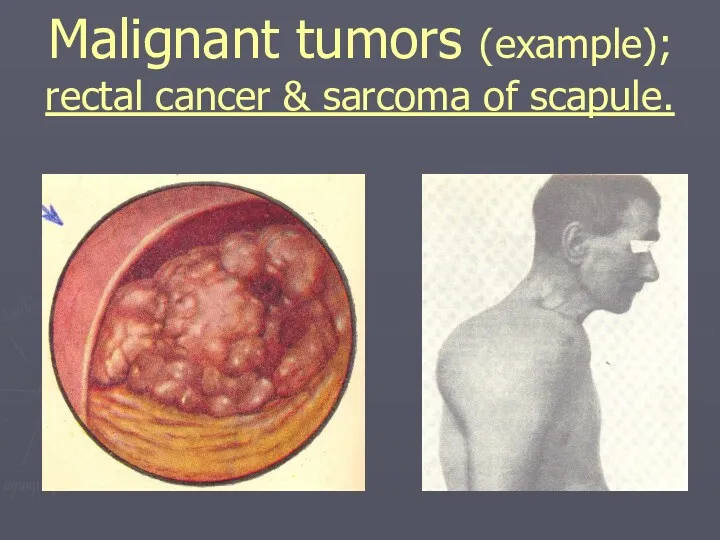
Malignant tumors (example);
rectal cancer & sarcoma of scapule.
Malignant tumors (example);
rectal cancer & sarcoma of scapule.
Annually
6 mln people fall ill with tumors and 5 mln
Annually
6 mln people fall ill with tumors and 5 mln
In males the most part from all cases of malignant tumors
In males the most part from all cases of malignant tumors
ETIOLOGY
1) Vihrov’s theory of irritation.
2) Kangeim’s theory of embryonic
ETIOLOGY
1) Vihrov’s theory of irritation.
2) Kangeim’s theory of embryonic
At present tumors are considered to be polyetiologic diseases.
In
At present tumors are considered to be polyetiologic diseases.
In
For the origin of tumor it is of necessity the presence
For the origin of tumor it is of necessity the presence
Various etiological factors predominate in tumours ethiology with different localization-I.
One
Various etiological factors predominate in tumours ethiology with different localization-I.
One
Various etiological factors predominate in tumours ethiology with different localization-II.
Tumors of
Various etiological factors predominate in tumours ethiology with different localization-II.
Tumors of
PATHOGENESIS-I.
Arise of cancer is always separated from the moment of
PATHOGENESIS-I. Arise of cancer is always separated from the moment of
PATHOGENESIS-II.
At that, the cell as a result of the genome modification
PATHOGENESIS-II.
At that, the cell as a result of the genome modification
PATHOGENESIS-III.
The increase of immune exertion is a result of the process
PATHOGENESIS-III.
The increase of immune exertion is a result of the process
PATHOGENESIS-IV.
The main components, predetermining the origin of tumor are:
a) local preparedness
PATHOGENESIS-IV.
The main components, predetermining the origin of tumor are:
a) local preparedness
PATHOGENESIS-V.
Presence of precancerous condition of the organ or tissue is the
PATHOGENESIS-V.
Presence of precancerous condition of the organ or tissue is the
PATHOGENESIS-VI.
Common factors predisposing to the development of malignant process:
1) genetic predisposion;
2)
PATHOGENESIS-VI.
Common factors predisposing to the development of malignant process:
1) genetic predisposion;
2)
Influence of benign tumors on the organism.
Despite of the fact
Influence of benign tumors on the organism.
Despite of the fact
Influence of malignant tumors on the organism (in common).
Two interrelated
Influence of malignant tumors on the organism (in common).
Two interrelated
Influence of malignant tumors on the organism-I.
In carbohydrate metabolism.
-
Influence of malignant tumors on the organism-I.
In carbohydrate metabolism.
-
Influence of malignant tumors on the organism-II.
In aminoacide metabolism.
Tumor tissue is
Influence of malignant tumors on the organism-II.
In aminoacide metabolism.
Tumor tissue is
Influence of malignant tumors on the organism-III.
In fatty /lipids/ metabolism.
Growth of
Influence of malignant tumors on the organism-III.
In fatty /lipids/ metabolism.
Growth of
Nomenclature, structure & classification of tumors-I.
Histogenetic and histological principles are
Nomenclature, structure & classification of tumors-I.
Histogenetic and histological principles are
Nomenclature, structure & classification of tumors-II.
In the name of tumor besides
Nomenclature, structure & classification of tumors-II.
In the name of tumor besides
Nomenclature, structure & classification of tumors-III.
Quite often in the name of
Nomenclature, structure & classification of tumors-III.
Quite often in the name of
Nomenclature, structure & classification of tumors-IV.
Under the conception of possible sources
Nomenclature, structure & classification of tumors-IV.
Under the conception of possible sources
Nomenclature, structure & classification of tumors-V.
Malignant connective (-tissue) tumors have got
Nomenclature, structure & classification of tumors-V.
Malignant connective (-tissue) tumors have got
Nomenclature, structure & classification of tumors-VI.
Technologically various is indication of tumor
Nomenclature, structure & classification of tumors-VI.
Technologically various is indication of tumor
Nomenclature, structure & classification of tumors-VII.
CANCER /from Lat./ - malignant tumor,
Nomenclature, structure & classification of tumors-VII.
CANCER /from Lat./ - malignant tumor,
Nomenclature, structure & classification of tumors-VIII.
However not all mentioned features of
Nomenclature, structure & classification of tumors-VIII.
However not all mentioned features of
Nomenclature, structure & classification of tumors-IX.
Macroscopic view of tumor is various
Nomenclature, structure & classification of tumors-IX.
Macroscopic view of tumor is various
Nomenclature, structure & classification of tumors-X.
Relating to the lumen of the
Nomenclature, structure & classification of tumors-X.
Relating to the lumen of the
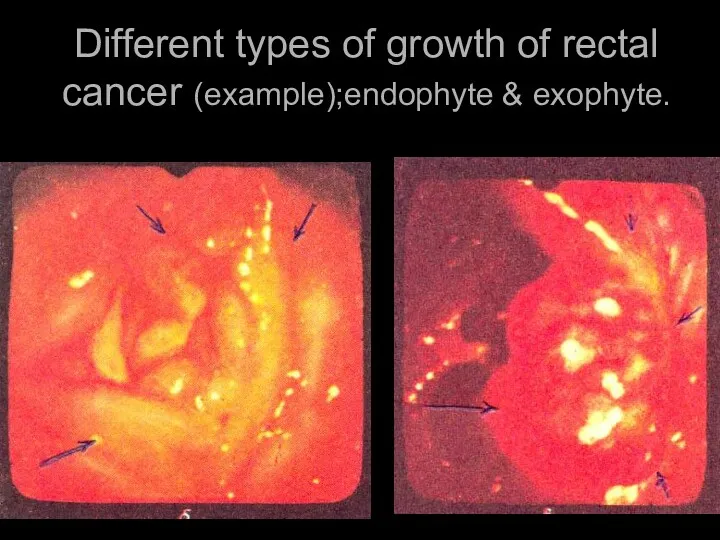
Different types of growth of rectal cancer (example);endophyte & exophyte.
Different types of growth of rectal cancer (example);endophyte & exophyte.
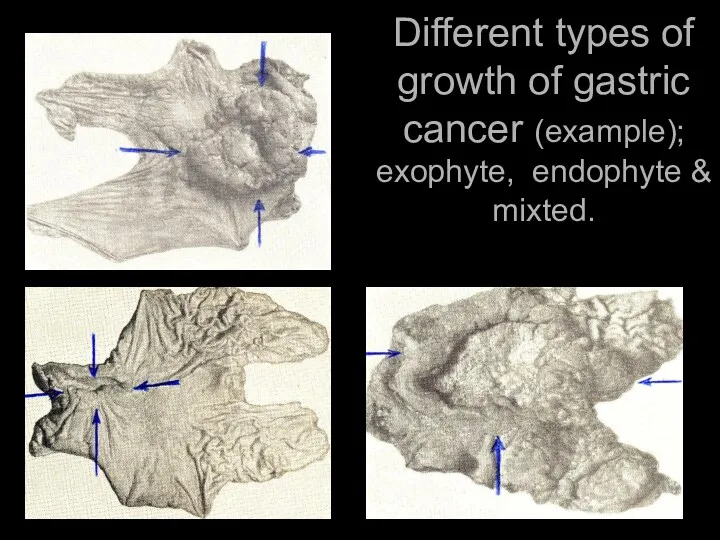
Different types of growth of gastric cancer (example); exophyte, endophyte &
Different types of growth of gastric cancer (example); exophyte, endophyte &
Nomenclature, structure & classification of tumors-XI.
Sometimes the tumor as if infiltrates
Nomenclature, structure & classification of tumors-XI.
Sometimes the tumor as if infiltrates
Nomenclature, structure & classification of tumors-XII.
The base for diagnosis of tumor
Nomenclature, structure & classification of tumors-XII.
The base for diagnosis of tumor
Nomenclature, structure & classification of tumors-XIII.
Microscopic investigation of tumor displays the
Nomenclature, structure & classification of tumors-XIII.
Microscopic investigation of tumor displays the
Nomenclature, structure & classification of tumors-XIV.
Structural atipicity of tumor spreads over
Nomenclature, structure & classification of tumors-XIV.
Structural atipicity of tumor spreads over
Nomenclature, structure & classification of tumors-XV.
Structure and classification of cancer.
The
Nomenclature, structure & classification of tumors-XV.
Structure and classification of cancer.
The
Nomenclature, structure & classification of tumors-XVI.
In benign tumors of epithelial nature
Nomenclature, structure & classification of tumors-XVI.
In benign tumors of epithelial nature
Nomenclature, structure & classification of tumors-XVII.
For the cancer in which tumor
Nomenclature, structure & classification of tumors-XVII.
For the cancer in which tumor
Nomenclature, structure & classification of tumors-XVIII.
Cancer, having endophytic growth spreads mainly
Nomenclature, structure & classification of tumors-XVIII.
Cancer, having endophytic growth spreads mainly
Nomenclature, structure & classification of tumors-XIX.
In some kinds of cancer due
Nomenclature, structure & classification of tumors-XIX.
In some kinds of cancer due
Nomenclature, structure & classification of tumors-XX.
Quite often the base for indication
Nomenclature, structure & classification of tumors-XX.
Quite often the base for indication
Nomenclature, structure & classification of tumors-XXI.
In intracellular production of mucus cancer
Nomenclature, structure & classification of tumors-XXI.
In intracellular production of mucus cancer
Nomenclature, structure & classification of tumors-XXII.
Some kinds of cancer have
Nomenclature, structure & classification of tumors-XXII.
Some kinds of cancer have
Nomenclature, structure & classification of tumors-XXIII.
At the same time epithelium of
Nomenclature, structure & classification of tumors-XXIII.
At the same time epithelium of
Nomenclature, structure & classification of tumors-XXIV.
Stromal component /besides epithelial component/ is
Nomenclature, structure & classification of tumors-XXIV.
Stromal component /besides epithelial component/ is
Nomenclature, structure & classification of tumors-XXV.
The other forms of cancer in
Nomenclature, structure & classification of tumors-XXV.
The other forms of cancer in
Nomenclature, structure & classification of tumors-XXVI.
On the ground of histological structure,
Nomenclature, structure & classification of tumors-XXVI.
On the ground of histological structure,
Nomenclature, structure & classification of tumors-XXVII.
It is International
Nomenclature, structure & classification of tumors-XXVII.
It is International
Nomenclature, structure & classification of tumors-XXVIII.
Spread of the primary tumor node
Nomenclature, structure & classification of tumors-XXVIII.
Spread of the primary tumor node
Nomenclature, structure & classification of tumors-XXVIX.
For mammary gland tumor the
Nomenclature, structure & classification of tumors-XXVIX.
For mammary gland tumor the
Nomenclature, structure & classification of tumors-XXX.
Symbol N (nodulus) is used to
Nomenclature, structure & classification of tumors-XXX.
Symbol N (nodulus) is used to
Nomenclature, structure & classification of tumors-XXXI.
Symbol M (metastases) indicates the presence
Nomenclature, structure & classification of tumors-XXXI.
Symbol M (metastases) indicates the presence
Nomenclature, structure & classification of tumors-XXXII.
Index G (grade) – defines the
Nomenclature, structure & classification of tumors-XXXII.
Index G (grade) – defines the
Nomenclature, structure & classification of tumors-XXXIII.
Index P (penetration) is introduced only
Nomenclature, structure & classification of tumors-XXXIII.
Index P (penetration) is introduced only
Nomenclature, structure & classification of tumors-XXXIV.
Classification by TNM system is considered
Nomenclature, structure & classification of tumors-XXXIV.
Classification by TNM system is considered
Nomenclature, structure & classification of tumors-XXXV.
According to clinical classification four stages
Nomenclature, structure & classification of tumors-XXXV.
According to clinical classification four stages
Nomenclature, structure & classification of tumors-XXXVI.
stage III– tumor has great sizes,
Nomenclature, structure & classification of tumors-XXXVI.
stage III– tumor has great sizes,
Nomenclature, structure & classification of tumors-XXXVII.
For every location of malignant tumor
Nomenclature, structure & classification of tumors-XXXVII.
For every location of malignant tumor
Clinical picture & diagnosis of tumors-I.
Diagnosis of benign tumors is
Clinical picture & diagnosis of tumors-I.
Diagnosis of benign tumors is
Clinical picture & diagnosis of tumors. (EXAMPLE).ELEVATED POSITION & RETRACTION OF
Clinical picture & diagnosis of tumors. (EXAMPLE).ELEVATED POSITION & RETRACTION OF
Clinical picture & diagnosis of tumors-II.
In clinical pictures of malignant tumors
Clinical picture & diagnosis of tumors-II.
In clinical pictures of malignant tumors
Сlinical picture of
malignant tumors-I
Syndrome “plus-tissue”. Tumor may be founded
Сlinical picture of
malignant tumors-I
Syndrome “plus-tissue”. Tumor may be founded
Сlinical picture of
malignant tumors-II
Syndrome of pathological discharge. In the presence
Сlinical picture of
malignant tumors-II
Syndrome of pathological discharge. In the presence
Сlinical picture of
malignant tumors-III
Syndrome of the functional disorder. Manifestations of
Сlinical picture of
malignant tumors-III
Syndrome of the functional disorder. Manifestations of
Сlinical picture of malignant tumors-IV
Syndrome of small signs. The patients with
Сlinical picture of malignant tumors-IV
Syndrome of small signs. The patients with
Diagnostics of tumors-I
The base of tumor diagnosis is their timely identification
Diagnostics of tumors-I
The base of tumor diagnosis is their timely identification
Diagnostics of tumors-II
Diagnostics of tumors are subdivided into:
1) primary diagnostics,
Diagnostics of tumors-II
Diagnostics of tumors are subdivided into:
1) primary diagnostics,
Diagnostics of tumors-III
Clarifying diagnostics in patients with already revealed malignant tumor
Diagnostics of tumors-III
Clarifying diagnostics in patients with already revealed malignant tumor
Diagnostics of tumors-IV
Local criteria include: 1) adjusted location of
Diagnostics of tumors-IV
Local criteria include: 1) adjusted location of
Diagnostics of tumors-V
Along with estimation of the local and common
Diagnostics of tumors-V
Along with estimation of the local and common
Diagnostics of tumors-VI
X-ray investigation includes: 1) uncontrast & contrast methods. Uncontrast
Diagnostics of tumors-VI
X-ray investigation includes: 1) uncontrast & contrast methods. Uncontrast
Roentgenologic method in diagnostics of cancer (stomach & esophageus)
Roentgenologic method in diagnostics of cancer (stomach & esophageus)
USI /Doppler scanning/. Metastases of cancer in the liver.
USI /Doppler scanning/. Metastases of cancer in the liver.
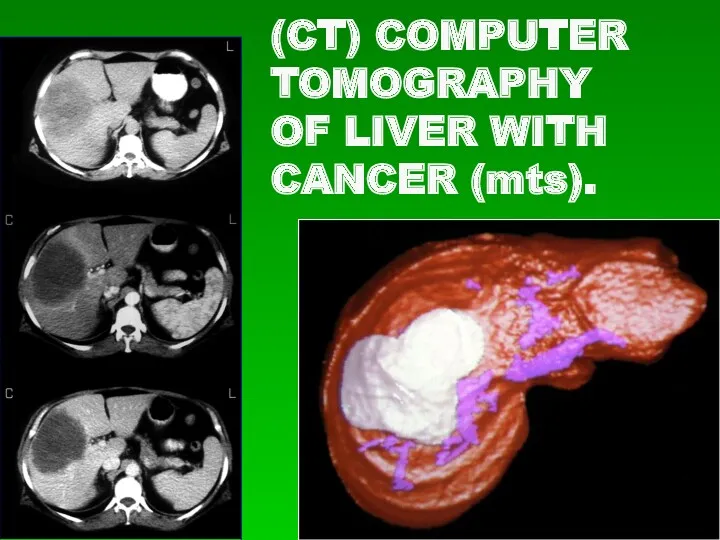
(CT) COMPUTER TOMOGRAPHY
OF LIVER WITH CANCER (mts).
(CT) COMPUTER TOMOGRAPHY
OF LIVER WITH CANCER (mts).
Diagnostics of tumors-VII
Endoscopic methods allow to carry out investigation with the
Diagnostics of tumors-VII
Endoscopic methods allow to carry out investigation with the
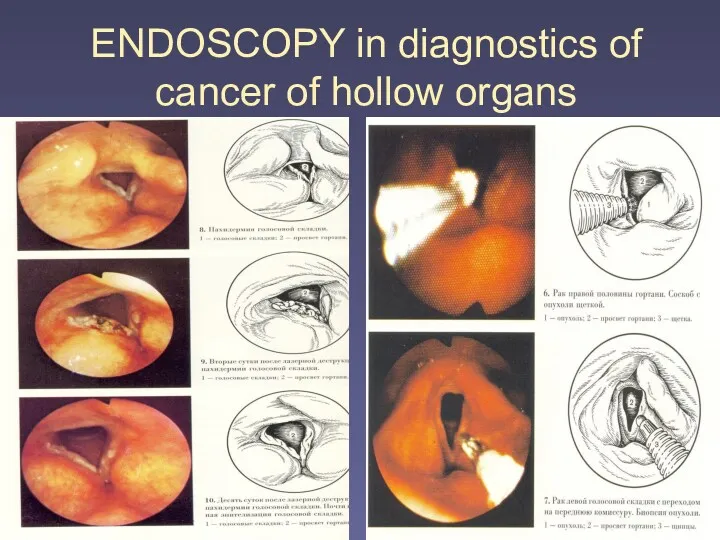
ENDOSCOPY in diagnostics of cancer of hollow organs
ENDOSCOPY in diagnostics of cancer of hollow organs
Diagnostics of tumors-VIII
In any case of tumor or in
Diagnostics of tumors-VIII
In any case of tumor or in
Diagnostics of tumors-IX
Radioisotopic methods of investigation are based on the ability
Diagnostics of tumors-IX
Radioisotopic methods of investigation are based on the ability
Diagnostics of tumors-X
Laboratory methods of diagnosis of malignant tumors are
Diagnostics of tumors-X
Laboratory methods of diagnosis of malignant tumors are
Diagnostics of tumors-XI
In the cases when the complex of clarifying
Diagnostics of tumors-XI
In the cases when the complex of clarifying
Treatment of tumors-I
Treatment of benign tumors - operative excision of
Treatment of tumors-I
Treatment of benign tumors - operative excision of
Treatment of tumors-II
Treatment of malignant tumors is fulfilled by various means
Treatment of tumors-II
Treatment of malignant tumors is fulfilled by various means
Treatment of tumors-III
The main methods of treating of malignant tumors are:
Treatment of tumors-III
The main methods of treating of malignant tumors are:
Treatment of tumors-IV
Surgical treatment is the main one in the most
Treatment of tumors-IV
Surgical treatment is the main one in the most
SURGICAL TREATMENT OF LIPOMA
SURGICAL TREATMENT OF LIPOMA
SURGICAL TREATMENT OF MELANOMA
SURGICAL TREATMENT OF MELANOMA
Treatment of tumors-V
During the removal of malignant new formation
Treatment of tumors-V
During the removal of malignant new formation
Example of principles of
oncological operations
D-S: CANCER OF RECTUM
OPERATION:
TOTAL ABDOMENO-PERINEAL
Example of principles of
oncological operations
D-S: CANCER OF RECTUM
OPERATION:
TOTAL ABDOMENO-PERINEAL
Example of principles of
oncological operations
D-S: CANCER OF STOMACH (IV stage).
Example of principles of
oncological operations
D-S: CANCER OF STOMACH (IV stage).
Treatment of tumors-VI
- Ablastics – complex of measures directed at prevention
Treatment of tumors-VI
- Ablastics – complex of measures directed at prevention
Treatment of tumors-VII
- Antiblastics – complex of measures directed at destruction
Treatment of tumors-VII
- Antiblastics – complex of measures directed at destruction
Treatment of tumors-VIII
- Zoning. During the operation for malignant tumor it
Treatment of tumors-VIII
- Zoning. During the operation for malignant tumor it
Example of principles of
oncological operations
D-S: C-r of the right part
Example of principles of
oncological operations
D-S: C-r of the right part
Treatment of tumors-IX
In exophytic growth of tumor /when its base is
Treatment of tumors-IX
In exophytic growth of tumor /when its base is
Example of principles of
oncological operations
D-S: С-r of the right mammary
Example of principles of
oncological operations
D-S: С-r of the right mammary
Treatment of tumors-X
(Saving/keeping/ «case»). Lymph vessels and nodes, through wich is
Treatment of tumors-X
(Saving/keeping/ «case»). Lymph vessels and nodes, through wich is
Treatment of tumors-XI
Radical operations in cancer of any location may be
Treatment of tumors-XI
Radical operations in cancer of any location may be
EXAMPLE OF MULTISTAGE OPERATIONS –I.
D-S: С-R OF COLON DESCENDENS
I – st
EXAMPLE OF MULTISTAGE OPERATIONS –I.
D-S: С-R OF COLON DESCENDENS
I – st
EXAMPLE OF MULTISTAGE OPERATIONS –II.
II –nd STAGE – EMBOLISATION OF RIGHT
EXAMPLE OF MULTISTAGE OPERATIONS –II.
II –nd STAGE – EMBOLISATION OF RIGHT
EXAMPLE OF MULTISTAGE OPERATIONS –III.
III – D stage – RIGHT HEMIHEPATECTOMY
EXAMPLE OF MULTISTAGE OPERATIONS –III.
III – D stage – RIGHT HEMIHEPATECTOMY
Treatment of tumors-XII
Besides classical surgical treatment laser- or cryodestruction is performed.
Treatment of tumors-XII
Besides classical surgical treatment laser- or cryodestruction is performed.
Cryodestruction of metastases
Cryodestruction of metastases
Treatment of tumors-XIII
Radiation therapy. Application of radiation therapy for treatment of
Treatment of tumors-XIII
Radiation therapy. Application of radiation therapy for treatment of
Treatment of tumors-XIV
The efficiency of the damage of tumor cells
Treatment of tumors-XIV
The efficiency of the damage of tumor cells
Treatment of tumors-XV
Existing difference in radio-sensitivity of tumor and normal tissue
Treatment of tumors-XV
Existing difference in radio-sensitivity of tumor and normal tissue
Treatment of tumors-XVI
Different kinds of electromagnetic or cor-puscular irradiation are used
Treatment of tumors-XVI
Different kinds of electromagnetic or cor-puscular irradiation are used
Treatment of tumors-XVII
In the external (distance) radiation devises for X-ray therapy
Treatment of tumors-XVII
In the external (distance) radiation devises for X-ray therapy
Treatment of tumors-XVIII
Intracaval radiation allows to move a source of radiation
Treatment of tumors-XVIII
Intracaval radiation allows to move a source of radiation
Treatment of tumors-XIX
Applique ’radiation is indicated in the relatively superficial
Treatment of tumors-XIX
Applique ’radiation is indicated in the relatively superficial
Treatment of tumors-XX
Interstitical radiation is carried out be introducing into tumoral
Treatment of tumors-XX
Interstitical radiation is carried out be introducing into tumoral
Treatment of tumors-XXI
Depending on the purpose of radiation therapy /if it
Treatment of tumors-XXI
Depending on the purpose of radiation therapy /if it
Treatment of tumors-XXII
Radiation methods of treatment may be a part
Treatment of tumors-XXII
Radiation methods of treatment may be a part
Treatment of tumors-XXIII
Medicinal treatment,or chemotherapy – means the use of medicinal
Treatment of tumors-XXIII
Medicinal treatment,or chemotherapy – means the use of medicinal
Treatment of tumors-XXIV
All preparations used for medicinal treatment of tumors
Treatment of tumors-XXIV
All preparations used for medicinal treatment of tumors
Treatment of tumors-XXV
Proper chemotherapeutic preparations are subdivided into:
1) cytostatics:
a)
Treatment of tumors-XXV
Proper chemotherapeutic preparations are subdivided into:
1) cytostatics:
a)
Treatment of tumors-XXVI
Cytostatics inhibit reproduction of tumor cells, oppressing their mitotic
Treatment of tumors-XXVI
Cytostatics inhibit reproduction of tumor cells, oppressing their mitotic
Treatment of tumors-XXVII
Antitumoral antibiotics (doxorubicin, bleomycin, rubromycin, mitomycin) suppress DNA and
Treatment of tumors-XXVII
Antitumoral antibiotics (doxorubicin, bleomycin, rubromycin, mitomycin) suppress DNA and
Treatment of tumors-XXVIII
Taking into account up-to-date abilities of chemotherapy all
Treatment of tumors-XXVIII
Taking into account up-to-date abilities of chemotherapy all
Treatment of tumors-XXIX
3. tumors with low sensitivity to the action
Treatment of tumors-XXIX
3. tumors with low sensitivity to the action
 Диагностика и лечение острой диареи
Диагностика и лечение острой диареи Жұлынның зақымдалу синдромдары
Жұлынның зақымдалу синдромдары Бабж – диарея
Бабж – диарея Движение крови по сосудам
Движение крови по сосудам Введение в травматологию и ортопедию. (Лекция 1)
Введение в травматологию и ортопедию. (Лекция 1) Қатерлі ісік ауруы
Қатерлі ісік ауруы Фармацевтическая технология жидких лекарственных форм
Фармацевтическая технология жидких лекарственных форм Закрытые травмы грудной клетки. Пневмоторакс.Гемоторакс.Тампонада сердца
Закрытые травмы грудной клетки. Пневмоторакс.Гемоторакс.Тампонада сердца Тауық гетеракидозын балау
Тауық гетеракидозын балау Порядок выдачи и оформления листков нетрудоспособности
Порядок выдачи и оформления листков нетрудоспособности ЭКГ-диагностика ишемической болезни сердца - стенокардии и инфаркта миокарда
ЭКГ-диагностика ишемической болезни сердца - стенокардии и инфаркта миокарда Салауатты өмір салтын қалыптастыру
Салауатты өмір салтын қалыптастыру Методы пренатальной дианостики
Методы пренатальной дианостики Распространенные заболевания в терапии
Распространенные заболевания в терапии Розовый лишай Жибера
Розовый лишай Жибера Сухожильный шов по Кюнео
Сухожильный шов по Кюнео Хронический панкреатит
Хронический панкреатит Әлеуметтік фактор эпидемиологияда
Әлеуметтік фактор эпидемиологияда Сыпной тиф
Сыпной тиф Риккетсиозы. Легионеллез. Возбудители, диагностика, эпидемиология, профилактика
Риккетсиозы. Легионеллез. Возбудители, диагностика, эпидемиология, профилактика Лечение в раннем восстановительном периоде перинатального поражения мозга
Лечение в раннем восстановительном периоде перинатального поражения мозга Возрастные особенности развития и функционирования эндокринной системы
Возрастные особенности развития и функционирования эндокринной системы Жүкті әйелдердегі ауруханадан тыс пневмония
Жүкті әйелдердегі ауруханадан тыс пневмония Сестринский уход при острых кишечных инфекциях у детей
Сестринский уход при острых кишечных инфекциях у детей Врачебный контроль в адаптивной физической культуре
Врачебный контроль в адаптивной физической культуре Классическая чума свиней
Классическая чума свиней Лечебно-охранительный режим в ЛПО
Лечебно-охранительный режим в ЛПО Дифференциальная диагностика острого аппендицита и сальпингоофорита
Дифференциальная диагностика острого аппендицита и сальпингоофорита